
Abstract
Study Design
Narrative review.
Objective
We aimed to propose the classifications of, risk factors for, and prevention strategies for perioperative complications from previously published papers in adult spinal deformity (ASD) surgeries.
Methods
A literature search was conducted in the PubMed/MEDLINE database to identify studies reporting perioperative complications of spinal deformity surgery, their classifications, risk factors, and prevention strategies. Main search terms included “perioperative complications”, “medical complications” and “adult spinal deformity”. In the various complications associated with deformity surgeries, we focused the medical complications which will directly link to patient’s life prognosis rather than postoperative mechanical complications.
Results
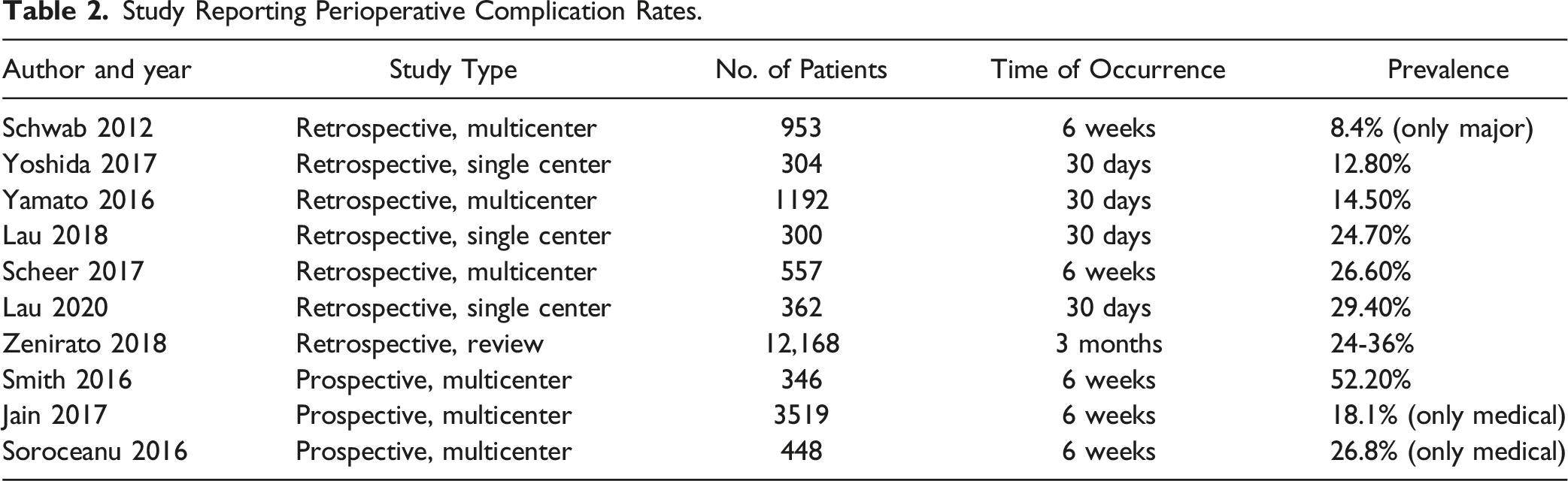
The overall perioperative complication rate ranged from 12.8% to 52.2%. Risk factors for perioperative medical complications included age, body mass index, osteoporosis, frailty, comorbidities, preoperative medication, smoking habit, and alcohol intake. Perioperative medical complications mostly depend on patient-related factors. Taking reference from the previous reported classification of surgical complications, the AO Spine Deformity Knowledge Forum developed a classification for complications of spinal deformity surgery via a Delphi exercise.
Conclusion
Complication classification system is important for understanding the impact of complications on patients. Further research should aim to determine the correlation between the new complication classification and patient outcomes in spinal deformity surgery. Various pre-, intra-, and postoperative strategies should be implemented to prevent perioperative complications.
Keywords
Introduction
Surgeries can provide better clinical, radiographic, and health-related quality of life (HRQOL) outcomes than nonoperative treatment for adult spinal deformity (ASD),1-3 but spinal deformity surgeries are often complex and may be exposed to high risks of perioperative complications.4-7 Previous studies of perioperative complications of spinal deformity surgery showed significant variability in complication rates, classifications, risk factors, and prevention strategies.4,8-18 This may be caused by the lack of uniformed assessments of etiologies (degenerative vs idiopathic), surgical procedures (with vs without three-column osteotomy [3-CO]), and revision status. In addition, reporting of patient- and procedure-related complications in previous studies varied by time (within 30 days, 6 weeks, 2 months, or 3 months after surgery), types (medical vs surgical, neurologic vs non-neurologic), and severity (minor vs major).4,8-14,16
Medical complications affect life support systems which impact patient’s life prognosis rather than surgical/mechanical complications. ASD surgeries were usually much more invasiveness to the patients than general spinal surgery. Prognosis prediction for patients considering surgery is essential to determine indication and informed consent for the patients,
Therefore, this review was conducted to propose the classifications of, risk factors for, and prevention strategies for medical complications from previously published literatures in ASD surgeries.
Methods
A literature search was conducted in the PubMed/MEDLINE database to identify studies reporting perioperative complications of spinal deformity surgery, their classifications, risk factors, and prevention strategies. The Scoli-RISK-1 study was a multicenter prospective study organized and conducted via the AO Spine Knowledge Forum platform to assess the surgical outcomes of spinal deformity surgery. The final search terms were: (“perioperative complications” AND “adult spinal deformity”) OR (“medical complications” AND “adult spinal deformity”). Inclusion criteria were: (1) published in English, (2) mean or median follow-up of at least 1 year, (3) studies reporting perioperative complications occurring within 30 days and (4) studies of classifications of or prevention strategies for medical complications in spinal deformity surgery. Regarding the timing of adverse event (AE) occurrence, perioperative AEs were categorized into occurring intraoperatively, within 30 days, within 6 weeks, and within 3 months of surgery. Perioperative complications caused by patient- and procedure-related factors were categorized as medical and surgical complications, respectively. We excluded the term “mechanical complication” from the classification as it is captured by surgical complications.
Results
Complication Classification Systems
Complications of spinal deformity surgery may have a significant impact on clinical outcomes, healthcare costs, and HRQoL.19,20 According to Appropriate Use Criteria, appropriate surgeries are procedures of which the expected health benefits outweigh the expected health risks by a wide margin. 21 A classification predictive of the impact of complications on various outcomes, such as length of hospital stay, healthcare costs, and clinical outcomes, would be useful for quality initiatives, protocol development, and clinical research. There were several classifications system for perioperative complication in ASD surgery. The Spine Adverse Events Severity System (SAVES) was reported by Degenerative Spine Study Group (DSSG) and Spine Trauma Study Group (STSG) in 2010 22 and modified as version 2 in 2016. 23
SAVES is a relatively simple, reliable for identifying AEs in degenerative or traumatic condition of spinal surgery, that takes into account the effect of the AE on length of stay (LOS). However, it does not focus on ASD surgery. International Spine Study Group and AO spine published an ASD specific ISSG-AO Multi Domain Spinal Deformity Complication Classification System which in 2020. 24
AO Spine Deformity Knowledge Forum Classification of Complications of Adult Spinal Deformity Surgeries.
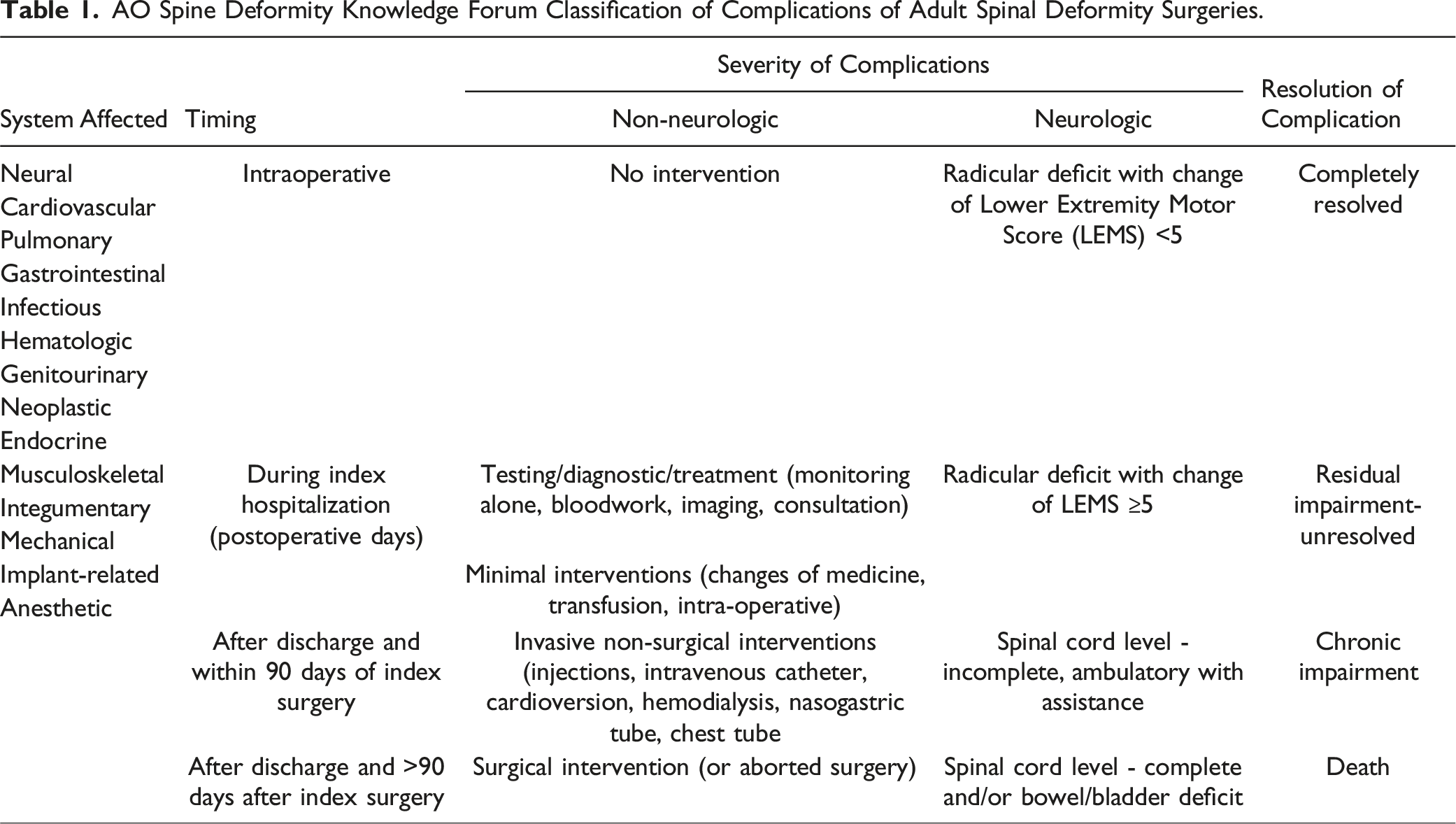
The time of occurrence of complications is important to guide prevention strategies and to develop risk-sharing protocols in alternative payment models. Risks of complications occurring at different timings can be minimized using different protocol-based care plans. Protocols of intraoperative standardization can significantly lower the risk of intraoperative complications.26,27 Perioperative complications can be minimized by protocols of preoperative optimization and enhanced recovery after surgery.28,29 Surgical strategies including circumferential fusion and instrumentation techniques may have a significant impact on late postoperative complications such as pseudarthrosis, implant failure, and junctional complications.30-32
Assessing the severity of complications is important for evaluating the expected impact of complications on clinical and patient outcomes. Glassman et al. found that major complications had a measurable impact on patients’ health status at 1 year after surgery, while minor complications did not. 5 However, the value of classifying complications as major and minor is limited because there is a poor correlation between this classification and patient outcomes, patients’ perception of complications, and changes in health status.33-35 Clavien and Dindo developed and validated a classification of complications in surgery based on the intensity of therapy required to treat the complication. 36 Their goal was to eliminate the use of subjective terms such as major vs minor and severe vs non-severe.37,38 The AO Spine Deformity Knowledge Forum classification adopted the Clavien-Dindo classification to describe non-neurologic complications (Table 1).
Complication Rates
Study Reporting Perioperative Complication Rates.
Risk Factors for Medical Complications
Perioperative complications can be categorized as medical or surgical and major or minor, each of which could be influenced by different risk factors. Risks of perioperative medical complications are largely influenced by patient factors, including age, body mass index, osteoporosis, frailty, comorbidities (the American Society of Anesthesiologists [ASA] physical status classification, craniocervical instability, hypertension, heart disease, depression, diabetes, anemia, malignancy, etc.), preoperative medications (anticoagulant, antihypertension, and antibiotics), smoking habit, alcohol intake, etc.4,10-14,16,40
Discussion
Surgical Site Infection (SSI)
SSI is associated with significant healthcare costs of spinal deformity surgery.51,52 Generally, SSI has been categorized as early or late infection; however, their definitions varied in studies. Early infection was often defined as infections occurring within 30 days or 6 weeks of surgery. Early infection rate ranges from 1.7% to 10.7%7,9,13,53-56 and from 2% to 7.6% in patients undergoing 3-CO.7,49,57-59 Late infection was found to be less common than early infection.9,60 Apart from well-known factors such as diabetes and obesity, risk factors reported in previous studies included revision surgery, prior SSI history, mental illness, a higher ASA grade, existing kyphosis, age, and 3-CO.7,13,56,58,61-63 In addition, patients undergoing vertebral column resection or multilevel 3-COs are also at a higher risk of SSI.58,59 Experience of the surgeon has also been identified as a risk factor for superficial but not deep SSI. 54 SSI is associated with prolonged hospital stay and is one of the most common causes of readmission within 30 days of surgery. 64 A case-control study showed that SSI significantly affected patients’ HRQoL and increased the risk of more complications such as wound problems or proximal junctional failure at 1 year of surgery; however, its negative impact appeared to be diluted at 2 years of surgery. 65
Vancomycin powder is considered a potential prophylaxis for SSI. Although a few meta-analyses supported its effectiveness and safety, its use is still controversial in spinal deformity surgery.66-68 Most of authors performed a study testing Vancomycin powder in surgical site before wound closure on the effect of SSI for spinal surgery. Negative pressure wound therapy is a treatment modality which could potentially reduce the risks of SSI and wound dehiscence. 69 Minimally invasive surgical technique of posterior instrumentation could also potentially reduce the risk of SSI. 70 In recent years, major organizations (American College of Surgeons and Surgical Infection Society, World Health Organization, and Center for Disease Control) announced new prevention and treatment guidelines for SSI and introduced a series of new treatment modalities that are supported by clinical evidence for preventing SSI. Apart from parenteral prophylaxis of antibiotics, these treatment modalities include alcohol-based skin preparation, perioperative glucose control, temperature regulation, and pre- and postoperative tissue. 71 The effectiveness of these treatment modalities in spinal deformity surgery has not been proven and will require future research to confirm.
Urinary Tract Infection (UTI)
Urinary Tract Infection (UTI) is one of the major perioperative complications in hospitalized post-operative spine patients. Increased risk of UTI is noted in ASD patients, particularly women, and is likely associated with decreased mobility related to higher degrees of spinal invasiveness. In spine cohort, .88% incidence of UTI was reported in 289,121 spine surgeries. 72 The inpatient UTI cohort had significantly longer operative time, more fusion procedures, more posterior procedures, and more procedures involving the lumbar levels than the post-discharge cohort. 72 Another study noted that the risk factors of UTI were patient’s comorbidities, longer operative time, large blood loss or ASA 3. 73 The management for UTI were early mobilization, increased water intake and antibiotics for target bacteria. 73
Respiratory and Pulmonary Complication
Respiratory and pulmonary complications can occur intraoperatively, such as intraoperative pneumothorax, or postoperatively, such as pneumonia, acute respiratory distress syndrome (ARDS), and respiratory failure. Smith et al. reported that respiratory and pulmonary complications were the most common cause for mortality after scoliosis surgery. 48 Men and patients with mental illness are at higher risks of respiratory and pulmonary complications.50,63
Rates of common perioperative pulmonary complications are .3% to 5.9% for pneumonia, and 4.3% to 4.7% for ARDS.4,7,12,49,53,55,60 An analysis of a national database in the US showed that the incidence of ARDS and pulmonary complication increased from 2003 to 2010. 74 Patients undergoing revision surgery have a higher risk of ARDS. 61 There are concerns over intraoperative pneumothorax in patients undergoing 3-CO in the thoracic region, with an incidence of 1.2%. 49
Deep Venous Thrombosis (DVT) and Pulmonary Embolism (PE)
The reported incidence of DVT and PE in spine surgery range from 4.3% to 15.4 and .2% to 3.2%, respectively.75-77 Patients with veinous thrombosis events include DVT and PE had a longer hospital stay and a higher mortality rate compared with non DVT/PE patients. There were several prevention methods for venous thrombosis that include prophylactic anticoagulation, compression stockings, and intermittent pneumatic compression (calf-thigh pump). Anticoagulation therapy include vitamin K antagonists, unfractionated heparin, low-molecular-weight heparin, anti-platelet and anti-factor Xa. Low molecular weight heparins are the current preferred pharmacological treatment in DVT prevention. Mechanical prevention with compression stockings are generally well tolerated by the patients. Intermittent pneumatic compression increases the venous blood flow velocity and as a result, can minimize the development of blood clots in deep vein. and may reduce distal DVT. However, mechanical prevention is generally not sufficient and the addition or sole use of pharmacologic prophylaxis is recommended to significantly reduce the prevalence of deep venous thrombosis. 78 Controversies exist related to the need for intra-op use, timing in initiating pharmacological treatment post-operatively, and duration and dosage. Balancing the risk of epidural hematomas from the use of anticoagulatants and the need for DVT prevention is often dealt with on a case by case basis by the treating physicians.
Delirium
In elderly population, postoperative delirium is one of the most common complications after spinal fusion, with the incidence rates of post-operative delirium ranged from .84% to 21.3% in patients undergoing spinal surgery.79-82
Reported risk factors for postoperative delirium included age, length of surgery, amount of intraoperative blood loss, intraoperative hypotension <80 mmHg, prescription medications and peri-operative narcotic use.83,84
Furthermore, intraoperative autologous and allogenic blood transfusions have been associated with increased risk of postoperative delirium following complex spinal fusion for ASD. 85 Additionally, the number of prescribed medications and intraoperative opiate analgesic drug were predictors of postoperative delirium. 86 Intra-operative medications required to control pain during ASD surgeries, including narcotics and ketamine, are associated with post-operative delirium. The American Pain Society released guidelines for the management of postoperative pain emphasizing multimodal approaches and minimizing the use of opioids. 87 Postoperative electrolyte disorders (hyponatremia and hypocalcemia) are risk factors for postoperative delirium in patients undergoing orthopedic surgeries. 88 Therefore, adequate medical work-up, including electrocardiogram and bloodwork, is required in the management of patients with delirium to rule out and manage any reversible causes.
Gastrointestinal Disease
Gastrointestinal diseases (GI) were one of the major complications after complex spine surgery. GI includes ileus, enteritis, mesenteric ischemia, and gastroesophageal reflex disease.89,90 Postoperative ileus (POI) is an abnormal pattern of gastro-intestinal motility, that cause nausea, vomit-ing, inability of oral diet, abdominal distension or delayed passage of stool. The incidence of POI was reported to relatively common, ranging from 2.6% to 8.4%. 91
Longer surgical time larger estimated blood loss, surgery with an anterior approach, lower BMI, and a history of smoking were also increasing the risk of POI. The risk factors of for post-operative ileus include male sex, large surgical invasiveness and anterior approach, and may be correlated with patient health before surgery. Hypokalemia is common and can be associated with serious adverse consequences, including paralysis, ileus, and death. 92
The problem is compounded by peri-operative narcotic use. Recognition of the possibility of Ogilvie’s Syndrome, dilatation of the cecum in the presence of a competent iliiocecal valve, can help prevent bowel perforation in this setting.
Prevention Strategies for Perioperative Complications
Specific medical complications and major prevention strategies were summarized in Figure 1. We divided the general prevention strategies to preoperative, intraoperative and postoperative strategies as followings. Medical complications and prevention startegies.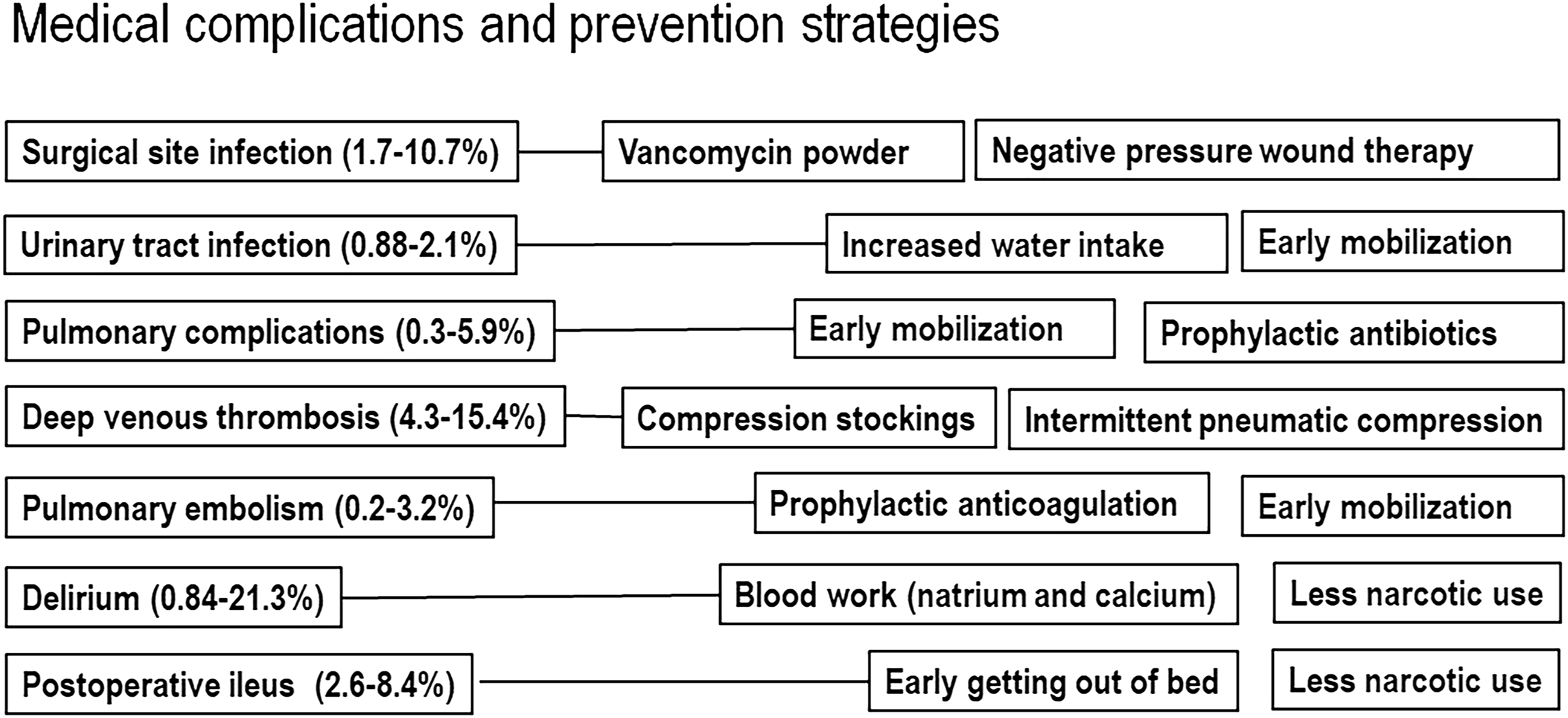
Preoperative Strategies
Prevention of complications begins in the preoperative period and includes careful patient selection, optimization of modifiable risk factors, and thorough surgical planning.
The appropriate selection of patients with ASD that should and could be treated with major spinal surgery is challenging but critical to avoid complications. 93 This process should include careful consideration of the patient’s age, comorbidities, frailty, neurologic status, functional status, and type/degree of spinal deformity.2,93 In less severe cases of ASD, nonoperative treatments such as physical therapy, pain medications, and injections should be exhausted before considering surgery. 94 Ultimately, the surgeon and patient should participate in a shared decision-making process in which the benefits of the treatment tailored to the individual patient are weighed against its risks.
Patient optimization, which is the effort to normalize patients’ preoperative lifestyle and health risk factors, has a major impact on patient outcomes and the risk of complications. 95 Optimization should include cessation of smoking whenever feasible, management of alcohol/opioid/other drug dependence, cardiac assessments to determine the risk of surgery and potentially to identify reversible ischemia, medication review and adjustments, as in the case of anticoagulants, and normalization of biochemical parameters such as bone mineral density, blood glucose or hemoglobin A1C, electrolytes, coagulation factors, platelets, and hemoglobin. The value of preoperative nutrition, physical fitness, and psychiatric wellness has been understudied, but their optimization may potentially facilitate postoperative recovery and mitigate the risk of perioperative complications.
Surgical planning for deformity correction is a complex process of incorporating a series of measurements to decide on how the correction will be achieved. 96 Images should be carefully studied for neural element compression and vascular structures. 97 Preexisting neurologic deficits must be identified and documented as they add insight into the elements requiring decompression. Furthermore, all relevant measurements should be obtained, including pelvic parameters, sagittal angles, coronal angles, and pedicle dimensions. 96
Surgeons can choose from a wide variety of approaches, techniques, and devices, but evidence is scant to guide treatment selection for individual patients. The choices of surgical approach, instrumented levels, type(s) of osteotomies, and interbody implants usually come down to the surgeon’s experience and expert opinion. The classic open posterior midline approach can be supplemented or supplanted by anterior or lateral interbody fusions and minimally invasive surgery approaches. 3-COs are known to substantially increase postoperative morbidity and mortality and therefore, should be reserved for patients that cannot be adequately treated with simpler and safer methods such as posterior column osteotomies. 49 Ultimately, the surgeon must perform a balancing act by weighing all measurements, patient factors, treatment options, and risks to create a viable treatment plan that maximizes the likelihood of a good outcome.
Intraoperative Strategies
The procedure begins with positioning, which includes planning for the spinal correction (eg, open frame or motorized table) and avoiding skin ulcers, peripheral nerve compression palsies, and abdominal compression that can cause venous hypertension. 98 From the initial incision onward, strict minimization of blood loss should be a top priority as it helps avoid numerous medical complications such as cardiac issues, disseminated intravascular coagulation, coagulopathy, and transfusion-related complications. 74 Although safety should not be compromised for speed, the surgeon should also aim to be efficient as shorter operative time has a strong association with less blood loss and fewer infections. 99 Exposure and laminectomy should be performed cautiously to avoid dural tears, particularly in the context of history of previous surgery, severe stenosis, spondylolisthesis, synovial cysts, and ossified ligamentum flavum.100101,102 Finally, wound closure requires the same level of attention and discipline as the rest of the procedure as large incisions are at high risks for breakdown, dehiscence, and infections. Multi-layer water-tight closure is important, and skin sutures appear to perform better than staples. 103 Strategies such as placing local vancomycin powder, reinforcing the fascia with nonabsorbable sutures (eg, Ti-cron), sealing the wound with cyanoacrylate glue (eg, Dermabond), and applying antibiotic ointment over the wound may also be beneficial, and require further study.
Postoperative Strategies
The postoperative care of patients after major deformity surgery has implications for preventing complications and optimizing outcomes. It may be advisable to routinely admit these patients to a critical care unit for optimal respiratory, hemodynamic, and medical care. If a neurologic injury or suspected injury (eg, loss of motor evoked potentials) occurs intraoperatively, admission to critical care and optimizing mean arterial pressure targets for up to 1 week are indicated. 104 An ideal hemoglobin target has not been well established, but avoidance of severe anemia is key to minimizing cardiac risk during the immediate postoperative period, and a higher target may be helpful to improve tissue oxygen delivery. Postoperative bracing may help avoid early instrumentation and mechanical complications due to excessive stress on the construct and bone-hardware interface, however, there is limited research to support it use. In addition, the roles of early mobilization, physical therapy, fall prevention, and intensive inpatient rehabilitation programs are not well established, but may have potential in reducing early complications. 105
Future Directions
Spinal deformity surgery is rapidly evolving with new implants, techniques, tools, and technologies. The majority of these developments aim directly at reducing complications. One of the difficulties in this field is the proliferation of numerous different methods to achieve the same goal, which makes it difficult to study and even more so, to apply evidence-based decision making. Future studies need to establish the safety of each novel technique and subsequently compare their complications, clinical outcomes, radiographic outcomes, and longevity. High quality investigator-driven prospective multicenter data that encompass all techniques to treat ASD and capture both academic and community surgery practices need to be collected. 9
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.