
Abstract
Study Design:
Literature review.
Objectives:
Systematic review of the existing literature to determine the safety of minimally invasive (MI) sacroiliac (SI) joint fusion through the determination of the rate of procedural and device-related intraoperative and postoperative complications.
Methods:
All original studies with reported complication rates were included for analysis. Complications were defined as procedural if secondary to the MI surgery and device related if caused by placement of the implant. Complication rates are reported using descriptive statistics. Random-effects meta-analysis was performed for preoperative and postoperative Visual Analog Score (VAS) pain ratings and Oswestry Disability Index (ODI) scores.
Results:
Fourteen studies of 720 patients (499 females/221 males) with a mean follow-up of 22 months were included. Ninety-nine patients (13.75%) underwent bilateral SI joint arthrodesis resulting in a total of 819 SI joints fused. There were 91 reported procedural-related complications (11.11%) with the most common adverse event being surgical wound infection/drainage (n = 17). Twenty-five adverse events were attributed to be secondary to placement of the implant (3.05%) with nerve root impingement (n = 13) being the most common. The revision rate was 2.56%. MI SI joint fusion reduced VAS scores from 82.42 (95% confidence interval [CI] 79.34-85.51) to 29.03 (95% CI 25.05-33.01) and ODI scores from 57.44 (95% CI 54.73-60.14) to 29.42 (95% CI 20.62-38.21).
Conclusions:
MI SI joint fusion is a relatively safe procedure but is not without certain risks. Further work must be done to optimize the procedure’s complication profile. Possible areas of improvement include preoperative patient optimization, operative technique, and use of intraoperative real-time imaging.
Introduction
Chronic lower back pain is a problem encountered frequently in the primary care setting and certainly in the spine surgeon’s office. It is a public health epidemic, and in highly developed countries, it is one of the top 3 causes of degradation in quality-adjusted life years, along with ischemic heart disease and chronic obstructive pulmonary disease. 1 Although the differential diagnosis for lower back pain is quite broad and the lumbar spine is certainly an important pain generator in many of these patients, sacroiliac (SI) joint pathology cannot be ignored. The SI joint has been implicated as a source of chronic low back pain in 15% to 30% of patients. 2,3 Sembrano and Polly found that of 200 patients with the chief complaint of low back pain and no prior history of spine, SI joint, or hip surgery, 65% had pain attributed to the spine only, while 5% were attributed to the SI joint only and 14.5% were attributed to both. 4 Although it is certainly not a rare cause of low back pain, SI joint dysfunction remains as a diagnosis of exclusion at this time. In any patient with lower back pain, the lumbar spine should be cleared before turning attention to the SI joint as the possible source of discomfort.
The SI joint functions to transfer force and energy from the spine to the pelvis. Proper functioning of the SI joint requires articular congruity with balanced muscular and ligamentous attachments. 5 Imbalances between the two can result in increased or asymmetric stress through the joint leading to pathological motion and pain. This discomfort is a result of the presence of abundant nociceptive receptors 6 and mechanoreceptors 7 in the joint along with innervation from the dorsal sacral nerve root. The ablation of this nerve root has been attempted as a nonoperative treatment option for SI joint pain with good albeit temporary results. 8,9 Other nonsurgical treatment options for SI joint pain include medical management with anti-inflammatory medications, weight loss, physical therapy, chiropractic manipulation, and intraarticular steroid injections. Apart from radiofrequency ablation, no high-quality evidence exists to support the efficacy of nonsurgical treatment for SI joint pain. 10
SI joint arthrodesis was originally described in the early 1920s by Smith-Petersen 11 and first performed using an open approach, which is an invasive procedure with high morbidity and minimal to moderate effectiveness. 12 Open SI joint fusion is associated with prolonged hospital stays and recovery times, high nonunion rates, poor long-term response rates, intraoperative blood loss, and low levels of satisfaction. 13 Additionally, the open operation requires a relatively large incision, autograft bone harvesting, and the avoidance of weight bearing postoperatively. 14 Recent advancements both in the field of spine surgery and radiology have led to a development of a minimally invasive (MI) approach to perform SI joint arthrodesis. 14 The MI technique has increased in popularity as it has been shown to be associated with minimal blood loss, less surgery time, decreased length of hospital admission, and a lower reoperation rate. 15,20 Currently, 90% of all SI joint fusions are performed using the MI technique with open arthrodesis now mostly reserved for traumatic pelvic ring fractures. 13 Although less morbid compared with the open procedure, MI SI arthrodesis is not without the risk of adverse events or complications. Due to its recently gained popularity, literature addressing the complications of this surgical procedure is scarce. To the best of the authors’ knowledge, this is the most comprehensive study to date examining the safety profile of MI SI joint fusion and the first to directly assess industry sponsorship in the MI SI joint fusion literature.
Methods
Minimally Invasive Surgical Technique Overview
MI SI joint fusion is performed under general endotracheal anesthesia with the patient in the prone position on a radiolucent table. Using fluoroscopy, inlet, outlet, and lateral sacral views should be obtained with visualization of the sacral ala line, anterior/posterior sacral lines, and S1 foramen. A 3- to 5-cm incision is made over the lateral buttock. Gluteal fascia is bluntly dissected and gluteus maximus is split in the direction of its fibers down to the outer table of the ilium. Under indirect visualization using fluoroscopic guidance, a guidewire is passed through the ilium, over the SI joint, and into the sacrum superior, lateral, or inferior to the S1 foramen depending on the number of implants inserted and the surgeon’s preference. A depth gauge is used to determine implant length. A soft tissue protector is passed over the wire and a hand drill or broach is used to decorticate the bone. A pin-guide system is used to place the implant in the desired location of arthrodesis. Most patients receive 2 to 3 implants to stabilize the SI joint. The incision is irrigated and tissue layers closed. Postoperatively, physical therapy is initiated immediately and the patient is instructed to be toe-touch weight bearing for a period for 3 weeks. Weight bearing status is then progressed as tolerated until patient is ambulating bearing full weight.
Study Design
Two independent reviewers performed a systematic review and meta-analysis of the literature according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The databases queried included PubMed and Scopus and the selected search terms were “sacroiliac joint AND arthrodesis OR fusion.” In addition to these database searches, the bibliographies of selected articles were examined for additional studies not retrieved in the original database search. The search terms were intentionally broad to minimize excluded relevant studies. A third reviewer was designated to resolve disagreements regarding study inclusion and data collection. All original studies published in the English language consisting of at least 3 patients with reported complication rates for MI SI joint fusion were included for analysis. The quality of selected articles was quantified using the modified Coleman Methodology Score. Case reports and insurance claim database studies were not included. We only examined studies utilizing the lateral transarticular approach. All articles involving non–minimally invasive open surgery, a dorsal surgical approach, or the management of infection, malignancy, or fractures were excluded. In studies with overlapping cohorts, the article with shortest mean follow-up was excluded. Complications were defined as procedural if reported as secondary to the MI surgery and device related if directly caused by placement of the implant device across the joint. Study patients had received the diagnosis of either dysfunction or osteoarthritis of the SI joint. All included studies excluded patients with rheumatoid arthritis and ankylosing spondylitis. Diagnosis of SI joint pathology was only obtained after pain relief with a SI joint analgesic injection to confirm the SI joint was the pain generator. Information extracted from each study included demographic data, sample size (baseline and follow-up), trial design, type of implant used, length of follow-up, number of bilateral cases, number of adverse events or complications, preoperative and postoperative pain scores, and preoperative and postoperative disability scores. Subjective pain was quantified by the Visual Analog Scale (VAS), which allows patients to rank current pain on a scale of 0 to 10. VAS scores recorded on a scale of 0 to 100 were converted to the 0 to 10 scale to facilitate statistical analysis. Disability due to SI joint dysfunction was measured using the Oswestry Disability Index (ODI). Only studies providing both mean and standard deviation values for both preoperative and postoperative VAS or ODI scores were included in the meta-analysis portion of the study. Postoperative VAS and ODI scores were taken from the last recorded follow-up. Random effects meta-analysis using the Comprehensive Meta-Analysis software was performed for the patient-reported outcomes measures to quantify the efficacy of MI fusion in pain reduction and improving patient functionality. Patient satisfaction with the MI SI joint fusion procedure and willingness to have the same surgery again were also recorded. Last, each included article was reviewed for industry funding and potential conflicts of interest. This systematic review and meta-analysis received no outside financial assistance.
Results
Our database search yielded 259 results in PubMed and 370 in Scopus. After duplicates, non-English papers, abstracts, and nonhuman studies were removed, a total of 210 articles remained. These articles were screened and studies involving fractures (11), case reports (18), malignancy/tumors (8), biomechanics (19), anatomy/cadavers (10), basic science (4), open fusion (15), radiology (31), nonoperative therapeutic treatments (17), epidemiology (9), other surgical procedures (26), pathology (6), financial efficacy (8), and infections (5) were excluded. Of the remaining 23 studies, 9 consisted of overlapping cohorts and were also excluded (Figure 1).
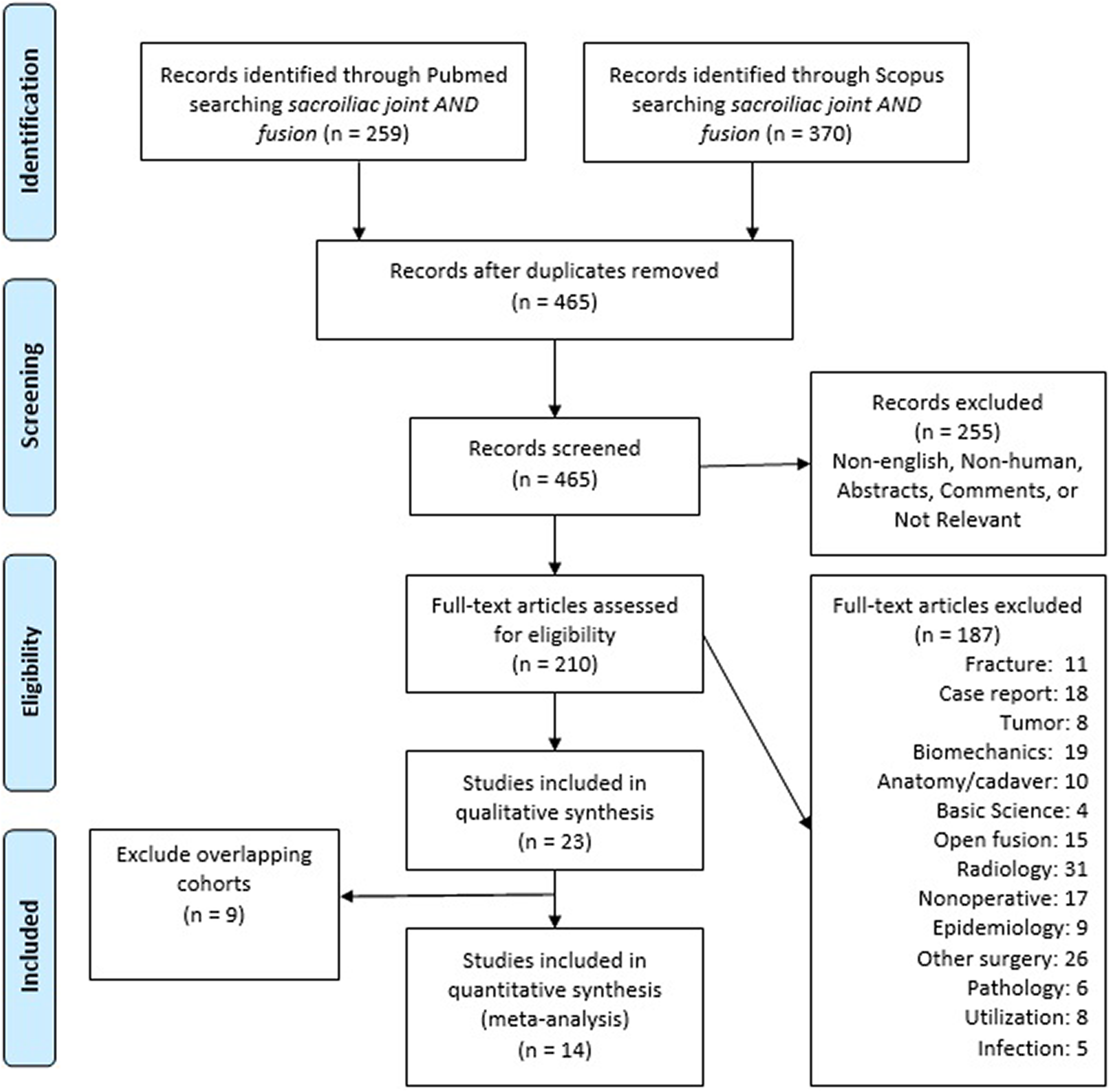
PRISMA diagram illustrating literature search.
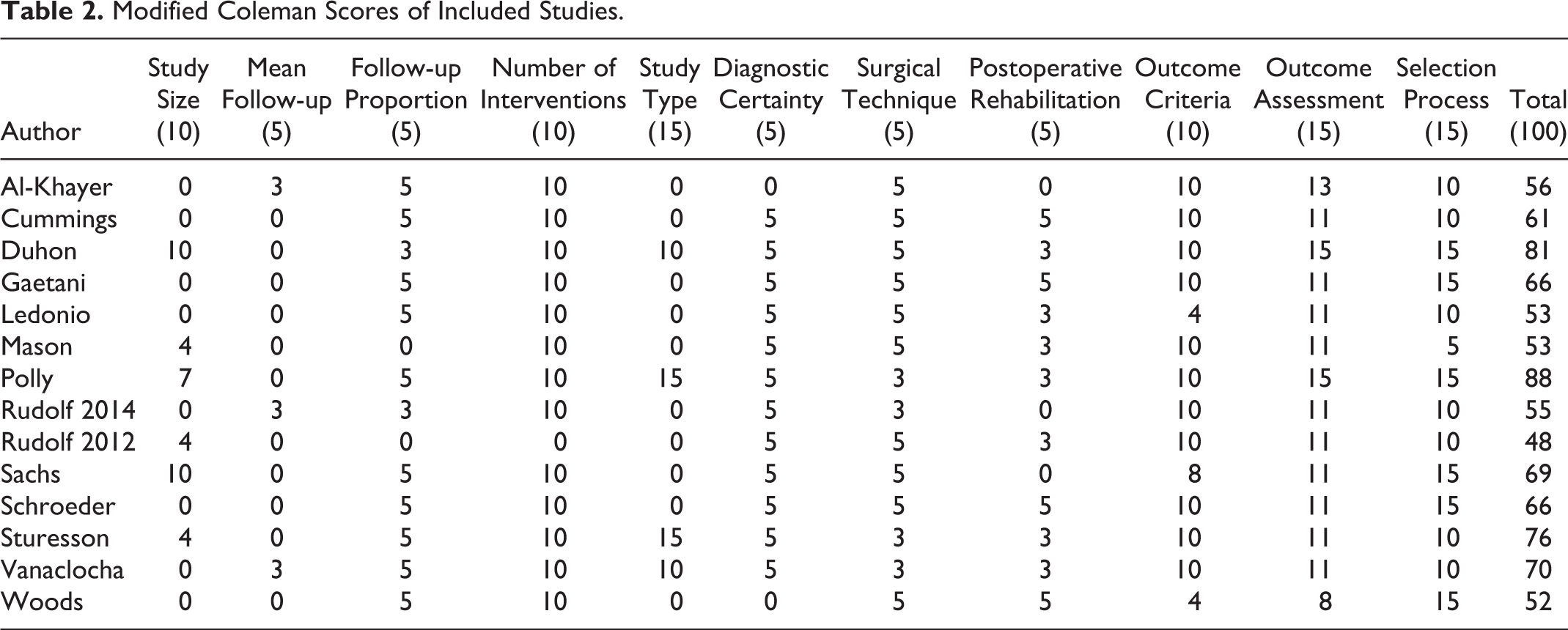
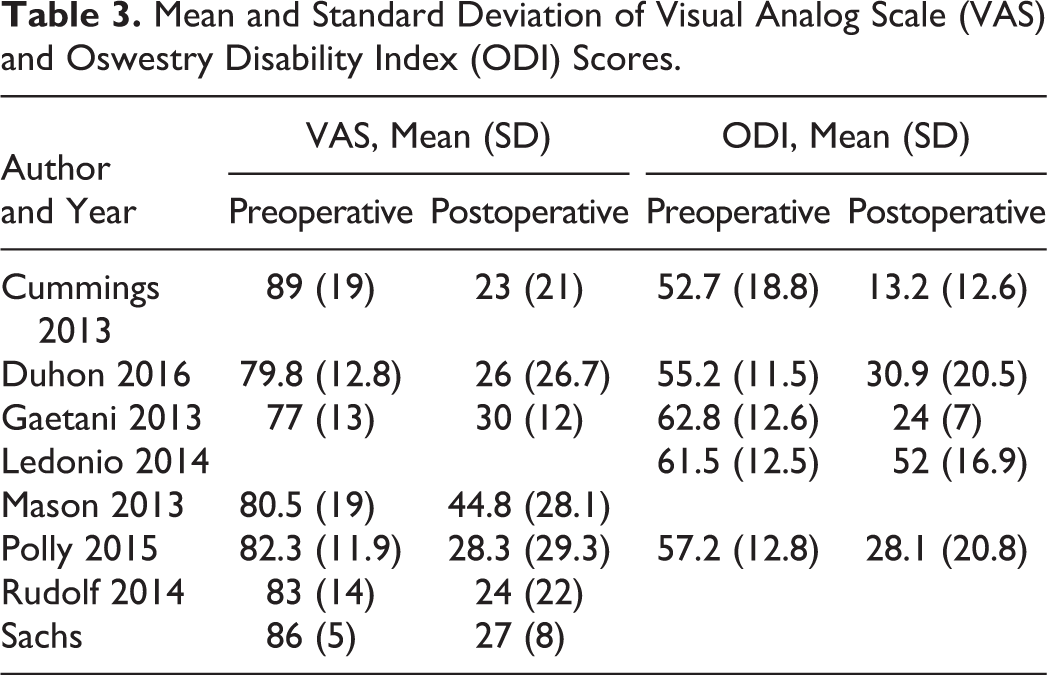
A total of 14 articles 10,16 -28 met our inclusion criteria and were included in our systematic review and meta-analysis (Table 1). The mean modified Coleman Methodology Score was 63.9 (range 48-88) with a standard deviation of 11.6 (Table 2). We included 7 retrospective single-center case series, 16,17,19,22,23,25,28 2 prospective multicenter randomized controlled trials, 10,26 2 prospective single-center case series, 21,27 1 prospective multicenter comparative cohort study, 18 1 retrospective multicenter case series, 24 and 1 retrospective single-center comparative cohort study. 20 Seven studies 10,17 -19,21,22,24 reported the mean and standard deviation of preoperative and postoperative VAS scores, while 5 studies 10,17 -20 provided the mean and standard deviation of preoperative and postoperative ODI values (Table 3). Twelve of the studies 10,17 -20,22 -28 investigated triangular porous titanium plasma spray coated implants, while 2 studies 16,21 used hollow modular anchorage screws packed with demineralized bone matrix. Seven articles received industry-sponsored funding, and 8 articles had at least one author with a relevant disclosure listed.
Demographic Information.
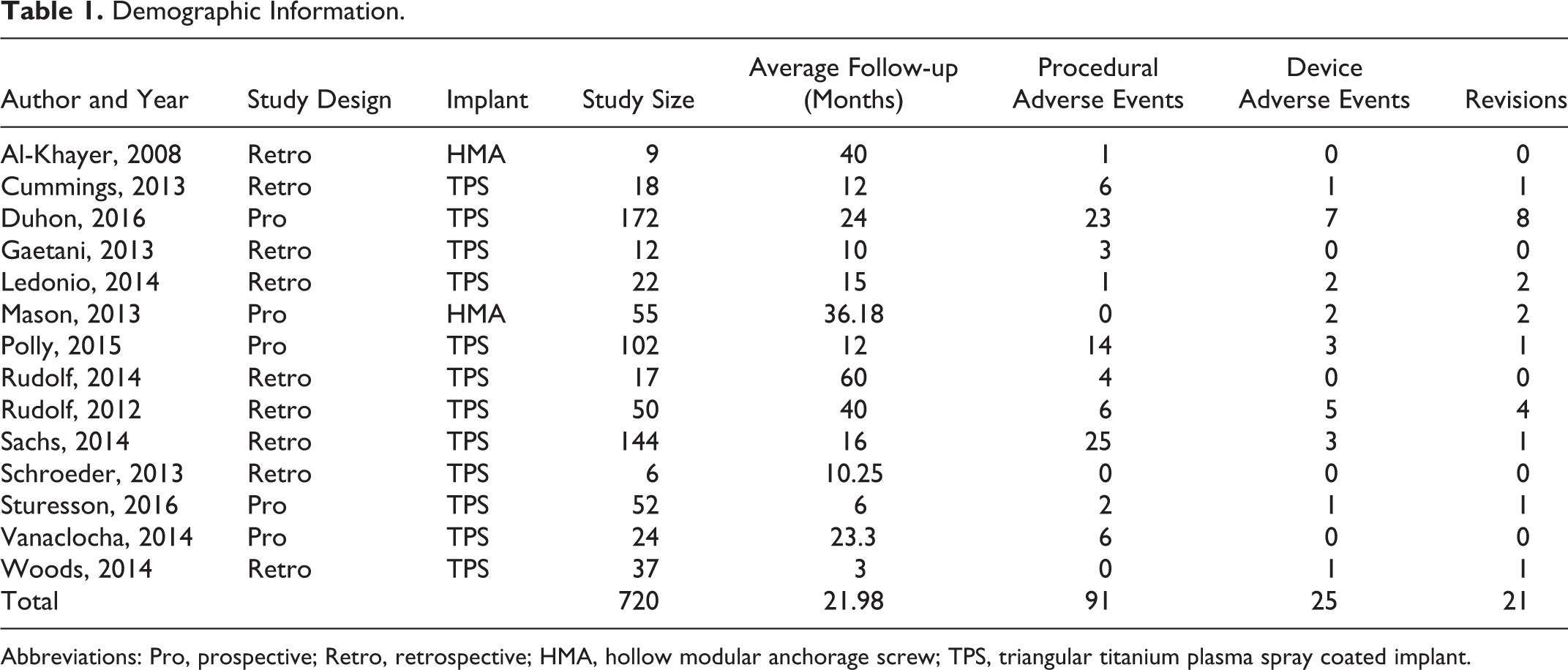
Abbreviations: Pro, prospective; Retro, retrospective; HMA, hollow modular anchorage screw; TPS, triangular titanium plasma spray coated implant.
Modified Coleman Scores of Included Studies.
Mean and Standard Deviation of Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) Scores.
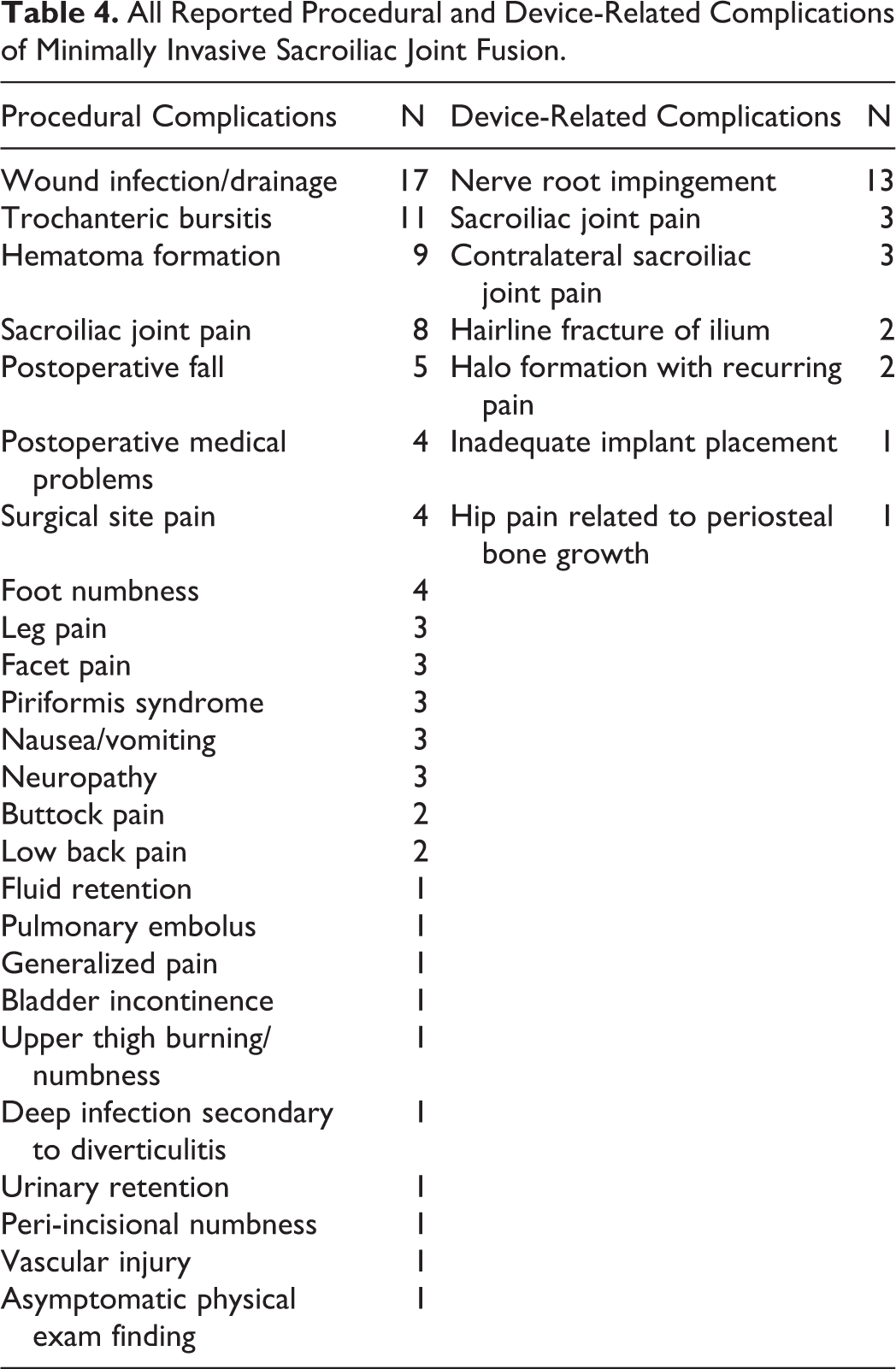
A total of 720 patients (499 females/221 males) with a mean follow-up of 22 months were included in the analysis. Ninety-nine patients (13.75%) underwent bilateral SI joint arthrodesis resulting in a total of 819 SI joints fused. There were 91 documented procedure-related complications (11.11%) with the most common adverse events being surgical wound infection/drainage (n = 17; 2.07%), trochanteric bursitis (n = 11; 1.34%), and hematoma formation (n = 9; 1.10%). Twenty-five adverse events were attributed to be directly caused by the implant device (3.05%) with nerve root impingement (n = 13; 1.59%) being the most common (Table 4). The rate of revision was found to be 2.56%. The association between the type of implant and device related complications was not statistically significant (P = .955).
All Reported Procedural and Device-Related Complications of Minimally Invasive Sacroiliac Joint Fusion.
MI SI joint fusion reduced VAS pain scores from 82.42 (95% confidence interval [CI] 79.34-85.51) to 29.03 (95% CI 25.05-33.01) and ODI scores from 57.44 (95% CI 54.73-60.14) to 29.42 (95% CI 20.62-38.21). Patient satisfaction with outcomes was high at 93.14%, with 86.01% stating they would have the same surgery again.
Discussion
While proven in the literature to be superior to the open approach, the results of the current study suggest that MI SI joint fusion is associated with a significant number of perioperative and postoperative complications. In our study, we distinguish between adverse events secondary to the surgical procedure and adverse events caused by the SI joint spanning implant. Procedural complications are defined as risks present in any invasive surgical procedure such as bleeding and infection, as well as adverse events associated with hospital admission such as pneumonia. The total surgical time, risk to surrounding structures, blood loss, and possibility of intraoperative imaging are some of the factors that determine the risk for procedural complications. Our analysis revealed that MI SI joint fusion has a total procedural complication rate of 11.11%, with the most common adverse events being wound infection, trochanteric bursitis, and hematoma formation.
Consistent with our results, Heiney et al reported surgical wound infection as the most common complication associated with the procedure in a systematic review of 432 subjects. They do, however, report a higher rate of wound-related complications than our study (3.9% vs 2.1%). 29 This may be explained by the fact that Heiney et al included hematoma formation as a wound complication while we report hematoma formation as a separate surgical adverse event. Consistent with our study, they report trochanteric bursitis as a surgical complication with a rate of 1.85% while we list it as 1.53%. 29
Device-related complications can be contributed to the actual implant used for SI joint arthrodesis. We found an overall device-related adverse event rate of 3.05% with the most common being nerve root impingement followed by both ipsilateral and contralateral SI joint pain. The location of the SI joint places the lower lumbar and sacral nerves roots at risk during this procedure. An improperly placed implant can easily stress one of these nerve roots resulting in immediate radicular symptoms postoperatively. This complication is corrected by taking the patient back to the operating room and backing the implant up or repositioning it altogether. The revision rate in our analysis was found to be 2.56%. The etiology of both ipsilateral and contralateral postoperative SI joint discomfort is unclear. Some physicians hypothesize that stabilizing one side alters the biomechanics of the contralateral SI joint leading to SI joint dysfunction later. Of note, this belief has not been substantiated in the literature at this time.
In the previously mentioned retrospective review, Heiney et al found a rate of nerve root impingement following SI joint fusion of 2.08%, which is slightly higher than our reported value of 1.80%. 29 In another study investigating adverse events reported to the device manufacturer (SI-BONE, Inc), Miller et al reported an overall complication rate of 3.8% in 5319 patients. These complications include nerve impingement, hematoma, iliac fracture, wound infection, device migration, and implant malposition. 30 Other complications reported in the literature at a lower frequency include piriformis syndrome, facet joint pain, and toe numbness. In a retrospective study of 40 patients with 1-year follow-up, Sachs et al reported a relatively high rate of facet joint pain of 20%. 31 This finding can possibly be attributed to underlying lumbar spine pathology. We suggest that SI joint dysfunction be a diagnosis of exclusion and MI SI joint fusion only performed when all other possible pain generators are cleared. The overall rate of postoperative complications reported by Sachs et al was 32.5%, which is significantly higher than our reported overall complication rate of 11.11%. 31 Again, this can be explained by preoperative lumbar spine degenerative disease.
Intraoperative imaging, implant type, and the surgeon’s familiarity with the procedure and relevant anatomy certainly play a role in reducing the rate of complications. In a systemic review of postoperative complications associated with minimally invasive spine procedures, Sclafani and Kim report that with 20 to 30 consecutive cases surgeons can overcome the learning curve with respect to operative time and risk of complication. 32 Given the wide range of institutions represented in our patient cohort, we are unable to confirm the surgeons’ level of comfort and familiarity with the MI SI joint fusion procedure. A closer look at the incidence of adverse events at high-volume versus low-volume centers is warranted to further define this relationship.
Absent or poor intraoperative imaging is an additional risk factor for complications associated with this procedure. More specifically, poor visualization can lead to implant malposition and subsequent lower lumbar or sacral nerve root impingement requiring revision. Miller et al reported a revision rate as high as 0.9% in the early postoperative period for treatment of a symptomatic malpositioned implant. 30 Careful evaluation of preoperative computed tomography (CT) and intraoperative fluoroscopic views (inlet, outlet, lateral, and oblique) is essential for proper implant placement. Implants must cross the SI joint while remaining fully contained within the SI osseous envelope to avoid iatrogenic nerve injury. The use of CT-guided procedures in MI spine surgery has increased in use, and subsequently lowered the complication rate in many procedures. 33 Given the high variability in sacral and iliac wing anatomy, the use of a surgical navigation system utilizing intraoperative CT can potentially reduce the complication rate by allowing surgeons to optimize correct implant position and minimize iatrogenic nerve injury.
Regardless of the risk of perioperative and postoperative adverse events, good patient postoperative satisfaction scores have been reported in the literature. In a 5-year study of clinical and radiographic outcomes, Rudolf et al showed VAS pain scores improved from 83 to 24 following MI SI joint fusion. Furthermore, they concluded 88% of their patient cohort reached substantial clinical benefit at 12 months, which was maintained for 5 years. 22 Similarly, Sachs et al showed an average improvement of 78 VAS pain score points after a follow-up period of 12 months of 40 patients. 31 In another case series of 50 patients, Rudolf et al reported a statistically significant improvement in pain and functional scores independent of a history of lumbar spine fusion. 23 Our results were consistent with the previously stated studies. We showed an improvement in VAS scores of 53.39 points and ODI scores of 28.02 points. Most important, 93.14% of our patients were satisfied with their outcome and 86.01% stated they would have the same procedure again.
Last, the degree of industry involvement in the MI SI joint arthrodesis literature was examined. Seven of the included articles (50.0%) received industry-sponsored funding, and 8 studies (57.1%) had at least one author with a relevant disclosure. In a review of clinical trials on http://www.clinicaltrials.gov, Cher and Capobianco found that 90.5% of randomized multicenter trials with at least one site in the United States were financed by industry. 34 Nonetheless, the possibility of financial conflicts of interest may leave some readers skeptical of reported results. A well-designed, prospective, and independently financed study of MI SI joint fusion would certainly be well received by those interested in the procedure.
Limitations of the current study can be attributed to its systematic review design and the previously mentioned industry involvement. It is reliant on the work of other spine surgeons with significant variability in experience and comfort level with the procedure. Although the authors performed a comprehensive literature review, the incomplete retrieval of information is a possibility. Additionally, publication bias should not be ignored as series with overwhelmingly negative results may not be submitted or accepted for publication. Also, certain complications deemed as minor by some may be underreported in the selected studies.
In conclusion, MI SI joint fusion is a relatively safe procedure; however, it is associated with certain risks and adverse events that must be considered before the procedure is performed. Further high-quality studies are needed to enhance or minimize associated complications with technology such as improved intraoperative real-time imaging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.