
Abstract
Study Design
Prospective Cohort Study.
Objective
The present study aims to determine if the racial representation of patients enrolled in a large prospective scoliosis registry is reflective of the general United States population. Further, we studied whether there was an association between race, pre-operative parameters, outcomes and loss to follow-up.
Methods
Prospectively collected data for patients who underwent spinal fusion for adolescent idiopathic scoliosis (AIS) was reviewed, including self-reported race/ethnicity. The U.S. pediatric population and U.S. patients enrolled in the prospective registry were compared. The data obtained was analyzed for variations between races, for pre-operative variables and follow-up.
Results
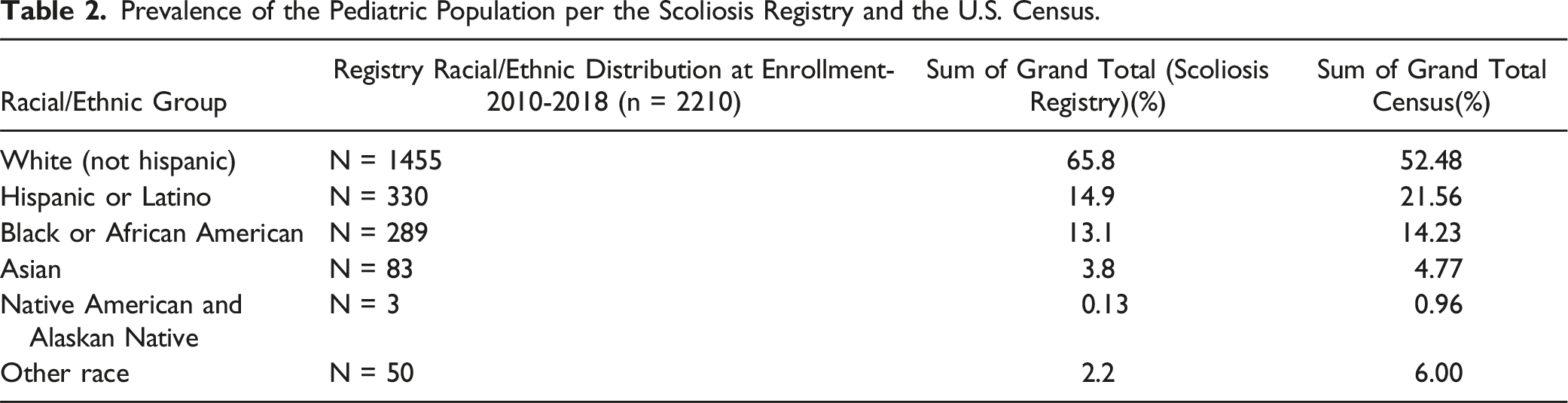
Of the 2210 included patients in the registry 66% of patients reported as White, while 52% of the 2018 U.S. pediatric population reported as White. 15% of the registry reported as Hispanic/Latino compared to 22% of the U.S. pediatric population, 13% Black compared to 14% of the U.S. pediatric population, and 4% Asian compared to 5% of the U.S. pediatric population. Asian and White patients had statistically significant higher 2-year follow-up in all but one of six enrollment sites (P < 0.001). Native American, Other, and Hispanic/Latino patients had the highest BMIs. Native American and Black patients had the highest pre-op thoracic Cobb angles. Pre-op ages of Black, Hispanic, and Native American patients were statistically lower (P < 0.01).
Conclusion
This study demonstrates the association between race and patient follow-up and pre-operative factors in patients who underwent surgery for AIS. Black, Native American, and Hispanic populations were underrepresented both at pre-op and follow-up when compared to their relative proportion in the U.S. pediatric population.
Introduction
Despite continued progress in healthcare, disparities in access to quality medical care continue to impact health outcomes across different communities and populations. While some illnesses and prognoses are attributable to inheritance within ethnic and racial groups, studies have shown that clinicians are not always fully informed of the lifestyle and struggles that vulnerable populations face. Inequity in medicine continues to affect vulnerable populations and patients that identify with underrepresented and underserved racial or ethnic identities. 1 Social determinants of health compound with racial and ethnic disparities at every level of health care systems. Black maternal mortality is a prominent contemporary example of these disparities in health, with a disproportionate and multi-factorial increase in morbidity and mortality affecting Black women in the United States. 2 Cultural differences, implicit biases, and patterns of mistrust guide care and follow-up for pediatric and adult populations. Within surgical outcomes, a 2006 Medicare study concluded that Black patients have higher mortality for 88% of surgical procedures and that worse socioeconomic status (SES) translated to increased surgical mortality. 3 This may be caused by generalizations from limited data availability sourced from single selected populations, thereby guiding clinical practices and public health measures that are not accurately reflective of the population. 4
Existing research addressing the relationship between race/ethnicity on scoliosis progression and outcomes is limited. Within the adolescent idiopathic scoliosis (AIS) population specifically, Zavatsky et al, have found that Black patients had larger curve magnitudes, larger curves in the surgical range, may select surgery as an initial management procedure, and that race had more of an impact on disease severity than SES. 5 Higher BMI was also associated with increased Cobb angle at presentation. 6 Additionally, although race had a minimal impact on 30-day surgical outcomes in AIS patients, Black patients were most likely in the lowest income quartile of this population. 7 Conversely, a retrospective chart review done at the University of Texas suggested that disease severity measured by Cobb angle at presentation was not influenced by ethnicity. 8 However, this analysis used data limited to a single county that was not reflective of the general U.S. pediatric population. Considering previous research, future priorities should include engaging more marginalized groups in research; it is vital that registries are representative of a larger cohort so that findings can be appropriately applied to the national population.
Thus, our study aimed to compare the racial distribution of a large prospective multicenter scoliosis registry to the U.S. population. The secondary aim was to illustrate any potential differences in preoperative factors and loss to follow-up, which has shown to not only affect a patient’s prognosis after surgery but can be important in determining the validity for future studies that utilize this nation scoliosis registry. 9 The hypothesis in the present study was that the scoliosis registry was representative of the national pediatric population’s racial proportions, and that ethnic minorities would have higher pre-op Cobb angles and an increased loss to follow up when compared to white patients.
Materials and Methods
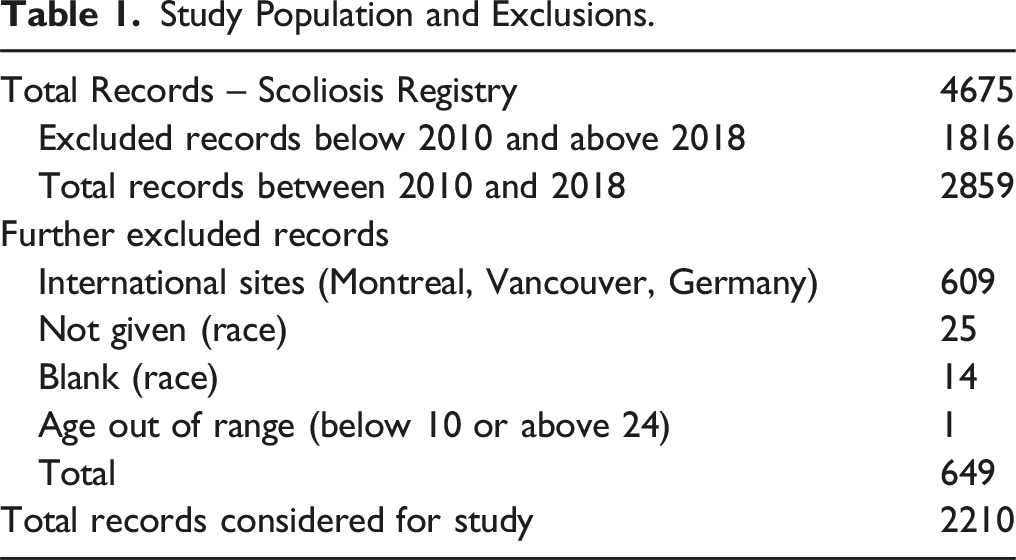
Study Population and Exclusions.
Ethics Approval
The institutional ethics approval was obtained for the study. Patients/parents/legal guardians prospectively consented to participate in the registry study (IRB 19-001728), and informed consent for use of anonymized patient information was obtained.
Data Collection
The data was collected for the United States pediatric population and demographics from Annie E. Casey Foundation Kids Count Data Center. 10 We compared the racial/ethnic distribution of a large scoliosis registry for those enrolled between 2010-2018 to the U.S. population between the years 2010-2018. While the registry also contains data from health systems in Canada and Germany, these sites were omitted to more accurately compare populations. The data was analyzed for the various ethnicities and the racial distribution of the intended population, with race being self-reported by the individual patients/parents/legal guardians at the time of enrollment. For the purpose of this study, individuals reporting two or more races were categorized as ‘Other’.
Statistical Analysis
Data was evaluated using the JMP 17.1.0 (SAS, Cary, NC). Standard descriptive statistics such as mean as well as the standard deviation were reported. The values obtained were compared for clinical variables such as BMI, pre-operative age, preoperative thoracic and lumbar Cobb angles, and for loss to follow-up using Chi-square tests. A level of significance of P < 0.05 was considered significant.
Results
In the present study, a total of 4675 patients with AIS who were included in the registry narrowed to a study population of 2210 finalized for consideration. Patients outside of the study years, aged below 10 or above 24, from non-U.S. enrollment sites, or with no reported race were excluded (Table 1). Of the 2210 patients with AIS who were enrolled between 2010 and 2018, 65.8% (n = 1455) of patients reported as White.
Prevalence of the Pediatric Population per the Scoliosis Registry and the U.S. Census.
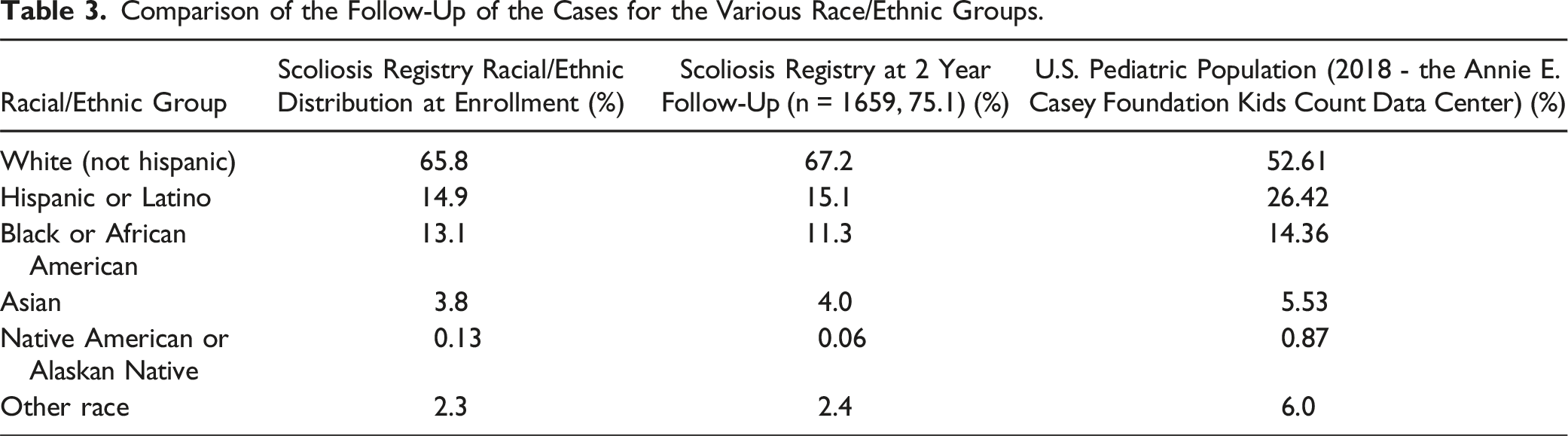
Comparison of the Follow-Up of the Cases for the Various Race/Ethnic Groups.
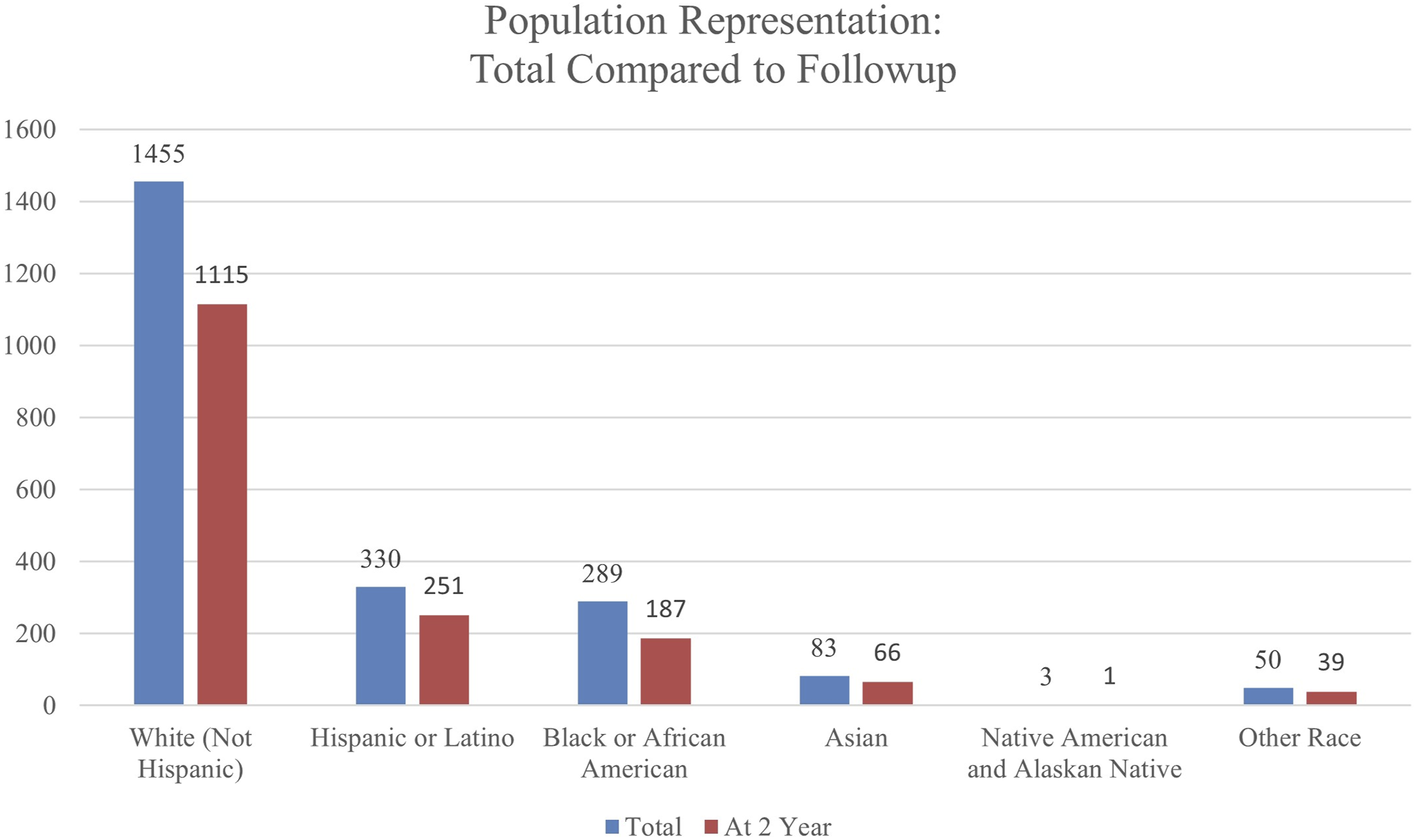
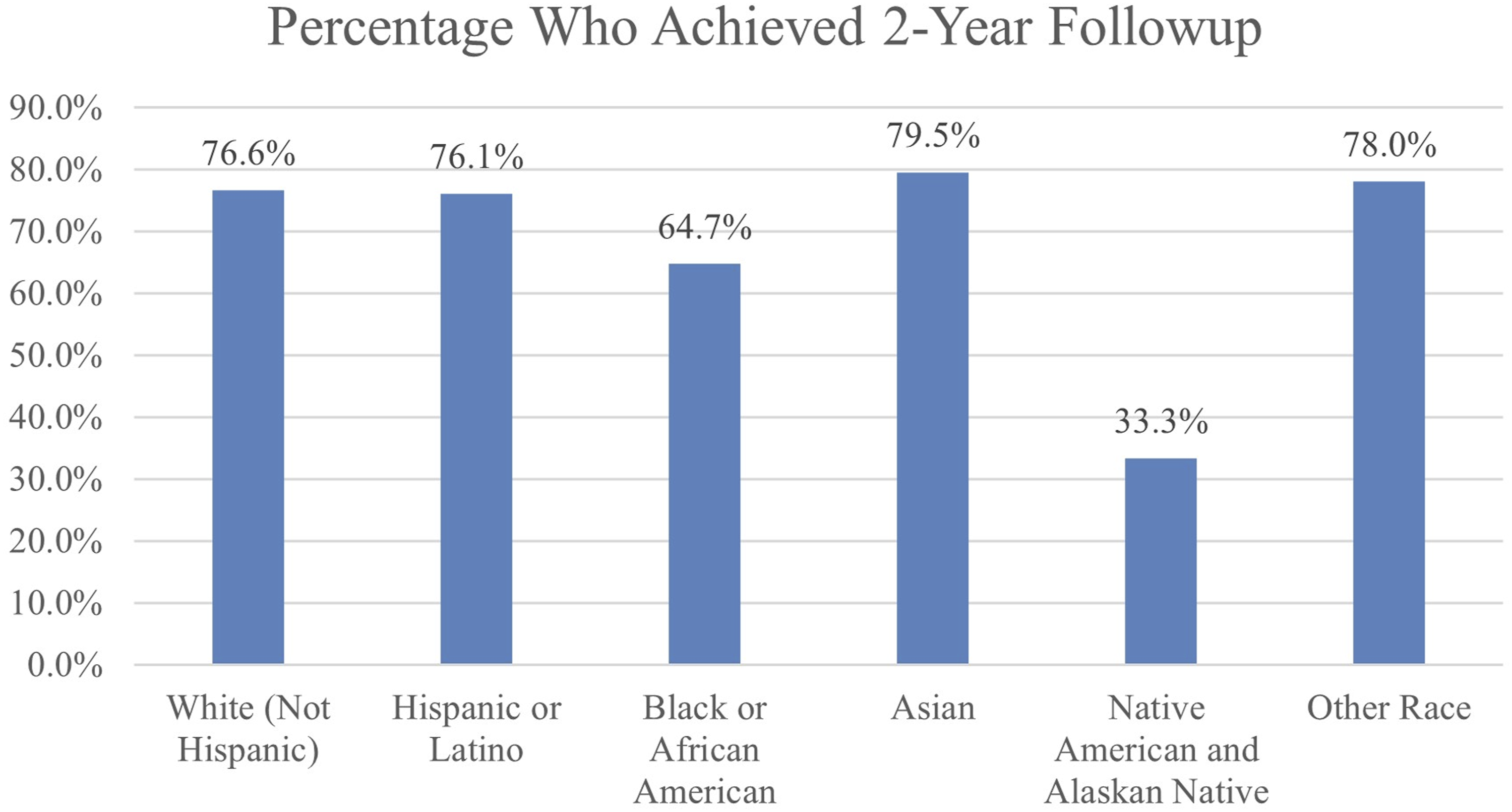
Distribution of the patients based on the race/ethnicity at the end of 2-year follow-up.
Comparison of the groups for the follow-up periods.
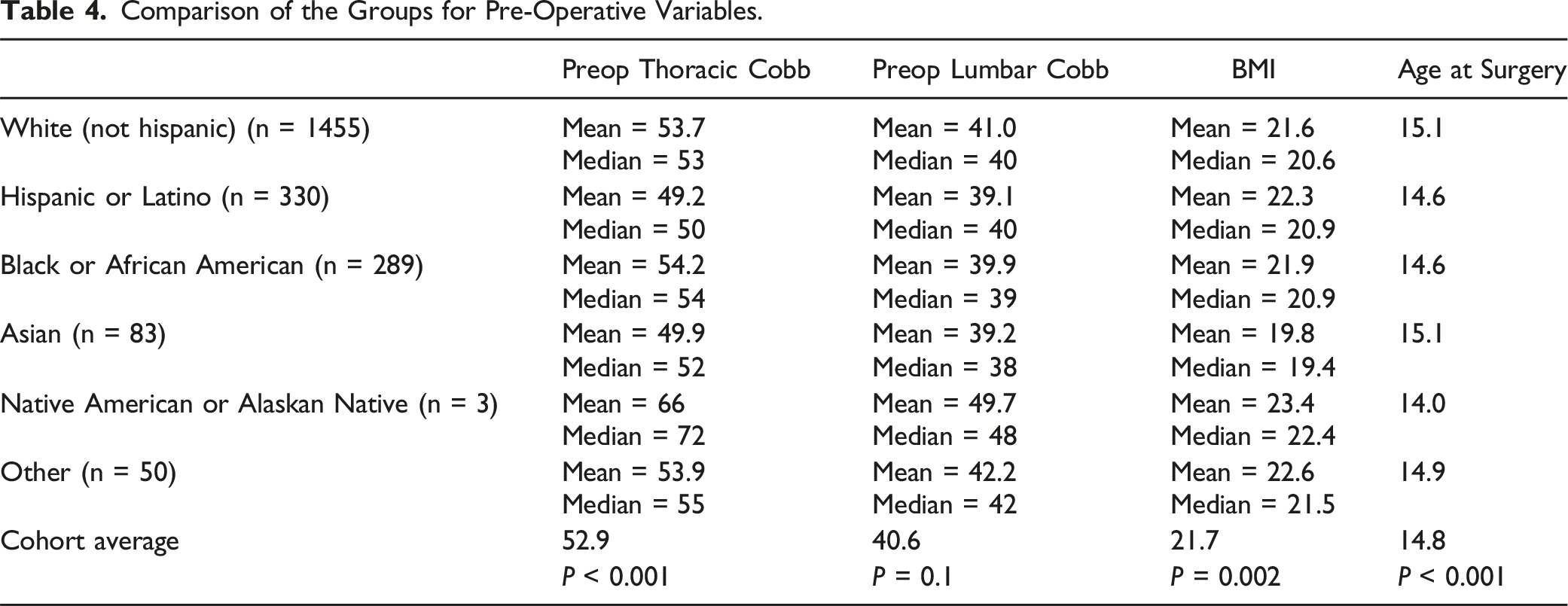
Comparison of the Groups for Pre-Operative Variables.
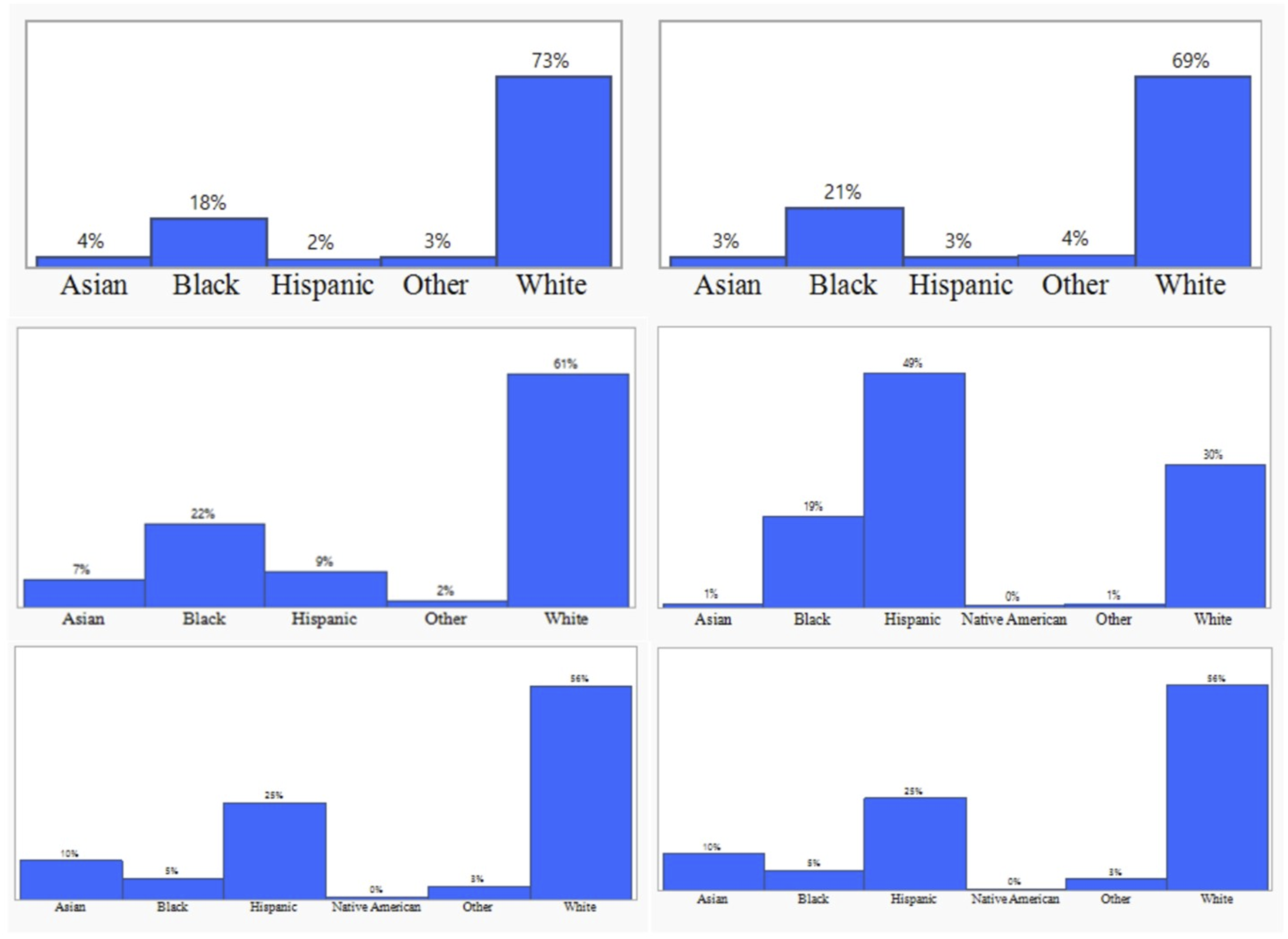
Subset examples of the enrollment sites for the representation of different races/ethnicities.
Discussion
AIS is thought to affect all populations equally, with no predisposition associated with race suspected, although severe scoliosis is much more frequent in females compared to males. 11 Genetic factors have been implicated in the incidence of the AIS; thereby, AIS incidence may vary between populations. 12 AIS is the most common spine deformity in children and can affect health-related quality of life, self-image, and pulmonary function in adulthood. 13 Ideally, all populations should have access to AIS surgical care and be represented in AIS prospective clinical research. Prospective data from large multicenter registries play a large role in advancing patient care through research. This data reflects the quality and generalizability of the registry data to U.S. patients and whether historically under-represented groups are included in the study population. Thus, it is important to have such a registry represent the wide spectrum of the U.S. pediatric population. Further, we sought to determine whether there were differences in baseline demographics by race for patients enrolled in the registry and whether they were successfully followed for two years.
Our study’s first aim was to determine whether patient demographics in a large prospective registry are representative of the U.S. pediatric population as a whole. We found that there was reasonable representation of Black, Hispanic, and Asian patients, but less than the U.S. pediatric population with room for improved enrollment in these groups. Native American/Alaskan Native patients were severely under-represented, which could be addressed with addition of enrollment sites. Since the time of this study, the registry has added new sites including Colorado, Washington, Georgia, and Minnesota, which may help address these challenges and work toward serving wider populations. In addition, it is possible that patients and parents from under-represented racial and ethnic groups are declining enrollment in the registry. These differences between racial and ethnic groups have systemic, historical, social, and cultural foundations. Patients who are racial minorities, for example, have been demonstrated to be more prone to decline suggested treatments, experience difficulty following treatment regimens, and delay seeking care. These actions are most often attributed to a lack of understanding of a patient’s viewpoint on the health condition, a lack of cultural fit between provider and patient, or a lack of communication from the provider.1,5,14-16
Evaluating differences in patient follow-up, Asian (79.5%) and White (76.6%) patients reported higher 2-year follow-up rates than other races in the present study. This factor has potential impact for differential longitudinal outcomes in these patient groups. Health care coverage policies and clinical procedures are examples of potential barriers that affect patient access to care.17,18 We also found that patients reporting Black, Native American, and Other racial/ethnic group had larger thoracic curve magnitudes at the time of surgery. Though these values indicate statistical significance, the average peroperative thoracic cobb measurements of each group are within 3 degrees of the overall average, indicating potential for variations in measurement of cobb contributing to these differences. Access to care and rates of surgical procedures have known racial differences.15,18 To reduce surgical inequalities, more studies are needed to understand variables including the duration between diagnosis and surgical referral, as well as delays in accessing treatment. 14 While several of these differences were statistically significant, the clinical significance of these metrics requires further consideration.
Nuno et al previously evaluated inequities for treatment and outcomes with the management of idiopathic scoliosis patients in the U.S. 16 They concluded that there was significant disparity between the outcome as well as the choice of treatment for populations of different races. When compared, Black orthopedic patients had a greater operative mortality and morbidity than White orthopedic patients across multiple surgical modalities.19,20 In the present study there was a significant variation between the races for all the parameters considered, including the preoperative factors of BMI, age, thoracic and lumbar Cobb angles. The Hispanic and Latino, Black, and Native American groups had the highest pre-op BMI and Cobb angles, congruent with previous research demonstrating a positive association between the two factors. 21 Black, Hispanic and Native American patient groups were also younger than their White and Asian counterparts, similar to previous findings that Black patients were more likely to be recommended surgery at the first visit. The factors contributing to younger age at surgery for underrepresented populations does require further research, with some theorized contributors including lack of preoperative bracing and shared decision making. Additionally, Tarrant et al. showed that severe preoperative spinal curvatures were linked with longer surgical length, greater blood loss, and delayed return to school. 22 The more severe preoperative spine curvatures relation to surgical results indicates Black patients may be increased risk for poor outcomes.
There are several limitations to this study. We only evaluated the impact of race/ethnicity; factors including gender/sex, socioeconomic status, educational differences were not studied. From the registry data, race and ethnicity are self-reported by the patients and families. Further, modern reporting verbiage such as used by the U.S. Census bureau was not utilized, and thus reporting of multi-race or race plus ethnicity was not clearly separated. Thus, the category of ‘other’ reported in this study may include multiple groups. Our study did not evaluate enrollment patterns at the individual sites or whether the racial/ethnic distribution at each site was representative of the regional population as we aimed to evaluate whether the registry would be representative of the US population on the larger scale. There was significant variation in racial/ethnic distribution among the sites (Figure 3). Further in-depth studies are warranted to elucidate the causes for lower registry enrollment among patients who reported Black, Native American and other race/ethnicity.
This study compares the racial disparity between a large scoliosis registry and the U.S. census from data collected over a period of 8 years among AIS patients. Large multicenter registries are helpful in addressing national trends in health resource consumption, health care, and disparities. They are especially important in analysis of patient safety and outcomes, necessitating study populations that reflect the diversity of the patient population. It can be concluded within the limitations of the study that in the United States, there was a significant relationship between race and patient follow-up and pre-operative factors among patients who underwent surgery for adolescent idiopathic scoliosis. Asian and White patients had higher proportions of 2-year follow-up and older ages at surgery. Black and Native American patients had higher pre-operative Cobb angles, while Native American and Hispanic/Latino patients had the higher BMIs. These gaps could relate to variations in patient access to healthcare facilities and cultural variables that influence the patient-doctor relationship. The differential rate of follow-up establsihes an area for action, with a need for further intentional effort to provide continued communication and care for underrepresented patients. Additional studies are needed to understand the impact of these discrepancies and outcomes on quality-of-life indicators and future health resources. Continued and growing efforts must prioritize health equity practices of health literacy, social services, outreach, and assistance to serve underserved patients. Future investigations assessing the effect of race and other social determinants on surgical outcomes are needed to highlight potential differences, prioritize ongoing efforts to recruit a wide variety of patients, and address barriers in access to equitable healthcare.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Julia Todderud, Bharadwaj Jilakara or any member of his or her immediate family, has no funding or commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. Setting Scoliosis Straight Foundation receives research grants from DePuy Synthes Spine, Medtronic Spine, ZimVie, NuVasive, Stryker Spine, Atec/EOS Imaging in support of Harms Study Group research. Dr Larson reports consulting activities with OrthoPediatrics, Medtronic, Zimmer Biomet, Depuy Synthes, and Globus Medical outside of the submitted work. Ms. Marks reports she is employed at Setting Scoliosis Straight Foundation. Dr Newton reports grants/research support to his institution from Depuy Synthes, EOS Imaging, Scoliosis Research Society Stryker Spine, Alphatech, Setting Scoliosis Straight Foundation, and royalties from Depuy Synthes, Thieme Publishing, Stryker/K2M, and consulting feeds from Depuy Synthes, Stryker/K2M, MiRus, Globus Medical, Pacira, and Medtronic, and other stock with Accelus and with Spinology. Dr Fletcher reports consulting activities with Medtronic, CRICO, and Orthopediatrics and research funding from Harrison Foundation, Scoliosis Research Society, and 1998 Society outside of the submitted work. Dr Pahys reports consulting with DePuy Synthes, Nuvasive, and ZimVie outside of the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
Institutional review board approval was obtained for all aspects of this study (IRB #19-001728).