
Abstract
Objectives
To investigate prospectively the rate of, and factors influencing, delayed extubation following infratentorial craniotomy in a Chinese neurosurgical centre.
Methods
Patients undergoing infratentorial craniotomy for tumour resection were prospectively enrolled and stratified according to whether extubation was attempted in the operating theatre (early extubation) or not (delayed extubation). Pre- and intraoperative variables were collected and analysed. Multiple logistic regression analysis was performed, to identify factors related to delayed extubation.
Results
The study included 800 patients, 398 (49.8%) of whom underwent delayed extubation. The overall rate of extubation failure was 3.6%. Independent factors related to delayed extubation were: preoperative lower cranial nerve dysfunction; hydrocephalus; tumour location; duration of surgery ≥6 h; estimated blood loss ≥1000 ml. Compared with patients in the early extubation group, those in the delayed extubation group had a higher rate of pneumonia, longer intensive care unit and postoperative hospital stays, and higher hospitalization costs.
Conclusions
Brain stem and lower cranial nerve function were the main factors affecting extubation decision-making. Further research is required, to establish criteria for delayed extubation following infratentorial craniotomy.
Introduction
The ideal timing of postoperative extubation following infratentorial craniotomy is unclear. Early extubation allows detection of postoperative neurological complications but may increase the risk of extubation failure.1–3 Delayed extubation has been advocated in high-risk patients, to limit postoperative stress and avoid serious complications such as intracranial haematoma,4,5 but is associated with increases in pneumonia incidence, morbidity, mortality, tracheotomy, length of stay (LOS) in the intensive care unit (ICU), and hospitalization costs. 6
The timing of extubation after intracranial surgery is usually a combined decision, made by the anaesthetist and the neurosurgeon. It has been shown that patients who fail early extubation have more postoperative complications and a higher mortality rate, compared with those in whom early extubation succeeds; 7 physicians may therefore overestimate the harm of early extubation. Criteria for delayed extubation after intracranial surgery have been described in review articles,6,8,9 but prospective studies of the prevalence and factors related to delayed extubation are scarce.
The aims of the present prospective study were to investigate the rate and factors influencing delayed extubation following infratentorial craniotomy in a Chinese neurosurgical centre, in order to provide basic data for further establishment of delayed extubation criteria in these patients.
Patients and methods
Study Population
This observational cohort study consecutively recruited all adult patients (aged ≥ 18 years), undergoing infratentorial craniotomy for brain tumour resection at the neurological ICU of Beijing Tiantan Hospital, Capital Medical University, Beijing, China, between July 2010 and June 2011. Exclusion criteria were emergency surgery and preoperative endotracheal intubation or tracheotomy.
The study was approved by the Institutional Review Board of Beijing Tiantan Hospital, Capital Medical University, Beijing, China. Written informed consent was obtained from all patients prior to enrolment in the study.
Anaesthesia
All craniotomies were performed under balanced general anaesthesia. Patients received 1.0–3.0 mg midazolam via intravenous (i.v.) injection, 30 min before anaesthetic induction with 1.5–2.0 mg/kg propofol i.v. and 3.0–5.0 µg/kg fentanyl i.v. or 0.4–0.7 µg/kg sufentanil i.v. Tracheal intubation was facilitated with 0.1 mg/kg vecuronium i.v. or 0.8 mg/kg rocuronium i.v. Anaesthesia was maintained with sevoflurane in oxygen (end-tidal concentration 1.5–2.0%), propofol (target-controlled infusion at 4.0–5.0 µg/ml), and 0.05–0.3 µg/kg per min remifentanil. Sufentanil or fentanyl were given intermittently during surgery, when increases in the patient’s blood pressure and/or heart rate indicated inadequate analgesia. Vecuronium (0.05 mg/kg bolus) or rocuronium (0.2 mg/kg bolus) were administered according to the results of train-of-four monitoring. The choice of agent was at the discretion of the anaesthetist, but the same analgesic and muscle relaxant were both chosen during the induction and maintenance periods, in individual patients. Propofol and remifentanil infusions were discontinued at the time of dural closure; sevoflurane was discontinued during skin closure.
Extubation
Screening checklist used by the anaesthetist in charge or neurological ICU physician, to determine a patient’s suitability for extubation following infratentorial craniotomy. The answer to all questions must be ‘yes’ in order for extubation to be approved.

F
Patients who remained intubated at the end of surgery were transferred directly to the neurological ICU with manual ventilation and underwent delayed extubation. In these patients, a 30-min spontaneous breathing trial was carried out with a T-piece at pressure support (PS) 8 cm H2O, then the extubation screening checklist (Table 1) was completed by the neurological ICU physician on duty. The neurosurgeon in charge was notified once the patient had passed the screening checklist questions. Extubation was attempted when agreement was reached between the neurosurgeon and neurological ICU physician. Screening was repeated at 0
Re-intubation was performed in any patient who fulfilled at least one of the following criteria: (i) decreased mental status (Glasgow coma scale [GCS] score ≤ 810); (ii) worsened spontaneous respiration; (iii) oxygen saturation <90% despite fraction of inspired oxygen (F
Postoperative Care
Standard clinical monitoring was applied on arrival in the neurological ICU, including five-lead continuous electrocardiography, pulse oximetry, noninvasive blood pressure monitoring, capnography and rectal temperature monitoring. All patients were warmed with a forced-air warming blanket, to maintain a rectal temperature of >36 °C. Analyses of arterial blood gas, serum electrolyte, complete blood count, blood urea nitrogen and blood glucose levels were performed within 2 h of arriving in the ICU. Neurological examinations (GCS score and pupillary examination) were performed every 1 h. Postoperative computed tomography (CT) was carried out in all patients after transfer to the neurological ICU.
Shivering was treated with 0.5 mg/kg meperidine i.v. Persistent systemic hypertension (systolic blood pressure [SBP] >140 mmHg or 20% above preoperative base level, for >5 min) was treated with 0.05–1 mg/kg urapidil i.v. infusion, to a target SBP of 90–140 mmHg or the preoperative level.
All extubated patients received supplemental oxygen by face mask. In patients in whom tracheal intubation continued, mechanical ventilation was performed with an additional inspiratory mixing chamber. Ventilation was supported by synchronized intermittent mandatory ventilation plus pressure support with F
Patients were discharged from the neurological ICU the morning after their physiological status had stabilized, usually with normal neurological, respiratory and haemodynamic status. Patients who underwent endotracheal intubation were not discharged until successful weaning from mechanical ventilation had occurred.
Data Collection and Study Definitions
Data were prospectively collected using a standardized case report form. Preoperative data included: age; body mass index (BMI); sex; history of hypertension (SBP > 140 mmHg), chronic obstructive pulmonary disease (COPD), diabetes or craniotomy; American Society of Anesthesiologists (ASA) physical status. 11 Lower cranial-nerve dysfunction was identified by preoperative routine neurological examination and defined as one or more functional abnormalities of the lower cranial nerves (IX, X, XI or XII). Tumour size and location, and hydrocephalus, were quantified by preoperative CT or magnetic resonance imaging (MRI). The largest cross-sectional diameter of the tumour was used to define tumour size, with >30 mm classified as large, in accordance with another study. 12 Tumour location was classified as brain stem, oppressing the brain stem, or not oppressing the brain stem.
Intraoperative data included duration of surgery, fluid balance, estimated blood loss, and use of analgesics and muscle relaxants.
Extubation outcome, reoperation, postoperative pneumonia, ICU and postoperative hospital LOS, and hospitalization costs were also recorded. Failed extubation was defined as the need for tracheal reintubation or tracheotomy ≤48 h after extubation for any reason but reoperation. Pneumonia was defined according to the national nosocomial infections surveillance system definition. 13 Glasgow outcome scale (GOS) scores at discharge were categorized as unfavourable (1–3) or favourable (4–5). 14 ICU LOS was categorized as ≥24 and <24 h.
Statistical Analyses
Patients were stratified according to whether extubation was attempted in the operating theatre (early extubation) or not (delayed extubation). Categorical data were shown as a percentage and analysed by the χ2-test, with the exception of small-size data that were analysed using Fisher's exact test. Continuous data were checked for normal distribution and presented as mean ± SD or median (interquartile range), as appropriate. Comparison of continuous data was performed using Student's t-test for normally distributed variables and Mann–Whitney U-test for non-normally distributed variables. Univariate analyses were performed, followed by multiple logistic regression analyses to identify factors related to delayed extubation. Pre- and intraoperative factors were analysed as predictors of delayed extubation, and factors with a P-value < 0.05 were included in multivariate analysis (stepwise forward logistic regression), to identify the independent factors of delayed extubation. Statistical analyses were performed with SPSS® software, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. A P-value < 0.05 was considered statistically significant.
Results
During the study period, 2269 adult patients who underwent elective craniotomy were transferred to the neurological ICU for postoperative care. Of these patients, 800 fulfilled the inclusion criteria and were enrolled into the study (300 males/500 females; mean age 44.8 ± 13.2; age range 18–81 years; early extubation n = 402, 50.3%; delayed extubation n = 398, 49.8%). Successful extubation occurred in 396/402 (98.5%) of patients in the early extubation group and in 358/398 (89.9%) of patients in the delayed extubation group (P < 0.001). The overall rate of extubation failure was 3.6% (29/800). Figure 1 depicts the patient flow and provides additional details of the study.
Screening, recruitment and outcome of patients recruited to a study investigating factors influencing delayed extubation after infratentorial craniotomy.

Data presented as median (interquartile range) or n (%) of patients.
Extubation in neurological intensive care unit.
Extubation in operating theatre.
χ2-test for categorical data; Mann–Whitney U-test for continuous data.
Any functional dysfunction of the lower cranial nerves (IX, X, XI or XII).
NS, not statistically significant (P ≥ 0.05); BMI, body mass index; COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiologists.
Stepwise forward regression analysis to identify factors independently associated with delayed extubation a in patients undergoing infratentorial craniotomy for brain tumour resection (n = 800).

Extubation in neurological intensive care unit.
B, regression coefficient; SE, standard error; CI, confidence interval.
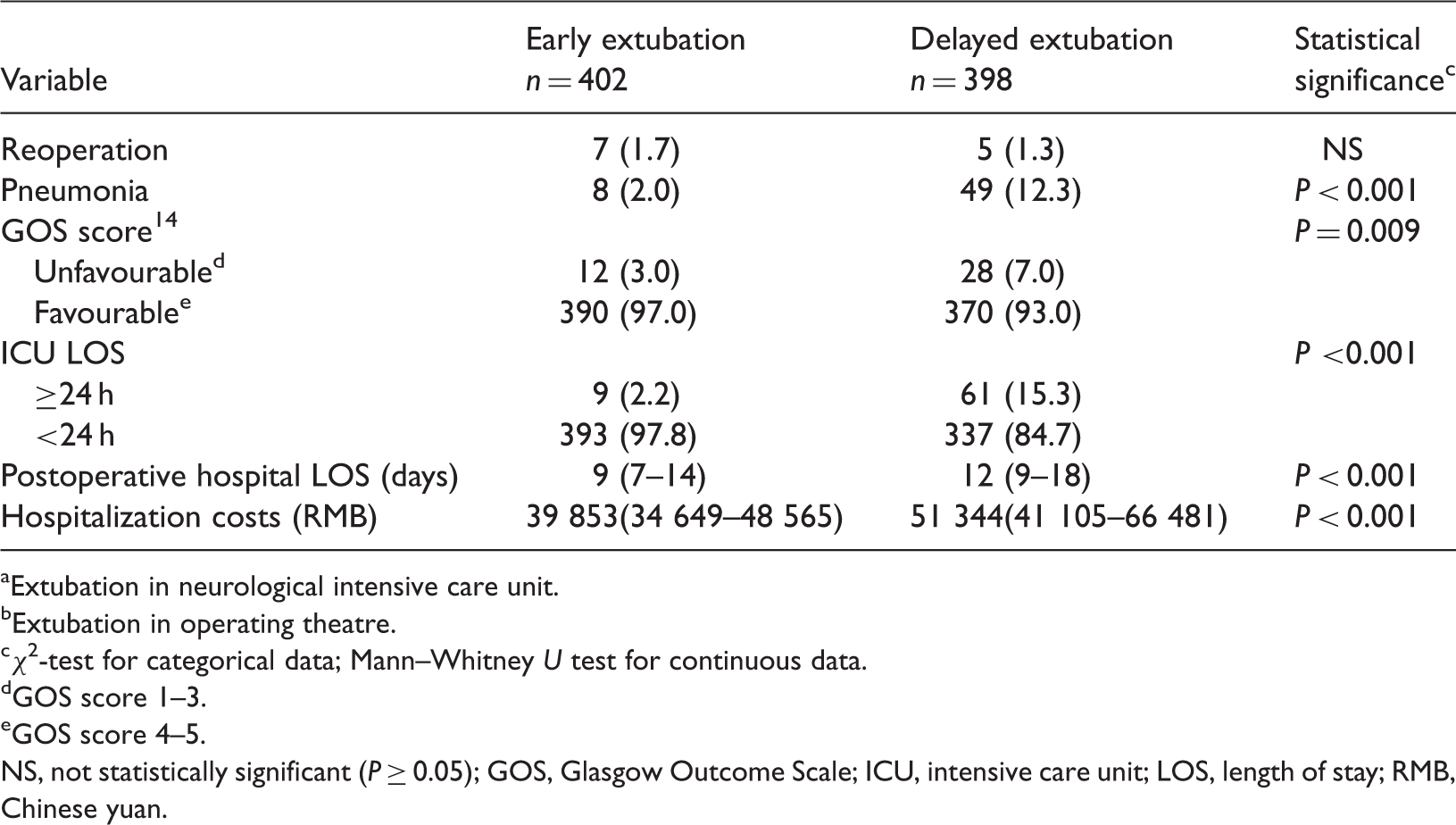
Extubation in neurological intensive care unit.
Extubation in operating theatre.
χ2-test for categorical data; Mann–Whitney U test for continuous data.
GOS score 1–3.
GOS score 4–5.
NS, not statistically significant (P ≥ 0.05); GOS, Glasgow Outcome Scale; ICU, intensive care unit; LOS, length of stay; RMB, Chinese yuan.
Discussion
There are no well-accepted criteria for determining the optimum timepoint for extubation after infratentorial craniotomy. The proportion of patients who underwent delayed extubation was 49.8% in the present study, but other centres have reported rates of 18% 15 and 10%. 16 It has been suggested that patients who undergo posterior fossa surgery should be extubated only after they have fully recovered from anaesthesia, at least 1–2 h postoperatively. 9 In addition, if there is any doubt about the integrity of bulbar function, the endotracheal tube should be kept in place for 24 h after surgery. 17 The high rate of delayed extubation in the present study suggests that the decision-making process in the authors’ study centre may be over-conservative. It should be noted that 69.9% of patients included in the present report had tumours ≥30 mm in diameter, which is a higher rate than the 54% incidence reported elsewhere. 12 It is possible that patients in developing countries are likely to present with lesions that are more severe, compared with those that are seen elsewhere, but this hypothesis remains to be tested.
The rate of extubation failure in the early extubation group in the present study was 1.5%, which is comparable with the 0.8% failure rate reported by Cata et al. 15 The failure rate in the delayed extubation group (which excludes those in whom extubation was never attempted) was 6.0% in the present study, which is lower than the 8.2% reported elsewhere, in critically ill patients with brain injury. 1 A study including 378 patients intubated for >6 h in the neurological ICU found an extubation failure rate of 16.8%. 2 Others have reported extubation failure rates of 10–15% in mechanically ventilated patients (as reviewed by Boles et al.). 18 Few studies have investigated the rate of extubation failure in patients with delayed extubation after infratentorial craniotomy, however. 15
Extubation after craniotomy is a two-step process. The first step is to decide whether the patient is fit to undergo extubation, and the decision is largely determined by the subjective opinions of clinicians.8,19 The second step uses a checklist (such as that shown in Table 1) to decide whether to proceed with extubation, and is therefore less likely to be affected by subjective opinions. The objective of the present study was to investigate the factors involved in the first step of the decision-making process. In cardiac surgery these factors are largely associated with preoperative cardiac function and intraoperative parameters, such as duration of surgery and blood loss.20–22 The present study determined that preoperative lower cranial nerve dysfunction, hydrocephalus and tumour location were independent factors in predicting delayed extubation after craniotomy. Lower cranial nerve function is a major concern of medical staff, because tumours within (or involving) the brain stem usually impair the respiratory centre, and lower cranial-nerve dysfunction may occur because of brain stem involvement. 17 These patients should be carefully evaluated in order to avoid extubation failure and possible tracheotomy. Complicated surgical procedures are associated with extended duration of surgery and increases in fluid administration, blood loss and drug consumption, elevating the risks of cerebral oedema, delayed recovery and delayed extubation.15,23 The findings of the present study provide basic data for further establishment of delayed extubation criteria in patients undergoing infratentorial craniotomy.
Early extubation was associated with a significantly lower rate of postoperative pneumonia than delayed extubation in the present study, suggesting that prolonged intubation might increase the risk of pneumonia. In a finding similar to others, delayed extubation in the present study was associated with significantly longer durations of stay in the ICU and hospital, and (consequently) higher hospitalization costs than early extubation.16,24,25 It is possible that these differences are related to disease severity, as patients in the delayed extubation group were more likely to have preoperative lower cranial nerve dysfunction, hydrocephalus and large tumours than those in the early extubation group.
This study had several limitations. First, it was a single centre study: the results therefore reflected the experience of one hospital and cannot be directly applied to other institutions. Nevertheless, we strongly encourage medical teams to conduct similar evaluations in their own centres to define the best strategy for neurosurgical patients. Secondly, the study population was limited to patients who underwent infratentorial craniotomy, with the result that a large proportion of patients had brain stem or lower cranial-nerve involvement: this may have obscured the effects of other variables. Thirdly, it was not possible to identify correlations between the study variables and extubation failure, which would have been extremely useful to clinicians. Further studies are required to establish extubation criteria after infratentorial craniotomy.
In conclusion, delayed extubation was performed in 49.8% of patients who underwent infratentorial craniotomy in our hospital. The main factor in determining when to extubate is the relationship between the tumour and brain stem, and lower cranial nerves. The findings of this study provide basic data for further establishment of criteria for delayed extubation, in patients undergoing infratentorial craniotomy.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Beijing Municipal Health Bureau, Beijing, China (2009-03-28).