
Abstract
Study Design
Retrospective cohort study.
Objectives
Patients with IBD are at an increased risk for postoperative complications following surgery. The goal of this study is to investigate if inflammatory bowel disease (IBD) is a risk factor for complications following lumbar discectomy.
Methods
We identified IBD patients who underwent lumbar discectomy for lumbar disc herniation (LDH) and matched to them with controls without IBD in a1:5 ratio. We excluded patients with a history of spinal injury, cancer, infection, trauma, or surgery to remove the digestive tract. We used multivariate logistic regression analyses to compare postoperative outcomes, including 90-day complications, 90-day emergency department visits, and 90-day readmissions. In addition, 2-year re-discectomy rates and a 3-year lumbar fusion rate were compared between the cohorts.
Results
After applying the study criteria, we identified 6134 IBD patients with LDH for further analysis. With the exception of dura tears, patients with IBD had significantly higher rates of medical complications, incision-related complications, ED visits, and readmission rates compared to patients without IBD, especially for the 2-year and 3-year rates of disc recurrence and revision surgery.
Conclusions
Patients with IBD who underwent lumbar discectomy are at a significantly higher rate of complications. Therefore, spine surgeons and other health care providers should be aware of this higher risk associated with IBD patients and properly treat the patients’ IBD before surgery to lower these risks.
Keywords
Background
Low back pain (LBP) is a prevalent and disabling condition that impacts millions of people worldwide, limiting their ability to engage in daily activities. 1 Intervertebral disc degeneration (IDD) is 1 of the leading causes of LBP. IDD weakens the structural integrity of the disc, rendering it vulnerable to herniation, which can lead to both LBP and leg pain. 2 While conservative treatments are effective for many patients, some may still require surgical intervention, with discectomy being the most commonly performed procedure.3,4 Although there are various surgical techniques available for the initial operation. The primary objective of surgery is to alleviate symptoms by removing the protruding intervertebral disc that compresses the nerves.
Recent studies have suggested that the gut-spine axis may be 1 of the important causes play a significant role in the development of IDD and LBP. 5 The interaction between the gut and the spine is mediated through the nervous and immune systems, and some studies suggest that gut microbiota and their metabolites may affect the spine and intervertebral discs through this axis. 5 Inflammatory bowel disease (IBD) is a chronic inflammatory condition affecting the intestines, with over 1.4 million patients in the United States. 6 Patients with IBD are at an increased risk for postoperative complications following surgery, such as total knee arthroplasty, 7 hip arthroplasty, 8 and prostatectomy. 9 One possible explanation for this is that IBD can result in poor nutritional status, which is a well-known predictor of adverse outcomes after spinal fusion surgery. 10 However, the impact of IBD on patients undergoing lumbar discectomy for LDH is not yet clear.
This study aims to investigate the impact of IBD on the outcomes of lumbar discectomy for LDH using the PearlDiver national insurance database. Our hypothesis is that patients with IBD are at a greater risk of developing postoperative complications following lumbar discectomy, compared to those without IBD. It is crucial for spine surgeons to recognize the potential impact of IBD on patients undergoing this procedure to ensure the best possible outcomes.
Methods
Data Source
A retrospective cohort analysis was performed using the Mariner subset of the commercially available PearlDiver (PearlDiver Inc., Colorado Springs, CO, USA; https://www.pearldiverinc.com/) fee-based patient records database. This database contains more than 160 million de-identified patient records and compiles variables such as demographics, comorbidities, and procedural codes. The database can be queried using unique subset criteria based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), International Classification of Diseases, 10th Revision (ICD-10-CM), and Current Procedural Terminology (CPT) codes. Access to the server that houses the database was granted by PearlDiver Technologies for academic research. Considering the de-identified nature of the database, this study was exempt from the institutional review board review and informed consent approval process.
Study Population
The PearlDiver database (https://www.pearldiverinc.com/, Colorado Springs, CO) was queried for IBD patients greater than or equal to 18 years old with IDD who underwent single level lumbar discectomies from 2010-2020 using a combination of ICD-9, ICD-10, and CPT codes. We excluded patients with any history of spinal surgery and etiologies of spinal tumor, infection, or trauma. Patients with a history of any digestive tract removal surgery were also excluded from the analyses. A control group of patients who had lumbar discectomies for LDH but didn’t have IBD were matched in a 1:5 ratio based on age, gender, and comorbidities including obesity, chronic kidney disease, chronic obstructive pulmonary disease, diabetes mellitus, coronary artery disease, tobacco use, congestive heart failure, hyperlipidemia, peripheral vascular disease, hypertension, and depression. The workflow of patient selection is depicted in Figure 1. Flowchart and exclusion criteria for this study.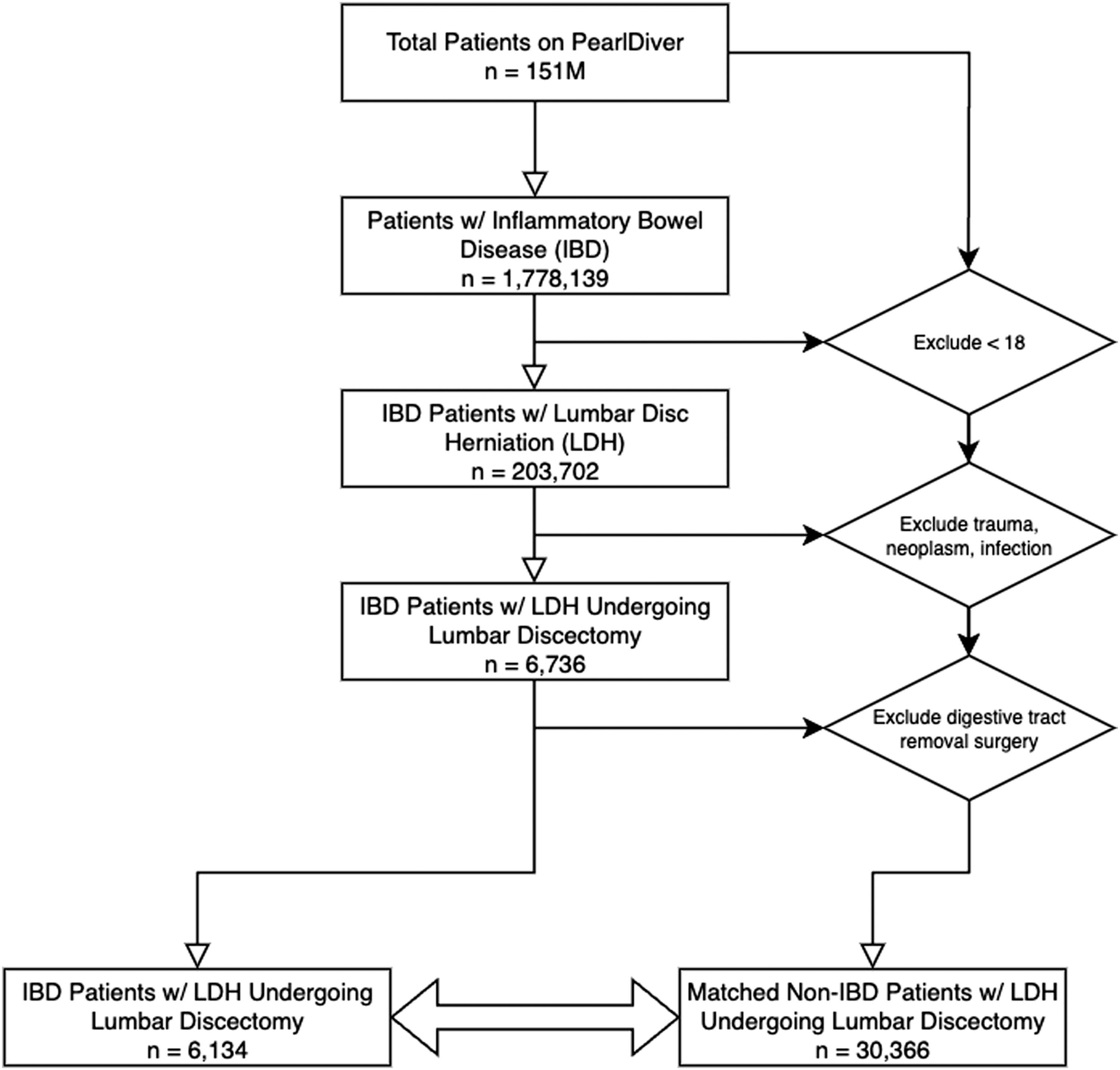
Outcomes
IBD Patients undergoing lumbar discectomies were compared to controls for 90-day medical complications and incision-related complications, 90-day emergency department (ED) visits, and 90-day readmissions. Medical complications included intubation, aspiration, pulmonary embolism, pneumonia, cerebrovascular accident, deep vein thrombosis, transfusion, acute kidney injury, urinary tract infection, sepsis, and myocardial infarction. Incision-related included 90-day wound complications and surgical site infection. Considering the relatively high recurrence rate of this surgery, we have calculated the 2-year subsequent revision discectomy and 3-year subsequent lumbar fusion rates for patients.
Statistical Analysis
Baseline demographics and preexisting comorbidities were compared using Pearson χ2 analysis. In addition, Pearson χ2 analysis was used to compare medical and surgical complication rates. After adjusting for age, gender, and preexisting comorbidities, the effect of IBD on postoperative outcomes was determined using multivariable logistic regressions. All statistical analyses were conducted with the R Project for Statistical Computing software (R Foundation for Statistical Computing, Vienna, Austria), which was a built-in analytic tool in PearlDiver. P value less than 0.05 was considered statistically significant.
Results
Patient Demographics and Comorbidities
Inflammatory Bowel Disease vs Matched Controls Undergoing Single-Level Lumbar Discectomy (Demographics).
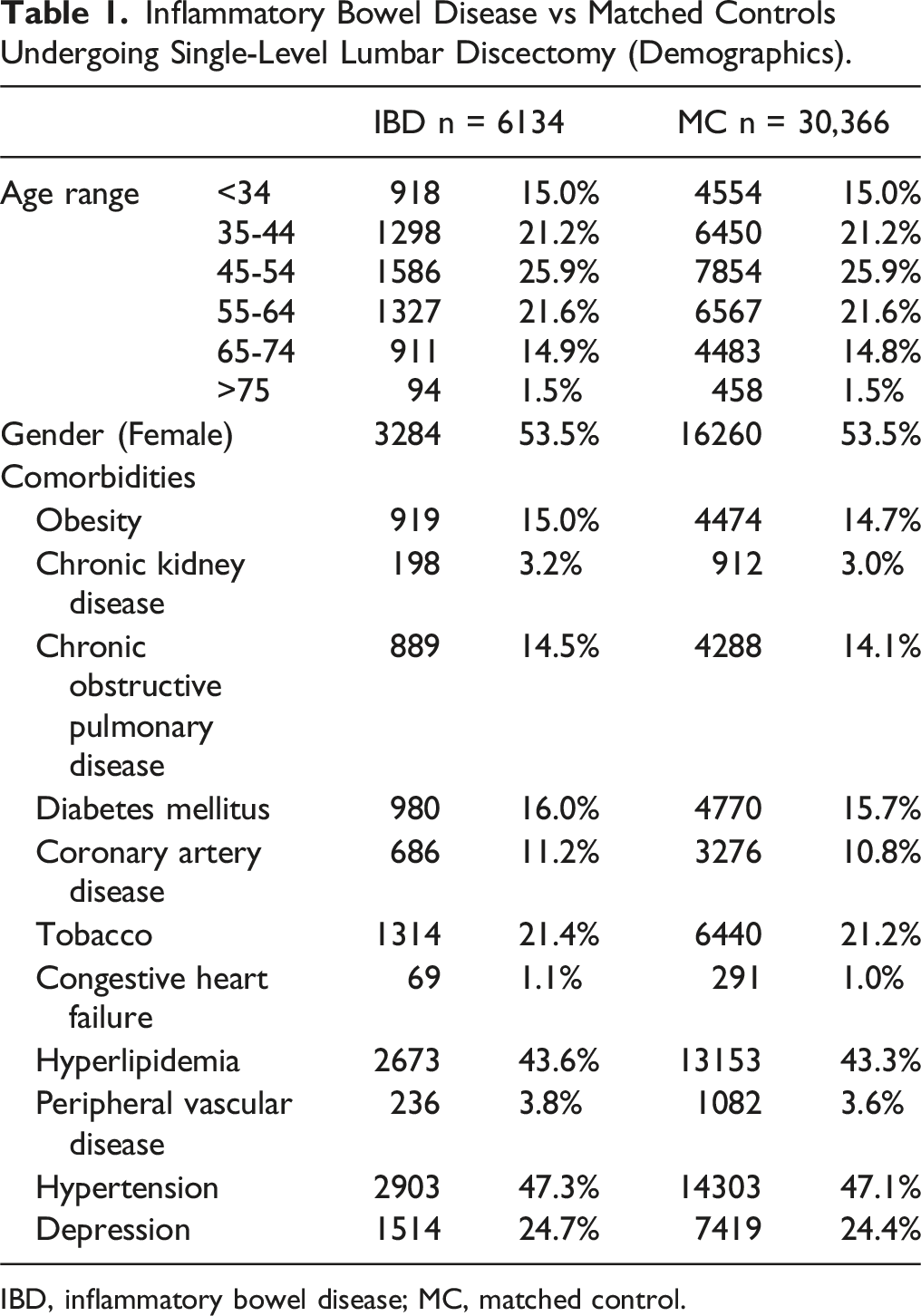
IBD, inflammatory bowel disease; MC, matched control.
Increased Risk of Postoperative Complications in IBD Patients
Inflammatory Bowel Disease vs Matched Controls Undergoing Single-Level Lumbar Discectomy (Outcomes).
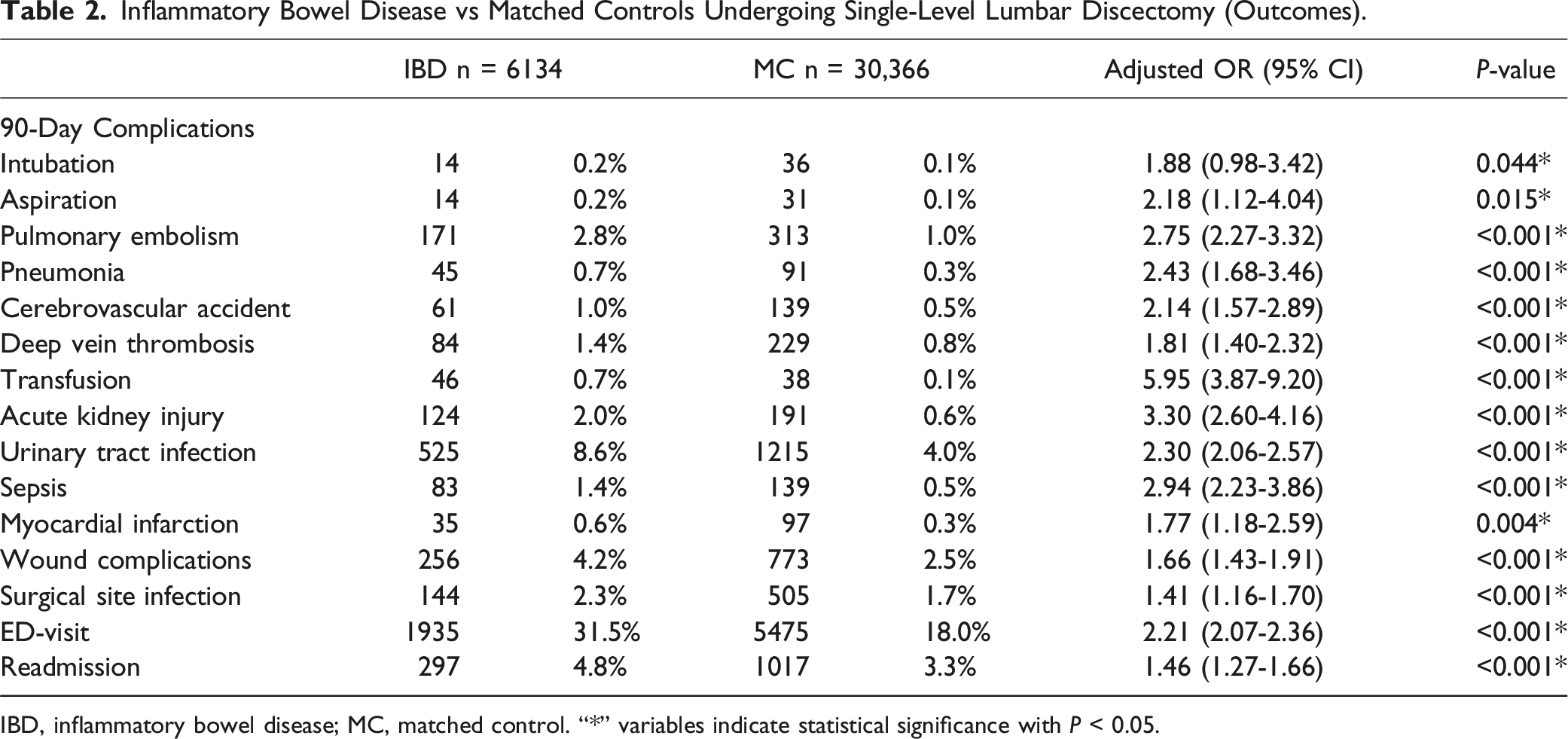
IBD, inflammatory bowel disease; MC, matched control. “*” variables indicate statistical significance with P < 0.05.
Increased Risk of Revisions in IBD Patients
Inflammatory Bowel Disease vs Matched Controls Undergoing Single-Level Lumbar Discectomy (Incidences of Revisions).

IBD, inflammatory bowel disease; MC, matched control. “*” variables indicate statistical significance with P < 0.05.
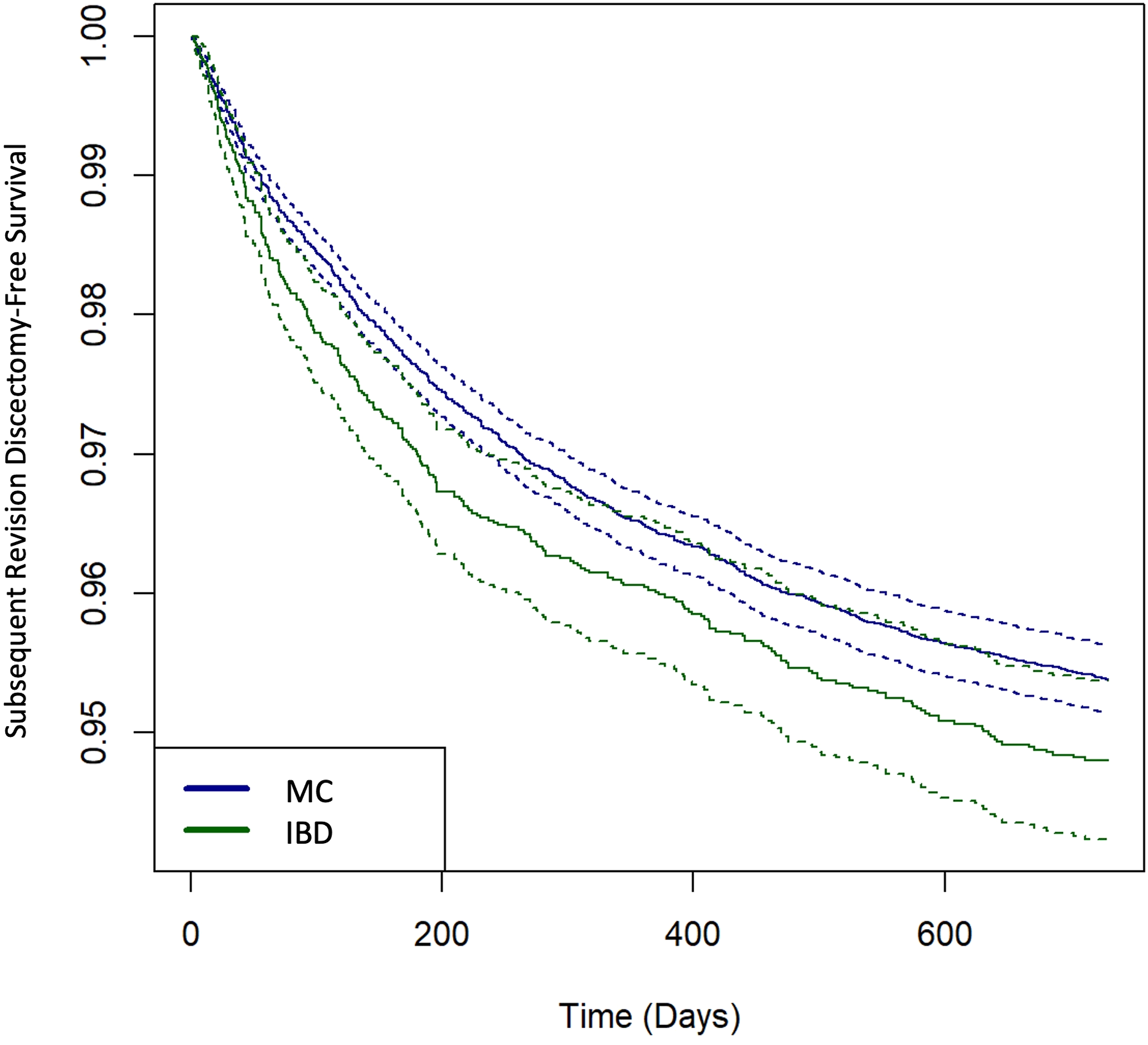
Kaplan-Meier curve for subsequent revision discectomy-free survival between IBD patients and matched controls. Dotted lines indicate 95% CI.
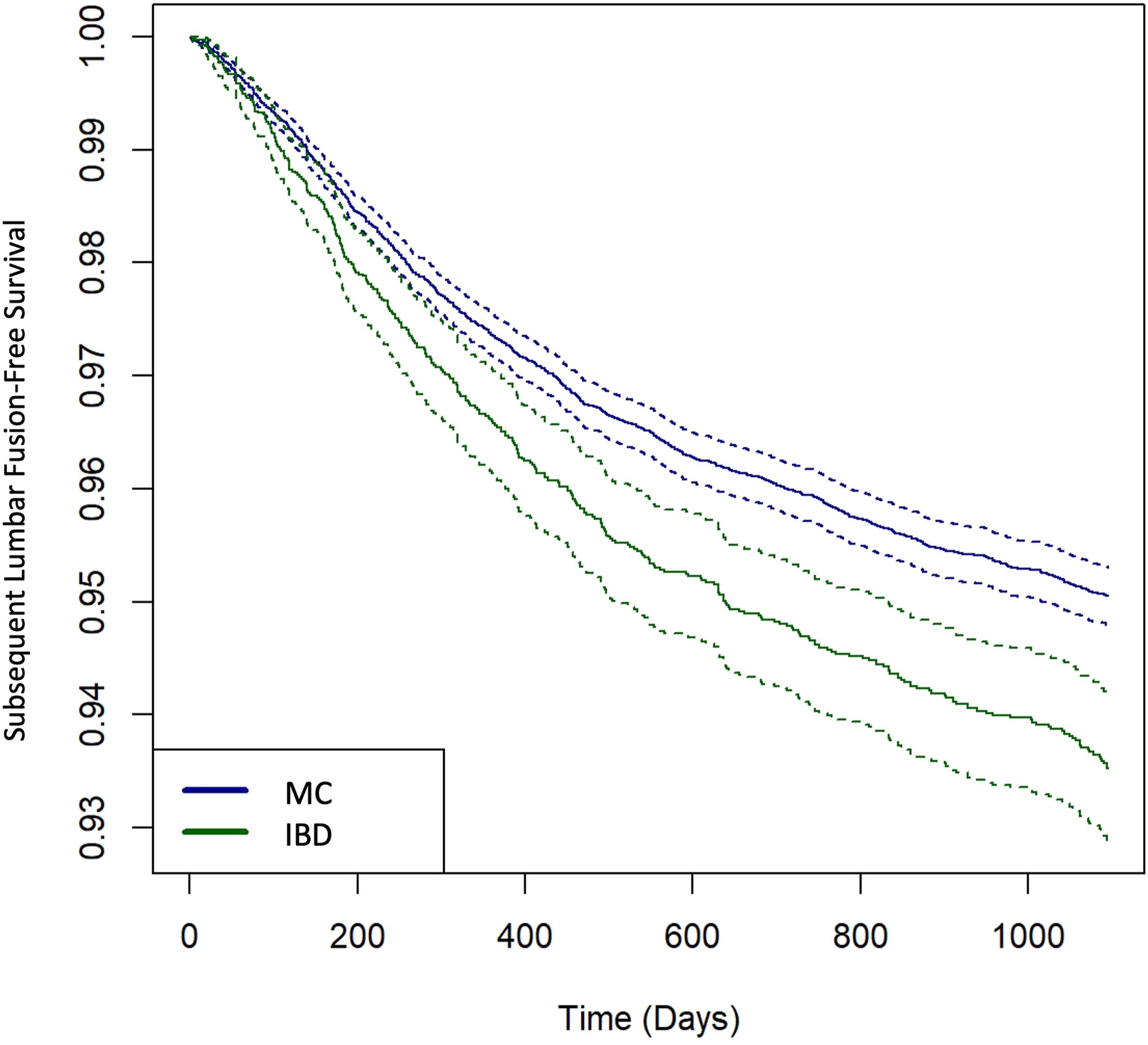
Kaplan-Meier curve for subsequent lumbar fusion-free survival between IBD patients and matched controls. Dotted lines indicate 95% CI
Discussion
With approximately 300,000 lumbar discectomies performed annually in the US 4 and more than 2 million people suffer from the IBD. 11 There have been numerous studies indicating that both of these conditions are immune-related diseases. It is become increasingly crucial for spine surgeons to consider the potential complications and risk profiles of IBD patients before surgery. To the best of our knowledge, some previous studies have identified IBD as a risk factor for spinal fusion surgery 12 ; however, the relationship between IBD and the postoperative complications of single-level lumbar discectomy for LDH remains underexplored in the existing research.
Our findings indicate that patients with IBD who underwent lumbar discectomy are more likely to experience post-surgical complications compared to those without IBD (as shown in Tables 2 and 3). This result demonstrates that IBD is a risk factor for high postoperative complications after lumbar discectomy. These results are consistent with previous research on non-spine procedures.
Numerous studies have reported a close association between gut inflammation and various joint pathologies, including spondylarthritis, psoriatic arthritis, reactive arthritis, and others. 13 As a unique type of joint, the intervertebral disc can also potentially be affected by IBD. A recent study has also shown that intestinal inflammation can promote intestinal permeability, allowing more bacteria to cross the epithelial barrier. 14 Even though the immune system quickly kills the majority of translocated bacteria, some bacteria can enter and survive by dodging the immune response. 15 Li et al. have proposed a possible link between the gut microbiome and IDD via the translocation of bacteria across the gut epithelial barrier and eventually to IVD, mis regulation of the mucosal and systemic immune systems, and metabolite movement from the gut to the IVD 5 Recently, a revolutionary link between gut dysbiosis and inflammation has been linked with the development and progression of IDD. 16 In patients with IBD, the intestine produces many inflammatory factors and immune cells. These factors and cells can enter the bloodstream, causing the body to be in a relatively high inflammatory state. Neovascularization is a major sign of IDD. Damaged IVDs show infiltrating vascularization through the outer annulus fibrosus and into the inner nucleus pulposus.17,18 Inflammatory factors and cells in the blood can enter the intervertebral disc, further accelerating the degeneration of the disc.19,20 Furthermore, the intervertebral disc itself is an avascular structure, which to some extent escapes surveillance by immune cells within the bloodstream. According to our previous research, 20 when the intervertebral disc herniates, the body recognizes it as a foreign object and attracts a large number of immune cells, such as neutrophils and macrophages, to its surrounding area. These immune cells secrete a significant amount of pro-inflammatory and anti-inflammatory factors, creating an inflammatory state in the local microenvironment of the intervertebral disc. This further accelerates the degeneration of the intervertebral disc. Increased GI permeability and IVD vascular penetration, Infiltration of multiple immune cells as well as the anatomical proximity of the intestines to the lumbar spine, combine to form a potential shunt of pathogenic bacteria to the IVD. In addition, many results have shown that IBD can lead to malnutrition, 21 which is associated with poor wound healing. 22 According to the existing evidence, we believe that IBD could be related to inducing and aggravating IDD through changing or regulating the outside and inside microenvironment of the IVD, thereby accelerating the probability of disc herniation and revision surgery.
Our clinical findings also support this hypothesis. Patients with IBD who underwent lumbar discectomy were more likely to experience relapse compared to those without IBD. The 2-year follow-up period revealed a statistically significant difference in the rate of discectomy revision surgery. Although the time difference between the first and second surgeries was not statistically significant, individuals with IBD underwent the second surgery approximately 27 days earlier than those without IBD. Additionally, patients with IBD had a significantly higher likelihood of requiring revision and fusion surgery 3 years post-surgery compared to those without IBD. While there was no statistical difference in the time between revision surgery and initial surgery, the average time between revision fusion surgery and initial surgery was approximately 54.5 days shorter for patients with IBD compared to those without IBD.
The utilization of extensive nationwide databases in this study offers significant advantages, particularly in investigating diseases at a broad national level. Additionally, the PearlDiver database stands out due to its exceptional ability to track patient data postoperatively over a long period of time, enabling recording of outcomes at any point during enrollment, ensuring a dependable source of data for short- and medium-term analysis.
However, the utilization of a large retrospective database does present certain inherent limitations. The reliability of our findings hinges upon the accuracy of the coding within the database. While a comprehensive multivariate regression analysis can address potential confounding factors related to coding, it is unable to control for variables that exist outside the scope of the coding database, such as operative time, blood loss, and surgical technique. This limitation arises due to the limited level of detail provided by the database, which may potentially introduce biases in the outcomes. Our study is also unable to include information regarding the indication for reoperation or the rationale behind selecting revision discectomy or revision lumbar fusion, as this data is not available in the PearlDiver database (a common limitation in insurance database studies). Several variables, including the nature of the recurrent lumbar herniation, the progression of degenerative disease, and the presence of other comorbid conditions, could influence these decisions.
Conclusion
In summary, our study showed that patients with IBD have higher rates of postoperative complications and relapse following lumbar discectomy. Patients with IBD were significantly more likely to require revision and fusion surgery. More clinical studies are needed to figure out how this relationship works and to help spine surgeons know how to treat IBD patients who need a lumbar discectomy. Particularly in pre-operative communication, we should inform patients of their relatively high incidence of surgical complications and relapse rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.