
Abstract
Study Design
Retrospective Cohort Study.
Objectives
There is an ongoing debate as to the influence of specialty training on spine surgery. Alomari et al. indicated the influence of specialty on ACDF procedures. However, deeper analysis into other spine procedures and lower-acuity procedures has yet to occur. In this study, we aim to determine if the outcomes of the low American Society of Anesthesiologists (ASA) classification (ASA 1&2) patients undergoing spine surgery vary based on whether the operating surgeon was an orthopedic surgeon or a neurosurgeon.
Methods
The NSQIP databases from 2015 to 2021 were queried based on the CPT code for nine common spine procedures. Indicators of surgical course and successful outcomes were documented and compared between specialties.
Results
Neurosurgeons had minimally shorter operative times in the ASA 1&2 combined classification (ASA-C) group for cervical, lumbar, and combined spinal procedural groups. Neurosurgeons had a slightly lower percentage of perioperative transfusions in select ASA-C classes. Orthopedic surgeons had shorter lengths of stay for the cervical groups in ASA-C and ASA-1 classes (ASA-1). However, many specialty differences found in spine patients become less pronounced when considering only ASA-1 patients. Finally, postoperative complication outcomes and re-admission were similar between orthopedic and neurological surgeons in all cases.
Conclusions
These results, while statistically significant, are very likely clinically insignificant. They demonstrate that both orthopedic surgeons and neurosurgeons perform spinal surgery exceedingly safely with similarly low complication rates. This lays the groundwork for future exploration and benchmarking of performance in spine surgeries across neurosurgery and orthopedics.
Keywords
Introduction
Spinal surgery encompasses a broad spectrum of diagnoses, procedure types, anatomical locations, and patient outcomes. Common spine surgery types include decompressive laminectomies, discectomies, instrumented fusion, deformity correction, or combinations thereof, and are typically performed by neurosurgeons or orthopedic surgeons. Detailed analyses comparing specialty-specific spinal procedure outcomes are still limited.1-5 In many studies, the effect size was small and likely clinically insignificant. Other related studies supported few statistically significant differences and, when significant, were unlikely to have an impact on clinical practice.2,6 Recently, Alomari et al. revealed that neurosurgeons perform about three times as many anterior cervical discectomies and fusions (ACDFs) as orthopedic surgeons. 1 They also showed that statistically, neurosurgeons achieved shorter hospital stays, lower perioperative blood transfusions, lower rates of sepsis, and operated on patient populations with more preoperative comorbidities; however, neurosurgeons did show longer operative times. 1 A study comparing 90-day outcomes of elective 1 and 2-level posterior lumbar fusions between the specialties indicated similar outcomes, except for increased wound complications and decreased dural tears when surgery is conducted by neurosurgeons. 2 Similarly, retrospective analysis of anterior lumbar fusions between specialties did not yield significant differences, aside from a higher risk for urinary tract infections and 30-day reoperation in the neurosurgery group. 7 Other studies have also supported small differences and mostly have not seen significant outcome differences between the two specialties.2,6 McCutcheon and colleagues presented data displaying that orthopedic patients have higher rates of perioperative blood transfusions after matching for various factors. 2 McCutcheon and other past studies focused on high-acuity patients or combined ASA classifications (ASA class 2+ patients)1,2 showing that high-acuity patients are more likely to be treated by neurosurgeons. While these studies have provided valuable insights into statistical specialty-specific differences, there remains a gap in the literature regarding the impact of surgeon specialty on patient outcomes in lower acuity cases.
Documentation of post-surgical outcomes for all surgical procedures has improved over recent decades partly due to the continuously expanding use of the National Surgical Quality Improvement Plan (NSQIP). 8 Created in the 1980s and currently managed by the American College of Surgeons, this database provides commonly accepted metrics for postoperative outcomes. As of today, more than 600 hospitals and over 65 Collaboratives participate in the quality metric reporting conducted by the NSQIP.8,9 The cost of spinal procedures often imposes a significant burden on both the healthcare system and the patient. As indicated in the report on Operating Room Procedures During Inpatient Stays in U.S. Hospitals in 2018, hospital stays involving spinal fusion accounted for the highest total expenditure for any procedure type, totaling $14.1 billion. 10 Surgical interventions that yield improved outcomes are crucial for alleviating this cost burden. 10 Understanding the differential outcomes between orthopedic and neurological approaches not only aids referring physicians in making informed clinical decisions but also opens avenues for understanding and collaboration between the specialties to optimize patient care. Given the considerable overlap in surgical competencies, cost burden, inconclusive historical results, and lack of outcome results on collective spinal operations, additional data comparing neurosurgical and orthopedic approaches to spine surgery is necessary.
In this study, we aim to determine if the outcomes and characteristics of low-ASA classification patients undergoing surgical interventions vary based on whether the surgeon operating was trained in orthopedics or neurosurgery. We obtained deidentified patient data on spinal surgical interventions, stratified according to the surgeon’s specialty. Indicators of the surgical course and outcomes were documented and compared between specialties at a patient population level.
Methods
Data Acquisition and Variables Collected
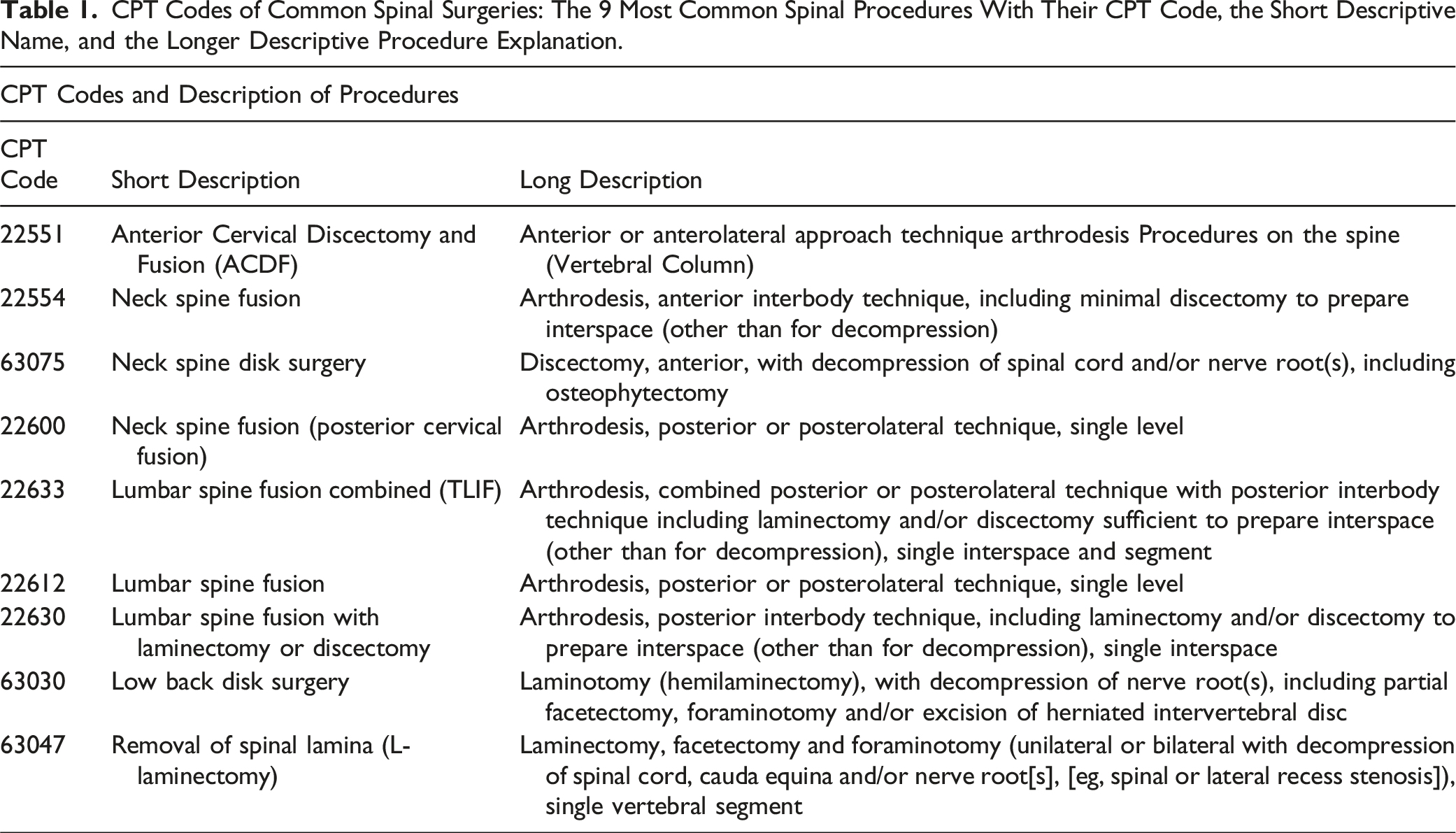
CPT Codes of Common Spinal Surgeries: The 9 Most Common Spinal Procedures With Their CPT Code, the Short Descriptive Name, and the Longer Descriptive Procedure Explanation.
Descriptive Statistics of Combined Spinal Procedure Patients: Demographic, Preoperative Comorbidity, and Surgical Outcome Data of the ASA-C Class Patient Population.
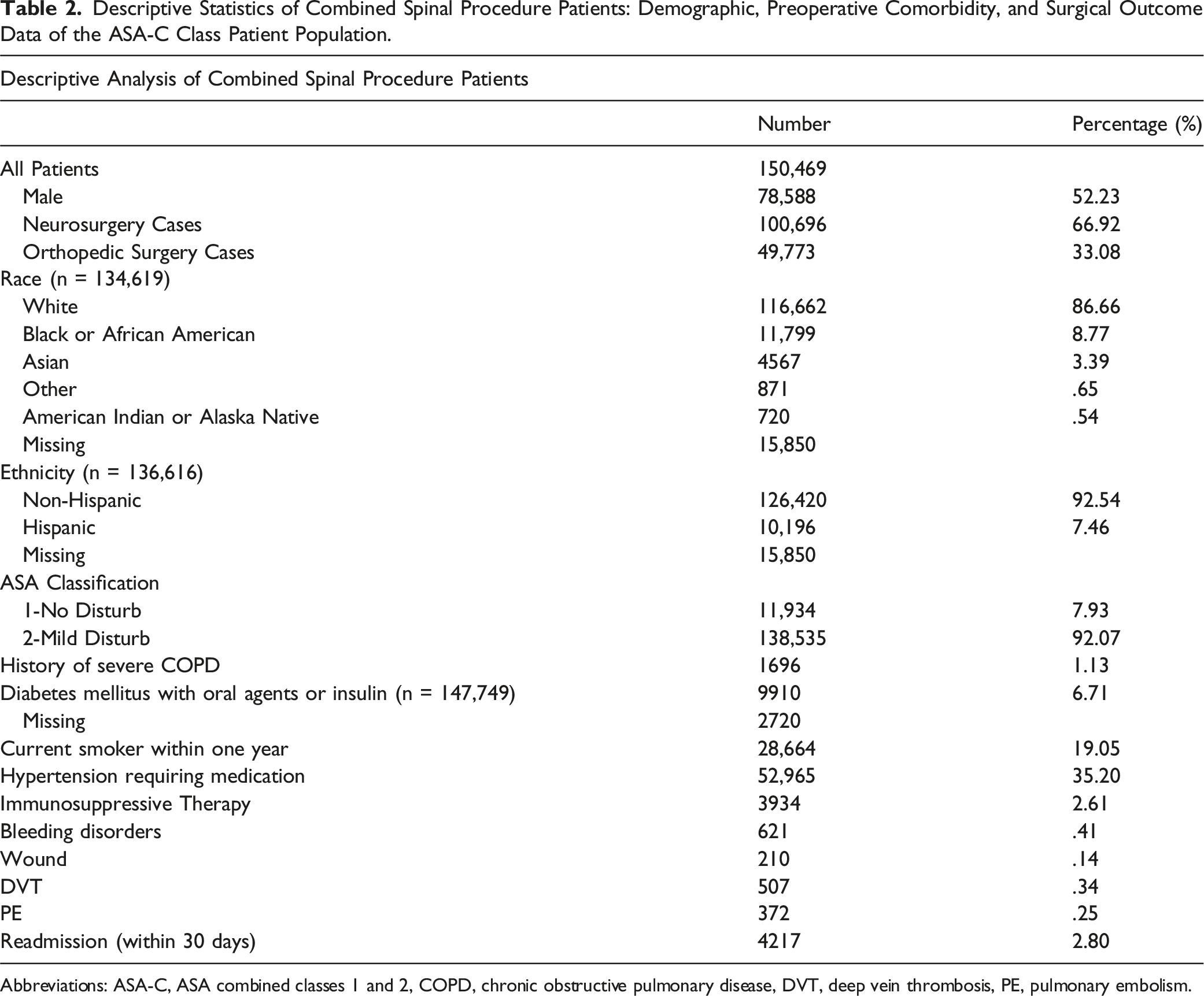
Abbreviations: ASA-C, ASA combined classes 1 and 2, COPD, chronic obstructive pulmonary disease, DVT, deep vein thrombosis, PE, pulmonary embolism.
Data Stratification
Patients were stratified into three spinal procedure groups by anatomical clusters (cervical, lumbar, and combined spinal procedure codes) since spinal operations are rarely completed as single CPT codes but rather as clusters of procedures (eg, laminectomy plus fusion). The combined spinal group consists of CPT codes 22551, 22554, 63075, 22600, 22633, 22612, 22630, 63030, and 63047. The cervical spinal group consists of CPT codes 22551, 22554, 63075, 22600, and 63047. The lumbar spinal group consists of CPT codes 22633, 22612, 22630, 63030, and 63047. These groupings can be found in Figure 1. The CPT codes for 63047, laminectomy, are recorded in both anatomical locations, so they were included in both anatomical location groups. CPT procedure codes by anatomical region: reported as CPT number - procedure name. CPT, current procedural terminology, ACDF, anterior cervical discectomy and fusion, created with biorender.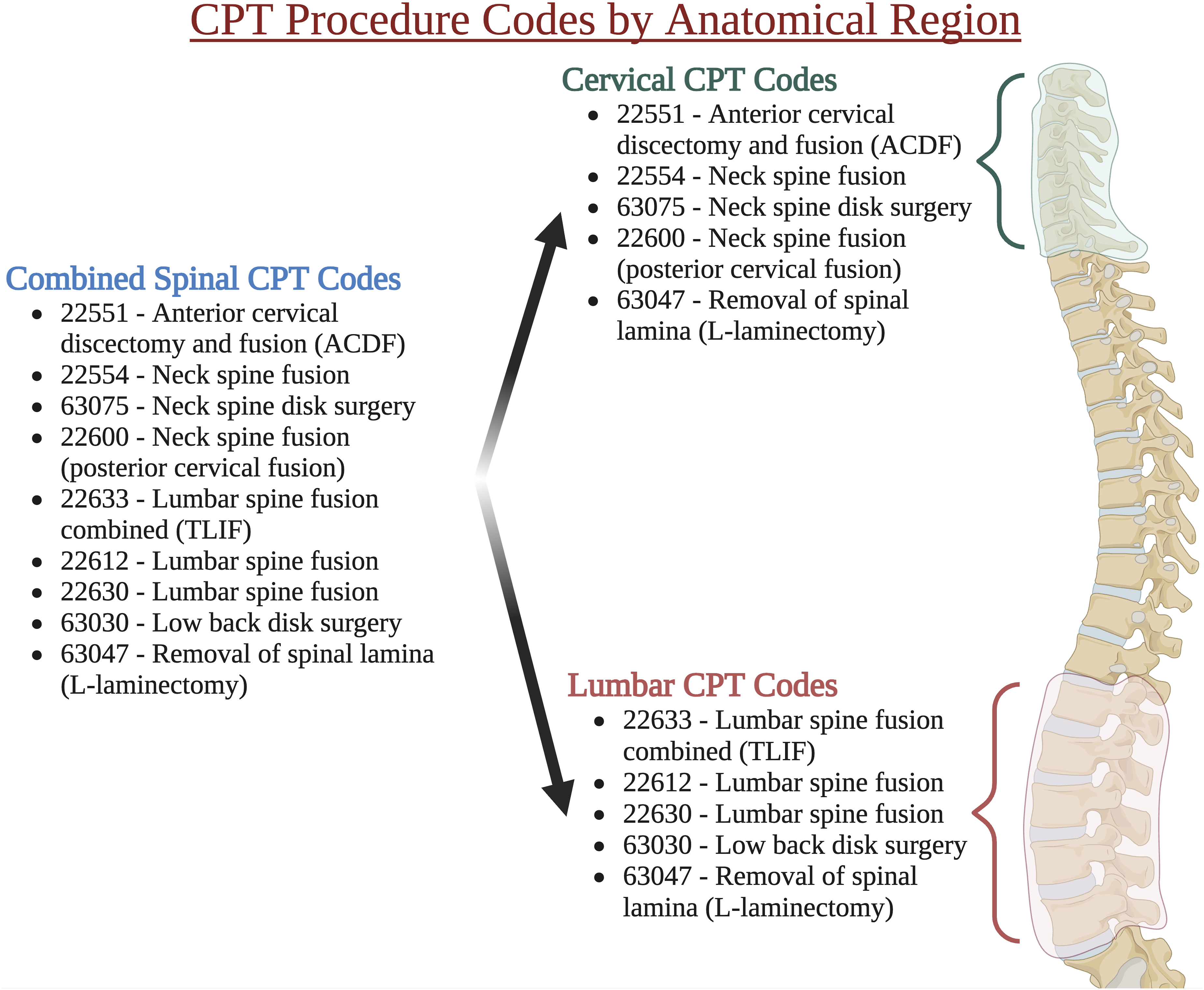
This data was then further stratified by ASA classification: a combined ASA-1&2 group (ASA-C), and an ASA-1 group (ASA-1). ASA classifications 1 and 2 indicate a healthy patient or a patient with non-life-threatening comorbidities, respectively. 13 These ASA classes were selected to minimize any potential contributing factors of more severe systemic disease and higher levels of comorbidities that may occur in ASA classes ≥ 3. The other demographic and preoperative factors above were chosen for their potential influence on the hospital course, discharge, and postoperative complications, and many were also included in past studies. 1
Initially, the study aimed to analyze and present ASA-1, ASA-2, and ASA-C individually between the two specialties. However, given the majority of patients fell under the ASA-2 classification (>90% for all given surgery comparisons) the presentation of only the ASA-2 classification is similar to the ASA-C group, so we chose to only present ASA-1 and ASA-C for comprehensive analysis.
Statistical Analysis
Continuous and categorical variables were described using means (standard deviations) and frequencies (proportions), respectively. For each categorical outcome, association with independent variables was assessed using t-tests and chi-squared tests, for continuous and categorical independent variables, respectively. For each continuous outcome, association with independent variables was assessed using correlation coefficient and t-test/ANOVA, for continuous and categorical independent variables, respectively. The surgical specialty was included in all models. The analysis was repeated restricting the dataset to ASA-1 patients, to those with cervical procedures, and to those with lumbar procedures.
All analyses were carried out using R version 4.3.1. and RStudio Build 421. 14
Results
Combined Spinal Procedure Outcomes
Combined Spinal Outcomes by Specialty: Comparison of Demographics, Preoperative Comorbidities, and Outcome Measures for ASA-C and ASA-1 Patients Between Neurosurgery and Orthopedic Surgery for all Spinal Procedures. The Data is Reported as Either: Mean ± Standard Deviation or as Number (Percentage). Data With Significant P-Values are Bolded. Operation Time is Reported in Minutes and Length of Stay is Reported in Days.
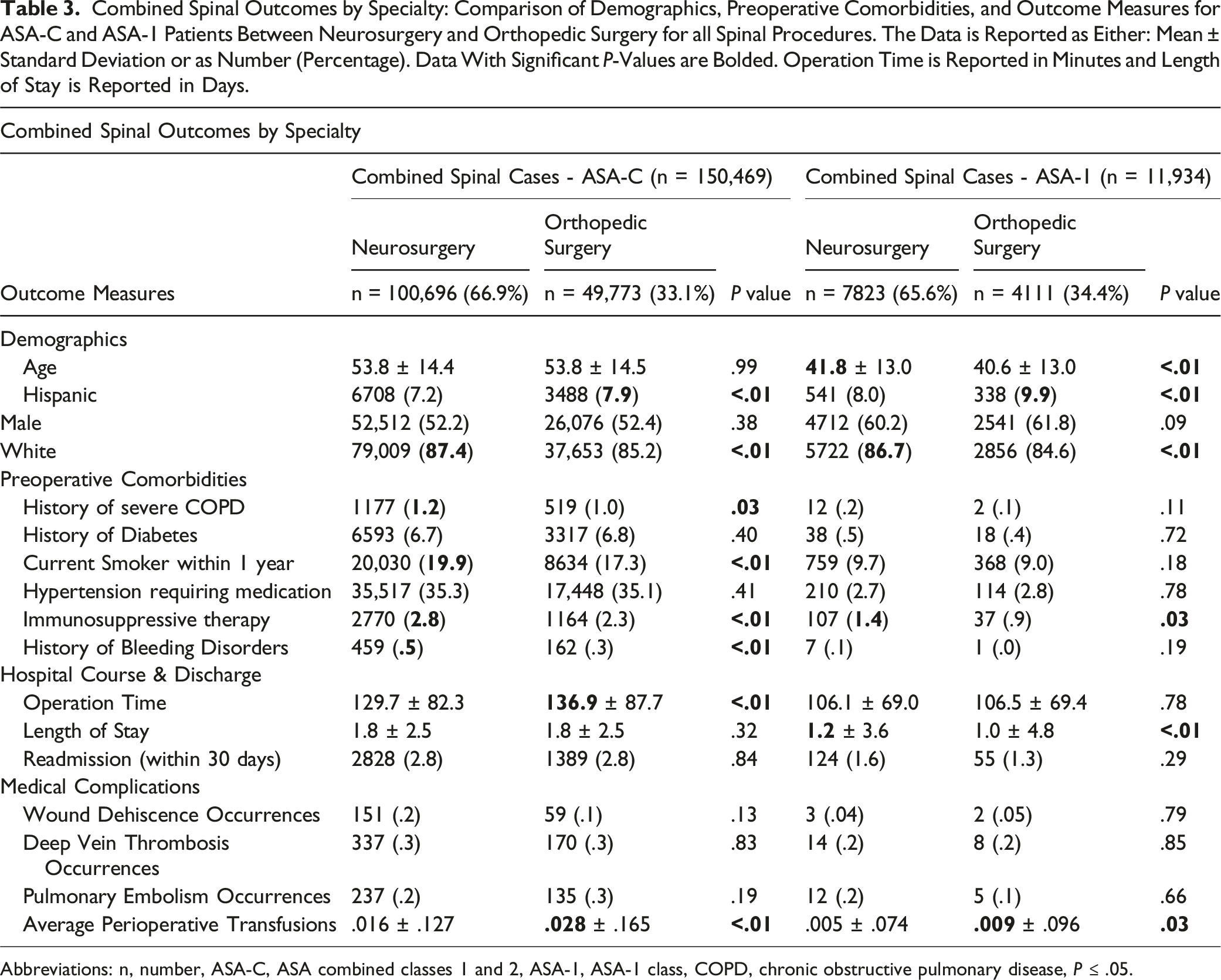
Abbreviations: n, number, ASA-C, ASA combined classes 1 and 2, ASA-1, ASA-1 class, COPD, chronic obstructive pulmonary disease, P ≤ .05.
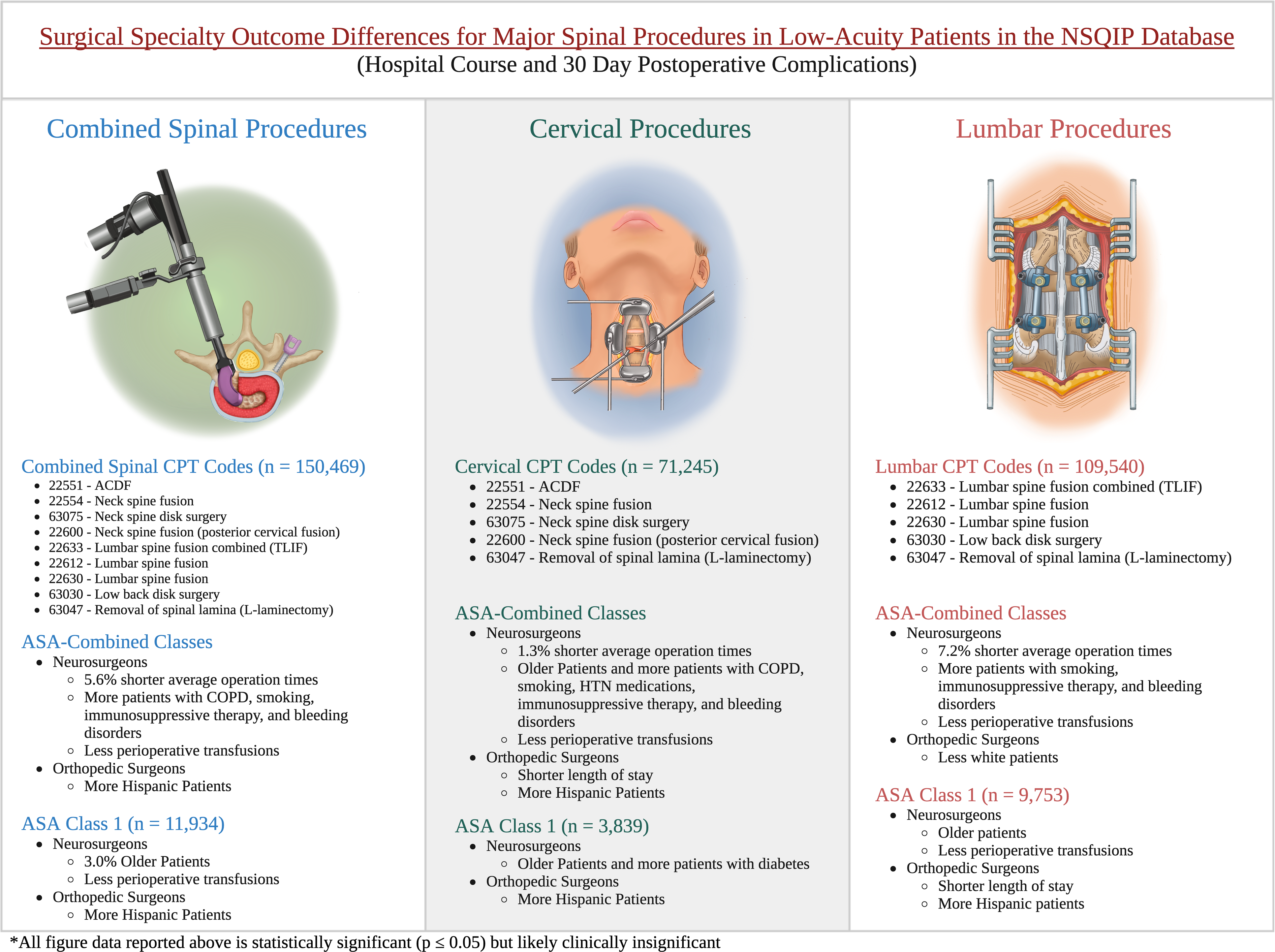
Surgical specialty outcomes by ASA-classification and anatomical region: generalized differences regarding the demographics, preoperative comorbidities, and surgical outcomes of ASA-C and ASA-1 patient populations between neurosurgery and orthopedic surgery by surgical region. ASA-C, ASA combined classes 1 and 2, ASA-1, ASA-1 class, CPT, current procedural terminology, ACDF, anterior cervical discectomy and fusion, COPD, chronic obstructive pulmonary disease, HTN, hypertension, created with biorender.
Cervical Procedure Outcomes
Cervical Spine Procedure Outcomes by Specialty: Comparison of Demographics, Preoperative Comorbidities, and Outcome Measures for ASA-C and ASA-1 Patients Between Neurosurgery and Orthopedic Surgery for Only Cervical Procedures. The Data is Reported as Either: Mean ± Standard Deviation or as Number (Percentage). Data With Significant P-Values are Bolded. Nearly Significant P-Values are Highlighted. Operation Time is Reported in Minutes and Length of Stay is Reported in Days.
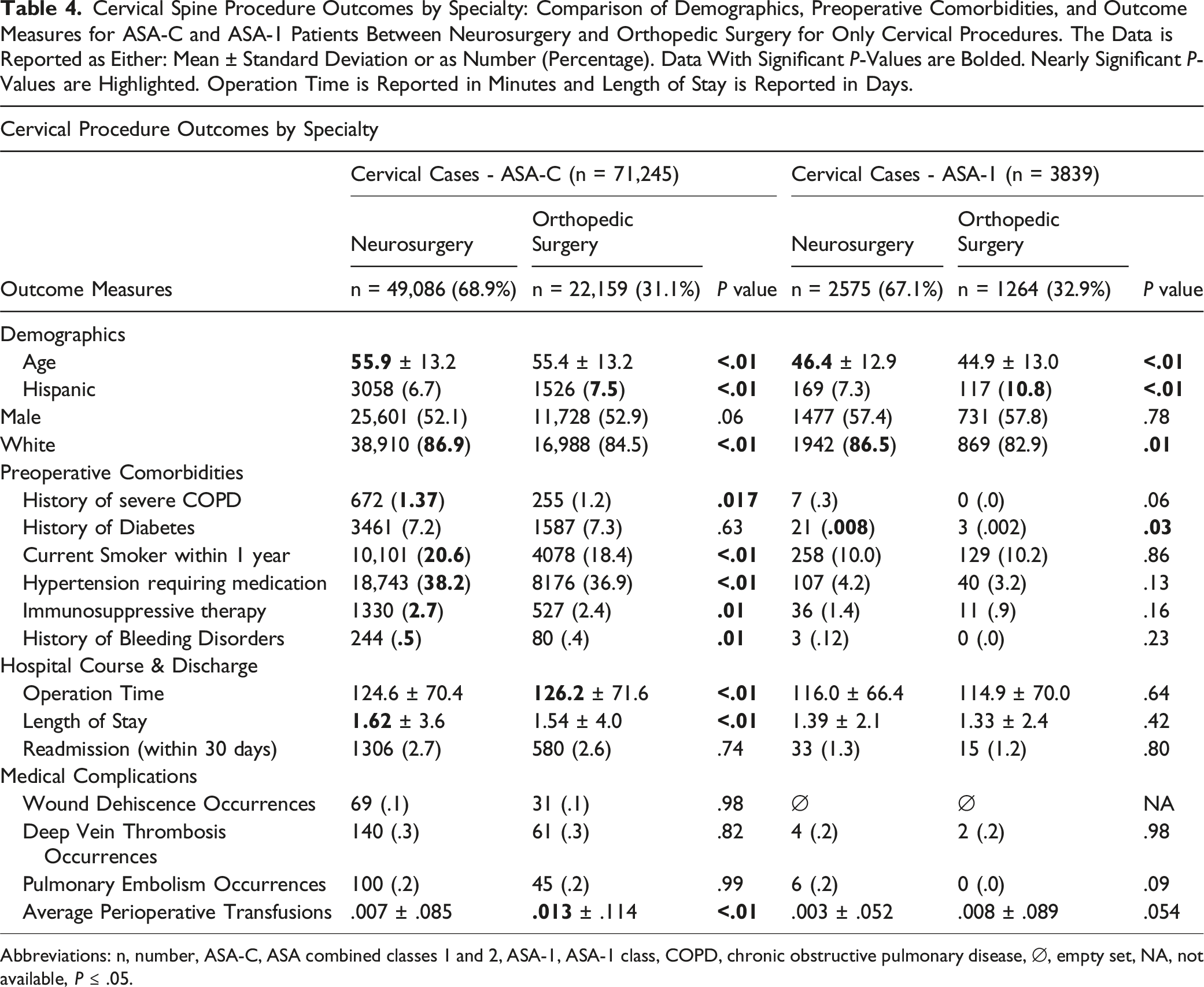
Abbreviations: n, number, ASA-C, ASA combined classes 1 and 2, ASA-1, ASA-1 class, COPD, chronic obstructive pulmonary disease, ∅, empty set, NA, not available, P ≤ .05.
Lumbar Procedure Outcomes
Lumbar Spine Procedure Outcomes by Specialty: Comparison of Demographics, Preoperative Comorbidities, and Outcome Measures for ASA-C and ASA-1 Patients Between Neurosurgery and Orthopedic Surgery for Only Lumbar Procedures. The Data is Reported as Either: Mean ± Standard Deviation or as Number (Percentage). Data With Significant P-Values are Bolded. Operation Time is Reported in Minutes and Length of Stay is Reported in Days.
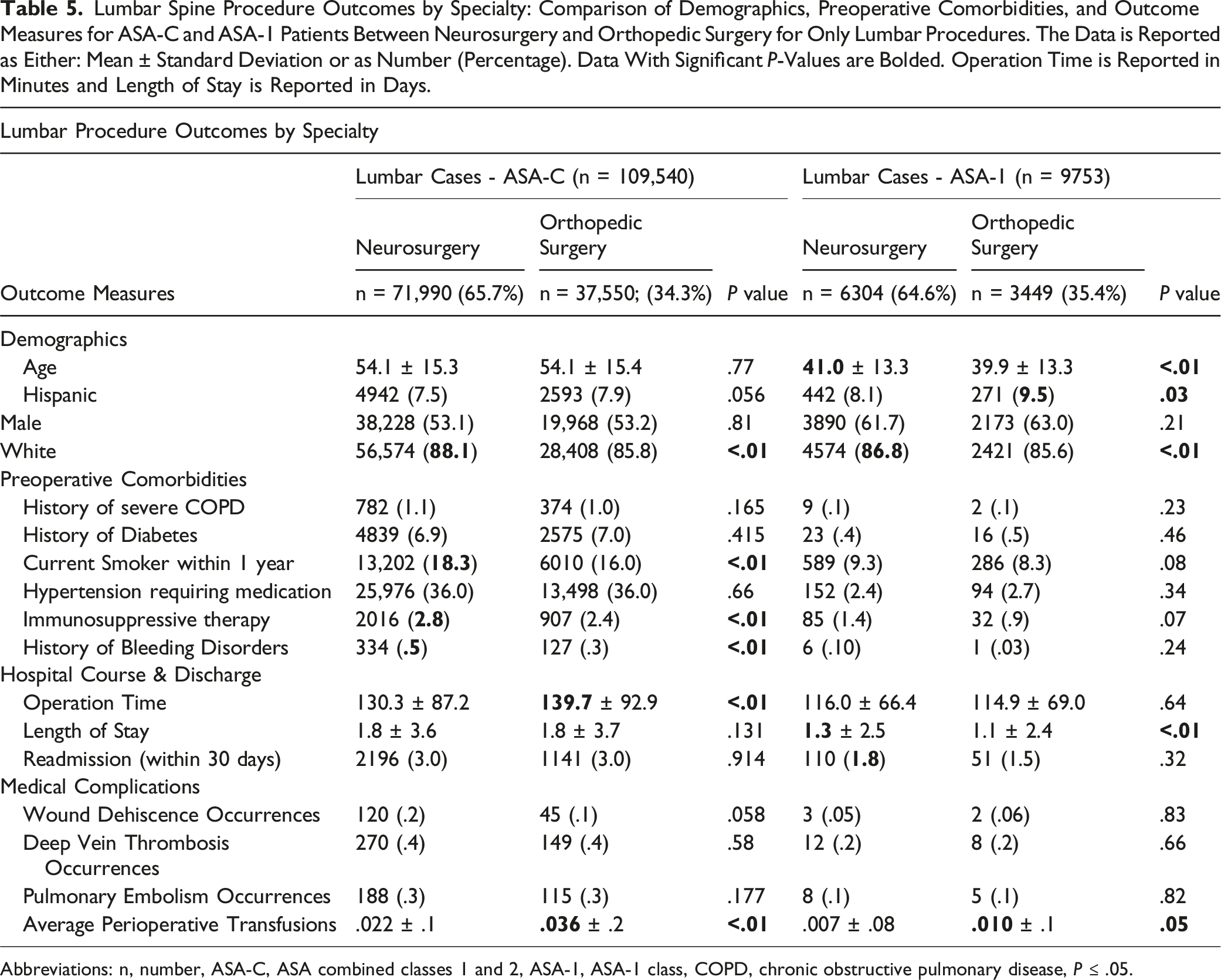
Abbreviations: n, number, ASA-C, ASA combined classes 1 and 2, ASA-1, ASA-1 class, COPD, chronic obstructive pulmonary disease, P ≤ .05.
Discussion
Comparing surgical specialties regarding spine outcomes continues to be challenging due to the varying metrics that define success. Commonly held qualities of a “successful” surgery, such as shorter operation times and fewer postoperative complications, have been previously used for comparison of orthopedic and neurological spine surgery.1,2,15 The observed differences are often clinically negligible. This analysis reaffirms many previous findings, highlighting statistically significant yet likely clinically insignificant differences between the specialties. Regardless of the training path, these outcomes represent real patients and the relief provided by both orthopedic and neurological surgeons. To date, there have been multiple database studies comparing orthopedic and neurosurgery outcomes for spine surgery, most of them (eg, McCutcheon 2 ) propensity match the patients to minimize any potential confounding variables and compare outcomes within groups of essentially identical patients. Our focus was slightly different, intending to compare the patient outcomes for these two specialties at a larger, unfiltered population level. This allows us to discuss the potential impacts of confounding variables on the outcomes. Past analyses have also investigated specific surgical procedures; however, spinal operations are rarely completed as single CPT codes but rather as clusters of codes (eg, laminectomy plus arthrodesis plus segmental instrumentation) usually pertaining to specific anatomical regions. This necessitates reconsideration for reporting categorical spinal outcomes such as our proposed anatomical groups (cervical, lumbar, and combined spinal procedures) rather than singular procedure types so that more generalizable inferences can be made (Supplemental Material).
We identified consistent demographic and pre-morbid patterns among patients in the ASA-C class undergoing orthopedic and neurosurgical interventions. The focus on the ASA-C group allows us to discuss outcomes in patients that are a majority ASA-2. Neurosurgeons tended to operate on patients with a greater burden of comorbidities, a trend that held across anatomical subgroups. Specifically, cervical cases managed by neurosurgeons more often involved hypertensive patients. Conversely, the prevalence of COPD, diabetes, and hypertension were statistically comparable between the two surgical specialties in the lumbar region.
When comparing all spinal cases in this study, neurosurgeons had statistically significantly shorter operation times by an average of 7.2 min. This difference, notably, is in opposition to past studies that reveal shorter operative times for orthopedic surgeons. Lambrechts et al. found that orthopedic surgeons were finished, on average, 14.28 min faster (95% CI: 8.07, 20.49) while Alomari et al. found orthopedists were finishing earlier in both single and multi-level ACDFs.1,15 However, the difference shown in our analysis was no longer observable when inspecting just the healthiest ASA-1 cases in both the combined spinal and anatomically divided groups. This suggests that routine procedures on the healthiest patients are performed with similar speed. Additionally, neurosurgeon operative times were a statistically significant 9.4 minutes shorter on average for lumbar spine surgery. It is unclear if shorter lumbar procedural times represent differences in case mix, surgical technique, training, or surgical efficiency. Future studies may address this.
It is also important to consider the clinical impact of these differences. While statistically significant, differences in surgical times under 10 min are by no means clinically significant for operations that are hours long. Though neurosurgeon surgery times were, on average, less than 10 min longer, outcomes between specialties were indistinguishable for post-operative wound dehiscence, deep vein thrombosis, pulmonary embolism, and re-admission. These similarities in positive outcome measures were consistent across each anatomical location and patient class. Additionally, previous studies have not established consistent differences in patient-reported outcome measures between specialties, and while we have presented statistically different differences, the clinical implications are likely marginal at best.
One important factor to consider is how operative time may affect transfusion rates. In our analysis, neurosurgical cases required slightly fewer transfusions in cervical, lumbar, and combined cases. This difference remained when specifically addressing the ASA-1 class which was possibly driven by the larger quantities of transfusions in lumbar cases. The shortened operative times could be a contributing factor to this decrease in intraoperative bleeding, and thus the lower transfusion rate seen in neurosurgeon cases. That said, it is difficult to confirm that differences in operative time under 10 min would make a clinical impact on postoperative transfusion rates. For example, Alomari et al. and Lambrechts et al. both found neurosurgeons to have longer operative times but also fewer post-operative transfusions.1,15 This is more indicative of other factors at play besides small differences in operative time. It is possible that criteria for transfusion may vary between specialties and neurosurgeons may be more conservative in this regard.
Clinically, differences in transfusion rates offer a possible way to maximize patient safety and minimize healthcare costs. Because increased blood transfusions lead to higher perioperative morbidity, reductions in transfusion rates not only protect patients but also can save health systems financially.16,17 One major hospital reduced the use of blood products by 26.1% and saved over $2,200,000 in a single year. 17 This highlights both the medical and financial benefits of reducing transfusion rates for colleagues in both neurosurgical and orthopedic specialties. While both specialties boast low transfusion rates for spine surgery, the goal should always be fewer if possible.
For postoperative stay, in all anatomical and ASA subgroups except the cervical ASA-1 and lumbar ASA-C cohorts, neurosurgery patients experienced longer stays compared to their orthopedic counterparts. It is plausible that orthopedic surgeons may systematically aim for earlier discharges, potentially emphasizing outpatient management as part of a care strategy. By emphasizing earlier discharge, patients can return to a more comfortable environment to both begin recovery as well as avoid major healthcare costs associated with inpatient stays. As for ASA-C cervical cases, the significantly longer hospital stays observed among neurosurgeons’ patients could be linked to a higher incidence of comorbidities, which may necessitate more extensive inpatient management and rehabilitation.
As with transfusion rates, reducing the length of stay poses significant opportunities for health systems to reduce the financial burdens of surgical intervention.18-20 While reducing the length of stay relies on many moving pieces, surgeons play a central role in postoperative planning. When surgeons implement programs such as at-home rehab programs or case management, patients are able to move to at-home recovery more quickly. In one New York study across all surgical patients in multiple hospitals, physicians found that length of stay-reducing measures could save over 10,000 inpatient days for surgical patients, by conservative estimates. 19 Higher estimates found that as many as 25,000 inpatient days were prevented for surgical patients across the health system studied. 19 When costs were accounted for, the study estimated that length of stay interventions saved between 4.2-6.3 million dollars over five years. Additionally, a large study with over 670,000 spine surgery patients found that a 1% increase in length of stay led to a .47% increase in cost. 20 This demonstrates, on a large scale, how important it is to minimize length of stay. When considering the impact that these interventions can have, it becomes clear how important it is for spine surgeons to encourage patients to recover at home as soon as is reasonable and safe. This will help patients to save money, time, and has the potential to help reduce patient burdens on the larger healthcare ecosystem.
Discrepancies in the data may exist as compared to other data sets since we did not propensity score match cohorts. Significant factors, including demographics and comorbidities, could potentially influence the final observed differences in our study. To account for this, we controlled our data analysis based on ASA class, a system used to classify patients’ operative and perioperative risk according to their comorbidities. While the difference in these rates of comorbidities was small, these results showed significant differences between the specialties. The ASA-1 classification, despite being described as “normal, healthy patients” by the ASA, still contains patients with comorbidities. We observed comorbidity disparities in these patients between neurosurgeons and orthopedic surgeons performing spine surgery even in this lower ASA-1 classification. This could be contributing to the differences in outcomes seen in the specialties.
Another weakness of the study is the lack of evaluation of multiple levels operated in each case by not delineating in our analysis the additional spinal level CPT codes (eg, a one-level fusion vs a three-level fusion). Naturally, the number of levels operated affects the complexity of the case, perioperative blood loss, the likelihood of complications, and the potential operative outcome prognosis. McCutcheon et al. already explored the effect of multiple levels on outcomes with no significant difference found between specialties. 2 We believe that the sheer volume of cases explored in this study (150,469 cases) and McCutcheon’s findings are enough to make this lack of data delineation negligible, but further studies should be done to help explore the effect of the number of levels on outcomes.
Given the above, our results should be considered preliminary and indicative of areas for further, more detailed investigation. Future studies should aim for more controlled and granular analyses to provide deeper insights into specialty-specific outcomes in spine surgery.
The authors plan to bring this information to the attention of the American Spine Registry (ASR) and the Neuropoint Alliance Quality Outcomes Database (QOD) Spine Registry. The ASR, a collaborative effort between the American Association of Neurological Surgeons (AANS) and the American Academy of Orthopaedic Surgeons (AAOS), was designed to create a more comprehensive, collaborative effort between specialties to improve patient care and spinal surgery.21-24 The QOD Spine Registry is the United States’ largest spinal registry. 25 The above findings can be used to inform the ASR’s and QOD’s current data collection metrics and benchmarks of potential outcome differences that warrant deeper examination. The ASR and QOD already use similar systems of cervical and lumbar procedure stratification easing the incorporation of our performance measures. This study can also steer future projects led by the ASR and spinal surgeons to improve future clinical outcomes and improve standards of care.
Further, the findings of the study demonstrate the opportunities for continued collaboration between the two specialties to leverage the strengths observed in each field to improve patient care and health systems. Future research should prioritize cross-specialty collaborative investigations into the minutia of operative techniques and the decision-making processes employed by the observed specialties which underpin the marginal differences in operative statistics discovered by this study. Additionally, future studies focusing on minimally clinically significant measures can help to distinguish impactful areas of improvement between specialties. Overall, this research will be useful in driving essential initiatives, like those mentioned above, to foster shared learning and protocol development, particularly focusing on managing comorbidities and the optimization of operations times and transfusion practices. Additionally, this research advocates for the continued development and growth of robust and nuanced standardized data registries containing pertinent surgeon and hospital identifiers to allow for increased granularity and applicability in future studies. By doing so, we can aim to improve patient outcomes, reduce healthcare costs, and set new benchmarks for excellence in spinal surgery.
Conclusion
The NSQIP database was examined to compare preoperative comorbidities and common metrics for successful outcomes in neurological and orthopedic spine. Overall, many operative characteristics and postoperative outcomes were statistically similar in almost all categories in low-acuity patients. However, while statistically significant, clinical significance is unlikely. This finding is further supported by isolating ASA-1 patients, which showed both fewer differences in each group as well as a smaller effect size. This preliminary study lays the groundwork for future collaboration, benchmarking of performance, and exploration in spine surgery across neurosurgery and orthopedics.
Supplemental Material
Supplemental Material - Surgical Specialty Outcome Differences for Major Spinal Procedures in Low-Acuity Patients
Supplemental Material for Surgical Specialty Outcome Differences for Major Spinal Procedures in Low-Acuity Patients by Anthony Price, Christopher File, Alvin LeBlanc, Nathan Fredricks, Rylie Ju, Nathan Pratt, Rishi Lall, and Daniel Jupiter in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.