
Abstract
Study Design
Broad narrative review.
Objectives
Intramedullary spinal cord tumors (IMSCT) are uncommon lesions that can affect any age group or sex. However, numerous IMSCT exist and the clinical course of each tumor varies. The following article addresses the various management options and outcomes in patients with IMSCT.
Methods
An extensive review of the peer-reviewed literature was performed, addressing management options and clinical outcomes of patients with IMSCT.
Results
Early diagnosis and intervention are essential to obtain optimal functional outcome. Each IMSCT have specific imaging characteristics, which help in the clinical decision-making and prognostication. A comprehension of the tumor pathology and the clinical course associated with each tumor can allow for the proper surgical and nonsurgical management of these tumors, and reduce any associated morbidity and mortality. Recent advances in the operative management of such lesions have increased the success rate of tumor removal while minimizing iatrogenic-related trauma to the patient and, in tandem, improving patient outcomes.
Conclusions
Awareness and understanding of IMSCT is imperative to design proper management and obtain optimal patient outcomes. Meticulous operative technique and the use of surgical adjuncts are essential to accomplish proper tumor removal, diminish the risk of recurrence, and preserve neurologic function. Operative management of IMSCT should be individualized and based on tumor type, location, and dimensional extensions. To assist with preoperative and intraoperative decision-making, a general algorithm is provided.
Introduction
The first successful removal of an intramedullary spinal cord tumor (IMSCT) was performed in 1907 by Eiselberg. 1 , 2 A few years later, Elsberg and Beer advocated a two-staged approach for an IMSC tumor removal. The procedure consisted of a posterior midline myelotomy overlying the tumor followed by a nondural closure. 3 A second surgery followed a week later in which the wound was reopened, allowing extrusion of the tumor through the myelotomy. As a result, the treatment of such a tumor as described by Elsberg and Beer had become known as “extrusion of intramedullary tumors.” In 1918, Frazier promoted the efficacy of a one-stage approach and asserted the idea that the encapsulation of these tumors is essential in obtaining suitable morbidity. The diagnosis and treatment of spinal cord tumors was demonstrated by Elsberg in the early 20th century,3,4,5,6 and primarily documented in his 1925 seminal text-based publication that provided the clinical manifestations resulting from such cord lesions.5 The potential for gross proliferation of IMSCT was underlined in 1939 when Horrax and Henderson reported total enucleation of an ependymoma extending the entire length of the spinal cord. 7 The tumor was removed through a series of operations and good recovery was noted with long-term survival.
Intraspinal tumors in children have also been reported but are very uncommon. Between 1910 and 1926, Stookey of the New York Neurologic Institute documented eight cases of intraspinal tumors occurring in children. 8 Similarly, Ingraham noted 16 cases between 1918 to 1938 at the Boston Children's Hospital. 9 In the early 1970s, Banna and Gryspeerdt evaluated the radiologic features of IMSCT in children and noted that the predominant manifestation in 32 patients was scoliosis. 10 In the ensuing years, a handful of clinicians documented their experience with spinal cord tumors in children. 11 , 12 , 13
Although many notable physicians reported their experience with intradural tumors, poor instrumentation and diagnostic equipment hindered proper diagnosis and outcome. High mortality and morbidity rates were often associated with surgical tumor removal. Thus, radiotherapy was implemented as the treatment modality of choice, reserving surgery for diagnosis and cyst aspiration. A half-century progressed until Greenwood heralded a new era in the surgical treatment of intradural tumors by introducing bipolar cautery and the implementation of magnifying loupes, offering safer tumor removal. 14 , 15 , 16 The feasibility of safe tumor removal was greatly facilitated with the introduction of the operating microscope in the 1970s and the implementation of intraoperative motor evoked potential monitoring in the 1990s. The addition of ultrasonography, ultrasonic aspirator, and laser enhanced the surgeon's ability to safely remove tumor. IMSCTs are rare manifestations that escape proper diagnosis and management by many surgeons. Before the advent of magnetic resonance imaging (MRI), computed tomography (CT), and myelography, tumor diagnosis was achieved through bony erosion visualized on plain radiographs providing inaccurate locations of tumors and often misleading diagnosis and inappropriate operative intervention. Diagnostically, MRI enabled significant advances in tumor identification, localization, and characterizations, over the previous modalities of X-rays, myelograms, and CT scans. Nonetheless, despite significant advances in diagnosis and surgical technique and new high-tech gadgetry, IMSC tumor management demands a thorough comprehension of the clinical course and the practice of delicate caution while performing surgical removal.
Operative Treatment
Surgical Adjuncts
The goals of surgery are to obtain tissue diagnosis, obtain maximum tumor removal, and improve neurologic function while maintaining spinal stability. The surgical management of IMSCT has been greatly facilitated by use of the operative microscope; however, ultrasonography, 17 , 18 , 19 , 20 ultrasonic aspiration, 21 , 22 and laser 23 have also been instrumental in defining the tumor, and tailoring the appropriate surgical technique by identifying the tumor glial interface, facilitating debulking of the tumor, and ascertaining the presence of residual tumor.
Since its introduction to neurosurgery in 1982, ultrasonography has been used as a surgical adjunct. Ultrasonography is a noninvasive intraoperative diagnostic device that is typically used before dural opening. Ultrasonography can be helpful in locating the tumor, marking its dimensions, ensuring adequate bony exposure, and demarcating the transition zone between the lesion and the spinal cord. 17 Furthermore, specific tumor components can be characterized through its echogenic characteristics. With this information, a decision on the proper surgical technique can be made, and the feasibility for a gross total resection (GTR) can be determined. 18 , 19 , 20
Performing a proper myelotomy is vital. Because the majority of intramedullary tumors arise dorsally, a posterior midline myelotomy is commonly performed. However, the cord contour is altered from tumor infiltration, and a blind myelotomy may provide inadvertent injury to the dorsal columns and disrupt the posterior vascular supply. Therefore, ultrasonography highlights the cord distortion and provides useful information via transverse and longitudinal cuts to identify the dentate ligaments. In the presence of rostral or caudal cysts, an incision is made from the cyst–tumor junction and extended to the opposite pole. Conversely, if cysts are not present, the incision is performed at the location of the most voluminous region of the tumor provided that the distinction between the cord and tumor is obvious. Ultrasonography is objectively used to limit the incision and thus minimize the spinal instability.
On axial cuts, astrocytomas produce an asymmetrical cord expansion and present with variable echogenicity but with slightly pronounced signal intensity compared with the surrounding cord. Conversely, ependymomas are symmetrical, centrally located, and portray hyperechoic signal characteristics. Cysts are commonly found in irradiated tumors and reveal an asymmetrical shape, variable irregular hyperechogenic walls, septations, and a “Swiss cheese” appearance. Nonirradiated lesions demonstrate larger solitary cysts. Alternatively, cysts not of tumor origin tend to be larger, contain smooth walls with no echogenicity, and expand the canal symmetrically.
Surgical Considerations
The feasibility of tumor resection is dictated by tumor location, pathology, the presence of infiltration of the tumor into the surrounding tissue, and operative exposure. A preoperative assessment via MRI can assist in determining the location, size, and infiltrative and cystic properties of the tumor. However, the final tumor identification is determined by a biopsy.
Astrocytomas are infiltrative nonencapsulated tumors that may present a pseudoencapsulated appearance during surgery. For high-grade astrocytomas, the prognosis is poor and no known cure is available. High-grade astrocytomas are soft, rapidly spreading tumors that can develop intracranial extensions. Separation of these tumors can be challenging. Removal can sometime be augmented by a two-staged approach, similar to Elsberg and Beer's extrusion method. Conversely, low-grade astrocytomas may not be amenable to dissection from the cord unless exploration depicts a pseudocapsule. Nonetheless, prognosis for a low-grade astrocytoma is generally more positive.
Ependymomas are generally benign lesions. They demonstrate distinct encapsulation and possess visible tumor–cord margins (Fig. 1). These tumors are usually curable via GTR. Regardless of the size of the tumor or the features indicating cord compression, total removal should be attempted if the histology indicates benign features. An ample biopsy specimen should be obtained to eliminate erroneous interpretations of the tumor. A tanycytic variant of ependymomas exists that often masks the presence of an ependymoma and should be considered when interpreting the histology. 24 Syrinx activity can mimic an ependymoma, thus demanding a thorough cord–border analysis to dismiss the presence of a tumor. Rarely, high-grade (anaplastic) ependymomas are encountered and have both increased infiltration of the cord parenchyma and a poor prognosis.
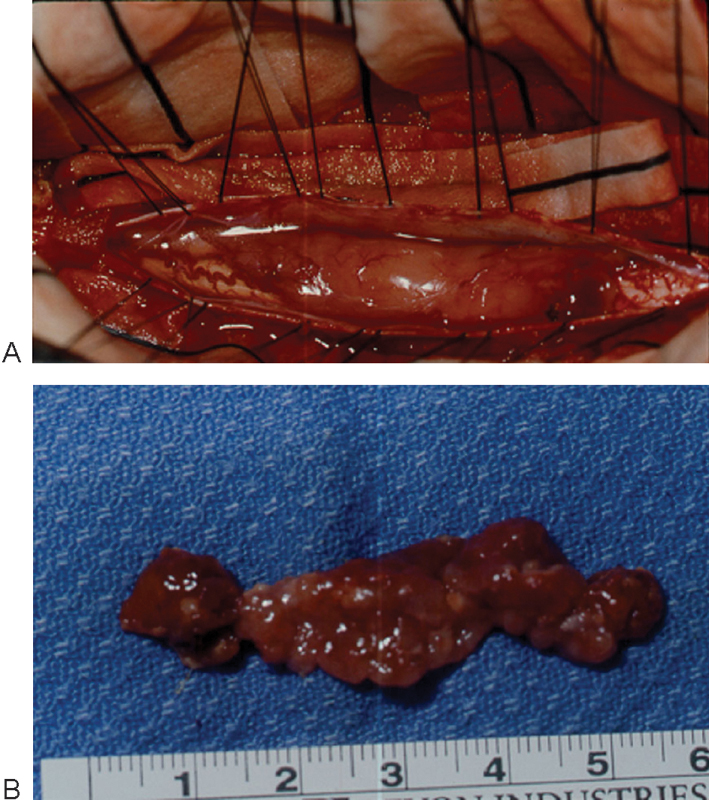
(A) Intraoperative view of cervical intramedullary ependymoma with large extramedullary extension. Tumor also wrapped around spinal cord to occupy the ventral extramedullary space. (B) Pathology specimen demonstrating “red, beefy” appearance of resected intramedullary ependymoma.
Similar to ependymomas, hemangioblastomas, lipomas, and other rare intramedullary tumors are resectable. Hemangioblastomas present a more pronounced vascularity and respond well to circumferential capsular dissection, and they often contain a cystic portion or can appear as a cyst with an enhancing portion. Embolization can facilitate the removal of the tumor in a safe and effective manner. There have been reports describing hemorrhage associated with the embolization procedures performed on hemangioblastomas of the cerebellum, though this phenomenon is not encountered with spinal lesions. 25 Successful embolization of these lesions can help facilitate the ease of removal. 26 Lipomas possess concomitant exophytic masses that lead to tethering of the spinal cord. Lipomas also present a distinctive tumor–cord interface. These masses tightly adhere to neural tissue, possibly because they are congenital and radical removal can contribute to neural damage. 27 Therefore, lipomas do not require total resection. An ultrasonic aspirator may prove beneficial in debulking the tumor and detethering the spinal cord. Because lipomas have high water content, a CO2 laser may be particularly effective is removing the remaining tumor rim.
The metastatic potential of IMSCM tumors is dictated by the presence of malignant features inherent in the primary neoplastic source. The early detection and diagnosis of these tumors is imperative to avoid widespread infiltration. A multidisciplinary approach via radiation, chemotherapy, and surgery is used to treat these tumors. Radiosensitive tumors, such as oat cell carcinoma or lymphomas, have the benefit of longer periods of remission than other tumors when treated with radiotherapy. 28 , 29 However, the benefit from radiotherapy is dubious for most metastatic tumors. Some reports elucidate that even with radiation treatments, 80% of patients become paraplegic or die within 6 months. 27 , 30 , 31 , 32 The therapeutic benefit of steroid therapy combined with radiotherapy also remains uncertain. Because these tumors are encapsulated with some presenting cystic components, surgical removal is possible and recommended if neurologic compromise is apparent. Cord surface migration of the cystic components facilitates their extirpation and avoids deep cord investigation. Nonetheless, improvement of neurologic outcome, function, and quality of life can be accomplished with surgical tumor removal followed by chemotherapy and radiotherapy. 33
Arachnoid scarring is a manifestation attributed to tumor hemorrhage or arachnoid irritation and can be found in recurrent or nonoperated tumors. During surgery, arachnoid scarring complicates safe tumor removal. Astrocytomas are the most common IMSCT presenting with arachnoid scarring. Neurologic function is adversely affected by arachnoid scarring. Furthermore, arachnoid scaring contributes to the postoperative morbidity. 34 , 35 Reports indicate that 25% of patients with arachnoid scarring who undergo surgery develop dysesthesias or pain, which develop in relation to the scarred segment. 36 , 37 To reduce postoperative neurologic deterioration due to arachnoid scarring, Samii and Klekamp recommend lysis of arachnoid adhesions or utilizing a dural graft to decompress the surgical region to maintain patency of the subarachnoid space especially in the presence of highly vascularized tumors. 35
The surgical operation for tumor resection entails a laminectomy and posterior exploration via a durotomy. General anesthesia is used, and the patient is placed in the prone position. Perioperative steroids and preoperative standard prophylactic antibiotics are administered to the patient. The radiographic analysis dictates the planning of the incision. Usually, one level above and below the suspected tumor site is targeted. A subperiosteal dissection is used to remove the muscle, and a laminectomy is performed. Bone wax is placed along the bone edges. Absorbable porcine gelatin mixed with thrombin is placed in the epidural space to limit excessive oozing of blood. Cottonoid strips can be placed in the epidural space to provide additional tamponade. Once a proper exposure is achieved, ultrasonography is performed to determine the tumor margins, the presence of cysts, and the location of the voluminous region of the tumor. An operative microscope is implemented, and somatosensory evoked potentials and motor evoked potentials are monitored. A midline dural incision is then performed in a caudal direction exposing the underlying cord while being cautious not to violate the arachnoid layer or creating unintended vascular injury. Dural retention sutures are then applied to the paraspinal muscles or attached to free-hanging mosquito forceps (Fig. 2). Maintaining hemostasis is of the utmost importance and should be exercised throughout the procedure. An arachnoid knife is then utilized for the delicate myelotomy incision. The posterior median septum and the bilateral entry zones of the dorsal nerve rootlets are referenced to ensure a proper midline incision. The myelotomy should be centered over the most expansive portion of the tumor and extend the length of both tumor poles. Alternatively, the CO2 laser with a setting of 5 to 10 W can be used to accomplish the myelotomy. The multitude of small vessels located on the medial aspect of the posterior columns can also be referenced to direct a proper midline exploration. The small pial vessels can be cauterized, whereas the larger vessels are dissected and retracted laterally from the region of interest. Fine pial sutures are placed to avoid tissue trauma and to provide countertraction.
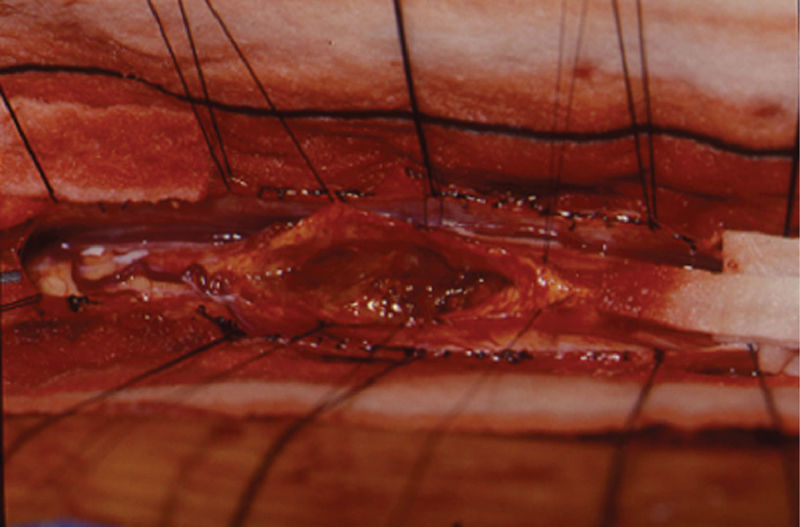
Intraoperative view of resection cavity of cervical ependymoma. Note the pial traction stitches.
Once the tumor is visualized, a portion of the tumor is removed and sent for pathologic evaluation. On visual inspection, if the tumor is not clearly demarcated or if the frozen section reveals an astrocytoma, caution is exercised to prevent unwanted neurologic deficits that may ensue with a complete resection. Delicate spreading of the microforceps or dissectors along the longitudinal axis of the tumor–cord interface may aid in establishing a dissecting plane. In the presence of an ependymoma, cyst formation may appear in either the rostral or caudal poles although they tend to favor the rostral poles. Countertraction with pial sutures may facilitate better visualization of the tumor–cord interface dorsally and laterally. Cauterizing the feeding vessels of the tumor is essential for liberating and removing the tumor. An attempt is made to circumscribe the tumor for resection. However, in the event of a large tumor, the ultrasonic aspirator may be utilized for internal debulking of the abnormal mass and removal via an inside-out approach. However, the internal removal must be minimized to avoid tumor surface fragmentation and obscuration of the dissection plane posing an undesirable piecemeal removal. 38 Ependymomas can also be found in the conus, filum terminale, and cauda equina. In these regions, the neural roots may intersect the tumor, which can prevent total en bloc resection of the tumor. Thus, meticulous dissection of the tumor mass from the neural elements is vital. With astrocytomas, the ultrasonic aspirator is implemented to safely debulk the visibly distinct tumor. This maneuver is followed by the use of the CO2 laser to eradicate residual tumor fragments adjacent to the cord. Hemangioblastomas are commonly found on the dorsolateral or dorsal pial surface and thus do not typically require a myelotomy. 25 ,39,40,41 Because hemangioblastomas are well-encapsulated vascular masses with an array of surface vessels feeding the tumor, resection is possible only after its vascular supply is controlled. A visible cleavage plane can be visualized allowing for the tumor to be circumscribed by cauterizing the capsule. Every attempt should be made to preserve the draining veins. Tumor removal is continued until no defining tumor remnant visibly remains.
After a thorough exploration and isolation/removal of the lateral and dorsal aspects of the tumor, focus shifts to the ventral plane. However, tumor removal from this aspect of the mass is a difficult task. Obtaining an appropriate visual field to discern the tumor–cord interface is hampered by the tumor mass and by difficulty maintaining pial countertraction. Furthermore, the vascular branches from the anterior spinal artery commonly supply the ventral aspect of the tumor, which contributes to the high vascularity of the ventral plane. Thus, careful cauterization should be performed to prevent unwanted bleeding.
After the appropriate tumor removal has been accomplished, the tumor bed is inspected and irrigated, and the pial sutures are removed. A watertight dural closure is then performed. If cerebrospinal fluid (CSF) leakage is still a concern, a dural patch graft or fibrin glue should be applied to prevent leakage and formation of an unwanted pseudomeningocele.
Following dural closure, appropriate spinal column reconstruction and stabilization may be necessary. Aggressive laminectomies should be avoided if possible to minimize spinal column deformity that tends to occur in the cervical and thoracic spine of children. 42 , 43 , 44 , 45 On occasion, a minimally invasive approach may be performed. 46 This approach utilizes tubular retractors to provide exposure. The surgical approach involves a hemilaminectomy and reduces trauma to the posterior tension band, which will theoretically reduce the incidence of postlaminectomy kyphosis. Laminoplasty is an alternative as is a unilateral laminectomy or laminotomy. 47 , 48 In the event of multilevel laminectomies through the cervicothoracic or thoracolumbar junction, lateral mass and pedicle screws are recommended to provide the necessary stability. Segmental instrumentation is applied after the termination of radiation treatment to give the best results. Although a laminectomy provides adequate operative exposure of the spinal cord and facilitates the accessibility of tumor removal for neoplasms located dorsally or dorsolaterally, the feasibility of such an approach may not be suitable for more ventral and ventrolaterally positioned tumors that demand an alternative route of resection other than a posterior approach to minimize cord manipulation and potential injury. 49 , 50 , 51 , 52 , 53
Operative Complications
Microscopic attention to detail in IMSC tumor removal is crucial. The essence of surgical tumor removal is to alleviate the distressing symptoms. If the symptoms persist after surgical tumor resection, arachnoiditis, syringomyelia, tumor recurrence, wound dehiscence, infection, neurologic or vascular compromise, or CSF leakage should be considered. Postoperative CSF leakage with IMSC tumor removal is a common manifestation that demands attention. However, if various perioperative precautions are followed, the frequency of postoperative complications can be minimized.
Prior to surgery, the presence of hydrocephalus must be established because this condition predisposes to postoperative CSF leakage. If hydrocephalus exists, the application of a CSF drain preoperatively is necessary to decrease the CSF pressure. Purposeful dural opening, as in the case of IMSCT, or any dural tear requires a watertight closure and repair to prevent CSF fistula, wound infection, postural headaches, risk of meningitis, formation of pseudomeningocele, and subsequent nerve root entrapment. Proper lighting, adequate hemostasis, and magnifying loupes or microscope provide good visualization of the dura and aid in tear identification. Postoperatively, if a leak is suspected, myelogram and/or radioiodinated serum albumin scans assist in distinguishing between wound drainage serous fluid or CSF fistula. Because glucose is present in both exudates of noninflammatory and inflammatory conditions, the glucose level from fluid drainage is not a reliable diagnostic predictor of postoperative CSF leakage.54 However, an unusually high concentration of glucose confirmed on glucose-oxidase paper is a good indication of a CSF leakage.
If the integrity of the dura is compromised, a pressure differential is created across the dura from the empty thecal sac facilitating accumulation of a postoperative hematoma from the surrounding epidural veins. In the occurrence of CSF leakage, the patient may experience low-pressure posture-related headaches relieved in the supine position but exacerbated when standing upright. Light-headedness, nausea, and sweating can also follow a CSF leak. Furthermore, CSF leakage can prevent proper wound healing and may increase infection. A pseudomeningocele is a fluid-filled pouch of accumulated CSF, which maintains a communication with the subarachnoid space. A thick fibrosed rim is delineated at the dural opening connecting the pouch and subarachnoid space. 55 , 56 Pseudomeningocele has been reported to cause postoperative cord compression and present with a delayed myeloradiculopathy. 55
Fixing a dural leak may require a fascial graft or tissue patch. 7 , 57 Multiple watertight layers should be attempted to eliminate dead space and prevent continued CSF leakage. However, a complete dural closure may be unattainable depending on the surgical approach performed and the location of the dural incision. If posterior decompression is performed, and the dural incision is performed laterally to remove a tumor in the lateral gutter, it may be difficult to achieve a suitable dural closure. Gelfoam or muscle coverage of the leak may not adequately prevent CSF leak. 56 , 58 Fibrin glue can be used to augmented closure in these cases. 59 , 60 Shaffrey et al reported a 94% success rate in closure of 16 patients with no CSF fistula preoperatively and an 80% success rate in closure with an established CSF fistula. 61 Finally, when direct dural closure is not possible, external subarachnoid drainage using a lumbar drain is an excellent adjunct to divert CSF flow from the opening, allowing the orifice to close. 62 Kitchel et al noted the value of external drainage with their report of 14 of 17 patients noting resolution of CSF leakage after 4 days of closed subarachnoid drainage. 63
With accompanying syringomyelia, neurologic deterioration can ensue for days or months postoperatively until functional recovery is noted. Edema or disruption of vascular supply to the spinal cord may result in delayed recovery. However, syrinx regression often develops with complete tumor removal.
A spinal deformity is a common complication of pediatric laminectomy. 43 , 44 , 45 Such a deformity is seen in the cervical and thoracic spine with an incidence of 24 to 100%, 42 , 43 with a reportedly lower occurrence in the lumbar and thoracolumbar spine (0 to 7%). 42 , 43 Spondylolisthesis is another postoperative complication stemming from multilevel laminectomies. 64 , 65 Because facet joints play an essential role in the stability and curvature of the spinal column, it is recommended that facet joints and pars interarticularis be preserved during laminectomy for tumor removal. Furthermore, prolonged follow-up evaluation is recommended for multilevel laminectomies because spinal deformity may manifest as late as 7 years after the surgery was performed. 42 , 66
Operative Outcomes
Many variables determine postoperative outcome. Aggressive tumor removal is commonly sought but is dependent upon the histology, location, and extent of the mass. GTR and subtotal tumor resection can affect the recurrence rate and outcome after surgery. Although certain tumors benefit more than others from radical resection, it is the surgeon's discretion to formulate a plan to achieve a desirable outcome while minimizing the risk of neurologic deficit. Complete tumor removal is the desired goal of any surgery. However, if the tumor–cord interface is poorly demarcated, complete tumor removal may be impossible. The ability to achieve a GTR is dependent on many factors. To date, there is disagreement on what those factors are. Although some may argue that obtaining a GTR is dependent primarily on tumor histology, 67 , 68 others point out that the presence of a tumor plane regardless of tumor histology can better predict whether a GTR is possible. 69
The location and size of the tumor can also affect outcome. A more posteriorly positioned tumor extending over multiple segments demands a more extensive myelotomy and may disrupt the dorsal column tracts. Cervicothoracic and upper thoracic lesions have been found to have less satisfactory postoperative results compared with lesions in other locations. 70 A GTR may be easier obtained with smaller tumors. 69
Acute perioperative decline is not unusual. Approximately 9 to 34% of patients will experience worsening of their neurologic condition during their hospitalization following their surgery. However, 25 to 41% of these patients who are acutely worse will revert back to at least their preoperative condition within 6 months of surgery. 69 , 71 Intraoperative changes in motor evoked potentials and increasing age are two risk factors that contribute to a worsening neurologic condition in the immediate postoperative period. 70 A good outcome following surgery is dependent on the preoperative functional status of the patient before the surgery as well as the tumor burden. 71 , 72 , 73 , 74 , 75 Garcés-Ambrossi et al also suggested that the identification of a tumor plane during surgery may be a positive predictor of the long-term neurologic improvement. 69 Furthermore, patients who have substantial recovery during the hospitalization following surgery are likely to have favorable improvement in their condition long-term.
The resection of intramedullary astrocytomas presents unique challenges. Cooper asserted that astrocytomas possess neuronal elements in their matrix that can mimic the adjacent cord and lead to inappropriate removal of normal tissue. 76 Thus, radical resection of astrocytomas has long been questioned. A higher morbidity is associated with radical resection of astrocytomas in some reports, whereas other reports do not assert such claims. In children, partial resection is more common. Clinical recurrence rates of partially excised astrocytomas is quite low at 18%. 35 Overall, GTR is possible for low-grade and high-grade astrocytomas in 41 to 55% and 9 to 17% of cases, respectively. 77 , 78 , 79 Furthermore, Nakamura et al reported that low-grade astrocytomas have a favorable 5-year survival rate (64%) compared with high-grade astrocytomas (25%). 77 In their study, all the patients who survived at 5 years had a GTR. The benefits of surgery for high-grade astrocytomas remain questionable. Surgery has been shown to worsen the clinical condition of patients with high-grade astrocytomas. 78 Cristante and Herrmann noted that all anaplastic astrocytomas radically or quasiradically resected recurred within 7 to 10 months after surgery. 70
The recurrence rates of ependymomas is dependent upon the extent of tumor removal. 80 , 81 Due to a discrete cleavage plane, ependymomas offer an obvious route for excision, making total resection possible. Modern techniques have facilitated a GTR for ependymomas in 90 to 93% of cases. 77 , 79 With a GTR, the 10-year disease-free survival rate for intramedullary ependymoma is between 80 and 93%. 82 In general, the postoperative tumor recurrence rates have ranged from 0% to as high as 33% for such IMSC lesions 83 , 84 , 85 ; however, such reports vary in terms of the degrees of tumor removal, the use of radiotherapy, and mean follow-up time.
Due to the low incidence of other rare IMSCTs, reports of clinical outcome are scarce and still speculative. The complete excision of hemangioblastomas is possible in 83 to 92% of patients. 78 , 86 Clinical improvement is noted in 70 to 75% with these lesions following surgical intervention. 39 , 86 Lee et al showed a 40 to 70% reduction of tumor size with surgical resection for spinal lipomas. 87 Surgery in these cases is helpful in alleviating pain but does not offer any significant neurologic improvement.
In general, a radical resection for any IMSCT has been correlated with long-term survival. 88 , 89 Furthermore, progression-free survival has been shown to be dependent on tumor histology. 67 , 69 , 90 To date, studies assessing the effects of GTR on progression-free survival yielded mixed results. 67 , 90 A summary of some of the largest reported series in the literature is provided in Table 1.
Summary of surgical resection series for ependymomas and astrocytomas illustrating the largest published series with at least 50 patients or greater
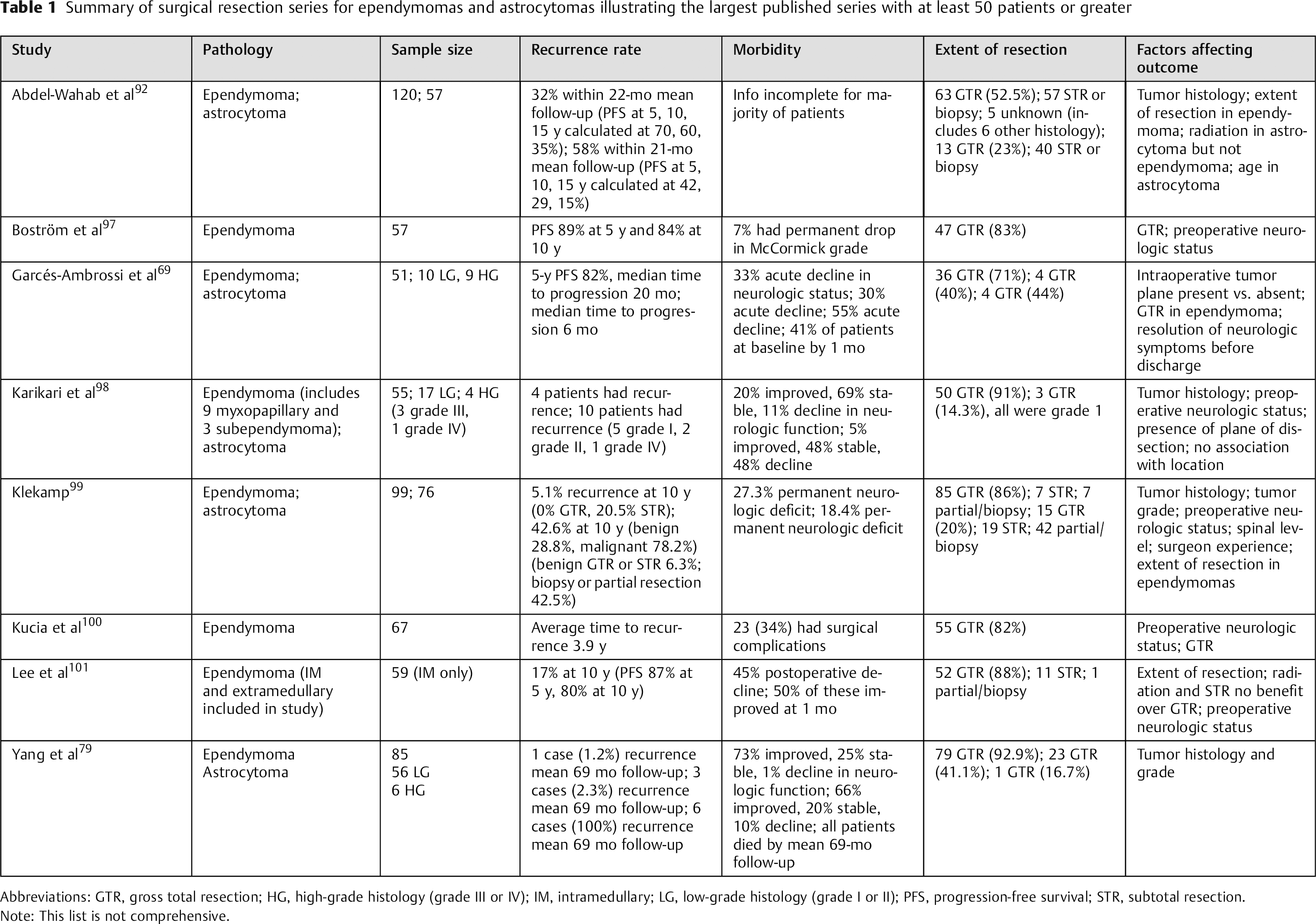
Abbreviations: GTR, gross total resection; HG, high-grade histology (grade III or IV); IM, intramedullary; LG, low-grade histology (grade I or II); PFS, progression-free survival; STR, subtotal resection.
Note: This list is not comprehensive.
Adjuvant therapies are offered to patients with high-grade tumors and subtotal resections and those with progressive disease. Postoperative radiotherapy has been noted to improve the survival in patients with grade II to IV astrocytoma in one retrospective study. 91 Another study suggested that radiotherapy has some benefit on progression-free survival and not overall survival. 92 Although data from Raco et al suggests that adjuvant therapies with temozolomide and radiation lead to improve survival rates, this difference is not statistically significant. 78 Current radiation protocols use fractionated doses of 180 cGy in 28 treatments for low-grade gliomas and 30 treatments for high-grade gliomas. 33 If additional radiation is needed, then tissue-sparing therapies are used such as cyberknife and tomo-radiotherapy. 93 Temozolomide has been used in patients with intramedullary astrocytoma with some promising results. 94 Given the benign course of spinal ependymoma, adjuvant therapies are used less frequently and the role of radiotherapy in the treatment of ependymomas remains speculative. Therefore, it is essential to target complete tumor removal in the case of ependymomas to avoid the incidence of recurrences and complications.
Involved-field external-beam-radiotherapy at doses of 50 to 54 Gy is recommended for malignant subtypes, subtotal resection, or progressive disease. 33 , 95 Etoposide, a topoisomerase 2 inhibitor, has been studied in a prospective fashion for treating spinal ependymomas and showed modest efficacy in controlling the tumor. 96 Thus, adjuvant therapies may provide some added benefits when surgical treatment is limited in controlling the tumor burden.
Reoperation on recurrent tumors that previously have undergone radiotherapy introduces several challenges. First, radiotherapy may cause gliosis that may obscure dissection planes. Also, neural plasticity may be jeopardized, and radiation may prevent proper wound healing as well as affecting the ability and rate for fusion. Patients who usually present with tumor recurrence have a poor prognosis. 80 , 81
Summary
Meticulous operative technique and the use of surgical adjuncts are essential to accomplish proper tumor removal, diminish the risk of recurrence, and preserve neurologic function. We provide a general algorithm to help with preoperative and intraoperative decision making (Fig. 3). The surgical planning is critical in these cases because intradural tumor removal involves purposeful dura incision and often myelotomy. Such an opening increases the risk of complications that require awareness and appropriate management. Operative management of IMSCTs should be individualized and based on tumor type, location, and dimensional extensions.
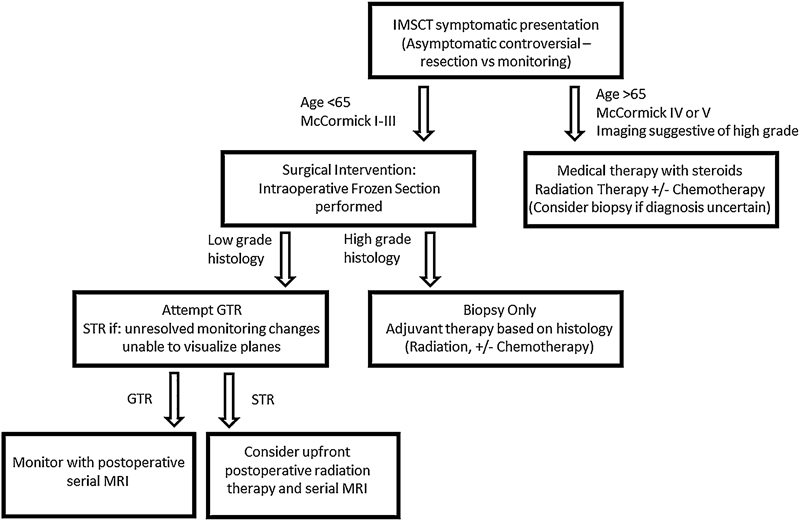
Treatment algorithm for IMSCTs. Abbreviations: GTR, gross total resection; IMSCT, intramedullary spinal cord tumor; MRI, magnetic resonance imaging; STR, subtotal resection.
Disclosures
Dino Samartzis, none
Christopher C Gillis, none
Patrick Shih, none
John E. O'Toole, none
Richard G. Fessler, none
Footnotes
Acknowledgment
We would like to thank the Hong Kong Theme-Based Research Scheme (T12-708/12N) for their support of this work.