
Abstract
Study Design
Narrative review.
Objectives
The purpose of this review is to outline the role of sex hormones, particularly estrogen, in the pathogenesis of degenerative disc disease (DDD).
Methods
A narrative review of studies discussing sex hormones and intervertebral disc (IVD) degeneration was conducted through a search of bibliographic databases to identify various mechanisms involved in effectuating DDD.
Results
Estrogen-deficient states negatively impact various aspects of IVD function. These internal hormone environments reflect routine changes that commonly arise with physiologic aging and can compromise IVD structural integrity through a host of processes. Additionally, allosteric molecules such as micro-RNAs (mi-RNAs) and G protein-coupled estrogen receptors (GPER) antagonists can bind to estrogen receptors and inhibit protective downstream effects with estrogen receptor signaling. Furthermore, cursory studies have observed chondrogenic effects with testosterone supplementation, although the specific mechanism remains unclear.
Conclusions
Regulation of sex hormones, namely estrogen and testosterone, significantly impacts the structural integrity and function of IVDs. Uncovering underlying interactions driving these regulatory processes can facilitate development of novel, clinical therapies to treat DDD.
Introduction
Degenerative disc disease (DDD) remains a leading cause of chronic back and neck pain, both which impart substantial clinical and economic burden. From 1996 to 2016, Americans spent a $76.9 billion through private insurance, $45.2 billion through public insurance, and $12.3 billion through out-of-pocket on treatment of neck and back pain. 1 Several predictors for DDD have been identified, in which increasing age was found to be most contributory. 2 As life expectancy and the average age of the population increase, 3 it is important to identify the associations and potential therapy targets linked to DDD.
A promising area of research looks at the intersection of sex hormones and intervertebral disc degeneration. As detrimental effects of sex hormone deficiencies on bone integrity have been well-established, recent attention has been directed toward their impact on stabilizing structures such as the intervertebral disc (IVD). Although studies investigating these relationships can emulate sex hormone deficient states characteristic of physiologic aging and degeneration, few clinical studies have discussed this possible interaction in human models We will explore in this review what is currently known about the function of the sex hormones estrogen and testosterone in the pathogenesis of DDD.
Section 1: Disc Anatomy, Structure, Function and Blood Supply
There are 25 intervertebral discs (IVDs), each composed of an annulus fibrosus that surrounds a nucleus pulposus, anchored to each other by cartilage endplates. The nucleus pulposus (NP), composed primarily of water, proteoglycans such as aggrecan, and type II collagen, provides vertebrae with the necessary elasticity and stability to absorb applied forces and redirect them appropriately. 4
The annulus fibrosus (AF), a band of connective tissue surrounding the NP, provides resistance against forces redistributed by the NP. Its unique heterogenous composition, which includes an outer layer of fibrotic type 1 collagen, inner layer of primarily cartilaginous type 2 collagen, elastic fibers, proteoglycans, and glycoproteins contribute to its tensile properties and resistance to fractures. 5 Cells present in the layers of the IVD are mainly responsible for secreting and maintaining the extracellular matrix (ECM). Despite being largely avascular, the IVD is sustained through diffusion of nutrients from the dense blood supply of the neighboring cartilage endplate (CEP). 6
Disc degeneration is a key area of research due to its substantial effect on patient quality of life. Various explanations have been offered to the origins of disc degeneration, including progressive deterioration, nutritional deficiencies, genetic predispositions, and hormone-related processes. The role of sex hormones, specifically estrogen, in the pathogenesis of DDD has gained considerable traction as a promising area of research. 7
Section 2: Effect of Sex Hormones, Regulatory Molecules, and Receptor-Binding on Disc Cartilage
Outline of Major Regulatory Receptors Involved in Estrogen-Mediated signaling and Their Interactions with inhibitory allosteric modulators.
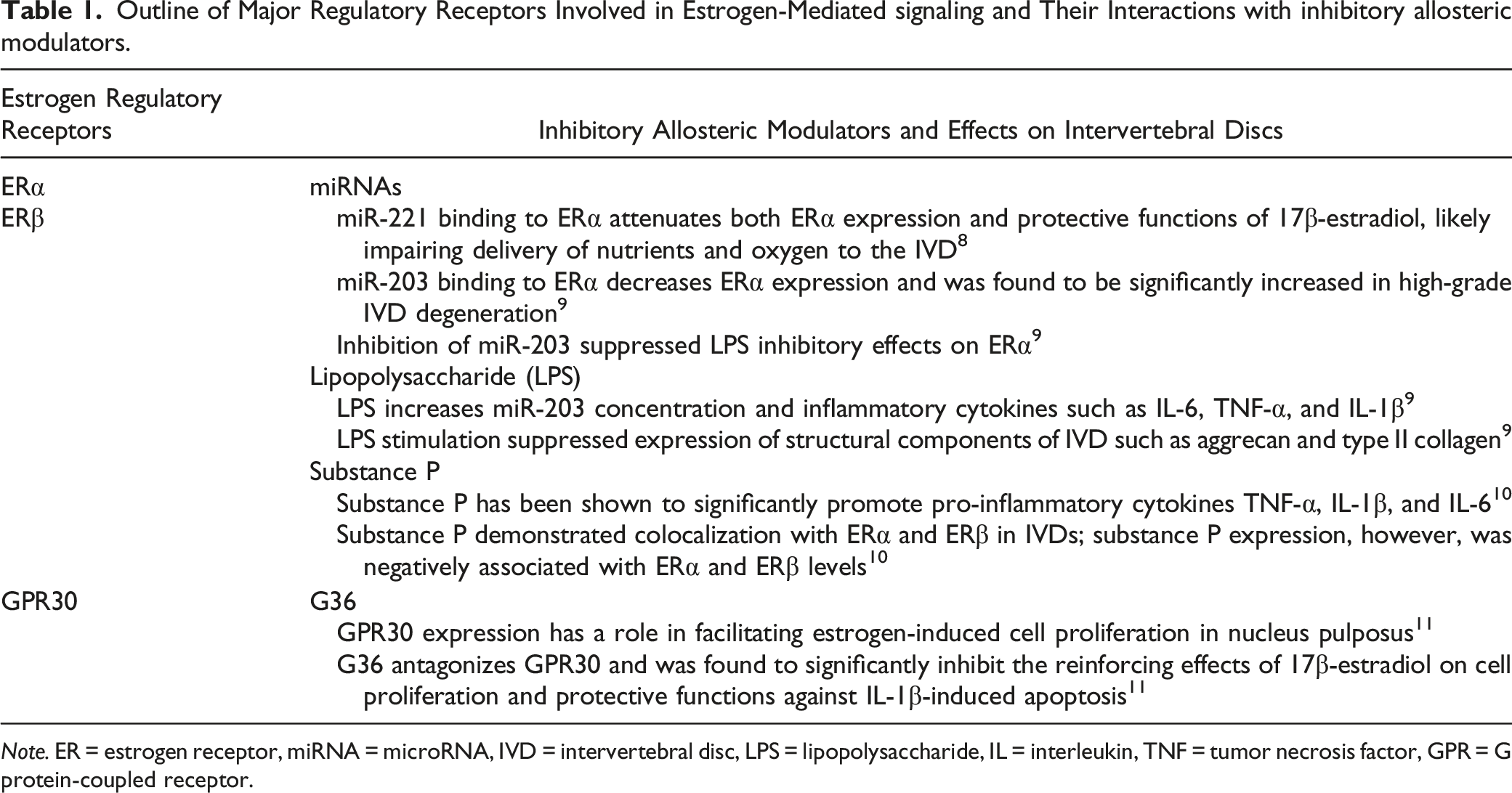
Note. ER = estrogen receptor, miRNA = microRNA, IVD = intervertebral disc, LPS = lipopolysaccharide, IL = interleukin, TNF = tumor necrosis factor, GPR = G protein-coupled receptor.
Intercommunication between estrogen receptors (ERs) and various microRNAs (miRNA) has been theorized to effectuate DDD. In a functional genomic analysis, Sheng et al showed that miR-221 inhibition was associated with preservation of TGF- β levels relative to samples without miR-221 inhibitors. TGF-β has been widely established as an anti-inflammatory cytokine integral to the synthesis and maintenance of core structural components comprising the IVD. 8 As such, conclusions from this study suggest contributory roles for miRNAs in the pathogenesis of DDD. Cai et al identified another miRNA subtype, miR-203-3p, in which levels correlated negatively with ERα expression; their findings are indicative of suppressive effects as a consequence of intermolecular interactions between miR-203-3p and ERα. This notion is further substantiated by prior studies which found significantly higher miR-203-3p levels within the NPs of higher severity DDD patients. 9 These findings have also been reproduced with various contexts. Using combined bilateral ovariectomy with intraarticular monosodium iodoacetate injections, Tian et al created postmenopausal rat models to characterize the protective function of ERα signaling on cartilage degeneration. The study observed significant improvements in cellular inflammation and cartilage destruction when using miR-203 specific inhibitors within the rat postmenopausal models and thereby highlight clinically relevant applications with use of estrogen-based therapy targets. 12
Estrogen has also been shown to exert its effects through G protein-coupled estrogen receptors. Wei et al affirmed this premise in a study using G36, a GPR30 antagonist, and ERα/ERβ antagonists where addition of these individual inhibitors suppressed IVD cellular proliferation. Furthermore, introduction of the two in tandem led to complete absence of cellular proliferation–this confirms the presence of multiple mechanisms by which estrogen is protective against degenerative processes. 10
Prior studies have also investigated intradiscal interactions between other molecular compounds and ERs; Elevated levels of Substance P for example, has been proposed as a predictor of pain severity in DDD. 13 Song et al investigated underlying processes driving this effect using immunoreactive staining within NPs of postmenopausal women – their analysis revealed significant colocalization of ERα/β and SP peptides along with a negative association between ER expression and SP concentration. 10 Song et al further characterized the impact of SP on estrogen regulation using DDD female mice models. The study observed significantly increased levels of estrogen-regulated proinflammatory cytokines, specifically TNF-α, IL-1β, and IL-6, in the presence of SP analogues. These findings suggest SP inhibition of estrogen’s anti-inflammatory effects and elucidates another pathway through which estrogen regulates cytokine activity as it relates to DDD. 14 This association may offer a pathway through which estrogen regulates cytokine activity.
Although estrogen has been extensively studied in the setting of disc degeneration, studies on its counterpart, testosterone, remain scarce. Bertolo et al conducted a study to elucidate the potential of testosterone supplementation for DDD. The study noted chondrogenesis upon introduction of testosterone to IVD and mesenchymal cells. Chondrogenesis, specifically of the structural essentials of the NP (proteoglycan, collagen II, aggrecan), was seen only in male IVD. 15 Though the specific mechanism is unclear, the authors propose a process involving translocation of the testosterone-androgen receptor complex to the cell nucleus; this is believed to induce transcription of the c-FOS/c-JUN complex which is responsible for ECM deposition within the IVD.
Section 3: Clinical Studies Specific to the Spine
Several studies have demonstrated the clinical significance of estrogen as it relates to intervertebral disc degeneration. Baron et al examined average disc heights of the 12th thoracic and 3rd lumbar vertebrae in 100 women, of which 23 were pre-menopausal, 33 were post-menopausal not on hormone replacement therapy (HRT), and 44 were post-menopausal on HRT. 16 In comparison to both pre-menopausal and post-menopausal on HRT, post-menopausal women not on HRT were found to have significantly decreased disc heights. The authors concluded from these results that women who are estrogen-replete are more likely to maintain intervertebral disc height than estrogen deficient women. A similar study by Lou et al investigating intervertebral disc height in pre- and post-menopausal women analyzed and graded a total of 4230 discs were analyzed and graded using the modified Pfirrmann grading system. 17 Post-menopausal women were found to have more severe disc degeneration than pre-menopausal women, with, and the majority of degeneration occurring the first 15 years after menopause. The authors conducted an age-, height-, and weight-matched study comparing disc generation in 1382 men and 1566 women using the modified Pfirrmann grading system. 18 Women were found to have more severe disc degeneration than men, suggesting that estrogen is likely an important factor in maintaining intervertebral disc integrity.
Gambacciani et al evaluated the effects of menopause on the intervertebral disc using dual-energy X-Ray absorptiometry (DEXA) to measure disc space in a cohort of 464 women. 19 Disc space measurements were found to remain stable between the ages of 20 and 50 years,, after which point measurements were noted to significantly decrease. Accordingly, post-menopausal women were significantly more likely to have decreased disc space compared to pre- and peri-menopausal women, with loss of disc height most commonly occurring in the first 5-10 years post-menopause. The authors concluded from these findings that the rapid decrease in estrogen that occurs in menopause may significantly affect disc metabolism.
Section 4: Conclusion
There is ample human and animal research delineating the association between estrogen and the health of the intervertebral discs. As described in this review, estrogen impacts the IVD by regulating various processes. Estrogen mediates vascular perfusion and nutrient diffusion, both of which are imperative to maintaining IVD integrity. Furthermore, estrogen supports cells by secreting ECM products and maintaining adequate water content within the disc structure. Beyond supportive roles, estrogen also enacts protective functions by inhibiting apoptosis and upregulating anti-inflammatory cytokines. Contrastingly, little is known about how testosterone affects health of IVDs. Despite ample evidence from basic science research to validate the association between low estrogen levels and worsening disc degeneration, few studies have analyzed sex hormone deficiencies in context of clinically significant disc degeneration–specifically DDD. Addressing this gap within the clinical setting may abet the translation of findings from molecular analyses into novel, clinically relevant therapies for DDD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.