
Abstract
Objective
To introduce the concept of ‘nerve root as the core’ and to investigate the surgical procedure and curative effect of percutaneous translaminar endoscopic discectomy (PTED) surgery in the treatment of different types of lumbar disc herniation (LDH).
Methods
This retrospective study analysed the clinical data from patients with LDH that underwent single-segment PTED surgery. They were divided into three groups based on LDH location: central canal zone group, lateral recess zone group and foraminal/far lateral zone group. Different working cannula placement methods were used for the different types of LDH. All patients were followed for at least 12 months. Clinical and follow-up data were compared between the three groups.
Results
A total of 130 patients were enrolled in the study: 44 (33.8%) in the central canal zone group, 72 (55.4%) in the lateral recess zone group and 14 (10.8%) in the foraminal/far lateral zone group. All three groups of patients achieved good postoperative results. The improvements in leg pain and disability were most marked in the first postoperative month in all three groups.
Conclusion
PTED achieved adequate decompression for different types of LDH. The concept of ‘nerve root as the core’ facilitated the accurate placement of the working cannula.
Keywords
Introduction
Compression of nerves by lumbar disc herniation (LDH) may cause a variety of sensory deficits and decreased motor function in patients, 1 the most common of which are pain, numbness and lower extremity weakness. Lumbar discectomy may relieve lower extremity symptoms in patients with LDH and is an extensively studied spinal procedure. 2 The most important trend in discectomy has been to minimize soft tissue stripping. 3 In recent years, with the rapid development of minimally-invasive spine surgery, percutaneous translaminar endoscopic discectomy (PTED) has provided a less invasive technique to address LDH. 4 It has become an increasingly popular surgical procedure for the treatment of LDH due to its advantages of low invasiveness, high accuracy and quick recovery.4,5 However, there are some differences in the surgical approaches for different types of LDH, which poses certain difficulties for spine surgeons. A steep learning curve and lack of experience can often lead to serious complications, including infections, late recurrence, nerve root damage, hypoesthesia, dural tear, vascular damage and death.6,7 Obviously, proficiency in the PTED technique is essential for spine surgeons.
Unfortunately, to the best of our knowledge, there are no descriptions of the surgical operations of PTED for the treatment of different types of LDH. The aim of this study was to investigate the surgical operation of PTED for different types of LDH. The efficacy was evaluated at a 12-month follow-up to provide a reference for clinical practice.
Patients and methods
Study population
This retrospective study analysed the clinical data from consecutive patients with LDH admitted to the Department of Orthopaedics, Affiliated Hospital of Chengde Medical University, Chengde, Hebei Province, China between May 2018 and May 2020. All patients underwent single-segment PTED surgery. All operations were performed by the same surgical team. The inclusion criteria were as follows: (i) patients with mainly symptoms of the legs; (ii) preoperative computed tomography and magnetic resonance imaging were consistent with the clinical symptoms; (iii) patients that had failed after at least 3 months of conservative treatment; (iv) patients that were scheduled for PTED. The exclusion criteria were as follows: (i) patients with significant lumbar instability and deformity; (ii) patients with large prominent or highly migrated nucleus pulposus; (iii) patients with pathological conditions such as spinal tumours and tuberculosis; (iv) patients with a history of lumbar fractures or surgery; (v) multisegment disc herniation requiring treatment; (vi) patients with incomplete data or those that could not be followed-up. A simple and practical method of defining LDH was used in clinical practice. Based on the location of the protrusion and the anatomical region, LDH was divided into the central canal zone, lateral recess, foraminal zone and far lateral zone (Figure 1A). 8

(a) The four types of lumbar disc herniation (LDH). (b) With the ‘nerve root as the core’, different types of LDH require the establishment of different working cannulas. The colour version of this figure is available at: http://imr.sagepub.com.
This research was approved by the Ethics Committee of Affiliated Hospital of Chengde Medical University, Chengde, Hebei Province, China (no. CYFYLL2021166). Written informed consent was obtained from the patient to undergo treatment and to publish this report.
Surgical procedure
The patient was placed in a lateral position with the affected side on top. A round pillow was placed under the lumbar region to increase the height of the intervertebral foramen on the affected side. Then, the torso was perpendicular to the bed surface and the lower limbs were slightly bent. The posterior lateral approach was used for the surgical approach. The responsible disc plane and the posterior midline of the spinous process were marked with the help of the C-arm. After skin disinfection and sterile towel placement, the skin and deep fascia were anaesthetized with 1% lidocaine.
The surgical procedure included three steps: (i) puncture – the puncture site depends on the patient's body type. It is usually 1–3 cm above the iliac crest and 8–12 cm horizontally from the midline of the posterior spinous process. The puncture needle points to the intersection of the coronal plane connecting the upper articular process and the horizontal plane of the responsible intervertebral disc. Based on the protruding position of the nucleus pulposus shown by preoperative imaging, under the guidance of the C-arm, an 18-gauge spinal needle was introduced into the corresponding target area; (ii) foraminoplasty – an approximately 8-mm incision was made at the skin entrance. The intervertebral foramen was shaped as needed, usually using continuous bone drills to moderately remove the superior articular process bone; (iii) discectomy – after insertion of a working trocar, an endoscope was placed. The protruding nucleus pulposus was removed using a clamp under the protection of a trocar. Then, the nerve root was explored and released. Finally, under endoscopy, the nerve root was seen to fall back and the surrounding space was fully decompressed. A negative intraoperative straight-leg elevation test further indicated that the decompression was definitive and effective. 9 This was a sign of the end of the procedure.
Nerve root as the core
The operational difference among the different types of LDH was mainly in the working channel. The idea of focusing on the nerve root requires precise placement of the working cannula. This allows the surgeon to find the compressed nerve as early as possible under endoscopy. Depending on the location of the disc herniation, the target area of the working trocar was located in the appropriate position. This is described as follows (Figure 1B). Anteroposterior X-ray images before the manipulation of the four types of LDH (Figures 2A–2D): (i) central canal zone: close to the posterior midline of the spinous process; (ii) lateral recess zone: approximately 3–5 mm from the posterior midline of the spinous process; (iii) foraminal: about 5–10 mm from the posterior midline of the spinous process but not more than the outer edge of the arch; (iv) far lateral zone: outer edge of the intervertebral foramen. Sequential sagittal X-ray images (Figures 2E–2G): as some large protruding nucleus and highly migrating nucleus pulposi were excluded, the working sleeve was generally located on the posterior upper edge of the lower vertebral body. Adequate decompression of the nerve root signalled the end of the procedure (Figures 2H). Under the concept of ‘nerve root as the core’, PTED was successfully completed for different types of LDH (Figure 3).

Representative anteroposterior X-ray images before endoscopic procedures for different types of lumbar disc herniation (LDH) are shown in Figures A–D: (a) central canal zone; (b) lateral recess zone; (c) foraminal zone; (d) far lateral zone. (e–g) The intraoperative sagittal X-ray images were similar for the different types of LDH. Intraoperative consecutive sagittal X-ray images of the central canal zone are shown. (h) The nerve root after adequate decompression.

Structural changes as demonstrated by magnetic resonance imaging undertaken before and after endoscopic surgery for two types of lumbar disc herniation (LDH). The red arrows indicate preoperative images and the green arrows indicate postoperative images. a and e are the preoperative images of the central canal zone. b and f are the corresponding postoperative images of the central canal zone. c and g are the preoperative images of the foraminal zone. d and h are the corresponding postoperative images of the foraminal zone. The colour version of this figure is available at: http://imr.sagepub.com.
Postoperative management and clinical evaluation
After 1 day of postoperative bed rest, the patient could wear a lumbar brace to move out of bed. After 1 week, light physical work was resumed, but bending and weight-bearing activities were avoided. The clinical outcomes were evaluated by using a visual analogue scale (VAS) to score leg pain and the Oswestry disability index (ODI) preoperatively and at 1 month, 3 months, 6 months and 12 months postoperatively. 10 In addition, surgical satisfaction rates were assessed by using the modified MacNab criteria at the final follow-up. 11
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). The data are presented as mean ± SD and n of patients. The independent sample t-test or one-way analysis of variance were used to compare the differences in the mean of the outcome scores from pre- and postoperative variables. A P-value < 0. 05 was considered statistically significant.
Results
This retrospective analysis included 130 patients (68 males and 62 females) that were followed up for a mean of 20 months (range, 12–36 months). There were 44 patients (33.8%) with LDH in the central canal zone and 72 patients (55.4%) with LDH in the lateral recess zone. Since the foraminal and far lateral zones accounted for a small number of patients, they were included in the same group (n = 14; 10.8%). The clinical and demographic characteristics of the three groups are presented in Table 1. The mean ± SD age of the overall study cohort was 44.4 ± 12.1 years. The mean age of patients in the foraminal and far lateral zone group was significantly higher compared with the other two groups (P < 0.05). The majority of herniated discs were located in the L4–L5 and L5–S1 segments (118 of 130 patients; 90.8%). The mean ± SD postoperative hospital stay of the overall study cohort was 4.7 ± 1.9 days and there was no significant difference between the three groups.
Demographic and clinical characteristics of patients (n = 130) with lumbar disc herniation (LDH) that were enrolled in a study to investigate the use of percutaneous translaminar endoscopic discectomy for different types of LDH.
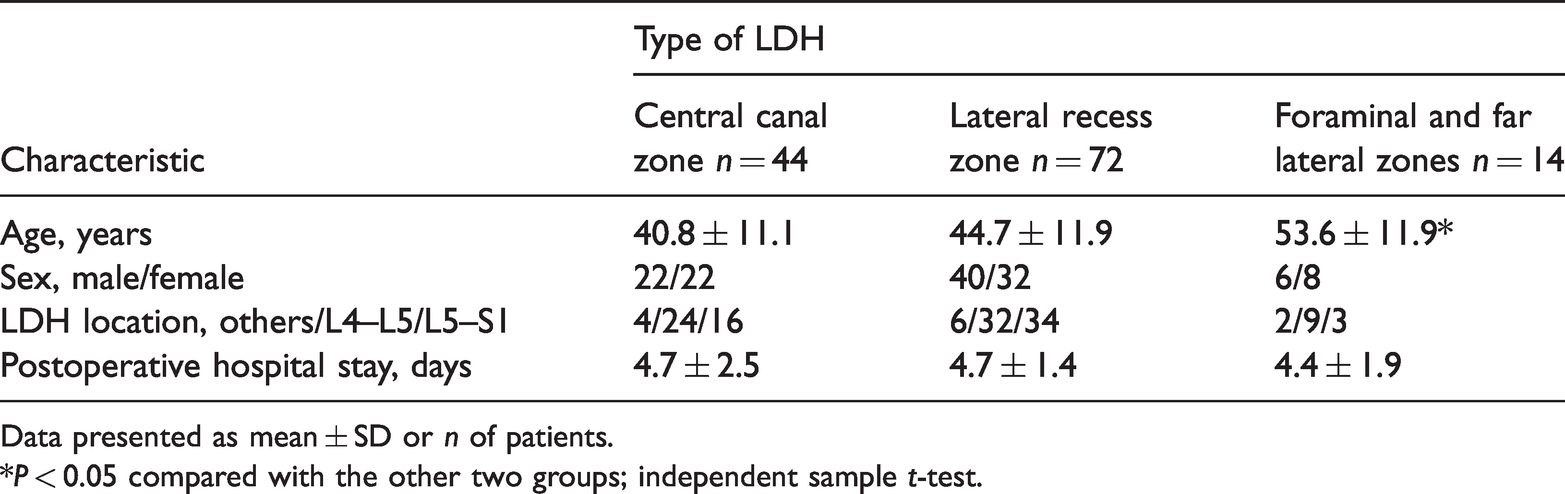
Data presented as mean ± SD or n of patients.
*P < 0.05 compared with the other two groups; independent sample t-test.
All patients were operated on successfully. Changes in the clinical outcomes before and after surgery were demonstrated by the VAS leg pain score, ODI score and modified MacNab criteria. For the overall study cohort (n = 130), the mean ± SD preoperative VAS score was 7.4 ± 1.1; and it reduced to 2.6 ± 1.0, 2.0 ± 1.0, 1.2 ± 0.9 and 0.8 ± 0.9 at 1, 3, 6 and 12 months after surgery, respectively (Figure 4A). The mean ± SD preoperative VAS score was 6.9 ± 1.1 in the central canal group and 8.4 ± 0.7 in the foraminal and far lateral group (P < 0.01). At 1 month after surgery, the VAS scores of the three groups were significantly reduced (P < 0.05). Among them, the VAS scores of the foraminal and far lateral group had the fastest decline (P < 0.05), which was 1.9 ± 0.9 at 1 month after surgery. At the subsequent follow-up time-points, there were no significant differences between the three groups.

Clinical outcomes at different follow-up stages from preoperation to 12 months postoperation: (a) visual analogue scale (VAS) leg pain scores; (b) Oswestry disability index (ODI) scores; (c) modified MacNab criteria at the last follow-up. The colour version of this figure is available at: http://imr.sagepub.com.
For the overall study cohort (n = 130), the mean ± SD preoperative ODI score was 63.5 ± 9.3; and it reduced to 34.2 ± 2.5, 24.2 ± 1.7, 19.4 ± 1.7 and 15.3 ± 2.8 at 1, 3, 6 and 12 months after surgery, respectively (Figure 4B). The mean ± SD preoperative ODI scores were 60.6 ± 8.3 in the central canal group and 68.9 ± 11.1 in the foraminal and far lateral group (P < 0.01). At 1 month after surgery, the ODI scores of all three groups showed a significant decrease (P < 0.05). At 1 month after surgery, the ODI scores of the foraminal and far lateral group showed a more significant decrease than the central canal group (P < 0.05). At the subsequent follow-up time-points, there were no significant differences between the three groups. In the long term, patients in the three groups had the fastest recovery at 1 month postoperatively, which gradually slowed down at 3 months postoperatively, stabilizing at 6 months postoperatively.
At the final follow-up, 124 of 130 patients (95.4%) achieved excellent and good based on the modified MacNab criteria (Figure 4C). One patient underwent revision surgery at a later stage and the other five patients reported that they were not sufficiently satisfied with the results.
There was no significant difference in the incidence of major complications among the three groups of patients (Table 2). One patient in each group had transient postoperative sensory disturbance (transient dysethesia). One patient in the central canal group had a minor dural injury, which was not repaired during the operation. The patient had no special discomfort 1 week after the operation. A male patient in the central canal group performed agricultural manual labour, prematurely, within 1 month after surgery and then relapsed during the follow-up period and underwent revision surgery. Two patients in the lateral recess group had minor nerve injury. None of the patients had serious nerve injury, haematoma formation or wound infection.
Major complications in patients (n = 130) with lumbar disc herniation (LDH) that were enrolled in a study to investigate the use of percutaneous translaminar endoscopic discectomy for different types of LDH.

Data presented as n of patients.
No significant between-group differences (P ≥ 0.05); one-way analysis of variance.
Discussion
Approximately 70–85% of the population will suffer from one or more episodes of lower back pain during their lifetime, the main cause of which is LDH. 12 What follows is motor dysfunction caused by nerve compression. 13 LDH is so prevalent that the problem of work incapacity it causes has been recognized as a global health problem. 14 The vast majority of patients with LDH do not require surgical treatment, but 1–5% of patients require surgery due to failure of conservative treatment. 15
Since the advent of percutaneous endoscopy, its advantages of minimal trauma, fast recovery and the ability to preserve the posterior ligament complex and other biomechanical structures have been recognized by spine surgeons and patients.16,17 As a minimally-invasive surgical method, PTED is widely used in the treatment of LDH. 5 Most hospitals at home and abroad have also successively developed PTED technology. 18 Unfortunately, the number of surgeons that have mastered this technology is still relatively small. 19 Inexperience often leads to serious complications, including infection, late recurrence, nerve root damage, hypoesthesia, dural tears, vascular damage and death.6,7
Theoretically, PTED can solve almost all types of LDH.20–22 However, behind similar symptoms lies different causes of the disease. The protruding nucleus pulposus may be located in different positions and different types of LDH surgery have different operating methods. This makes it difficult to adequately remove the intervertebral disc. The conventional transforaminal endoscopic surgical system can safely and effectively treat LDH, but the inside-out approach still presents difficulties in some aspects. 23 When the working channel is placed in the centre of the spinal canal, the soft tissue is not easily distinguished in the first view of the endoscope. The loss of spatial orientation can easily cause nerve damage. A previous study reported that a failure of decompression was associated with the location of the protruding nucleus pulposus. 24 If the working cannula cannot be placed better, it will make the operation difficult. Obviously, PTED focuses on the precise placement of the working cannula, which is an operation that guides the cannula to the target tissue. 20 Therefore, we have suggested the concept of ‘nerve root as the core’. Safety is a prerequisite for surgery. This concept takes the nerve root as the focal point and is dedicated to the precise placement of the working cannula. The aim was to make the working cannula open to the target tissue. This requires different operations with the aid of the C-arm for different types of LDH. The endoscopic operation with ‘nerve root as the core’ provides a clear sense of orientation and reduces the probability of accidental injury to the nerve root.
For spine surgeons that are good at minimally-invasive spinal surgery, the puncture strategy of PTED should be familiar and can be easily designed and successfully performed. 25 A study that followed 10 228 patients with LDH that underwent percutaneous endoscopic lumbar discectomy found that 95 (33.6%) of the 283 patients with incomplete removal of the herniated disc had improperly positioned working access; 91 of which (32.2%) occurred in the central herniated discs. 26 Central disc herniation is often accompanied by a higher failure rate. 26 Therefore, in the past, it was considered a contraindication for trans-hole endoscopic discectomy. In this current study, the puncture target for central disc herniation was close to the posterior midline. The premise of this process is the full expansion and formation of the intervertebral foramen. Therefore, there is enough space to remove the prominent nucleus pulposus tissue. Subsequently, the contralateral nerve root was explored to achieve the effect of ‘unilateral access, bilateral decompression’. For disc herniation in the lateral recess and the foraminal zone, the target points fall approximately 3–5 mm and 5–10 mm from the posterior midline. The working cannula was introduced into the target area in the ideal direction. Then, in the first field of view under the endoscope, it was easy to find the lifted nerve root. Finally, nucleus pulposus forceps were used to remove the protruding nucleus pulposus while avoiding damage to the nerve roots. Similarly, when the herniated disc was located in the far lateral zone, the puncture target was more distant from the posterior midline. For this type of LDH, the skin entry point was closer to the interior and the angle of entry was steeper. The target area was usually located at the outer edge of the intervertebral foramen. The tip of the working cannula was positioned posteriorly medial to the herniated nucleus pulposus and the compressed nerve. It is worth noting that the initial working cannula on the sagittal image was positioned at the posterior upper edge of the lower vertebral body. Then, the cannula was gradually moved up during the operation, which was conducive to smoothly removing the protruding tissue.
The safe completion of decompression operations is the expectation of every spine surgeon. Practically, the concept of ‘nerve root as core’ requires the combination of the prominent nucleus pulposus with the nerve root. The position of the working cannula depends on the type of LDH. This strategy is also the essence of the surgery. In addition, this current study followed the clinical results of each group after surgery. The first thing worth considering is the problem of recurrence. Recurrent nucleus pulposus herniation after lumbar discectomy is a common problem. 27 A 5-year survey that studied 1900 patients undergoing percutaneous foraminal discectomy found that recurrence occurred in 209 cases (11.0%) and it most often occurred within 2–30 days after surgery. 28 During the follow-up period in the current study, a male patient with central disc herniation performed agricultural manual labour, prematurely, within 1 month after surgery and then relapsed. A previous study reported that the growth of scar tissue after surgery can surround and protect the nucleus pulposus tissue. 29 Undoubtedly, this procedure helps stabilize the intervertebral space. Care should be taken to maintain the lumbar spine after surgery, such as not bending frequently, not lifting heavy objects and not maintaining the same position for long periods of time. 30 This is an important factor in preventing recurrent herniation. Therefore, the patient’s relapse might have been related to their premature physical work. Of course, for patients with central disc herniation, thorough decompression during the operation is important. At the same time, patients should pay attention to standardized rehabilitation after surgery. Fortunately, no recurrence was found in the other two groups during the follow-up period in the current study.
Overall, all three groups of patients had encouraging results after surgery in this current study. However, there were some differences among the groups. A previous study reported that approximately 7% of herniated intervertebral discs appeared on the outside of the spinal canal, most commonly in the L4–L5 segment. 31 This was similar to the findings of the current research, which showed that there were 14 patients (10.8%) with disc herniation located in the foraminal and far lateral zones, of which nine were located in the L4–L5 segment. Notably, the foraminal and far lateral group in this current study exhibited more severe pain and motor dysfunction preoperatively. The reason may be that the herniated disc tissue is more inclined to directly compress and irritate the dorsal root ganglion. 32 This directly causes more severe clinical symptoms. However, these symptoms were significantly improved 1 month after surgery. A previous study showed that the postoperative ODI score of far lateral disc herniation was higher than that of other types of herniation. 32 The authors suggested that one of the reasons was that the surgeon's unskilled operation of this type of LDH caused more soft tissue damage. 32 This was different from the findings of the current study, which showed more significant improvement in VAS leg pain scores and ODI scores in the foraminal and far lateral group at 1 month postoperatively compared with the other two groups. This phenomenon may be due to unbearable pain prompting patients to seek medical treatment in a timely manner. The short-term course of the disease did not cause serious nerve damage. The concept of ‘nerve root as the core’ was also beneficial for avoiding serious injuries during surgery.
At the end of the follow-up period, 124 of 130 patients (95.4%) indicated excellent or good outcomes according to the modified MacNab criteria. Only one patient experienced a relapse. A previous study demonstrated a recurrence rate at 1 year after posterolateral endoscopic discectomy of 6.9%. 33 At the 2-year follow-up, 85.4% of the patients still reported excellent or good results. 33 This was comparable with the results of the current study. None of the patients in the current study experienced serious complications such as severe nerve injury, cerebrospinal fluid leakage or wound infection. Overall, the patients in the three groups showed the fastest improvements in VAS leg pain scores and ODI scores at 1 month postoperatively, with the improvements gradually slowing down at 3 months postoperatively and stabilizing at 6 months postoperatively. Moreover, no significant difference was found in the efficacy of the three groups of patients at 12 months after surgery.
This current study had several limitations. First, even though the study included most of the patients with LDH, some were excluded, such as those with highly migratory and large protruding nucleus pulposi. Secondly, the learning curve for PTED surgery was high, making it difficult for junior surgeons to accurately establish working access. Thirdly, although PTED shows good short-term results, it still requires long-term follow-up.
In conclusion, using the concept of ‘nerve root as the core’ was beneficial for improving the safety and effectiveness of PTED surgery. Accurate placement of the working cannula was the key to satisfactory clinical results.
Footnotes
Authors' contributions
All authors contributed to the study conception and design. Pengfei Li, Fengkai Yang and Ying Chen prepared the materials and collected the data. The first draft of the manuscript was written by Pengfei Li. Pengfei Li and Youxin Song revised the manuscript. All authors read the manuscript critically to improve the intellectual content. All authors read and approved the final manuscript.
Acknowledgement
We would like to thank all of the study participants.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.