
Abstract
Study Design
Retrospective case series.
Objective
To assess the utility of postoperative computed tomography (CT) following anterior cervical diskectomy and fusion (ACDF) and to determine the clinical circumstances most likely to lead to an abnormal CT scan.
Methods
Patients who underwent ACDF at a tertiary center over a span of 5 years were investigated. Only patients who had a minimum of 6 months’ postoperative follow-up and a CT within 2 years after the surgery were included in the study group. All the postoperative notes were reviewed to determine indications for the CT, abnormalities identified, and whether the scan led to an alteration in the treatment course.
Results
The charts of 690 patients who underwent ACDF were reviewed. Of the 690 patients, 45 (7%) had postoperative CTs. These patients accounted for 53 postoperative CT scans, 45 (85%) of which were taken for patients who expressed persistent postoperative symptoms and/or had abnormal imaging. There were no indications for 8 (15%) of the CTs. Patients who had a CT for persistent symptoms and/or abnormal preliminary imaging were significantly more likely to have an abnormal CT (p = 0.03) and/or an alteration in treatment course (p = 0.04) compared with those with no symptomatic or radiologic indication for CT.
Conclusions
CT is associated with minimal utility regarding the alteration of treatment course when employed in asymptomatic patients. Postoperative CT should be ordered solely for symptomatic patients or those with other abnormal preliminary imaging. Judicious use of postoperative CT will limit the radiation exposure and cost.
Introduction
Anterior cervical diskectomy and fusion (ACDF) is commonly used as a surgical treatment for symptomatic cervical disk herniation and cervical spondylosis that is refractory to conservative management. 1 , 2 Following ACDF, imaging modalities such as standard radiography and computed tomography (CT) are used to assess the fusion, instrumentation failure, and postoperative change such as adjacent segment disease. 3 No standard algorithm for postoperative imaging following ACDF has been defined formally, and the frequency and type of imaging obtained is left to the surgeon's discretion. Due to their relatively low cost and ease of administration, 3 standard radiographs are often ordered for all patients following ACDF to assess fusion status. 4 , 5 , 6 However, the use of such “routine” postoperative radiographs has been found to be unwarranted in asymptomatic patients. 4 , 5 , 6 CT is a more sensitive alternative to plain radiography when assessing fusion because of its ability to detail bridging trabecular bone. 7 Analogous studies on the efficacy of postoperative CT scans following ACDF have yet to be published.
The use of CT in the United States has increased over the past decade. 8 Although CT is a valuable diagnostic tool, it is also a significant source of ionizing radiation, conferring 50 times more radiation to a patient than a conventional anteroposterior radiograph. 9 Such radiation doses can increase the risk of cancer. 9 , 10 , 11 Additionally, CT is a significant source of annual health care spending. 12 Because of these associated factors, CT imaging studies should be reserved for instances in which a high probability for alteration in treatment course exists.
This study investigates the utility of CT following ACDF. Our primary objective was to identify the patient and operative characteristics associated with abnormal postoperative CT scans. As the secondary objectives, we sought to evaluate the patient characteristics associated with an alteration in the treatment or outcome following the CT imaging study, as well as determine the rate at which CTs are ordered following ACDF. Finally, we compared the outcomes between postoperative symptomatic patients who received CT imaging and symptomatic patients who did not undergo a CT scan. We hypothesized that surgeons obtain routine postoperative CT scans (for reasons such as monitoring fusion mass and instrumentation placement) and that, when ordered in asymptomatic patients, such scans would not help alter or improve the treatment course.
Methods
Institutional Review Board approval (12-1365) was obtained prior to the start of this study. A retrospective review was performed of all patients who underwent ACDF at a tertiary center between 2007 and 2011. The patients underwent a single-level or multilevel ACDF between levels C3 and C7. The inclusion and exclusion criteria were selected based on the investigation's primary objective of identifying the pre- and perioperative characteristics that indicate a need for postoperative CT imaging. The patient inclusion criteria consisted of a minimum of 6-month postoperative follow-up. The exclusion criteria included prior cervical spine surgery, chronic neuromuscular disease (such as multiple sclerosis), and the attainment of a CT following an acute postsurgical traumatic incident or for the purpose of a clinical research study. The electronic medical record, including hospital, office, and radiographic notes, was reviewed for all patients in the study.
The patient demographics were collected and recorded. At each follow-up visit, whether or not a CT was ordered was noted. Any unresolved symptoms (i.e., radiculopathy or myelopathy) that remained despite the cervical fusion were also recorded; it was noted whether these symptoms continued to be present at the last documented follow-up visit within 2 years after the index operation. The CT scans were reviewed and abnormal findings were documented on the basis of both the radiologist's report and surgeon's note. The presence of abnormal postoperative imaging (i.e., radiograph or magnetic resonance imaging [MRI]) prior to the CT was recorded as well. The abnormal postoperative findings included pseudarthrosis, adjacent segment disease, foraminal stenosis, and instrumentation failure. All were recorded. Finally, it was noted if patients were offered or underwent any therapeutic intervention, such as revision surgery, an epidural steroid injection, or implantation of a spinal cord stimulator, on the basis of the findings on the CT imaging study.
Statistical Analyses
All statistical analyses were performed using JMP 10 (SAS Institute, Cary, NC, United States). Descriptive statistics summarizing patient demographic data were presented as the mean ± standard deviation or as the counts with percentages, as appropriate. The categorical variables were compared using Fisher exact tests, and the continuous variables were compared using Student t test. The statistical significance was set at p ≤ 0.05.
Results
Six hundred ninety patients who underwent ACDF between 2007 and 2011 were identified and their cases reviewed. Of these 690 patients, 45 (7%) underwent a CT within 2 years of the operation and satisfied the inclusion and exclusion criteria. The patient population included 14 men and 31 women, with an average age of 51.7 ± 11.6 years. There were 53 total postoperative CT scans assessed among the 45 patients. The mean follow-up period was 23.2 ± 16.4 months. Of the 45 patients assessed, 34 (76%) underwent ACDF due to degenerative pathology and 11 (24%) underwent ACDF due to trauma. Single-level ACDF was performed in 17 (38%) patients, and multilevel ACDF was performed in 28 (62%) patients. A summary of the patient demographic data, preoperative presentation, and operative levels is provided in Table 1.
Summary of patient demographics, preoperative presentation, and operative levels
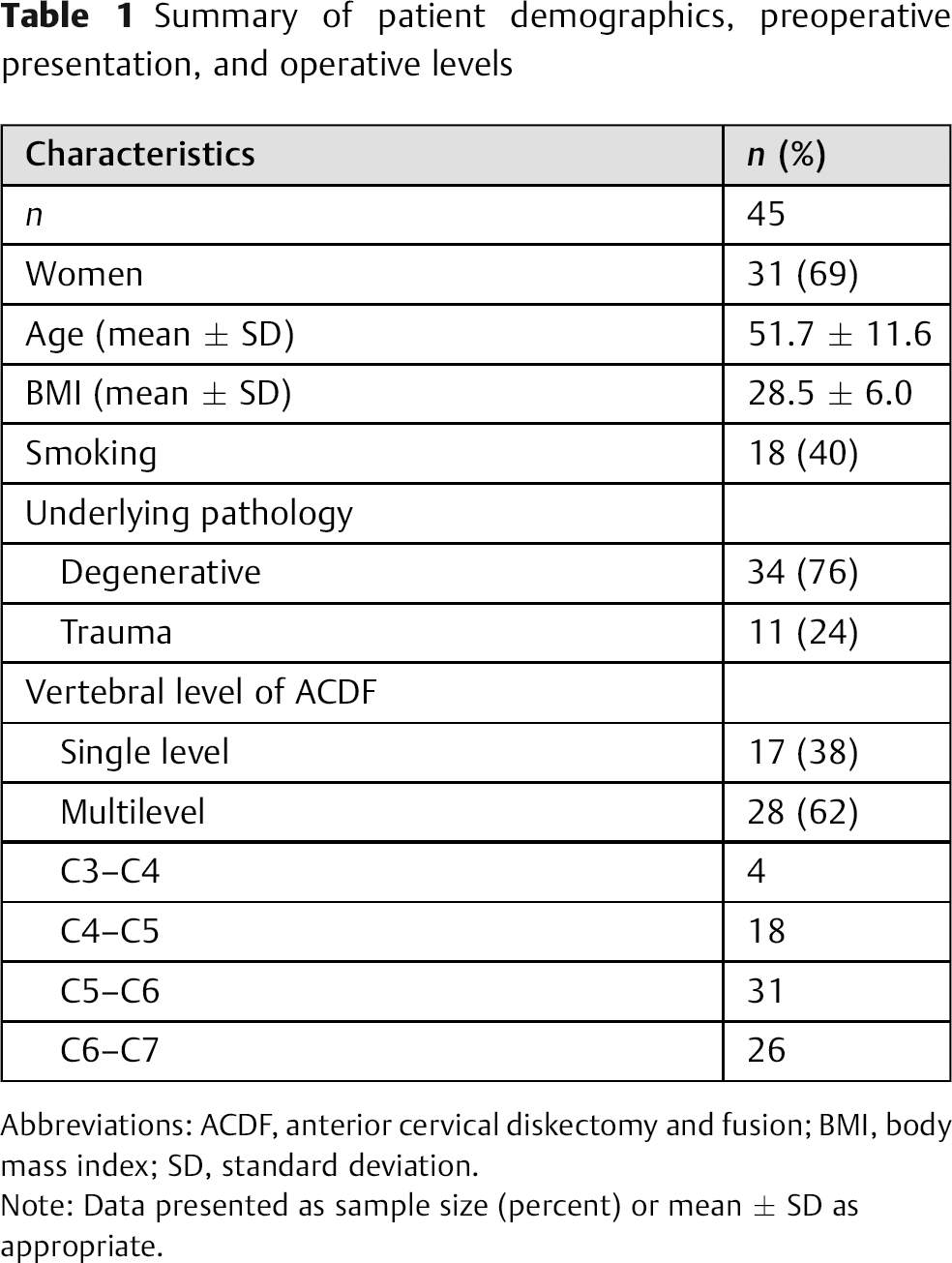
Abbreviations: ACDF, anterior cervical diskectomy and fusion; BMI, body mass index; SD, standard deviation.
Note: Data presented as sample size (percent) or mean ± SD as appropriate.
Of the 53 total postoperative CTs assessed, 27 (51%) were obtained between 1 and 6 months postoperatively, 21 (40%) between 7 and 12 months, and 5 (9%) between 13 and 24 months. The rationale for ordering the CT was abnormal preliminary imaging in 2 (4%) cases, persistent postoperative symptoms in 33 (62%) cases, abnormal preliminary imaging and persistent symptoms in 10 (19%) cases, and without any apparent indication in 8 (15%) cases. Unresolved postoperative symptoms noted prior to the attainment of CT scans included neck pain in 30 (57%) cases, arm pain in 33 (62%) cases, myelopathy in 32 (60%) cases, and no symptoms in 8 (15%) cases (Table 2). All such symptoms were present before the index surgery.
Summary of CT timing and indications
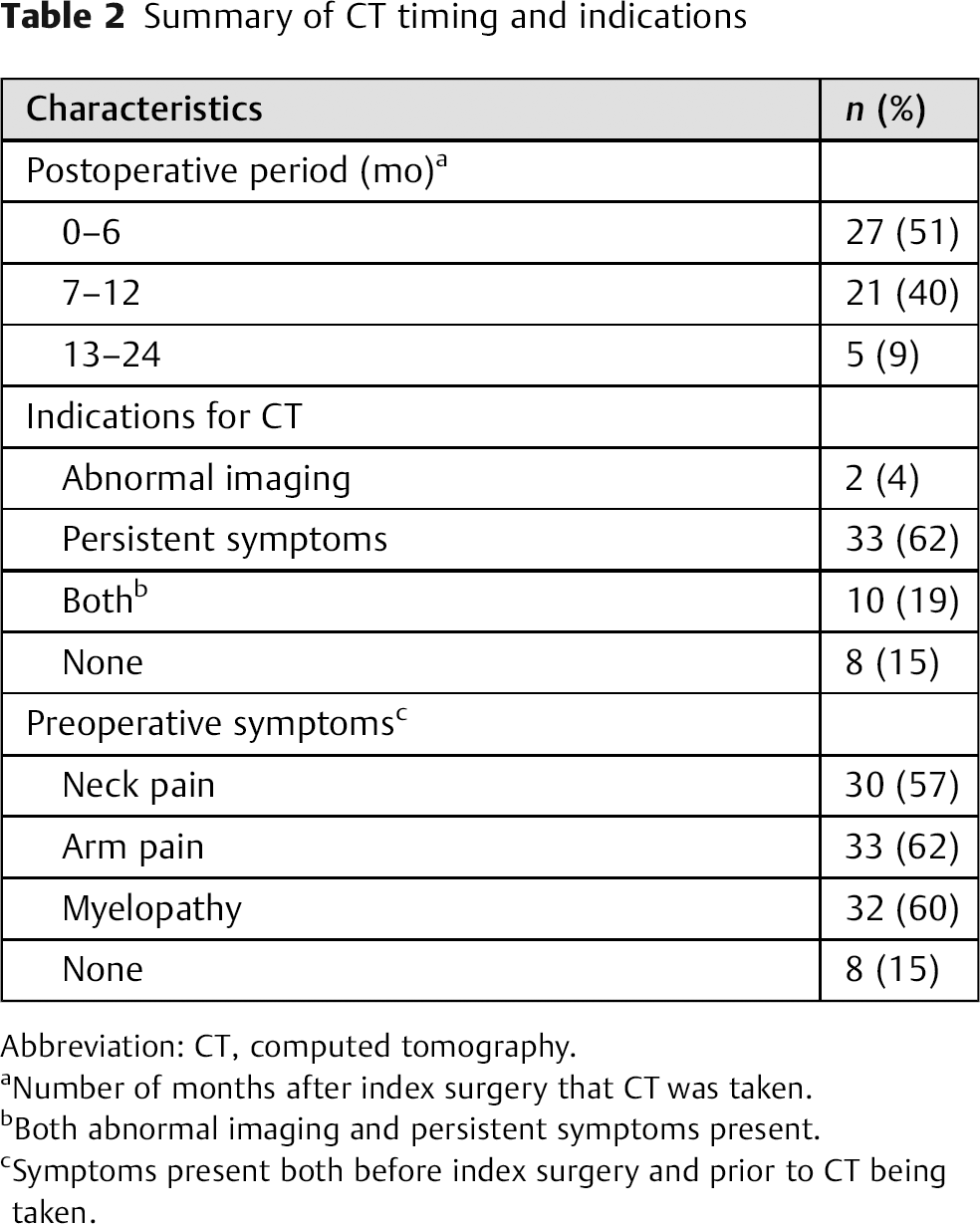
Abbreviation: CT, computed tomography.
Number of months after index surgery that CT was taken.
Both abnormal imaging and persistent symptoms present.
Symptoms present both before index surgery and prior to CT being taken.
Abnormal findings were noted only on 30 of the 53 (57%) CTs reviewed, and 23 scans (43%) demonstrated no unexpected findings. There were no significant differences in the probability of having abnormal findings on the CT scan based on patient demographic information (i.e., age, body mass index, sex, or smoking status), nor were there any significant differences in the frequency of imaging abnormalities based on the time after surgery during which the CT scan was obtained (i.e., 0 to 6 months, 7 to 12 months, 13 to 24 months). The abnormal findings included pseudarthrosis (n = 17, 57%), adjacent segment disease (n = 8, 27%), foraminal stenosis (n = 4, 13%), and instrumentation failure (n = 1, 3%). Patients expressed symptoms related to neck pain, arm pain, and/or myelopathy in 45 of 53 (85%) instances prior to the CT. There were 32 patients with myelopathic symptoms prior to the CT. Twenty-two (69%) of these patients had abnormal CTs. Thirteen patients did not have myelopathic symptoms, and of those only 5 (38%) had abnormal findings on CTs. The probability of an abnormal CT finding was associated with a trend toward significance when the patient experienced pre-CT myelopathy (p = 0.09, Table 3).
Differences between findings based on symptoms and timing
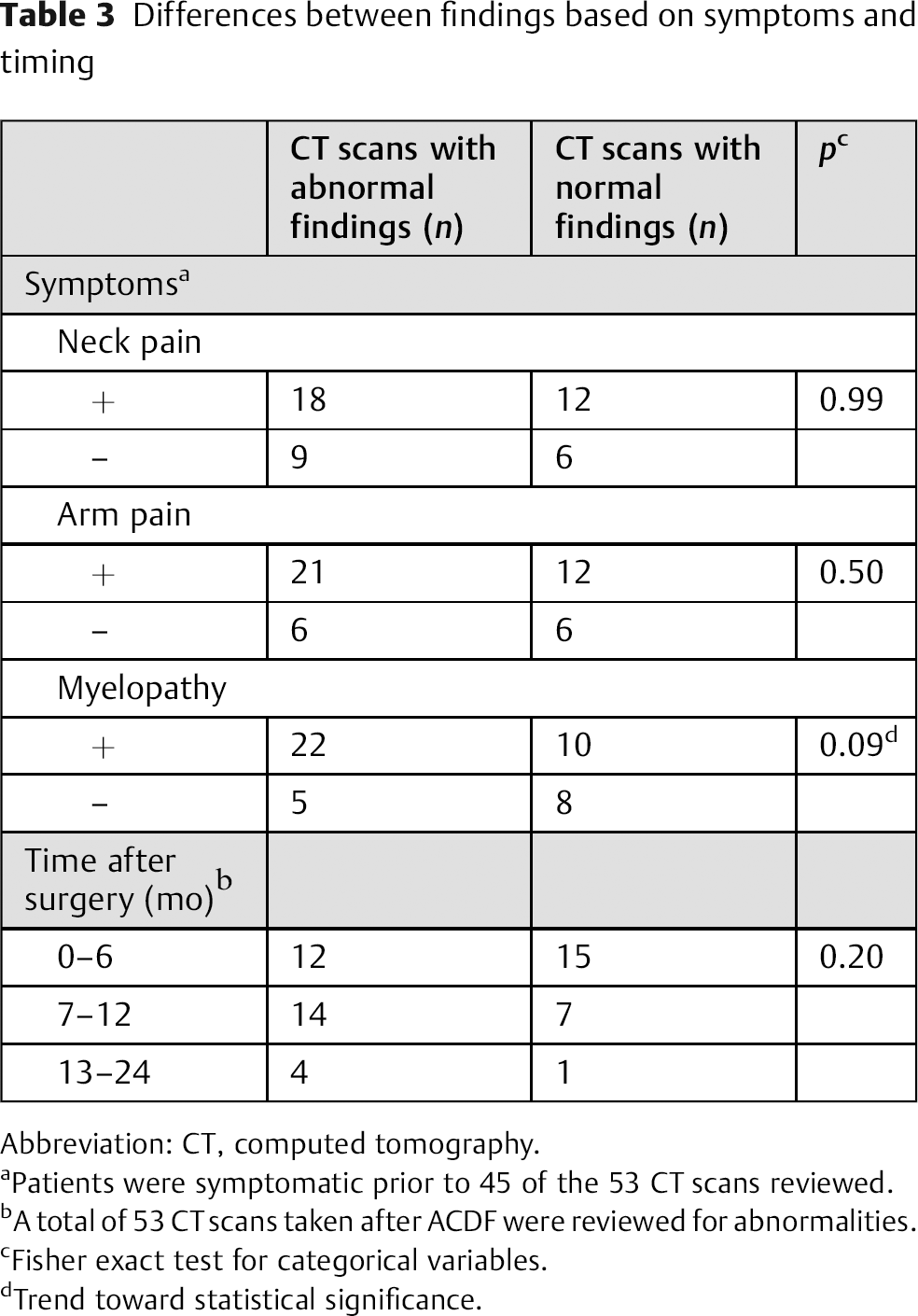
Abbreviation: CT, computed tomography.
Patients were symptomatic prior to 45 of the 53 CT scans reviewed.
A total of 53 CT scans taken after ACDF were reviewed for abnormalities.
Fisher exact test for categorical variables.
Trend toward statistical significance.
There were 45 (85%) cases in which the CT was ordered due to persistent symptoms (n = 33), abnormal preliminary imaging (n = 2), or a combination of the two (n = 10). There was a subsequent abnormal finding on the CT in 29 of these cases (64%). Of the patients with persistent symptoms, only 21 of 33 (64%) had an abnormal CT. The 2 patients who had abnormal preliminary imaging each had an abnormal CT (100%). Of the 10 patients who demonstrated both persistent symptoms and abnormal imaging, 6 (60%) also had an abnormal CT. In the 8 instances (15%) in which there were no indications that a CT was necessary, abnormal findings on the CT were apparent in only 1 patient (13%). As such, the probability of an abnormal CT was found to be significantly higher for patients who presented with persistent symptoms and/or abnormal imaging than for patients for whom there was no indication that a CT was necessary (p = 0.03, Table 4). Importantly, there was no change in the treatment plan for any of the asymptomatic patients (0 of 8, 0%) who received a postoperative CT, and 19 of the 45 (42%) CT scans ordered due to persistent symptoms and/or abnormal preliminary imaging led to an alteration in treatment course (p = 0.04, Table 4). Resolution of the postoperative symptoms in patients who underwent a CT imaging study occurred in 5 of 43 (12%) instances.
Abnormal CT findings and alterations in treatment course based on indications for CT
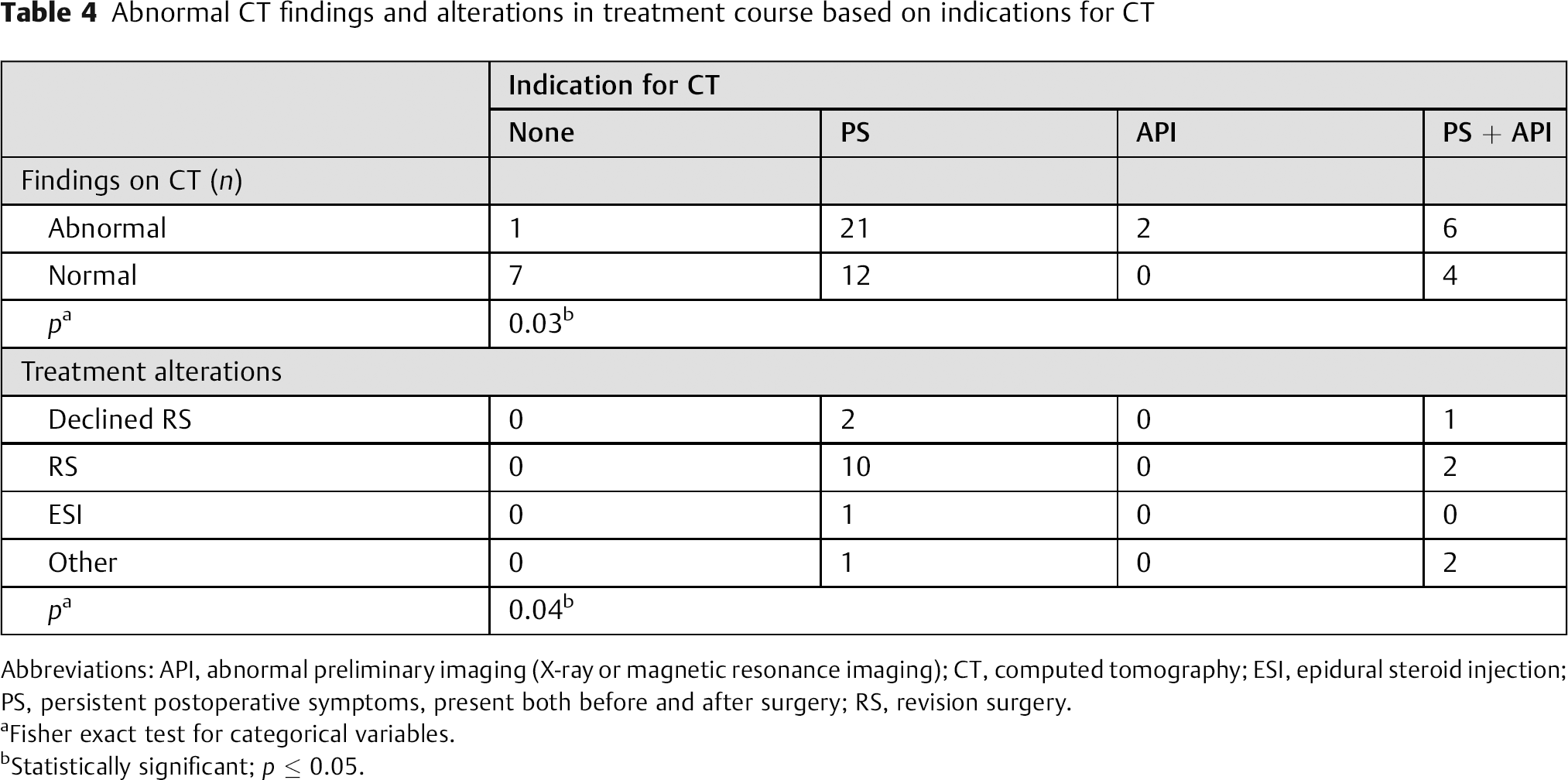
Abbreviations: API, abnormal preliminary imaging (X-ray or magnetic resonance imaging); CT, computed tomography; ESI, epidural steroid injection; PS, persistent postoperative symptoms, present both before and after surgery; RS, revision surgery.
Fisher exact test for categorical variables.
Statistically significant; p ≤ 0.05.
Thirty-six (68%) of the postoperative CTs were performed either following normal preliminary imaging or without preliminary imaging (absent = 16, normal X-ray = 18, normal MRI = 2). Of these cases in which abnormal preliminary imaging was not present, 19 (53%) patients had normal CTs and 17 (47%) had abnormal findings on CT. Of the 17 with abnormal preliminary imaging, 13 (76%) had abnormal CT findings as well, and 4 (24%) had normal CTs. The probability of an abnormal finding on a postoperative CT was associated with a trend toward significance when the preliminary testing also displayed abnormal findings (p = 0.07, Table 5).
Differences between CT findings based on preliminary imaging findings
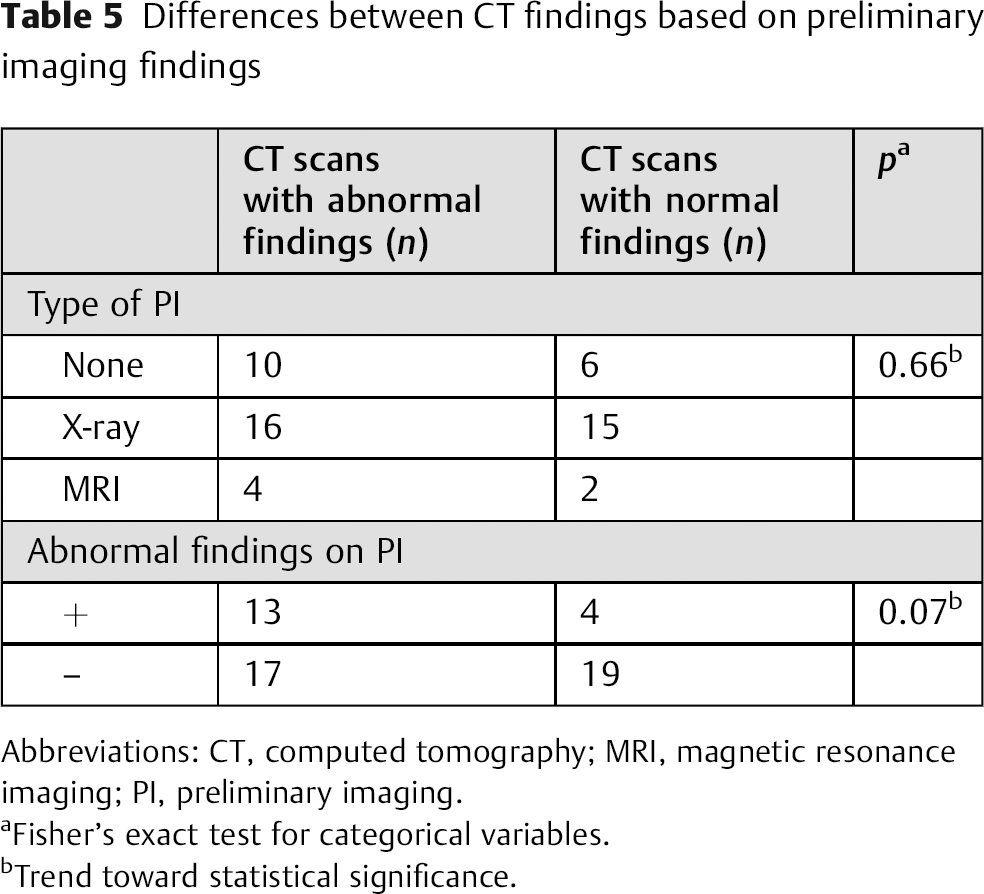
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; PI, preliminary imaging.
Fisher's exact test for categorical variables.
Trend toward statistical significance.
Of the 645 patients who underwent ACDF but did not have a postoperative CT scan, 129 (20%) were randomly selected for evaluation of their postoperative outcomes. Of these patients, 65 (50%) had postoperative radiculopathy and/or myelopathy within 2 years following their surgery and had at least 6 months of follow-up. Most of these patients (n = 47) were managed conservatively with nonsteroidal anti-inflammatory medications and physical therapy; the remaining (n = 18) were given corticosteroid injections (n = 1), referred to a spine medicine specialist (n = 10), underwent MRI imaging (n = 8), and/or underwent additional surgery (n = 5). Patients treated conservatively demonstrated complete resolution of their symptoms in 30 (64%) cases. The symptoms resolved in only 2 (11%) of those who received additional therapeutic or diagnostic modalities.
Discussion
CT is a useful imaging modality to detect incomplete or improper fusion of the vertebrae following ACDF. 7 It is the most sensitive and specific modality to assess spinal fusion, 7 , 13 , 14 , 15 and it effectively detects adjacent segment degeneration, 16 which occurs in 10 to 20% of patients following ACDF. 17 , 18 Nonetheless, no studies describe the indication for postoperative use of CT. Current U.S. trends show an increasing use of CT, which creates both a financial burden as well as a risk to patients from radiation exposure. Accordingly, in the present study, we sought to define the utility of CT in the postoperative period.
The primary objective of our study was to identify patient and operative characteristics associated with abnormal findings on postoperative CTs. We determined that abnormal CTs were significantly more likely to be found in patients who presented with postoperative symptoms (i.e., neck pain, arm pain, and/or myelopathy) and/or those who had abnormal preliminary imaging as compared with asymptomatic patients (p = 0.03). There were no significant differences in the probability of an abnormal CT based on age, gender, body mass index, smoking status, or indication for surgery. Patients who exhibited myelopathic symptoms postoperatively trended toward having significantly more abnormal CT findings compared with patients who did not have such symptoms (p = 0.09). In addition, patients who had abnormal preliminary imaging also trended toward having abnormal CT findings (p = 0.07). These findings suggest that CT use may be more justifiable with these clinical presentations.
A secondary objective of our investigation was to determine patient characteristics associated with treatment alteration following attainment of a CT scan after ACDF. We found that asymptomatic patients were significantly less likely to have a change in treatment course (e.g., revision surgery, epidural steroid injections, implantation of a spinal cord stimulator) than patients who exhibited symptoms (p = 0.04), although there were no statistically significant relationships relating the presence of a specific pre-CT symptom (i.e., neck pain, arm pain, or myelopathy) to altered treatment course. All of the 19 patients who underwent an alteration in treatment course presented with persistent symptoms. Five of these patients also had accompanying abnormal imaging. Interestingly, alterations in treatment course occurred in 60% of patients (6 of 10) who exhibited both persistent symptoms and abnormal imaging but only in 39% of patients who only had persistent symptoms (13 of 33). This data suggests that postoperative CTs should not be ordered unless patients demonstrate clinical symptoms and/or abnormal preliminary imaging (i.e., radiograph, MRI) that needs to be confirmed by CT, confirming our hypothesis that the routine ordering of postoperative CT scans after ACDF would not affect treatment course.
An additional secondary objective was to determine the rate at which CT scans are ordered following ACDF. There are currently no accepted guidelines for when and what postoperative imaging should be obtained following cervical fusion. As such, imaging is largely ordered based on the judgment and preference of the surgeon. CT imaging is done for asymptomatic patients in the postoperative setting to assess bone growth as well as to monitor hardware placement. 7 We hypothesized that a significant proportion of surgeons order routine CT scans following ACDF to review such outcomes. However, only 7% of patients who underwent ACDF had a subsequent CT within 2 years. Furthermore, of these CT scans, only 8/53 (15%) were taken routinely with no apparent indication (i.e., the patient had no symptoms or abnormal preliminary imaging). This finding suggested that, unlike plain radiographs, CTs are not frequently ordered routinely following ACDF. These findings are supported by a 2012 survey study by Bohl et al, which determined that although 96% of surgeons order regular postoperative radiographs following ACDF, only 14% of surgeons order routine CTs. 19
We also compared outcomes for symptomatic patients who received a postoperative CT scan with those who did not. Half of the cohort that did not undergo a CT scan displayed symptoms of radiculopathy and/or myelopathy; the majority of those managed with conservative therapy recovered fully within 2 years. Interestingly, patients who were handled with higher levels of care had nearly identical rates of recovery as patients who received a postoperative CT scan. These findings are likely because patients who received a more thorough workup had a higher burden of disease as depicted by clinical or radiographic evidence.
Although the clinical scenarios that merit postoperative CTs have not been previously investigated, several studies have been published on the utility of routine radiographs following spinal fusion surgery. Shau et al reported that routine postoperative radiographs provided minimal utility in altering the treatment course for asymptomatic patients following a variety of different cervical fusion operations. 4 Similarly, Ugokwe et al determined that regular radiographic examination of asymptomatic patients following ACDF was unwarranted. 6 Bartels et al concluded that among patients who undergo cervical anterior diskectomy with a stand-alone cage, radiographs should only be performed when the patients exhibit the appropriate signs and symptoms. 5 The results of the present study similarly indicate that CTs should be reserved for symptomatic patients and should not be used routinely.
CT scans are responsible for the majority of cumulative effective dose of radiation to which Americans are exposed. 20 This radiation exposure increases the risk of various cancers, as well as other conditions such as local tissue damage to the skin or gonads, cytogenetic effects, and hematologic effects. 21 CT of the cervical spine exposes patients to an effective dose of radiation equivalent to ∼54 chest X-rays. 11 For these reasons as well as the financial cost, it is important to identify which postoperative CT scans are needed to improve patient care.
Several limitations associated with this study must be considered when interpreting the data. The data was collected retrospectively and included patients from multiple surgeons. The impact of our secondary objectives was restricted by several factors. The identified rate of CT imaging studies ordered following ACDF was limited by an inability to identify imaging performed at other institutions. The sample size was also fairly small, which limited the statistical power. In particular, this restraint prevented us from better identifying specific patient characteristics that altered the treatment outcome after the attainment of a postoperative CT imaging study.
Future studies can extend on the present work. A matched case–control cohort study comparing patients who underwent ACDF and either did or did not have a postoperative CT scan could be implemented to more definitively determine if CT imaging studies alter the outcome after surgery. Prospective, multicenter studies would also afford better opportunities to analyze the postoperative utility of CT following ACDF in more depth. Nonetheless, this study is the first to examine the utility of CT scans following spinal fusion. Additional studies utilizing a larger cohort are needed to validate our results, but this preliminary data suggests that CT scans be used judiciously following ACDF, and only in symptomatic patients.
Conclusion
We found that CT scans following ACDF are not routinely ordered. A CT results in alteration of the treatment in 60% of patients with an abnormal MRI and/or radiograph and persistent symptoms. In contrast, if the patient only has persistent symptoms, only 39% of them will go onto further intervention, suggesting that CT has a limited utility in this population. The probability of detecting abnormal findings on CT subsequent to ACDF is significantly greater when the patient presents with persistent symptoms or abnormal preliminary imaging. Alterations in the treatment course based on abnormal postoperative CT are dependent on postoperative symptoms. Those patients who undergo CT without indication (i.e., without preimaging symptoms or abnormal imaging) are significantly more likely to have negative findings on CT, and even with abnormal CT findings, they are less likely to have an alteration in the treatment course. As such, postoperative CTs following ACDF should be limited to patients who have persistent debilitating symptoms or those with abnormal imaging. This practice will avoid unnecessary cost and patient exposure to ionizing radiation.
Disclosures
Adeeb Derakhshan, none
Daniel Lubelski, none
Michael P. Steinmetz, none
Edward C. Benzel, none
Thomas E. Mroz, none