
Abstract
Objective
To report clinical characteristics and course of care for patients diagnosed with hematogenous spinal osteomyelitis (HVO).
Methods
Medical records of patients presenting to two tertiary care centers with HVO were reviewed.
Results
96 consecutive patients with HVO were identified. Mean follow-up was 8.9 months. Most infections occurred in the lumbar region (50.0%). Of the cultures taken, MRSA accounted for 9%; MSSA, 26%; Streptococcus species, 12%; other gram-positive bacteria, 23%; gram-negative, 17%; fungal, 2.6%; and 11.5% of cultures returned no growth. 57 patients underwent surgery. Of these
Conclusions
Diabetes, hypertension, and renal failure appear to increase the risk of post-infection sequelae and death. While non-operative management was attempted in nearly 47%, ultimately 73% had surgery. This high rate may reflect our population of patients hospitalized in a tertiary care center. Available data suggests that patients presenting with hematogenous osteomyelitis be followed closely as failure of non-operative management, and resulting morbidity, was high.
Introduction
Spinal infections in adults occur in the wake of invasive procedures, wherein flora have been directly inoculated into the spine and its surrounding soft tissues of via hematogenous spread. Hematogenous vertebral osteomyelitis (HVO), also called spontaneous or native osteomyelitis, on the other hand, results from bacterial spread from a distant site and accounts for approximately 20% of osteomyelitis in adults. 1 These infections can involve several vertebral and perivertebral tissues, including the vertebrae, discs, facets and epidural space. However, spondylodiscitis, involvement of an intervertebral disc and the adjacent vertebral bodies, is the most common form. 2 HVO is often diagnosed in the setting of persistent neck or back pain that is unresponsive to conservative measures, in addition to elevated inflammatory markers, with or without signs of fever. Patients with HVO often have underlying medical conditions or recent surgery, and due its varied clinical presentation, HVO may initially be misdiagnosed as a symptom of a comorbidity or mismanaged as a degenerative process.3,4 Among all pathogens, Staphylococcus aureus is the most common cause of HVO, and usually a course of antibiotics with or without brace management is first-line treatment. 5 Early surgery is recommended in patients with neurological compromise, typically from epidural abscess, or mechanical spinal instability.3,6,7 The type and duration of antibiotic management is determined after culture confirmation and host characteristics such as age, diabetes, or other immunocompromised state. Although controlled trials are still lacking, a treatment duration of up to 6 weeks of antibiotics is generally recommended, with longer courses recommended for those with more complicated infections. 8 An example of an antibiotic regimen for gram positive bacteria such as S. Aureus, the most common cause of hematogenous vertebral osteomyelitis, include intravenous methicillin derivatives or vancomycin for several weeks followed by oral antibiotics for several months after. 9 Gram negative bacteria, such as E. Coli, on the other hand are oftentimes common in elderly patients or those with urinary tract infections, where treatment typically includes a similar duration period as gram positives but with a more sensitive regimen of antibiotics such as fluoroquinolones. 10 That being said, antibiotic treatment still fails in 29% of patients with typical vertebral spondylodiscitis.7,11
In earlier reports, HVO was considered a rare entity and surgical management was discouraged. 12 Over time, with our aging and increasingly immunocompromised population, studies have increasingly reported the role of surgical intervention in HVO patients.2,5,12-15 This study aims to understand the clinical characteristics and course of care for patients diagnosed with hematogenous spinal osteomyelitis.
Materials and Methods
We retrospectively examined the records of 96 patients who were diagnosed with hematogenous vertebral osteomyelitis from two tertiary care centers from January 2014 to January 2021 by reviewing all the patient charts which included ICD-10 codes between M46.20 to M46.59. This captured all the infective conditions of the spine that were of interest. Patients’ electronic medical records (EMR) were examined across multiple EMR platforms to collect demographics, comorbidities, presenting symptoms, antibiotic usage, type of treatment, length of stay (LOS), re-operations, re-admissions, micro-biological information, morbidity, and mortality. Long-term antibiotic use was defined as courses lasting longer than six months. This classification was based on surgeons's clinical experience in treating this patient population as the duration of therapy remains empiric. This is because there are no clinical studies or documented records indicating the superiority of the 4-6-week course of antibiotics over other durations.16,17 The changes in neurologic status were determined by comparing pre-treatment physical examinations to post-treatment physical examinations. Radiographic imaging (CT and MRI scans) results were utilized to determine the location and extent of disease.
We included patients with a diagnosis of hematogenous vertebral osteomyelitis, discitis, and spinal epidural abscess over 18 years of age as determined by radiographic imaging, operative diagnoses, and/or biopsies. Patients with a history of spinal surgery within the last six months were excluded. The mean follow-up was 8.9 months (range 0-48 months). Comorbidities, such as hypertension, diabetes, etc. were recorded. Antibiotic duration was determined through examination of infectious disease plans-of-care, medication records, and discharge summaries. Neurologic outcome was determined by review of documented physical exams at both the tertiary care centers and outpatient clinics. Motor and sensory weaknesses were defined by the American Spinal Injury Association grading system (ASIA). 18 Surgery as first-line treatment was defined as receiving seven days or less of antibiotics before operative treatment was utilized. The goals of surgery included neural element decompression, axial skeleton stabilization, and systematic debridement of the involved tissues. The causative organism was identified by blood and/or intraoperative cultures. Patient data was analyzed through Microsoft Excel to determine quantitative results through basic descriptive statistics such as sum, average, count etc. The study was approved by the Institutional Review Board (STUDY00000922-CR01). The study was exempt from consent. The PubMed database was used to generate tables to compare our results vs other studies recently published at the time of the collection of the data in this study in 2021, which was not performed as a systematic review. Our search strategy focused on the combinations of key terms: “vertebral osteomyelitis”, “hematogenous spinal osteomyelitis”, “spontaneous/native osteomyelitis”, “complications”, “infection”, “mortality”, “spinal surgery”, “microbiology”, “outcome”
Results
Overview of patient demographics.
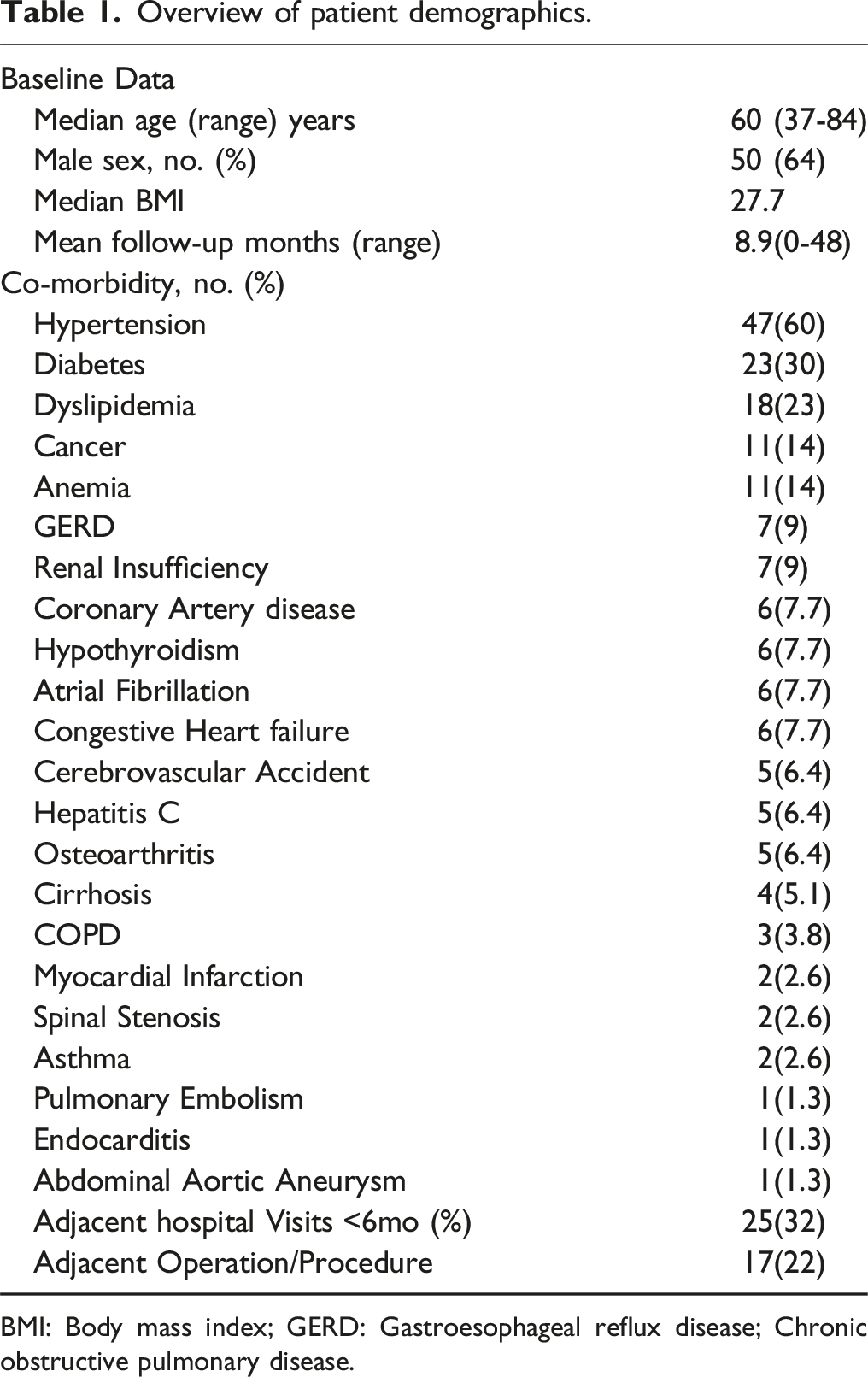
BMI: Body mass index; GERD: Gastroesophageal reflux disease; Chronic obstructive pulmonary disease.
Treatment duration, diagnostics performed, bacterial etiology, outcomes, post-infective sequelae, and clinical outcomes in patients with native vertebral osteomyelitis.
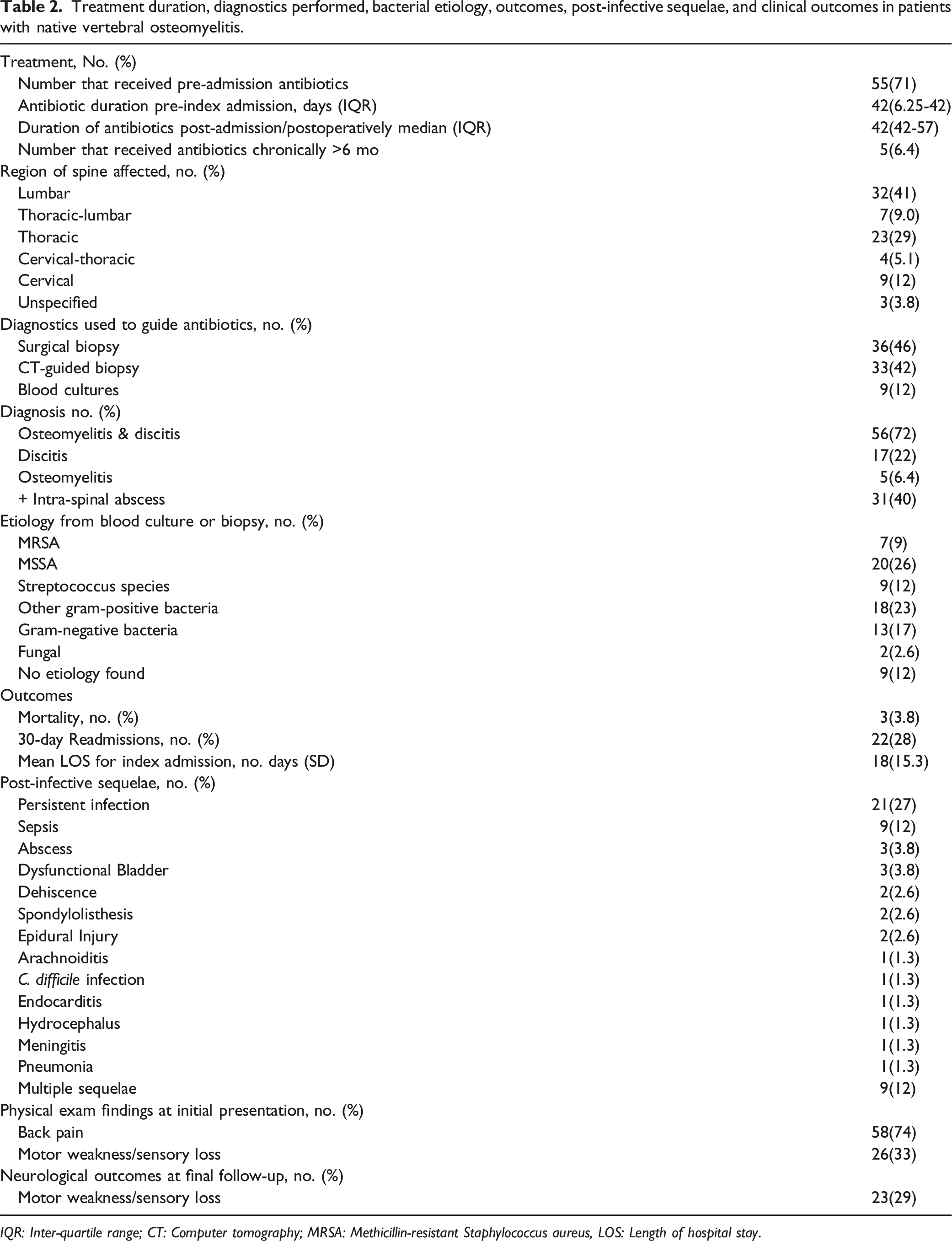
IQR: Inter-quartile range; CT: Computer tomography; MRSA: Methicillin-resistant Staphylococcus aureus, LOS: Length of hospital stay.
Major post-infection sequelae occurred in 37 (47.4%) patients (Table 2). Patients suffering sequelae had a mean age of 69.3 years, were mostly male 31 (84%) and carried major comorbidities including diabetes, anemia, hypertension, and renal disease. The most common sequelae were persistent infection: 21 (27%), sepsis: 9 (12%), and abscess: 3 (3.8%). 9 (12%) patients had multiple sequelae. 26 (33%) patients demonstrated motor weakness and/or sensory loss at initial presentation, while 23 (29%) demonstrated motor weakness and/or sensory loss at final follow-up. Of the 26 patients who initially presented with motor weakness and/or sensory loss at initial presentation 15 (58%) regained full strength and sensation after treatment, whereas 11 (42%) reported no improvement or worsening symptoms. Of the 52 who reported no neurologic symptoms at initial presentation, 11 (21%) reported new or worsening symptoms. Culture from biopsy was positive in 69 (88%) samples taken. Of the cultures used to guide antibiotics, 36 (46%) were from biopsies taken during surgery, 33 (42%) were taken from CT-guided biopsies, and 9 (12%) were gathered from blood cultures. Gram-positive bacteria were the most prevalent bacteria at 54 (69%), followed by gram-negative at 13 (17%), no etiology found at 9 (12%), and fungal at 2 (2.6%, Table 2).
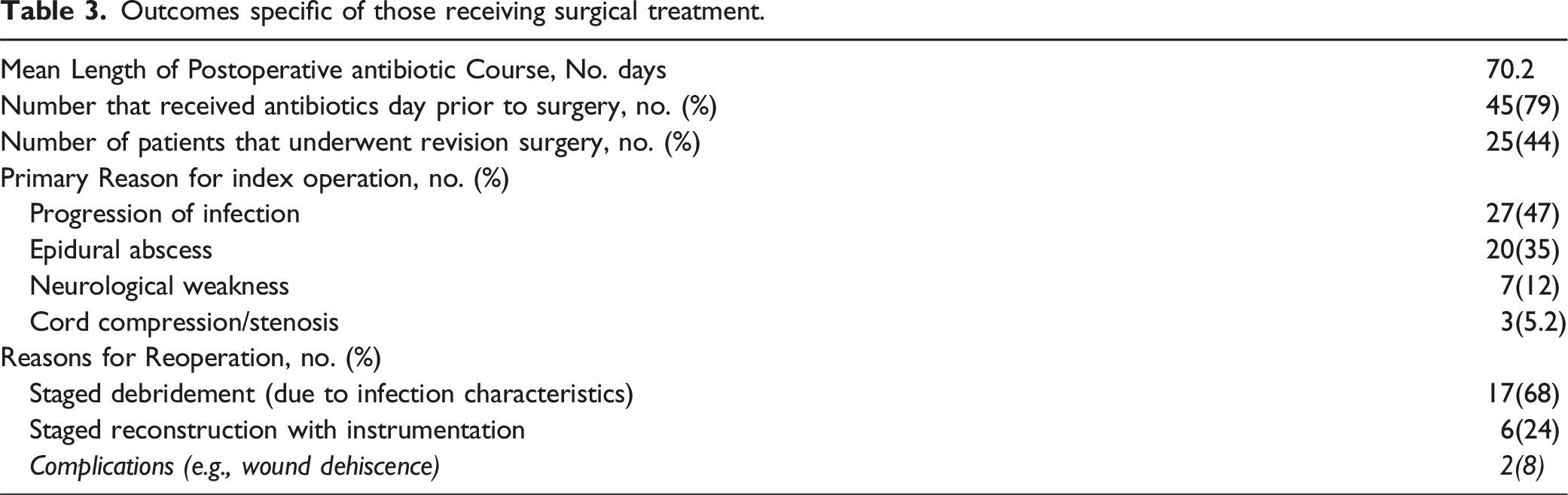
Outcomes specific of those receiving surgical treatment.
Discussion
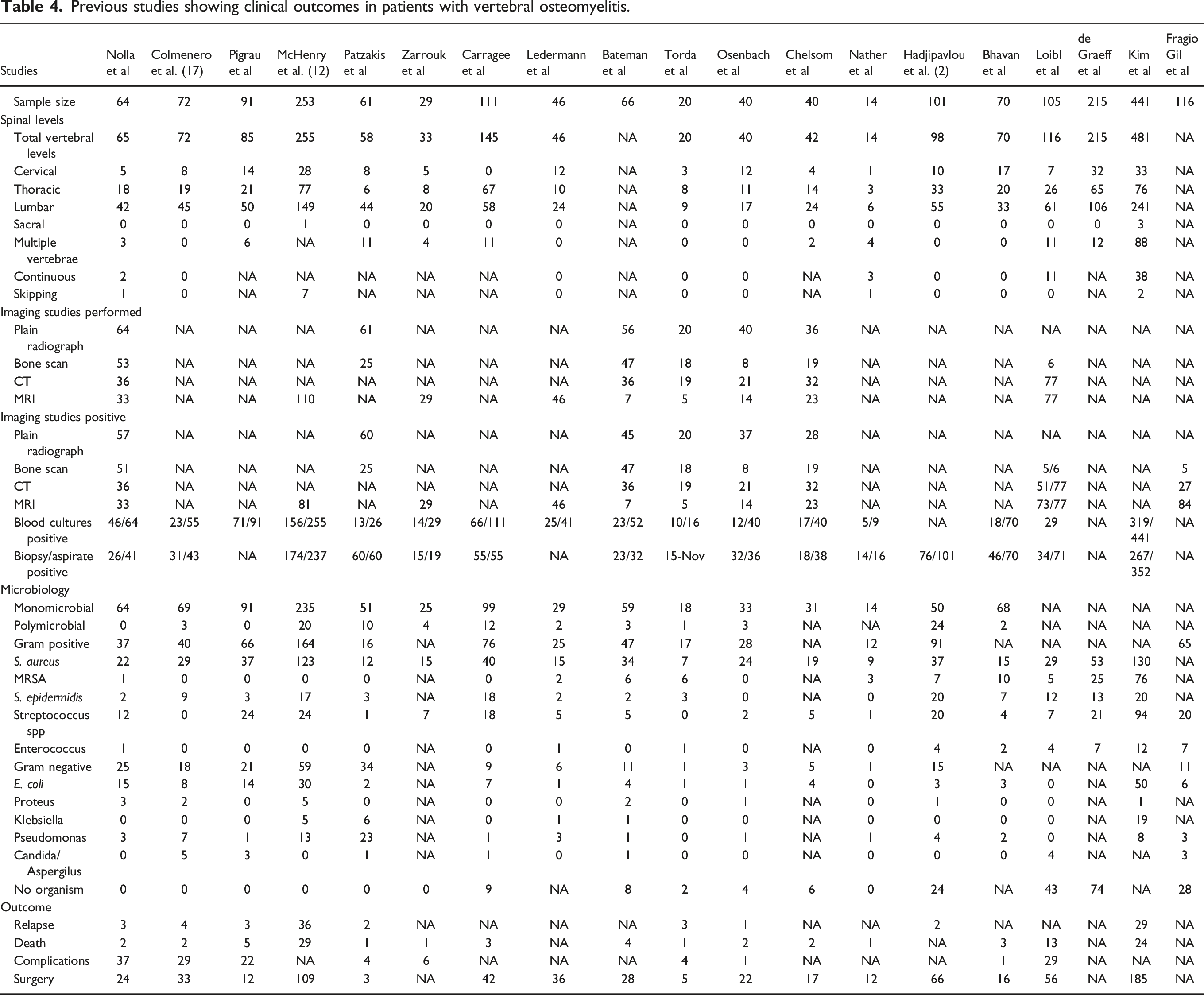
Previous studies showing clinical outcomes in patients with vertebral osteomyelitis.
Consistent with previous reports, HVO affected men more than women and was more likely in those with underlying medical conditions such as diabetes and malignancy. 9
Fragio Gil et al, demonstrated similar rates of comorbidities: hypertension (53%) and diabetes (22%) in their prospective cohort of HVO patients. 13 Our cohort demonstrated a high rate (23%) of dyslipidemia in our patients with HVO. This has not previously been reported.
This study is limited by its retrospective nature and length of follow up data. Additionally, subject inclusion required accurate ICD code documentation and is subjected to inherent bias based on accuracy of coding data. Complete documentation of diagnostic modalities, microbiology and treatment strategies tended to be available in those patients in whom spine surgery consultation had been ordered. This is likely to bias the results toward a sicker subset of patients with HVO as was the fact that many patients had been transferred into our tertiary care centers from outside hospitals. Thus, the generalizability of our conclusions may be limited to similar referral centers.
Our key points, however, are that a majority, 57 (73%) of patients underwent surgery. A trial of non-operative care e.g., antibiotics for >7 days was attempted primarily in 37 (47%) of the 78 patients. In 31 others, early surgery (defined as cases within the first week of receiving antibiotics) was performed, typically for epidural abscess or cord compression. Of those initially managed non-operatively, 26 (33%) ultimately had surgery due to either progression of the infection or neurological decline. The overall surgery rate is higher than previously some published studies reporting 23-58%, though we included both early and late surgery.2,5 Further, the overall trend in recent reports is for a higher rate of surgical intervention [see Table 4]. Nather and Ledermann, for example, report higher rates at 85.7 and 78.2%, respectively.19,20 These findings likely result from our follow-up period and the sicker nature of our patients. Antibiotic administration varied by duration and type according to the care provider, though all were prescribed by fellowship trained infectious disease specialists.
Of the patients included, 26 (33%) had weakness or sensory loss, consistent with previously published papers reporting between 5-40%.15,21-24 These findings, on the higher end of the reported spectrum, may be an artifact of the tolerant inclusion criteria that we used to classify this study variable, which was defined by a physical exam of motor and sensory grades in accordance with the ASIA classification system. 18 This finding may also have contributed to a higher than average rate of surgical intervention.
In our study, the lumbar region was affected most frequently; studies on both hematogenous spinal osteomyelitis (HSO) and pyogenic vertebral osteomyelitis (PVO) have noted this segment of the spine is affected near 55-58%14,22 of the time. The thoracic region was affected more often 30 (38%) in our study than a contemporary large study of HSO patients by Kim et al which demonstrated 17%. 22
The infecting organism(s) were identified in percutaneous biopsy in 68 (87%) patients, higher than previous reports ranging from 43-78%.14,25 Reasons for non-diagnostic biopsies may be secondary to poor sampling, antibiotic administration prior to biopsy, or the resolution of the infection. Current guidelines on antibiotic treatment for bacterial HSO recommends six weeks of parenteral or highly bioavailable antibiotic therapy and surgical treatment for progressive cases. 9 Moreover, the guidelines direct clinicians to focus empiric treatment on staphylococci, MRSA, streptococcus and gram-negative bacilli. 9 Our microbiologic results were consistent with these recommendations; however, we noted an increased percentage of MRSA at 9% in our patient sample as compared to the literature that demonstrated an average of 3%. 14 This may be due to increasing antibiotic resistance or caring for sicker, chronically hospitalized patients.26,27 The management of uncommon and resistant pathogens, such as MRSA, in the setting of orthopedics has been the subject of recent research and clinical recommendations. Primarily the use of local antibiotics such as vancomycin and gentamicin have been found to be effective in the management of orthopedic infections caused by MRSA.28,29 Other novel antibiotics such as ceftaroline, dalbavancin, and tedizolid have shown promising results in some clinical trials and may provide effective treatment options if resistant to first line antibiotics. 30
Our mortality recorded was 3 (3.8%), which is on the lower side of the 3-10% reported in the existing literature.14,22,23,31 These deaths occurred secondary to a gram-positive infection. From our data, it appears that comorbid conditions may contribute significantly to the mortality risk as all 3 patients were being treated for end stage renal disease. All 3 of these patients acquired bacteremia and were treated with multiple operations for their infection prior to their death. 2 of these patients were treated operatively after 40 days of antibiotic management. It has been previously reported that patients with surgical delays are more likely to have higher mortality rates, develop complications, and have a greater length of stay. 32 Further studies are needed to investigate whether earlier operative intervention may be key in preventing such outcomes.
This study represents one of the larger clinical series of its kind which investigates the relationship between risk factors, duration of antibiotic usage and clinical outcomes in patients with hematogenous spinal osteomyelitis. Additionally, long-term outcomes remain unclear as a large percentage of patient were lost to follow-up.
Conclusion
Risk factors such as being a male or having chronic diseases such as diabetes, hypertension, dyslipidemia, or a history of malignancy increase the likelihood of HVO and related complications. As the level of antibiotic resistance increases in MRSA and other lesser common pathogen, it will be critical to utilize proper antibiotic stewardship as well as develop novel antibiotic regimens in order to lessen the rates and complications of HVO moving forward. Likewise, the consideration of early operative intervention is important to understand in order to prevent higher mortality rates, more complications, and greater length of stays in the hospital.
Our data demonstrates that HVO remains a serious disease, with a high rate of early surgery due to symptomatic compression of the neural elements, failed non-operative care, and morbidity. These data suggest that most, if not all, patients with HVO should be evaluated and followed by a spine surgeon. That assessment should include a detailed history and exam along with both advanced imaging and weight-bearing radiographs (when able). All reasonable attempts, from blood culture to percutaneous and open biopsy, should be made to identify the causative organism. However, an in-depth understanding of the host’s vulnerability is also critical. In follow-up, persistence of elevated inflammatory markers, antibiotic resistant or multiple organism infections, mechanical collapse, persistent pain and neurological decline should warrant consideration of operative intervention. Close partnership between the infectious disease and spine surgical teams may optimize outcomes and reduce long term morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.