
Abstract
Study Design
A retrospective study.
Objectives
To investigate and compare the clinical and radiographical outcomes of endoscopic decompression alone and limited decompression/fusion surgery in the treatment of adult degenerative scoliosis (ADS).
Methods
Follow-up data of 53 patients with lower limb radiculopathy associated with ADS who underwent focal surgical treatment were collected (endoscope group: 31 patients treated by transforaminal endoscopic decompression alone; fusion group: 22 patients who underwent limited decompression/fusion). The following data were retrospectively analyzed and compared between the two group: the demographics, Lenke-Silva level, radiographic parameters, surgical data, visual analogue scale (VAS) for back/leg pain, the Oswestry disability index (ODI), and the modified MacNab criteria.
Results
The mean follow-up period was 15.68 ± 3.26 months. The most frequent Lenke-Silva level was I in the endoscope group, and III in the fusion group. Preoperative Cobb angle in the endoscope group was significantly lower than that in the fusion group (23.92 ± 9.06 vs 39.58 ± 13.12, P < 0.05). All patients exhibited improved VAS and ODI scores postoperatively (P < 0.05). At the last follow-up, the Cobb angle had progressed by 1.51° in the endoscope group, whereas radiographic parameters were significantly improved in the fusion group. The reoperation and complication rate in the endoscope group were lower than those in the fusion group. The satisfaction rate post-surgery was comparable between the two groups.
Conclusions
For patients with focal ADS, both limited decompression/fusion and transforaminal endoscopic decompression are viable treatment options. Advanced transforaminal endoscopic techniques enable effective decompression of the symptomatic foramen with minimal complication risk and negligible deformity progression, even in cases of significant scoliosis. While limited fusion surgery can achieve comparable clinical outcomes, it offers inferior deformity correction.
Keywords
Introduction
Adult degenerative scoliosis (ADS) is a 3-dimensional spinal deformity associated with skeletal maturation in which the scoliotic Cobb angle on the coronal plane is greater than 10°.1,2 The prevalence of ADS ranges from 1.5% to 32%,3-5 and the incidence of condition increases with age. Patients aged over 60 years approximately account for 15% of all the cases. 4 In recent years, ADS has become a major medical issue affecting the aging population necessitating the search for effective interventions to improve the quality of life of infected patients. 6 The lumbar spine is the typical location for the major curve in ADS, with a scoliotic Cobb angle ranging from 10° to 20°, 2 and less than 16% of cases have a curve larger than 30°. 7 A curve exceeding 30° may continued to develope rapidly because the apical vertebra has a higher degree of olisthesis and rotation.1,6 Furthermore, the uneven spinal stress caused by the asymmetrical degeneration of disk and facet joints not only increases the risk of high curve progression,6,8 but induces significant spinal stenosis at the fractional curve or the concave side of the major curve. 9 Patients tend to tolerate coronal deformity better than sagittal deformity due to lower associated energy expenditure.9,10 Consequently, they often present with symptoms of radicular pain or neurogenic claudication rather than disabling back pain as the primary reason for seeking medical intervention. 9
The suitable indicators for the optimal treatment of ADS have not been identified. In the absence of overt neurological decline, initial management often involves conservative measures. These typically include nonsteroidal anti-inflammatory drugs, muscle relaxants, and a structured exercise program emphasizing core strengthening and postural correction.11,12 However, although no randomized study has analyzed the specific nonoperative interventions, available evidence suggests that conservative measures are largely ineffective in improving outcomes in spinal deformity patients in terms of back pain, leg pain, and overall quality of life.12,13 Surgical intervention should be considered as a final resort after the failure of conservative treatments. 1 The decision to operate should be based on the patient’s specific deformity, clinical symptoms, and overall medical condition. While corrective surgery has demonstrated promising clinical and radiological outcomes,14,15 the increasing elderly population has highlighted the importance of managing perioperative medical complications in this patient group. 6
A focal approach to treating ADS patients with stenosis is gaining acceptance, 16 particularly when symptoms arise primarily from the focal pathology rather than the overall deformity. Several studies have reported positive clinical outcomes following limited decompression and fusion, 17 laminectomy decompression alone,18,19 and lamina fenestration decompression.18,20 However, complications, such as adjacent segment disease, iatrogenic instability, and deformity progression, cannot be completely avoided. 21 If the focal decompression is performed at the concave side of the main scoliotic curvature and/or the fractional lumbar curve, the deformity may worsen.22,23 In cases where the focal pathology occurs in a relatively larger deformity, minimally invasive techniques, such as oblique- or lateral-approach interbody fusion with percutaneous instrumentation, or a percutaneous transforaminal endoscopic decompression alone with preservation of posterior stabilizers and contralateral facet joint, may sufficiently prevent the worsening of the deformity by minimizing collateral tissue damage.24-27
To date, few comprehensive studies have evaluated the clinical and radiological outcomes of minimally invasive or limited surgical interventions for ADS with concomitant spinal stenosis. This study aims to compare the clinical and radiological outcomes of endoscopic decompression alone and limited decompression/fusion surgery in treating ADS patients with stenosis. Additionally, we will analyze patient characteristics and identify potential differences in outcomes between the two groups.
Methods
Patient Information
This single-center, retrospective study is approved by the Institutional Review Board of our hospital (IIT2023-019-002). All patients provided written informed consent. Between January 2018 and January 2021, the data of patients with a diagnosis of ADS related to lower limb radiculopathy and underwent surgical intervention in our department were reviewed. The diagnosis included comprehensive examination of medical history, pain referral pattern, compatible imaging findings, and positive physical signs. All patients were irresponsive to previous standardized conservative treatment, including physical therapy and oral anti-inflammatory analgesics. The surgical strategy adopted was based on the Lenke-Silva levels, a clinical and radiographical decision-making matrix. 2 The inclusion criteria included: (1) ADS with associated unilateral/bilateral lower limb radiculopathy; (2) patient aged over 40 years; (3) patients who underwent a percutaneous transforaminal endoscopic decompression alone, or a limited decompression/fusion surgery without intended deformity correction; (4) patients with no history of spinal surgery; (5) patients who underwent a follow-up of more than 12 months; (6) patients with complete follow-up data. The exclusion criteria included: (1) other types of scoliosis; (2) patients with evidence of an infectious or neoplastic disease. The recruited patients who underwent transforaminal endoscopic decompression alone were allocated to the endoscope group, while those who received limited decompression/fusion surgery were assigned to the fusion group. The collected surgical data included the number of decompressed segments, the operation time, the intraoperative blood loss, the surgical complications, the adverse events, and the reoperations.
Radiographical Evaluation
Pre- and postoperative (before discharge, six months post-surgery, and at the final follow-up) full-length, weight-bearing standing radiographs of the spine were retrieved from our institution’s picture archiving and communication system (PACS). These images were subsequently imported into Surgimap software, version 2.3 (Nemaris, New York) for precise measurement. The following items were collected and compared between the two groups: (1) the preoperative Lenke-Silva level, (2) the scoliotic Cobb angle, (3) the coronal balance distance (CBD): the interval between the C7 plumb line (C7PL) and the central sacral vertical line (CSVL), was used for coronal balance assessment, (4) the spinopelvic parameters: pelvic incidence (PI), lumbar lordosis (LL), and pelvic tilt (PT), and (5) the sagittal vertical axis (SVA). Coronal and sagittal plane imbalance was defined by a CBD exceeding 3 cm and a SVA deviation greater than 4 cm, respectively.
Surgical Intervention
Prior to surgery, patients in the endoscopic group underwent a selective spinal nerve root provocative pain test to identify the affected level. All patients received percutaneous endoscopic transforaminal decompression under local anesthesia. A precise and sufficient foraminoplasty was performed to facilitate decompression. An endoscopic trephine was employed to partially resect the superior articular process during the initial foraminalplasty; an endoscopic high-speed electric burr or a chisel would be more efficient to remove the hypertrophic and sclerotic bone. After enlarging the manipulating window, the dorsal side of the nerve root was decompressed by removing the hypertrophic ligamentum flavum with a Kerrison rongeur or a nucleus forceps. The herniated intervertebral disk can be first debulked to enlarge the working space during decompressing the ventral side of the nerve root, the osteophytes on the posterior wall of the vertebra and hypertrophic posterior longitudinal ligament were subsequently removed with a burr or a rongeur. After decompression, the perineural scars were removed with forceps, and the nerve root could be observed to freely move and pulse with the heartbeat. Patients were encouraged to mobilize as soon as possible postoperatively. A passive lumbar brace was prescribed for daytime use for approximately six weeks. Routine postoperative pain medication was generally not required. Patients experiencing postoperative numbness in the affected limb received neurotrophic drugs (e.g., cobamamide), while those with osteoporosis were treated with anti-osteoporotic medications (e.g., alendronate or teriparatide). Initial isometric and coordination exercises were supervised, followed by a self-directed home exercise program. The level of exercise can be increased depending on the pathology and the patient’s subjective sense of comfortableness. Limitations were imposed only to the extent that there should be no signs of increased pain during any activity. Patient were discharged after brief hospitalization. For patients who had adequate home care, outpatient program was advised.
Patients in the fusion group underwent general anesthesia for a limited instrumentation, decompression, and fusion procedure without intentional deformity correction. Interbody fusion was performed using either a posterior, transforaminal, or oblique approach. For the oblique fusion technique, posterior decompression was omitted when sufficient intervertebral space was restored. All instrumentation was placed posteriorly with the aid of a Tianji surgical robot (Tianji, Tinavi, Beijing). Cortical bone trajectory with midline interbody fusion was applied under osteoporotic condition. The postsurgical treatment regimen in this group was more restrictive than that in the endoscope group. Early ambulation was encouraged, typically initiated on the first postoperative day. Deep vein thrombosis prophylaxis included compression stockings and low-molecular-weight heparin, initiated one day after drain removal. Patients were required to wear a rigid brace for at least 12 weeks postoperatively.
Clinical Outcome Evaluation
Clinical outcomes were measured using the visual analogue scale (VAS) and Oswestry Disability Index (ODI) at preoperative, before discharge, postoperative 3 months, postoperative 6 months, and the final follow-up (at least 12 months after the surgery). The modified MacNab criteria were used to evaluate patient opinion of treatment satisfaction at the final follow-up.
Statistical Analysis
All data were statistically analyzed using SPSS software (version 25, SPSS Inc, Chicago, Illinois). Continuous variables were described by means and standard deviations, whereas categorical variables were described by frequencies and percentages. Categorical variables were assessed using the Chi-square test and Fisher’s exact test. Student’s t-test was used to compare continuous variables between groups at each follow-up. A paired-sample t-test was used to analyze the within-group variations in clinical outcomes and radiographical parameters during follow-up. A P < 0.05 was considered statistically significant.
Results
Patient Characteristics
Comparison of Demographics Between the Two Groups (n = 53).
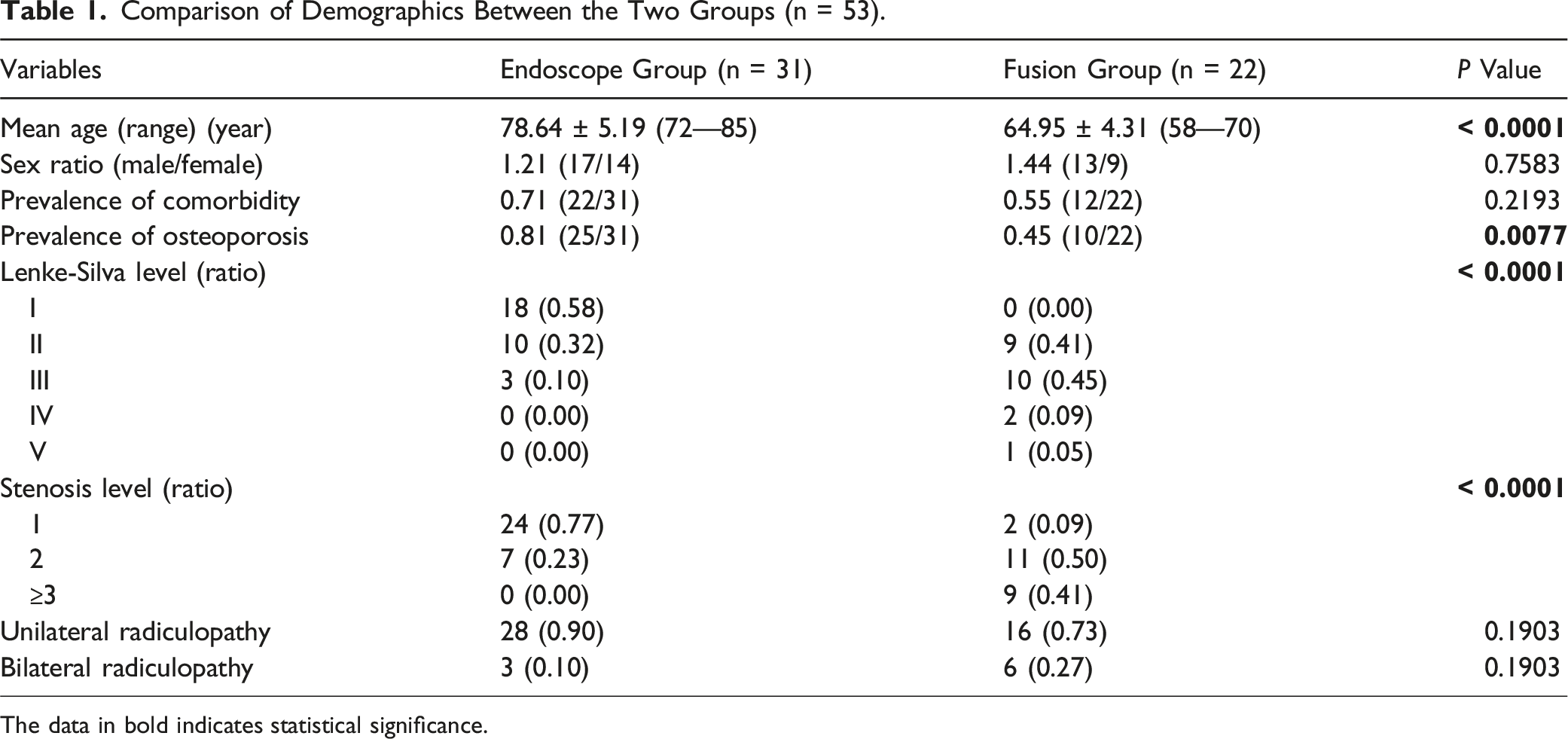
The data in bold indicates statistical significance.
Radiographical Outcomes
As shown in Figure 1a, the preoperative Cobb angle of the endoscope group was significantly lower than that of the fusion group (23.92° ± 9.06° vs 39.58° ± 13.12°, P < 0.0001). The endoscopic group demonstrated no significant progression of the Cobb angle during the follow-up period. Comparisons between preoperative and final follow-up Cobb angles revealed no statistically significant differences (23.92° ± 9.06° vs 25.43° ± 7.60°, P = 0.4799). The final Cobb angle of the fusion group was significantly decreased compared to the preoperative value (17.61° ± 7.07° vs 39.58° ± 13.12°, P < 0.0001). Within- and between-group comparisons of the Cobb angle (a), coronal and sagittal plane balance parameters (b, c) at each follow-up; **** indicates a P < 0.0001; “a” indicates a P < 0.05 for values at each follow-up compared with the preoperative values.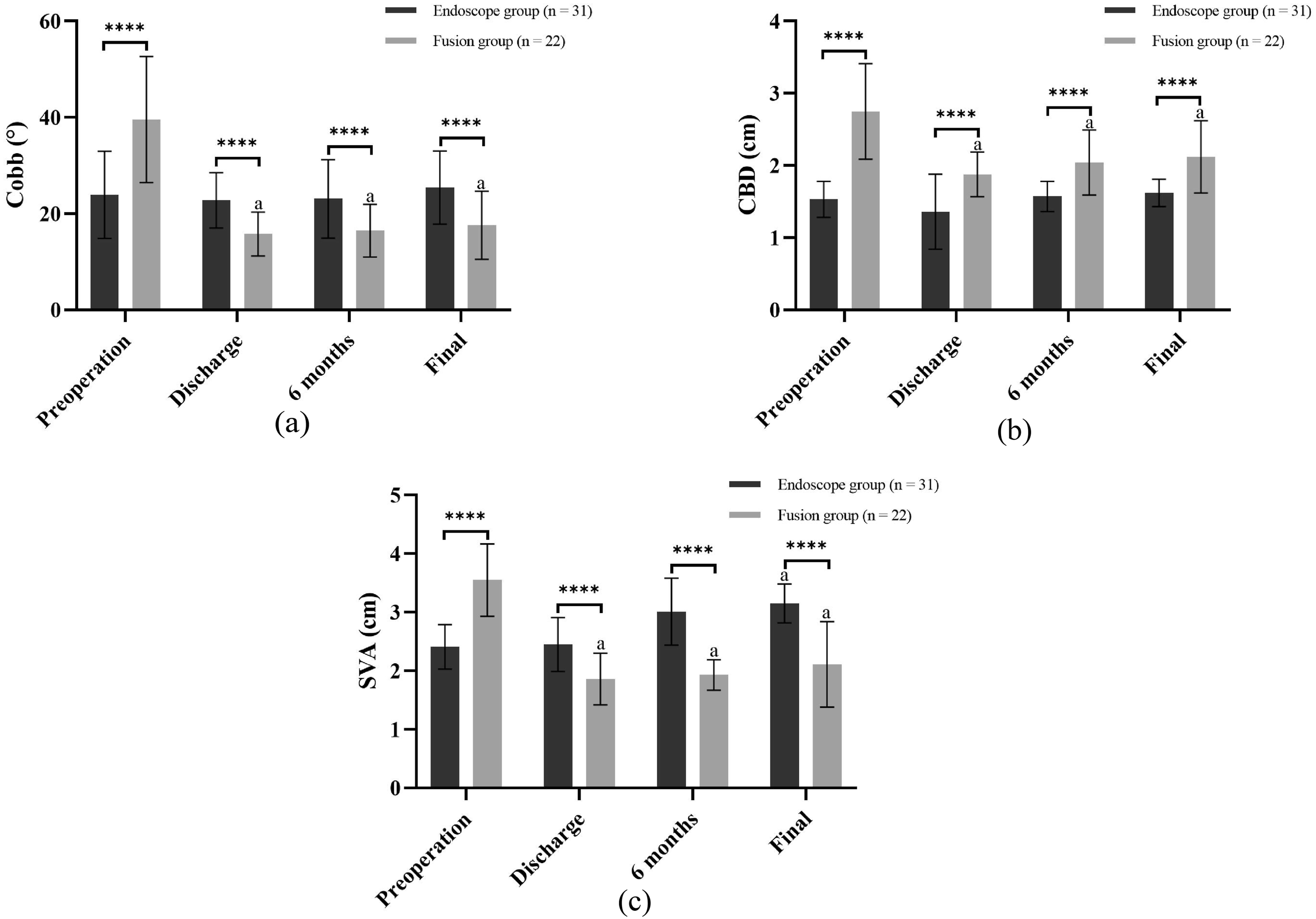
As illustrated in Figure 1b, the fusion group exhibited significantly higher CBD values compared to the endoscopic group at baseline and all postoperative follow-up points (P < 0.0001). Conversely, the endoscopic group demonstrated stable CBD values throughout the follow-up period (1.53 ± 0.25 mm preoperatively vs 1.62 ± 0.19 mm at final follow-up, P = 0.1158). The final CBD value in the fusion group significantly lower compared with the preoperative value (2.12 mm ± 0.50 mm vs 2.75 mm ± 0.66 mm, P = 0.0009). The CBD value in both groups at each follow-up did not meet the criteria for diagnosing coronal imbalance.
As shown in Figure 1c, the preoperative SVA value in the fusion group was significantly higher than that in the endoscope group (2.41 mm ± 0.38 mm vs 3.55 mm ± 0.62 mm, P < 0.0001), whereas the final SVA value in the endoscope group was significantly higher than that in the fusion group (3.15 mm ± 0.33 mm vs 2.11 mm ± 0.73 mm, P < 0.0001). In the endoscope group, the SVA value displayed a significant increase at the final follow-up compared to the preoperative value (P < 0.0001), whereas the preoperative SVA value in the fusion group was significantly lower at the final follow-up compared to preoperative values (P < 0.0001). The SVA value in both groups at each follow-up did not reach the threshold for diagnosing coronal imbalance.
In the endoscope group, the spinopelvic parameters at the final follow-up showed no significant variations compared to the preoperative values (P > 0.05). In the fusion group, the final PI was not significantly different compared to preoperative values (44.26° ± 4.08° vs 46.15° ± 3.69°, P = 0.1146). However, the final PT was significantly lower (13.53° ± 3.55° vs 20.53° ± 3.15°, P < 0.0001), the SS and LL values were significantly increased compared to preoperative values (SS: 31.46° ± 3.27° vs 24.39° ± 2.21°, P < 0.0001; LL: 30.32° ± 8.70° vs 22.41° ± 12.91°, P < 0.0001). No significant difference in pre-and post-operative PI values was observed between the two groups (P > 0.05). The PT value in the endoscope group was significantly lower than that in the fusion group (15.27° ± 2.33°, 20.53° ± 3.15°, P < 0.0001) during preoperative period, but significantly higher than that in the fusion group at the final follow-up (16.11° ± 3.56° vs 13.42° ± 3.55°, P = 0.0091). The preoperative SS and LL values in the endoscope group were significantly higher than those in the fusion group (P < 0.05). At the final follow-up, the SS in the fusion group was significantly higher than that in the endoscope group (31.46° ± 3.27° vs 27.79° ± 2.64°, P < 0.0001), whereas the LL was significantly lower than that in the endoscope group (30.32° ± 8.70° vs 34.62° ± 11.02°, P < 0.0001) (Figure 2). Within- and between-group comparisons of the spinopelvic parameters (a, b, c, d) during preoperative period and the final follow-up; **** indicates a P < 0.0001, *** indicates a P < 0.001, indicates a “ns” represents no statistical significance.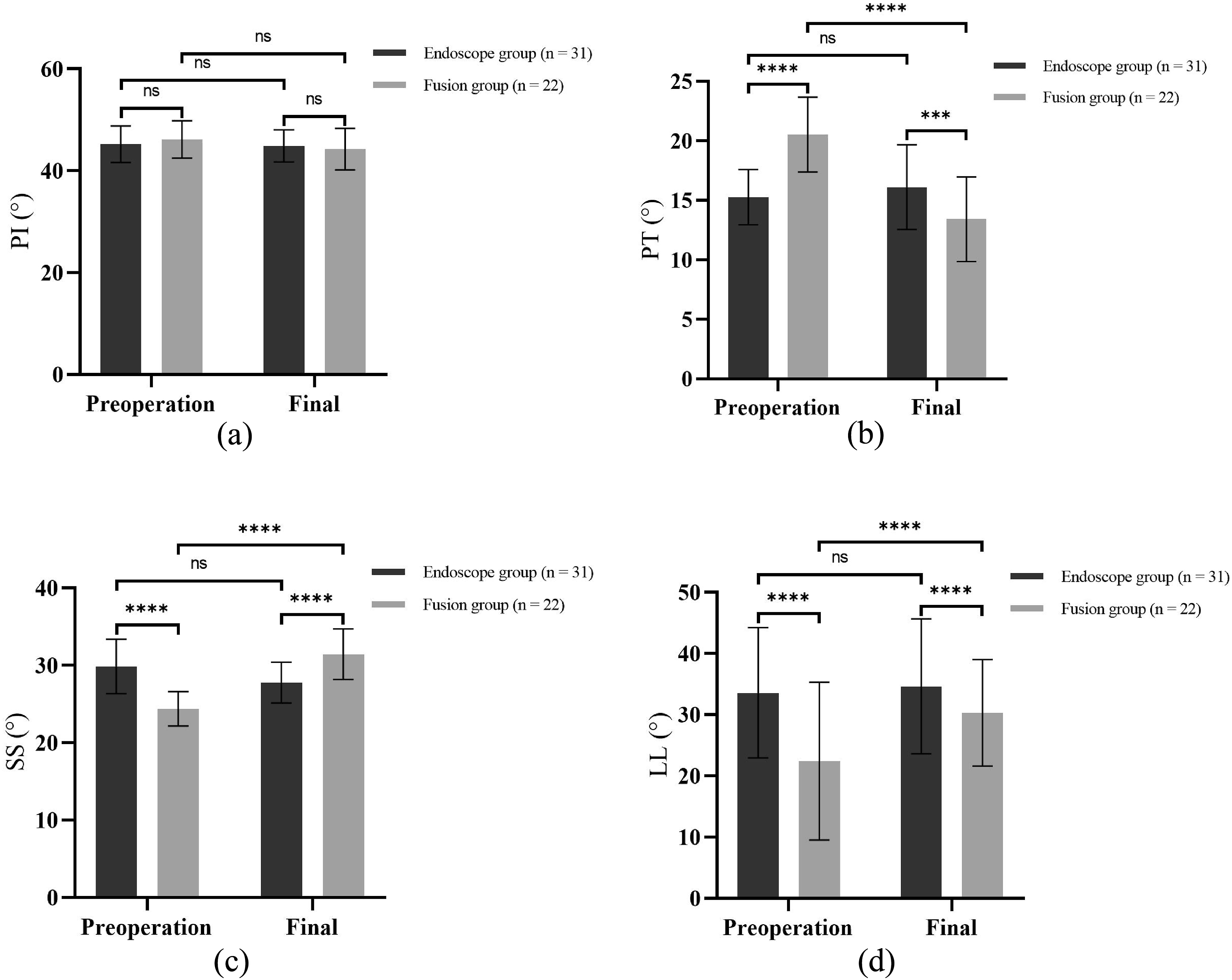
Clinical Outcomes
Data shown in Figure 3 indicate that both groups experienced significant improvements in back pain VAS, leg pain VAS, and ODI scores immediately postoperatively, with continued improvement throughout follow-up. No significant differences in preoperative back pain VAS scores were observed between groups (P = 0.4350). However, the endoscopic group demonstrated significantly lower back pain VAS scores compared to the fusion group at both 3-month (3.16 ± 1.09 vs 4.58 ± 1.32, P < 0.0001) and final follow-up (2.01 ± 0.68 vs 3.01 ± 0.78, P < 0.0001). No significant difference in leg pain VAS score was observed between the two groups during preoperative period and at each postoperative follow-up (P > 0.05). The ODI score in the endoscope group was significantly lower than that in the fusion group during preoperative period and each postoperative follow-up (P < 0.0001). At the final follow-up, 25 patients (80.6%) in the endoscope group and 17 patients (77.3%) in the fusion group were satisfied with the surgery (rated a ‘good’ or ‘excellent’ result per modified MacNab criterion), and no significant difference was noted between the two group (P > 0.05). Within- and between-group comparisons of the clinical outcome evaluations (a, b, c) during preoperative period and each postoperative follow-up; *** indicates a P < 0.001, “ns” represents no statistical significance.
Surgical Complications and Adverse Events
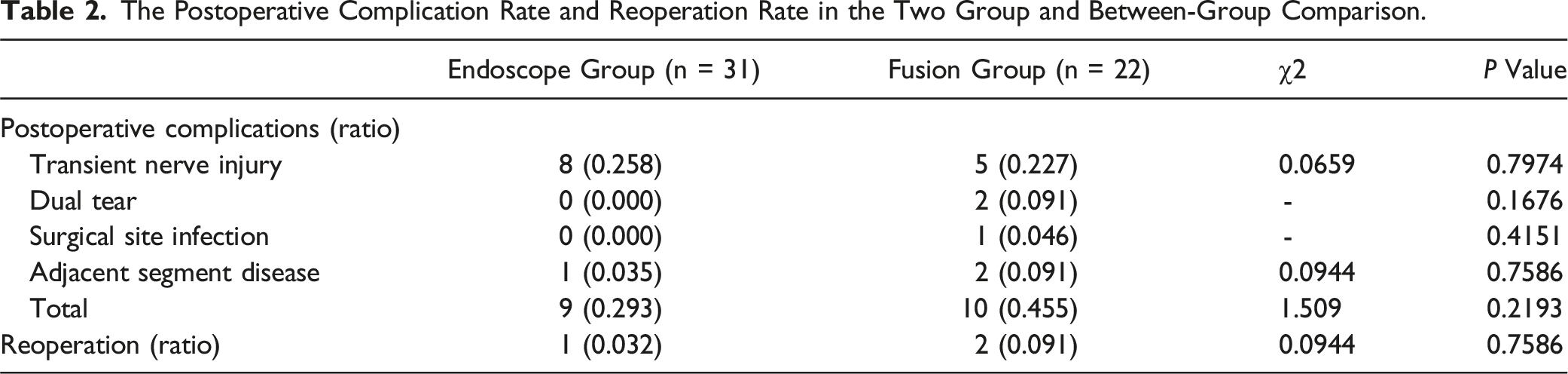
The Postoperative Complication Rate and Reoperation Rate in the Two Group and Between-Group Comparison.
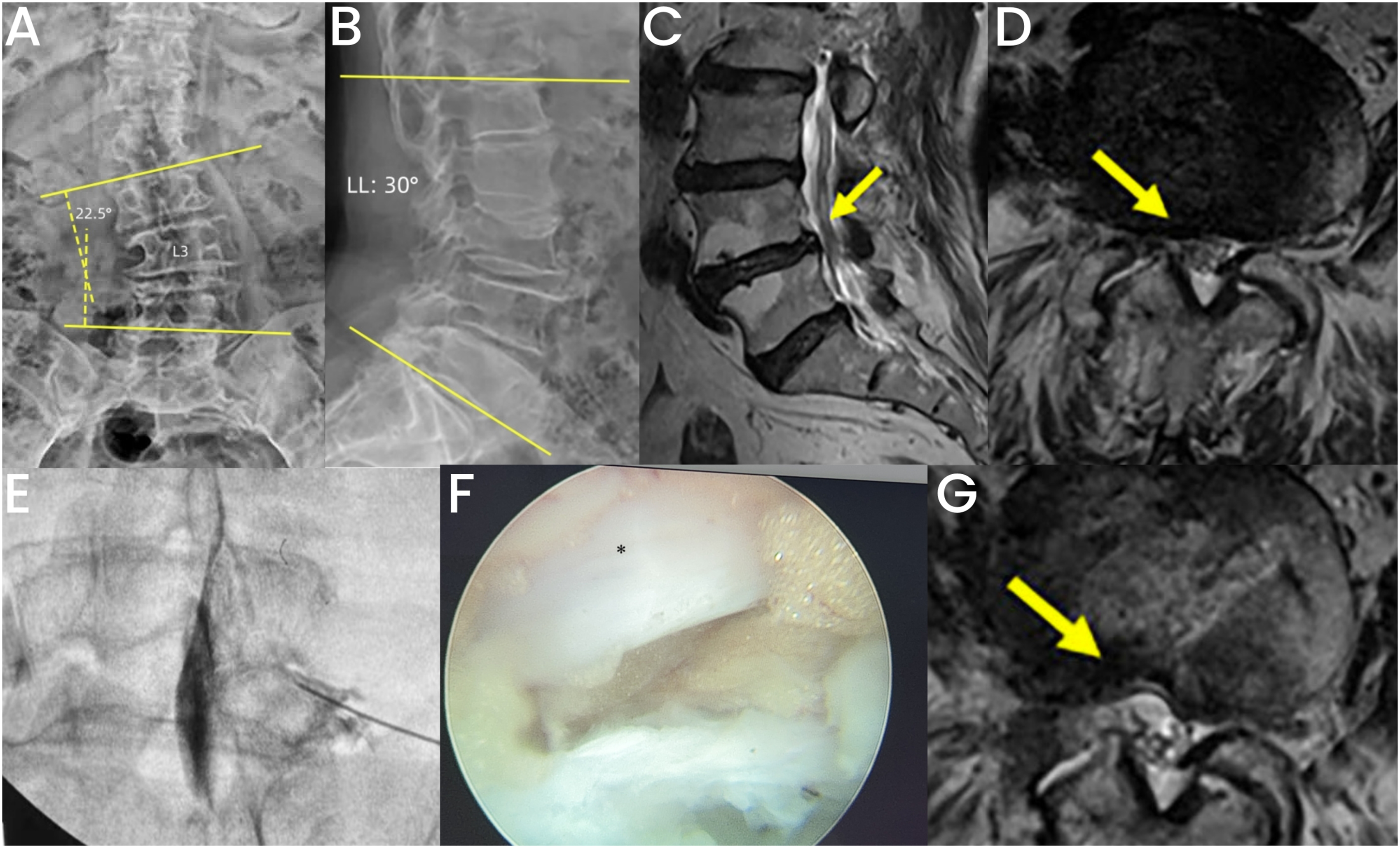
Presentation of a case with Lenke-Silva I deformity in the MIS group. (A, B) Preoperative anteroposterior and lateral view of lumbar spine X-ray showing a 22.5° of scoliotic Cobb angle and a 30° of LL; (C, D): Preoperative MRI of lumbar spine showing L4/5 lumbar disc herniation and right-sided foraminal stenosis; (E): The pain provocative test was positive for the L4 nerve root; (F): Transforaminal endoscopic decompression, * indicates impinged L4 nerve; (G): Postoperative MRI indicating a satisfactory decompression of dorsal and ventral side of nerve root.
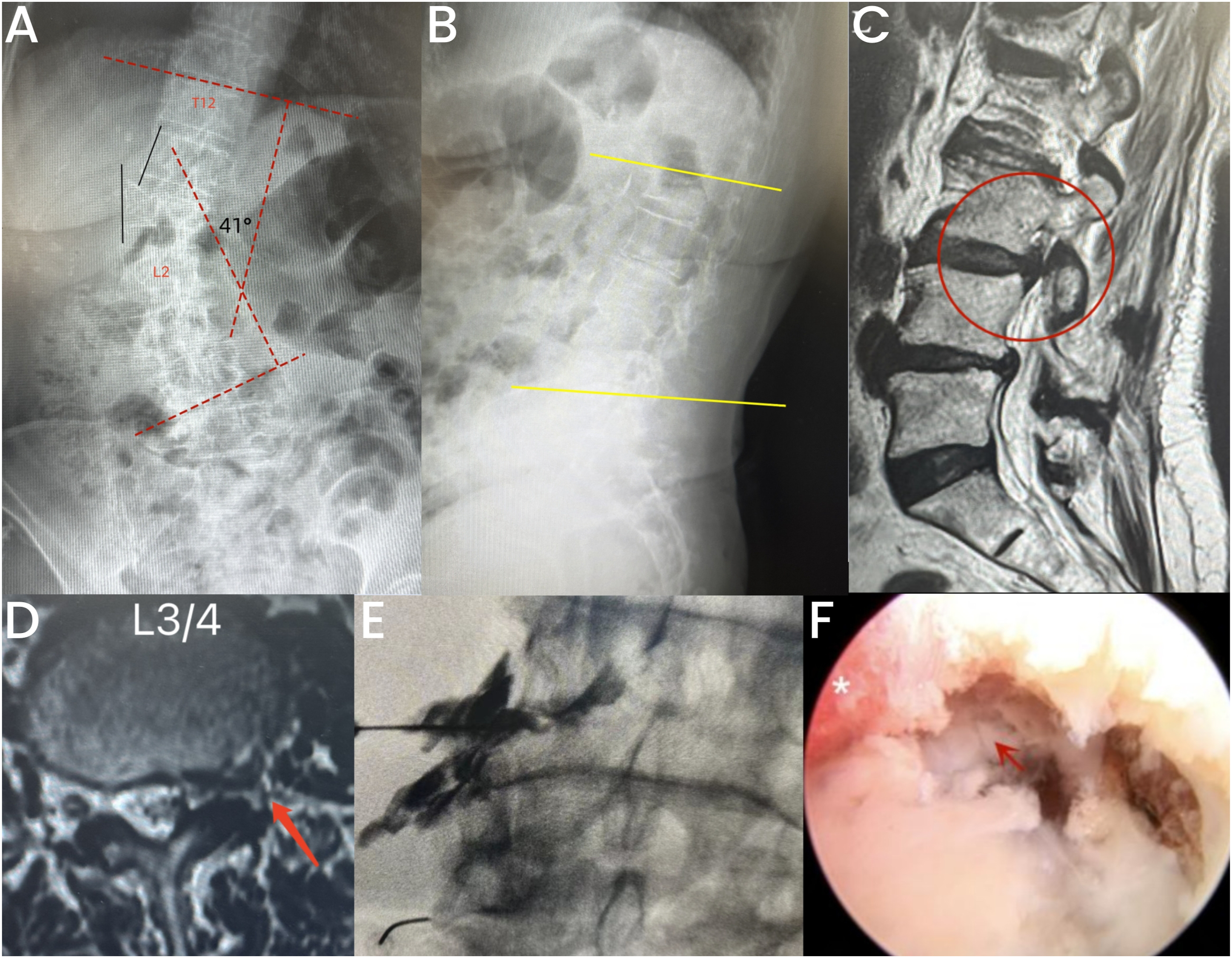
Presentation of a case with Lenke-Silva III deformity in the MIS group. (A, B) Preoperative anteroposterior and lateral view of lumbar spine X-ray showing olisthesis of apical vertebra, and a 41° of scoliotic Cobb angle without obvious lumbar kyphosis; (C, D): Parasagittal and cross-sectional view showing left-sided foraminal stenosis in L3/4, the L3 nerve was compromised; (E): The pain provocative test was positive for the L3 nerve root; (F): Transforaminal endoscopic decompression, * indicates impinged L3 nerve, the arrow indicates sequestered disc fragments.
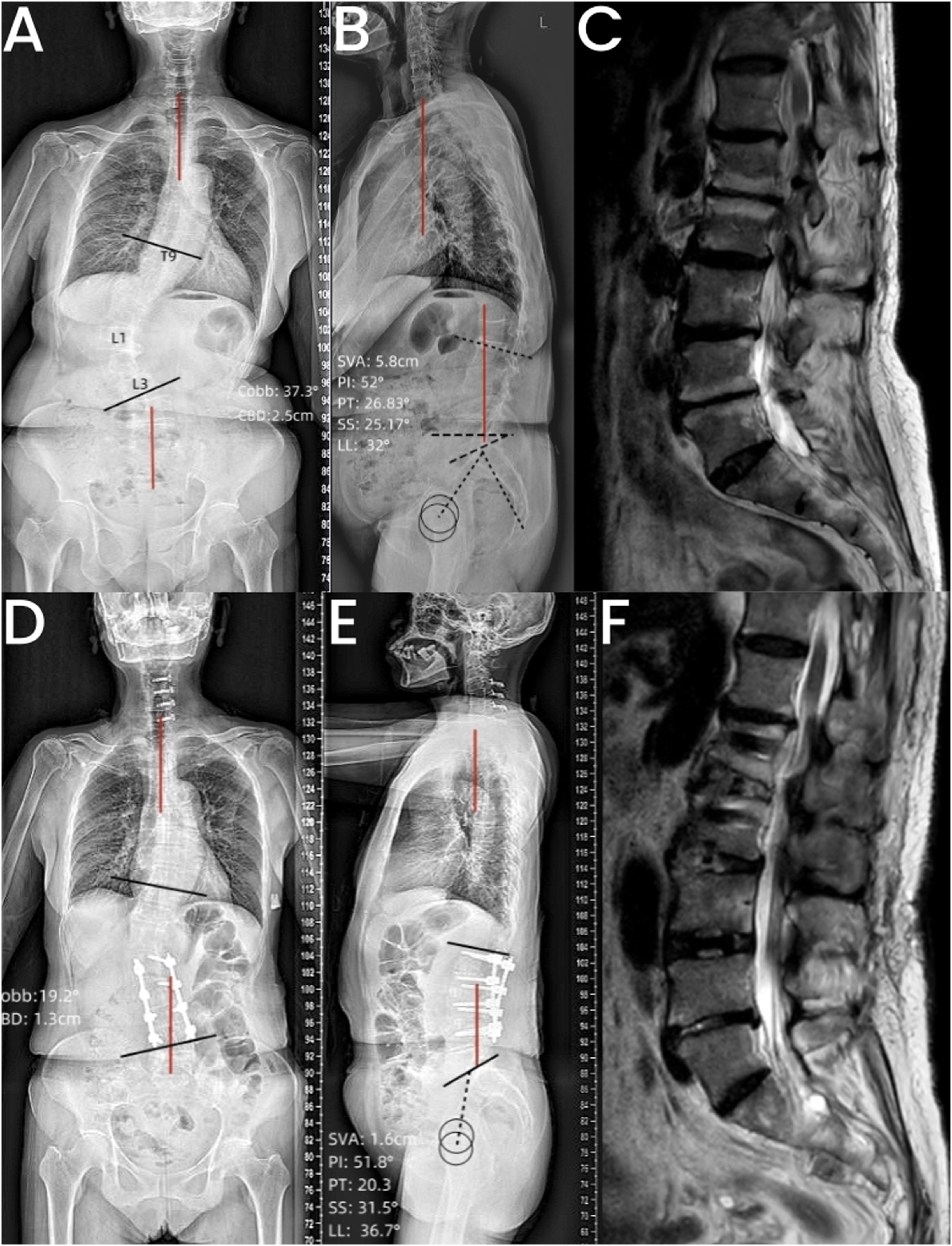
Case presentation of Lenke-Silva level V deformity in the Fusion group. (A, B) Anteroposterior and lateral view of the preoperative full-length standing radiography showing the scoliotic Cobb angle: 37.3°, CBD: 2.5 cm, SVA: 5.8 cm, PT: 26.83°, SS: 25.17°, LL: 32°; (C): Preoperative MRI of lumbar spine showing multisegmental lumbar stenosis, especially the L1/2, 2/3, and 3/4; (D, E): Anteroposterior and lateral view of the postoperative full-length standing radiography showing the scoliotic Cobb angle: 19.2°, CBD: 1.3 cm, SVA: 1.6 cm, PT: 20.3°, SS: 31.5°, LL: 36.7°; (F): Postoperative MRI of lumbar spine showing a satisfactory decompression of nerve root.
Discussion
The differences in patient characteristics, radiological parameters, and clinical outcomes were compared between two surgical fashions in the focal treatment of ADS associated with lumbar stenosis. For Lenke-Silva level I, II, or III deformity with one- or two-segment spinal stenosis, we found that the transforaminal endoscopic decompression alone yielded satisfactory clinical results without significant curve progression. For Lenke-Silva level III, IV, or V scoliosis with multi-segmental spinal stenosis, limited decompression/fusion can ameliorate patient symptoms and functional status, as well as improve the radiological parameters to some extent. While the fusion group demonstrated more favorable radiological improvements compared to the endoscopic group, both groups achieved comparable overall clinical outcomes.
The prevalence of ADS varies widely, ranging from 13% to 68% with an average of 37.6%. Notably, the condition is more common in individuals over 60 years old. 28 Back pain in ADS arises from multiple factors, including muscle fatigue, facet joint degeneration, and intervertebral disc disease. 6 Interestingly, the severity of back pain is not strongly correlated with the degree of coronal deformity, as patients tend to tolerate coronal curvature better than sagittal curvature due to lower energy expenditure. 29 Pérennou et al. 7 analyzed 671 adult patients with back pain and found that 7.5% of patients suffered from scoliosis and only 1% of all patients had scoliosis over 30°. Herein, we discovered no significant difference in preoperative VAS scores for back pain between the two groups (5.23 in the endoscope group vs 5.61 in the fusion group, P = 0.864), despite the mean scoliotic Cobb angle in the fusion group being significantly higher than that in the endoscope group (39.58° vs 23.92°, P < 0.0001). Our findings corroborate that of Jin et al., 26 i.e., they found no significant differences in preoperative back pain scores among patients with scoliotic Cobb angle of 10°—20°, 20°—30°, and >30°.
Although the Lenke-Silva level can guide the treatment decision for ADS to some extent, 2 there is no adequate data to help a surgeon decide between limited decompression alone, short segment fusion, or longer arthrodesis of the deformity. Interestingly, Smith et al.13,24 discovered that the fellowship and practice composition would greatly influence the surgical strategy in ADS. Surgeons who treat mostly degenerative spine prefer decompression alone or short-segmental fusion, whereas those who predominantly treat spinal deformity prefer longer arthrodesis of the deformity. The ADS that combine with rigid sagittal plane imbalance or PI-LL mismatch may benefit more from a major deformity correction procedure.30,31 However, this results in a high incidence of surgical complications and pseudoarthrosis. 32 Amara et al. 33 reviewed 99 patients with ADS and associated lower limb radiculopathy, they compared the radiographical and clinical outcomes between those who undergoing short-segment fusion (preoperative Cobb angle: 28.7°), long-segment fusion with correction of major lumbar curve (preoperative Cobb angle: 30.5°), and longer fusion with correction of thoracic and lumbar curve (preoperative Cobb angle: 42.7°). Consequently, they found the curve in the short-segment fusion group did not significantly progress during 1-year follow-up. Besides, patients in the short-segment fusion group had the lowest surgical complications and revision rates. In the present study, the mean preoperative Cobb angle in the fusion group was 39.58°, and we treated this group of patients with limited instrumentation and fusion, without intended deformity correction. The scoliotic Cobb angle, spinal balance, and spinopelvic parameters significantly improved at the final follow-up. Coronal correction may be equally well accomplished with minimally invasive techniques. 25 Notably, the patient who had level V deformity and imbalance on sagittal plane underwent limited indirect decompression and interbody fusion via an oblique approach obtained acceptable recovery of sagittal and coronal alignment. Within the available follow-up, we observed no internal fixation failure or pseudoarthrosis; the reoperation rate was 9.1%, and the overall satisfaction rate was 77.3%.
Patients with ADS often seek medical treatment for the debilitating radicular pain resulting from disc bulging, facet arthritis, and ligamentum flavum hypertrophy.1,9 The efficacy of focal treatment alone in adult degenerative scoliotic deformity has not been confirmed.16,34 In cases where the patient’s symptoms can be attributed solely to a focal pathology, a decompression procedure alone may achieve satisfactory clinical outcomes. Furthermore, in cases where a focal issue coexists with a larger deformity, minimally invasive decompression techniques can help mitigate deformity progression by preserving soft tissue on the unaffected side while minimizing disruption on the surgical side. The percutaneous transforaminal endoscopic decompression may serve as an alternative to the traditional microscopic decompression. Recent studies have reported the successful application of transforaminal endoscopic decompression in the treatment of ADS with symptomatic stenosis.26,27 In our study, patients in the endoscope group were characterized by advanced age, moderate coronal deformity (mean scoliotic Cobb angle: 23.92°), and a high prevalence of comorbidities. During the treatment, a selective spinal nerve root provocative pain test before surgery was used to identify the responsible disk level. We conclude that the transforaminal endoscopic decompression has the following benefits: (1) advanced endoscopic instruments promote adequate decompression of the ventral and dorsal side of the nerve roots; (2) the transforaminal approach does not disturb bony stabilizers, including lamina and spinous process, and can preserve facet joint as much as possible, thereby, reducing the risk of deformity progression; (3) part of the hypertrophic facet joint can be trimmed to alleviate mechanical back pain to some extent. We postoperatively observed a continued improvement in radicular pain and back pain. Moreover, the patients in the endoscope group had more tolerable back pain at the final follow-up and better functional capacity at each postoperative follow-up than those in the fusion group. Although radiological parameters did not improve postoperatively, the scoliotic Cobb angle increased minimally by only 1.51°, and neither CBD nor SVA reached criteria for imbalance at final follow-up. Although the endoscopic group exhibited lower complication and reoperation rates compared to the fusion group, these differences did not achieve statistical significance due to the limited sample size.
This study has several limitations. Firstly, the patient population was not randomly selected but rather consisted of specifically chosen individuals. Secondly, notable demographic and baseline differences between the two groups may have compromised the comparability of the results, potentially affecting the study’s conclusions. Thirdly, the relatively small sample size limited the statistical power to detect significant changes in radiographic and clinical outcomes pre- and postoperatively. Finally, the short follow-up duration restricted the ability to fully assess deformity progression and reoperation rates.
Conclusion
The optimal surgical treatment for ADS remains elusive. A focal approach targeting spinal stenosis within ADS is gaining prominence. This study shows that for patients with ADS and minimal sagittal or coronal plane imbalance, limited decompression and fusion offers satisfactory clinical outcomes with acceptable radiological results and low complication rates. Alternatively, endoscopic transforaminal decompression provides a safe and effective minimally invasive option for managing mild to moderate, or even more severe, deformities. This technique preserves bone structure, limits curve progression, and can potentially delay the need for major corrective surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support to this research was provided by National Key Research and Development Program of China (2022YFC3600402).