
Abstract
Study Design
Retrospective cohort study.
Objectives
Investigate the risk factors for delayed extubation after posterior approach orthopedic surgery in patients with congenital scoliosis.
Methods
The clinical data of patients who received surgery for congenital scoliosis at the First Affiliated Hospital of Xinjiang Medical University between January 2021 and July 2023 have been gathered. Patients are categorized into the usual and the delayed extubation groups, depending on the duration of tracheal intubation after surgery. The study employs univariate and multivariate logistic regression models to examine the clinical characteristics of the two cohorts and discover potential risk factors linked to delayed extubation. In addition, a prediction model is created to visually depict the significance of each risk factor in terms of weight according to the nomogram.
Results
A total of 119 patients (74.8% females), with a median age of 15 years, are included. A total of 32 patients, accounting for 26.9% of the sample, encountered delayed extubation. Additionally, 13 patients (10.9%) suffered perioperative complications, with pneumonia being the most prevalent. The multivariate regression analysis revealed that the number of osteotomy segments, postoperative hematocrit, postoperative Interleukin-6 levels, and weight are predictive risk factors for delayed extubation.
Conclusions
Postoperative hematocrit and Interleukin-6 level, weight, and number of osteotomy segments can serve as independent risk factors for predicting delayed extubation, with combined value to assist clinicians in evaluating the risk of delayed extubation of postoperative congenital scoliosis patients, improving the success rate of extubation, and reducing postoperative treatment time in the intensive care unit.
Keywords
Introduction
Congenital scoliosis is a progressive spinal structural deformity caused by abnormal longitudinal spine growth due to congenital developmental abnormalities. During the growth and development phase, patients experience a progressive deterioration of spinal curvature. 1 If not treated promptly, a substantial percentage of patients may experience a malformation angle exceeding 41° once they reach adulthood, greatly impacting their capacity to lead a typical lifestyle. 2 Generally, the earlier the age at which surgery is conducted for individuals with congenital scoliosis, the more positive results will appear because young people have more spinal flexibility, leading to more efficient corrective effects. 3 Therefore, the optimal age for surgical intervention is commonly considered to be between 4 and 5 years old. 4
However, it is worth noting that in economically underdeveloped areas, many patients often undergo surgery after the rapid skeletal growth period of adolescence, when the development of spinal scoliosis is completed, missing the optimal treatment period. 5 These patients frequently encounter appearance abnormalities, misalignment of the pelvis, neurological impairments, and may even develop cardiovascular and respiratory limitations, which can complicate the surgery, resulting in greater blood loss during the operation, heighten the chances of surgical failure, and increase the likelihood of postoperative complications. 4
Research has demonstrated that the formation of the spine follows a similar pattern to that of other organ systems during the embryonic stage, which means in patients with multi-segmental congenital scoliosis, rib deformities often coexist with vertebral deformities restricting the development of the thorax and lungs, leading to thoracic insufficiency syndrome and reduced lung and heart function.6–9 Relevant epidemiological studies have shown a significant number of individuals with congenital spinal abnormalities frequently exhibit aberrant lung function, including restricted ventilatory impairment and mixed ventilatory impairment. 10 The research conducted by Anastasian et al. has demonstrated a greater occurrence of postoperative pneumonia in patients who undergo multi-segmental spinal surgery and experience delayed extubation. 11 Similarly, Jonathan et al.’s study reveals a notable association between delayed extubation following spinal surgery and a higher frequency of postoperative complications in patients. 12 Patients with congenital scoliosis face an elevated risk of postoperative pulmonary complications due to the complexity of their condition, surgical trauma, extended operation time, and existing pulmonary dysfunction, which further increases the likelihood of failure to withdraw from tracheal intubation after surgery. Moreover, as a result of the high perioperative risk, a significant number of patients necessitate postoperative care in the intensive care unit (ICU).
Delayed extubation commonly refers to the failure to remove a patient from mechanical ventilator support within 24 hours after surgery. 13 In individuals with congenital scoliosis, this delay might result in respiratory-related infections, muscle weakness, malnutrition, and other consequences following surgery. This secondary consequence on patients is the ability to extend their stay in the ICU, escalate the expenses of their treatment, and potentially aggravate their prognosis.
At present, there is a scarcity of research regarding the risk factors that contribute to delayed extubation following surgery for congenital scoliosis. Accurately identifying the risk factors associated with delayed extubation in patients undergoing orthopedic surgery for congenital scoliosis would enable the identification of individuals at high risk and the implementation of appropriate preventative measures to facilitate early removal of the tracheal tube and gradual reduction of dependence on it. Li et al. conducted a study in which they examined the risk factors associated with delayed tracheal extubation following thoracic and lumbar spine surgery in 135 patients without spinal deformities. 14 Nevertheless, the study specifically examined patients who underwent simple decompression and short-segment decompression fusion for degenerative spine diseases. It is important to note that these patients, who are generally healthier, possess greater physiological reserves in different tissues and organs compared to patients with congenital spinal deformities.14,15 Additionally, the surgical trauma experienced by these patients is relatively less severe. The aforementioned considerations render the findings of the above-mentioned study insufficiently relevant for predicting the likelihood of delayed extubation following surgery in individuals with congenital spinal deformity. The objective of this study is to analyze the clinical data of patients who have undergone spinal orthopedic surgery for congenital scoliosis to investigate the risk factors that contribute to delayed extubation after posterior approach surgery and develop a risk prediction model, which will provide theoretical guidance for the early recovery of patients undergoing corrective surgery for congenital scoliosis.
Materials and Methods
This investigation is conducted as a single-center retrospective cohort study. This study encompasses individuals with congenital scoliosis who received orthopedic scoliosis surgery at the First Affiliated Hospital of Xinjiang Medical University from January 2021 to July 2023.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Patients with a confirmed diagnosis of congenital spinal scoliosis necessitating surgical intervention; (2) Surgical intervention performed using the posterior approach of spinal scoliosis orthopedic surgery; (3) Postoperative transfer to the Intensive Care Unit for monitoring and care; (4) Normal preoperative cardiac function (excluding the effect of abnormal cardiac function on delayed extubation).
Exclusion criteria: (1) Patients who have undergone surgical revision or secondary surgery; (2) Patients who have received treatment with growing rods; (3) Patients with preoperative coagulation abnormalities; (4) Patients who are not transferred to the intensive care unit post-surgery; (5) Patients diagnosed with Klippel-Feil syndrome; (6) Patients with incomplete data.
Collection of Clinical Data
Collect data on the following clinical indicators: Age (in years), sex, weight (in kilograms, KG), preoperative comorbidities, duration of anesthesia and surgery (in minutes, min), amount of blood loss during surgery (in milliliters, ml), the volume of autologous blood reinfusion during surgery (in ml), the volume of blood transfusion during the perioperative period (in ml), length of stay in the intensive care unit (in hours), surgical approach, osteotomy site, number of osteotomy segments, osteotomy difficulty level, the volume of allogeneic blood transfusion after surgery (in ml), complete blood count during the perioperative period, coagulation parameters, and occurrence of postoperative complications. The aforementioned data is obtained from the hospital information system (HIS).
Outcome Indicator
The primary outcome indicator being measured is the length of time it takes for patients to remove tracheal intubation. Patients are divided into two cohorts: those who are extubated within a standard timeframe and those who have a delay in extubation, defined as exceeding 24 hours. The secondary outcome indexes include the length of time spent in the ICU following surgery and the presence of postoperative complications, such as pulmonary infection, pleural effusion, coagulation dysfunction, and so on.
Statistical Analysis
The data are examined using R software version 4.3.3. The Shapiro-Wilk test is employed to evaluate the normality of collected data. Continuous data that follows a normal distribution is typically represented as the mean ± the standard deviation. On the other hand, continuous data that does not follow a normal distribution is represented as the median together with the first quartile (Q1) and third quartile (Q3). Categorical data is presented as numbers along with their corresponding percentages. Intergroup comparisons are conducted using statistical tests such as the Chi-square test,t test, or Mann-Whitney U test. Variables that have a significance level of P < 0.05 in the univariate analysis, as well as those that have potential clinical value, are included in a multivariate logistic regression model for further exploration. Based on this, the study developed a prognostic model to predict the likelihood of delayed extubation after surgery in patients with congenital scoliosis, visualized using a nomogram, and evaluated the model’s predictive performance.
Ethical Approval
All procedures are conducted in accordance with the ethical standards of the Declaration of Helsinki. Informed consent is obtained from all subjects and/or their legal guardian. The study design was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University before data collection and analysis (Approval No. 220525-01). All methods are carried out in accordance with relevant guidelines and regulations.
Results
General Information
Single Factors Influencing Delayed Extubation in Patients With Congenital Scoliosis.
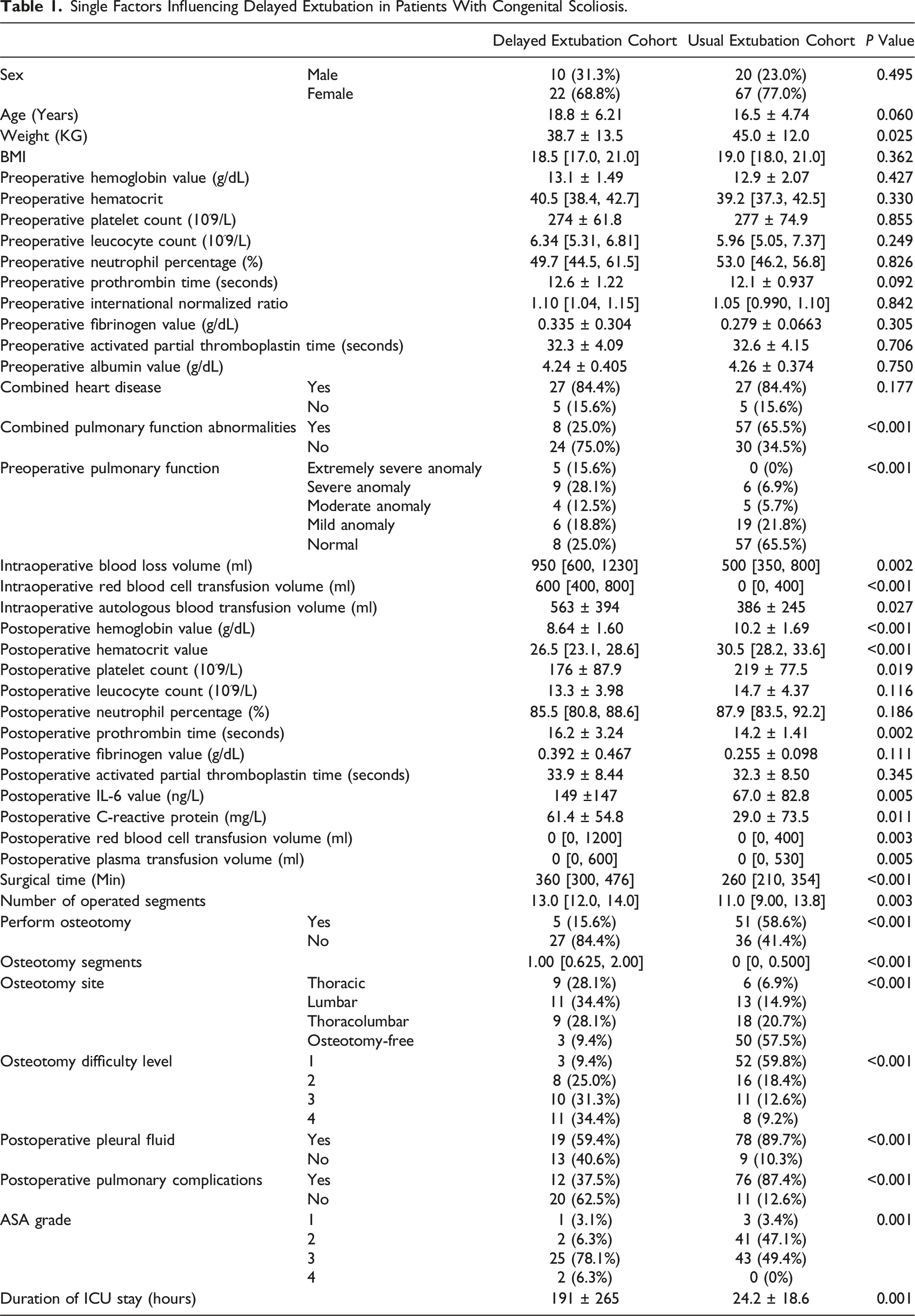
Single Factors Influencing Delayed Extubation in Patients with Congenital Scoliosis
The univariate analysis results show that the following factors are associated with delayed extubation in patients with congenital spinal congenital scoliosis (P < 0.05; see Table 1 for details): body weight, preoperative prothrombin time, preoperative pulmonary function conditions, postoperative hemoglobin value, postoperative hematocrit, postoperative platelet count, postoperative IL-6 value, postoperative C-reactive protein value, postoperative prothrombin time, postoperative albumin level, operative time, the number of the operated segments, whether performed osteotomy, number of osteotomy segments, osteotomy site, osteotomy difficulty level, intraoperative blood loss volume, intraoperative red blood cell transfusion volume, intraoperative autologous blood transfusion volume, postoperative red blood cell transfusion volume, postoperative plasma transfusion volume, whether postoperative pleural fluid, postoperative pulmonary complications, and duration of ICU stay.
Multifactorial Analysis of Factors Affecting Delayed Extubation in Patients with Congenital Scoliosis
Logistic Regression Analysis of Multiple Factors Affecting Delayed Extubation After Surgery in Patients With Congenital Scoliosis.

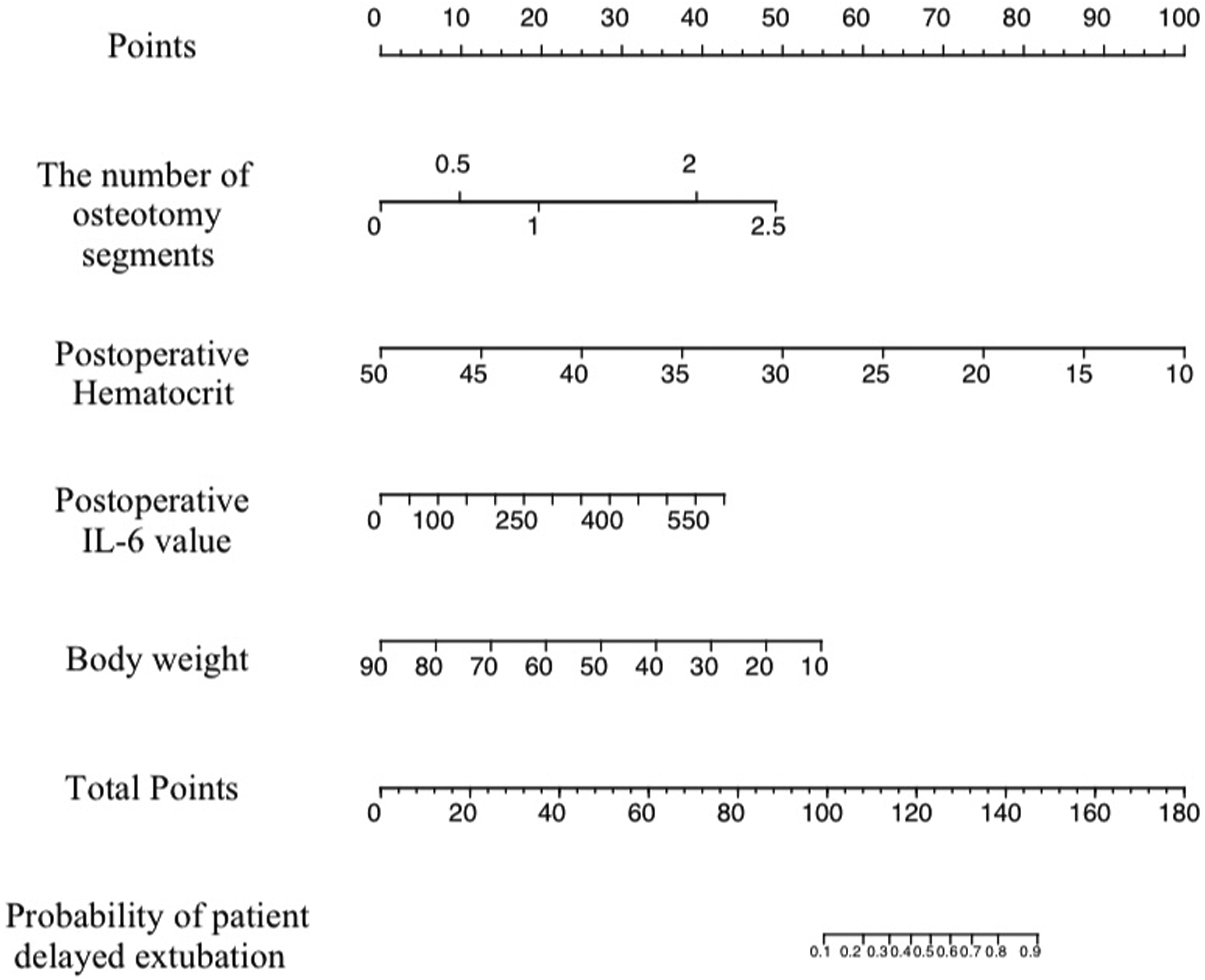
The predictive nomogram of patients with congenital scoliosis at risk of delayed extubation after surgery.
To evaluate the predictive performance of the model, the study plotted the receiver operating characteristic (ROC) curve (Figure 2). The results showed that the area under the curve (AUC) for the standard model is 0.926, with a specificity of 0.753 and a sensitivity of 0.966. The AUC for the number of osteotomy segments is 0.820, with a specificity of 0.765 and a sensitivity of 0.759. The AUC for postoperative hematocrit is 0.785, with a specificity of 0.765 and a sensitivity of 0.724. The AUC for IL-6 is 0.715, with a specificity of 0.776 and a sensitivity of 0.621. The AUC for body weight is 0.672, with a specificity of 0.674 and a sensitivity of 0.655. The ROC curves of risk factors for postoperative delayed extubation in patients with congenital scoliosis.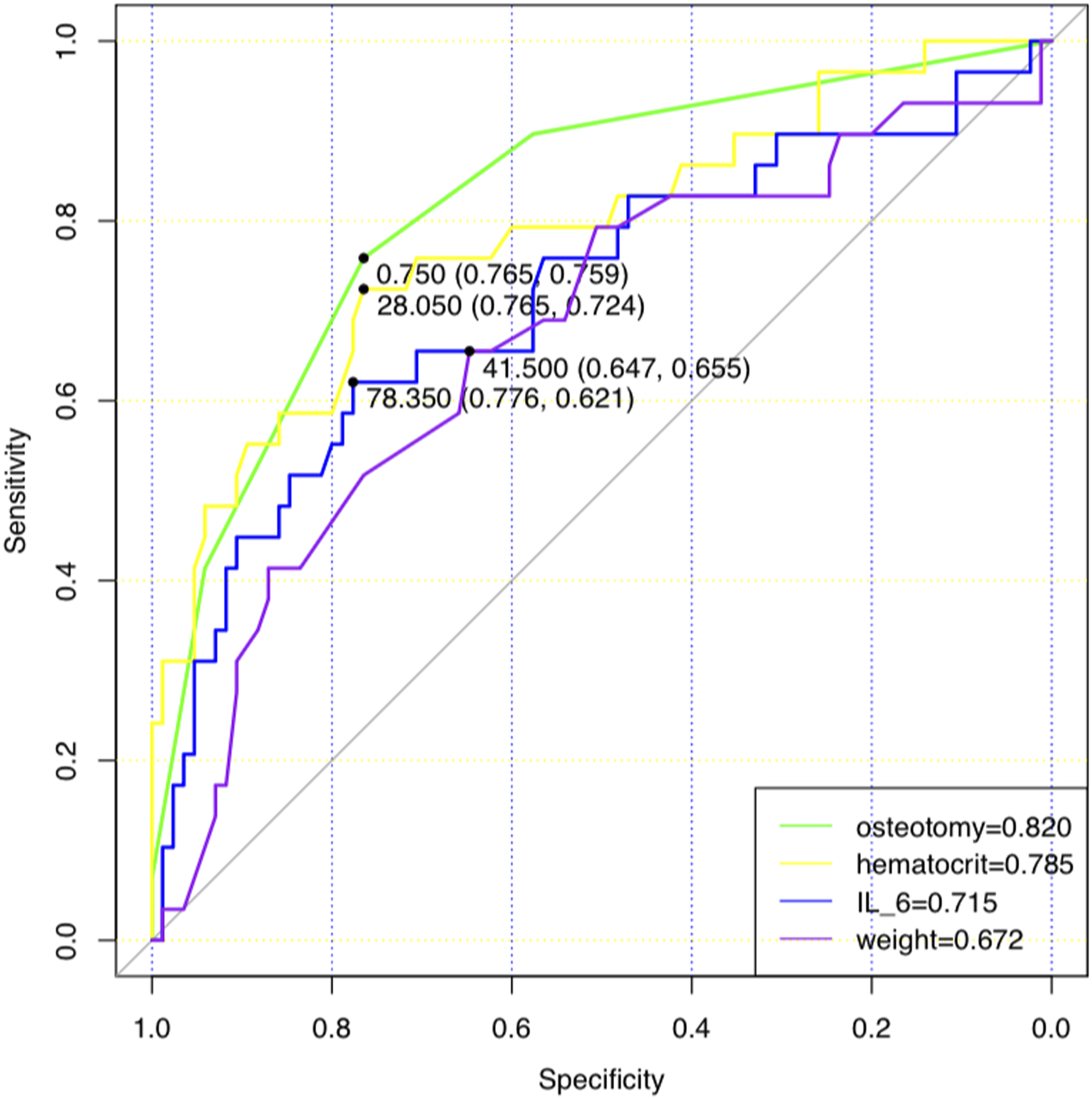
Discussion
Congenital scoliosis is a pathological condition characterized by an atypical sideways or front-to-back curvature of the spine, resulting from a variety of reasons, which includes environmental pollutants, genetic abnormalities, vitamin inadequacies, chemical medicines, or viral infections during embryonic development, poses a challenging treatment scenario because to its intricate nature. 16 If there are substantial spinal deformities or a progressive severe curvature caused, it is advisable to have early surgical intervention in order to stop or restrict the evolution of the spinal deformity. 4 However, due to the multisystem (respiratory system, circulatory system) functional impairments associated with congenital spinal deformities, these patients often experience difficulties in postoperative tracheal extubation compared to ordinary patients, which leads the probability of postoperative complications increases dramatically, resulting in a poorer prognosis. 17 Identifying risk factors that affect the delayed removal of the tracheal tube in patients with congenital scoliosis can contribute to patient recovery and, at the same time, save on hospitalization costs. This study identified several independent risk factors for delayed extubation in patients with congenital scoliosis, including the number of osteotomy segments, postoperative hematocrit levels, postoperative IL-6 levels, and body weight. The nomogram depiction of the prediction model showed an area under the ROC curve of 0.820 for the number of osteotomy segments, 0.785 for postoperative hematocrit, 0.715 for postoperative IL-6, and 0.672 for body weight, which indicates that the model has the ability to accurately forecast the likelihood of delayed extubation following surgery for congenital scoliosis patients. This is important for promptly identifying patients at high risk and enhancing personalized treatment strategies to enhance patient outcomes.
Research indicates that the amount of blood lost after surgery in individuals with congenital scoliosis is mainly influenced by the surgical approach used, the extent of spinal deformity, and the length of the operation, rather than the patient’s age.18–21 Spine osteotomy surgery is considered one of the most challenging directions in the field of spine surgery due to its intricate nature and demanding technical requirements. The complex and distinct anatomical characteristics of the spine and its surrounding structures present a significant danger of neurological and vascular harm during the treatment of spinal deformities. Even small mistakes can result in severe and disastrous outcomes. Generally speaking, the surgical difficulty can be determined by factors such as the number of osteotomy segments executed during the surgery, the surgical approach, and the osteotomy difficulty level. Spinal osteotomy difficulty level can be categorized into 6 stages based on the correctable angle of kyphosis and the number of osteotomy segments, with increasing complexity and higher surgical risks with increasing levels. 22 The osteotomy difficulty level in this study primarily spans from level 1 to level 4. In this study, the single-factor analysis reveals that the above three factors are strongly correlated with delayed extubation, with a P-value of less than 0.001. As the surgical difficulty level increased, the proportion of patients with delayed extubation also increased. Through correlation analysis, the number of osteotomy segments is found to be highly correlated with the osteotomy difficulty. Furthermore, logistic regression analysis demonstrated that the number of osteotomy segments compared to the osteotomy site and the osteotomy difficulty level more accurately predicted the likelihood of delayed postoperative extubation in scoliosis patients, leading to the selection of the number of osteotomy segments as a predictive indicator. The number of osteotomy segments performed is a significant predictor of the likelihood of delayed extubation in patients with congenital scoliosis, which has the highest predictive accuracy among all the parameters studied, with an AUC value of 0.820. The intricacy and duration of surgery in the treatment of severe congenital scoliosis are generally closely correlated with the number of segments of osteotomies performed. Consequently, as the duration of the surgery increases, the patient has a higher amount of blood loss during the operation and a decrease in their hematocrit levels after the surgery. 23 During the perioperative period, patients have bleeding that can be categorized as either overt or occult bleeding, and perioperative occult bleeding is more likely to be missed compared to overt bleeding. 24 The study revealed a positive correlation between the number of osteotomy segments performed during surgery and the amount of occult blood loss experienced by patients after the operation, which may be attributed to factors such as bleeding from soft tissues and osteotomy sites, as well as impaired blood clotting activity resulting from significant blood loss. 25 Consequently, there is a direct correlation between the number of osteotomy segments done and the extent of change in postoperative hematocrit, which aligns with the discovery that both the number of osteotomy segments and postoperative hematocrit are separate risk factors for delayed extubation. It is important to note that the risk of transfusion-related complications may be increased despite the fact that transfusion of blood products can enhance postoperative hemoglobin or hematocrit levels. The hemoglobin data gathered in this study is obtained immediately following transfer to the Intensive Care Unit and is not affected by any blood transfusions given after the surgery. Nevertheless, the administration of blood products after surgery does enhance the hemoglobin levels of the patients. Therefore, additional research should be conducted to examine whether this impacts the time of extubation in postoperative scoliosis patients. Additionally, the intricacy and duration of the surgical procedure not only heighten the likelihood of stress and infection but can also result in diverse postoperative complications during the rehabilitation phase. Hence, the quantity of osteotomy segments serves as a significant metric for evaluating the extent of surgical trauma and the complexity of postoperative recuperation. Martine’s study of risk factors for delayed extubation in patients undergoing general orthopedic surgery also showed that the intricacy of the surgical procedure is a significant determinant of both postoperative recovery and the likelihood of complication appearance, which aligns with the findings of this study. 25
IL-6 is a prevalent cytokine involved in immunological, infectious, and inflammatory responses, as well as participating in physiological functions of the central nervous system, with diverse biological effects.26,27 Studies have demonstrated that IL-6 influences the development of bacterial infectious diseases, and its concentrations are directly associated with the seriousness of the infection, making it a widely used marker for bacterial infection.28,29 Nevertheless, non-infectious factors like surgical trauma can also trigger the immune system, causing the release of inflammatory mediators such as IL-6. 30 This activation promotes the initiation of the immune defense system against external stimulation, resulting in the production of inflammatory factors and the occurrence of an inflammatory response. 31 The AUC for postoperative IL-6 is 0.715, suggesting that the elevated and extended levels of inflammation and stress in patients following surgery are linked to a greater likelihood of delayed extubation. The elevation of IL-6 levels after surgery not only represents the body’s reaction to the surgical trauma but also serves as an indicator of the likelihood of postoperative complications. Moreover, the prolonged presence of the inflammatory response can impact the patient’s lung function recovery, which in turn affects the time it takes for the patient to remove tracheal intubation.32,33 Thus, by the surveillance of postoperative IL-6 levels, physicians can more accurately evaluate the patient’s inflammatory condition and progress in recovery and implement suitable interventions to mitigate the chances of delayed extubation.
Patients with congenital scoliosis frequently have a steady deterioration of the spinal curvature if not treated appropriately, resulting in escalating deformities and a bleak prognosis. 34 These patients sometimes have additional anomalies in other systems, such as the circulatory, respiratory, and musculoskeletal systems, which have a severe impact on their growth and development. 17 Studies have demonstrated that persons who are underweight or extremely underweight have a notably elevated likelihood of acquiring scoliosis in comparison to those with a healthy weight, which suggests a strong correlation between low body weight and the risk of scoliosis. 35 This study reveals that the group of patients who experience delayed extubation has an average body weight of 38.7 ± 13.5 kg, whereas the group of patients who do not experience delay have an average body weight of 45.0 ± 12.0 kg, which indicates that the delayed extubation group has a considerably lower body weight. The delayed extubation group’s lower weight may be correlated with more severe congenital scoliosis based on factors such as surgery time, intraoperative blood loss, and postoperative hematocrit, resulting in more significantly associated detrimental impacts on physical development.
Patients with scoliosis may experience abnormal thoracic development during growth due to anomalies in spinal development, which can impact lung function. This study finds that preoperative lung function can be a reliable indicator for delayed extubation. Univariate analysis shows that impaired lung function is a risk factor for delayed extubation, with the percentage of postponed breathing tube removal increasing as preoperative lung function worsens. All five patients with significant preoperative lung dysfunction in this study experienced delayed extubation post-surgery. However, logistic regression analysis identifies the number of osteotomy segments, postoperative hematocrit levels, postoperative IL-6 levels, and weight as the most reliable predictors for delayed extubation after scoliosis surgery rather than preoperative lung function. This may be due to factors such as the study being conducted at a single site and having a limited sample size. Additionally, the study reveals that the group of patients who experienced delayed extubation following surgery exhibited a higher incidence of postoperative complications, including pneumonia, pleural effusion, and coagulation malfunction. Due to advancements in medical standards and the development and utilization of intraoperative Wake-Up tests and intraoperative neurophysical monitoring, 36 there has been a partial improvement in the likelihood of postoperative spinal nerve problems. Postoperative complications primarily manifest as pulmonary complications, which can be attributed to factors such as extended mechanical ventilation during the perioperative period, compression of the thorax during surgery, and the adverse effects of the surgical position on lung compliance, functional residual capacity, and total lung volume. 37 Excessive fluid and blood transfusion during surgery can lead to immune/volume-related lung injury and compromise the permeability of pulmonary capillaries. 38 In addition, certain patients may potentially encounter postoperative coagulation dysfunction, which could be attributed to significant intraoperative bleeding, depletion of coagulation factors, and dilution of blood due to fluid resuscitation.
The nomogram has emerged as a crucial instrument in data analysis and predictive modeling. It has the ability to convert intricate regression equations into straightforward and viewable graphs, hence enhancing the readability, applicability, and intuitive predictability of the findings obtained from predictive models. 39 The nomogram allows for the obtaining of the scores for each predictive indication, and by combining these scores together, the total score can be computed. This total score can then be turned into the corresponding predicted value, which represents the chance of delayed extubation for patients with congenital scoliosis after surgery. This study demonstrates a specific implementation of the nomogram, which is also an innovation of this research. The nomogram reveals that a patient with congenital scoliosis who undergoes surgery involving two segments of osteotomy (40 points), has a postoperative hematocrit of 30% (50 points), a postoperative IL-6 level of 50 (3.375 points), and a body weight of 50 kg (32.675 points), will have a total score of 126.05, which indicates a delayed extubation risk of approximately 0.6, corresponding to a probability of delayed extubation of around 60%.
However, this study has certain constraints. Given the small number of participants in this retrospective study, which is carried out at a single center, there is a possibility that the selection of the study population may be biased. However, strict inclusion and exclusion criteria were implemented to mitigate this issue. Therefore, additional further research and validation are necessary to confirm the results. Furthermore, alterations in the surgical team’s technical expertise, intraoperative anesthetic management, or criteria for admission to the ICU may have had an impact on the outcomes. Furthermore, the risk factors discovered by the univariate analysis in this study are not completely supported by the multivariate logistic regression analysis, primarily due to the restricted sample size. Therefore, it is imperative to conduct future multi-center investigations with higher sample sizes to confirm the findings of this study. When considering variables for the multivariate logistic regression analysis, the selection included the number of osteotomy segments, postoperative hematocrit, postoperative IL-6, and body weight. The number of osteotomy segments is an indication of the complexity of the surgery and the severity of scoliosis. Postoperative hematocrit is a more sensitive measure than hemoglobin and can also indicate the amount of blood loss during surgery, which may be related to the difficulty of the surgery and the severity of scoliosis. Interleukin-6, as a marker of the stress response to surgical trauma, indirectly reflects the complexity of the surgery. The patient’s body weight is associated with their developmental status, and the severity of scoliosis may also impact their weight. However, it does not use BMI as a measurement because scoliosis can affect the accuracy of height measurements.
Conclusion
Surgical intervention is a crucial therapeutic method for individuals diagnosed with congenital scoliosis. Delayed extubation following surgery is a frequent perioperative problem in these patients, necessitating doctors’ attention and appropriate intervention. Postoperative serum IL-6 level, body weight, number of osteotomy segments, and postoperative hematocrit can independently predict delayed extubation. Combining these factors can improve the accuracy of predicting delayed extubation and increase the success rate of extubation. Furthermore, it is essential to highlight the presence of significant perioperative blood loss and occult bleeding in cases of congenital scoliosis, and preventive actions should be implemented to guarantee the patient’s safety.
Footnotes
Acknowledgments
This study is conducted solely by the authors without any external assistance.
Author Contributions
Study design: Jian Cui, Jingjing Zhang, Yi Wang, and Xiangyou Yu; Data collection: Jian Cui, Wenzhi Li, Wei Liu, and Yixi Wang; Manuscript preparation: Jian Cui, Jingjing Zhang, Yi Wang, and Tao Xu; Data analysis & interpretation: Jingjing Zhang, Wenzhe Li, and Xiangyou Yu. All authors affirm their contributions to the manuscript reviews, involving critical revisions for significant intellectual content, and their approval of the final text for submission. Every author bears the responsibility for the content of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research is conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the National Natural Science Foundation of China (Grant Number: 82160360).
Ethical Statement
Data Availability Statement
The raw data supporting the conclusion of this article will be made available on request.