
Abstract
Background
Adolescent idiopathic scoliosis represents a complex three-dimensional spinal deformity of unknown etiology. It frequently results in visible deformities, decreased daily functional capacity, impaired pulmonary function, and psychological distress. Personalized treatment options for adolescent idiopathic scoliosis include exercise therapy, brace use, and surgical intervention, tailored to individual patient needs. Exercise therapy is often employed for patients with mild-to-moderate adolescent idiopathic scoliosis, those undergoing postoperative rehabilitation, or those ineligible for surgery because of its noninvasive nature, low cost, ease of application, and avoidance of prolonged brace use. However, a unified standard or guideline for the use of exercise therapy in managing adolescent idiopathic scoliosis is lacking. This study aimed to investigate the clinical efficacy of exercise therapy for adolescent idiopathic scoliosis and evaluate its therapeutic significance.
Methods
We conducted a systematic review by searching several databases, including China National Knowledge Infrastructure, Wanfang, PubMed, Web of Science, Excerpta Medica Database, MEDLINE, Ovid, and Cochrane Library, with no language restriction, to retrieve randomized controlled trials on exercise therapy for scoliosis. Meta-analysis was performed using RevMan 5.4. The protocol was registered with PROSPERO (registry number: CRD420251106878).
Results
A total of 9 studies involving 571 patients with adolescent idiopathic scoliosis were included. The pooled results revealed that the mean difference for the impact on Cobb angle was 3.31 (95% confidence interval: 2.56–4.05; P < 0.00001), indicating a statistically significant difference (P < 0.05). Regarding angulation of trunk rotation, the mean difference was 2.80 (95% confidence interval: 1.90–3.70; P < 0.00001), indicating a statistically significant difference (P < 0.05). For the Scoliosis Research Society-22 scores, the mean differences were as follows: pain, mean difference = 0.64 (95% confidence interval: 0.10–1.19; P = 0.02); function/activity, mean difference = 0.83 (95% confidence interval: 0.20–1.45; P = 0.009); self-image, mean difference = 0.51 (95% confidence interval: 0.10–0.91; P = 0.01); mental health, mean difference = 0.18 (95% confidence interval: 0.13–0.48; P = 0.25); and satisfaction with treatment, mean difference = 1.36 (95% confidence interval: 0.41–2.32; P = 0.005). Statistically significant differences were observed in all scores except for mental health (P < 0.05).
Conclusion
Specific spinal exercise therapy has demonstrated effectiveness in improving Cobb angle, correcting angulation of trunk rotation measurements, and positively impacting pain, functional activity, and self-image compared with other non-exercise conservative treatments, resulting in higher patient satisfaction with treatment outcomes.
Introduction
Scoliosis is a three-dimensional spinal deformity, defined as a spinal curvature exceeding 10° in the coronal plane toward the lateral side. 1 The potential causes of scoliosis include congenital spinal abnormalities, tumors, trauma, infectious diseases, and neuromuscular disorders.2–4 Scoliosis with identifiable causes excluded is generally referred to as idiopathic scoliosis. Adolescent idiopathic scoliosis (AIS), which commonly occurs in adolescents aged 10–18 years, is the most prevalent type, with a reported prevalence of 0.47%–5.20%.5–7 The spine has considerable growth potential during adolescence, representing the second peak of human development. Without timely treatment, AIS often leads to trunk deformity, limited spinal mobility, low back pain, impaired lung function, and other complications. Furthermore, the incidence of psychological disorders among these patients is significantly higher than that among their healthy peers due to their abnormal appearance.8–9 Various treatment options, such as exercise therapy, orthotic brace use, and surgery, are available depending on patient needs. Among these, exercise therapy is considered one of the most effective treatment approaches for patients with mild-to-moderate scoliosis or those who are not candidates for surgery. Most studies suggest that exercise therapy is primarily applicable to AIS patients with skeletal immaturity (Risser sign ≤ grade 3), those with mild scoliosis (10° ≤ Cobb angle ≤ 25°), and those at risk of progression. However, significant controversy remains regarding the specific timing and selection of indications, and unified standards for treatment methods and clinical efficacy evaluation of exercise therapy in AIS are lacking.6,10–12 Although numerous studies have investigated exercise therapy, these are limited by small sample sizes, low-quality evidence, and substantial heterogeneity. Recent developments in exercise therapy have demonstrated increased individualization and treatment precision as well as greater adoption of combined treatment strategies. Advances in mechanistic research have provided improved guidance for therapy. With the development of remote communication technologies and artificial intelligence, patients can now access standardized exercise therapy at home, improving treatment adherence and enabling the collection of extensive long-term follow-up data. This represents a marked difference from the research environment of previous studies on exercise therapy. This study has fully incorporated the latest advancements in exercise therapy for AIS from both domestic and international sources, without language restrictions, and has considered the changes brought about by this new environment, aiming to provide references for clinical treatment method selection.
Methods
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 13 The protocol was registered with PROSPERO (registry number: CRD420251106878).
Inclusion and exclusion criteria
The inclusion criteria were as follows: (a) patients with AIS; (b) a randomized controlled trial (RCT); (c) participants in the experimental group receiving exercise therapy, including physiotherapy scoliosis-specific exercises (PSSE) and general exercise therapy, while participants in the control group receiving conservative treatments other than exercise therapy, such as health education or bracing; (d) clearly defined and comparable control and experimental groups; and (e) outcome measures presented as continuous variables following a normal distribution and expressed as x ± s.
The exclusion criteria were as follows: (a) self-controlled studies and (b) participants who had undergone surgical treatment for scoliosis.
Literature search
This meta-analysis used keywords such as “exercise therapy,” “physiotherapy,” “functional exercise,” “non-operative treatment,” “adolescent idiopathic scoliosis,” “scoliosis,” and “AIS” to search several databases, including China National Knowledge Infrastructure (CNKI), Wanfang, PubMed, Embase, MEDLINE, Ovid, Cochrane Library, and Web of Science, with no language restrictions. The focus was on screening RCTs evaluating exercise therapy for scoliosis, with search strategies adjusted according to the characteristics of each database. The search period spanned from the inception of each database to January 2025.
Identification of studies
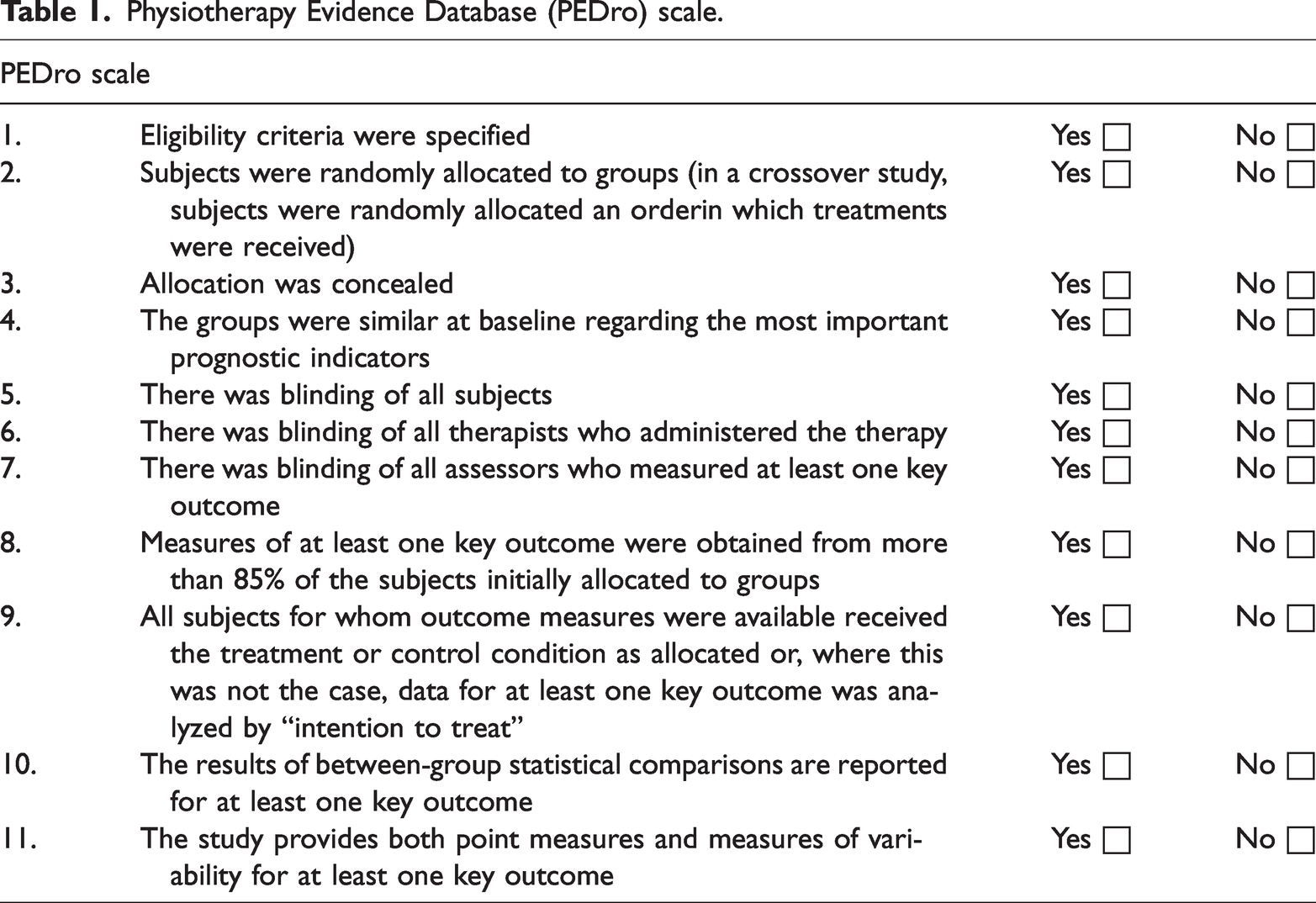
Two independent reviewers applied the eligibility criteria to select potentially relevant studies based on titles and abstracts from the aforementioned databases. Consensus was reached regarding study inclusion. The full texts of the studies meeting the eligibility criteria were then retrieved. Data were collected in the same manner by two independent reviewers. For each study, the following information was recorded: author, year of publication, sample size, average age of participants, sex ratio, intervention measures, intervention duration, Cobb angle, trunk rotation angle, and Scoliosis Research Society-22 (SRS-22) questionnaire scores (including self-image, pain, function/activity, mental health, and satisfaction with treatment scores). A third reviewer resolved any doubts or disagreements that arose during the study selection process. Two independent reviewers also assessed the methodological quality of the included controlled clinical trials using the Physiotherapy Evidence Database (PEDro) scale (Table 1). A total of 11 criteria were employed, with 1 point awarded for meeting each criterion. The retrieved literature was scored independently by both reviewers.
Physiotherapy Evidence Database (PEDro) scale.
Statistical analysis
The extracted data were analyzed to obtain the differences before and after treatment, and a meta-analysis was performed using RevMan 5.4. The mean difference (MD) and 95% confidence interval (CI) were used as the effect size measures. The analysis was conducted as follows: (1) Heterogeneity among the included studies was assessed. If the P-value was >0.1 and I2 value was ≤50%, heterogeneity was considered acceptable, and a fixed-effects model was used. (2) If the P-value was ≤0.1 and I2 value was >50%, heterogeneity was present, and a random-effects model was applied. (3) The P-value of the combined effect size was obtained. If the P-value was <0.05, the combined statistic was considered statistically significant, indicating that the data could be pooled. If the P-value was >0.05, the combined statistic was not statistically significant. (4) Heterogeneity was further explored through sensitivity analysis, and a parallel descriptive analysis was conducted.
Results
Search results
A total of 1827 studies were initially retrieved, and 9 RCTs were ultimately included after successive screening.14–22 The literature screening process and results are shown in Figure 1.

Article selection process.
Characteristics of the included studies
The 9 RCTs included in this study involved a total of 571 participants, with 285 in the experimental group and 286 in the control group. All participants were adolescents aged 10–18 years. Participants in the experimental group received various exercise therapies, including PSSE, whereas those in the control group received other non-exercise conservative treatments. The intervention period ranged from 12 weeks to 12 months. Specific details are provided in Table 2.
Characteristics of the included studies.

N: number of participants; T: treatment group; C: control group; PSSE: physiotherapy scoliosis-specific exercises; SEAS: Scientific Exercise Approach to Scoliosis; BSPTS: Barcelona Scoliosis Physical Therapy School.
Quality evaluation
This meta-analysis included five high-quality studies (scores ranging from 9 to 11) and four medium-quality studies (scores ranging from 6 to 8) (Table 3). Most studies did not employ blinding of therapists and participants, potentially introducing implementation and measurement biases.
Methodological quality of the included studies (PEDro scale scores).

PEDro: Physiotherapy Evidence Database.
Outcomes
Effect of exercise therapy on Cobb angle in patients with AIS
A total of 8 studies (involving 481 participants, with 240 in the experimental group and 241 in the control group) reported the Cobb angle before and after treatment.14,15,17–22 Differences in Cobb angle before and after treatment were calculated using the raw data. The heterogeneity test revealed a P-value of 0.93 and I2 value of 0%, indicating no heterogeneity. A fixed-effects model was used for analysis, and the combined statistical results were as follows: MD = 3.31, 95% CI: 2.56–4.05, P < 0.00001. The outcome measure was statistically significant (P < 0.05), indicating that exercise therapy effectively corrected the spinal Cobb angle in patients with AIS (Figure 2).

Forest plot of Cobb angle.
Effect of exercise therapy on angulation of trunk rotation (ATR) in patients with AIS
A total of 6 studies (involving 386 participants, with 192 in the experimental group and 194 in the control group) reported ATR before and after treatment.14,15,17,18,21,22 However, the intervention program in the study by Gu 17 differed significantly from that in the other five studies; hence, this study was excluded from the statistical meta-analysis. Differences in ATR before and after treatment were calculated using the raw data. The heterogeneity test revealed a P-value of 0.0003 and I2 value of 81%, indicating high heterogeneity. After excluding the study by Wu et al., 18 the heterogeneity decreased significantly (I2 = 49% and P = 0.12). A review of the original publications suggested that differences in sample sizes contributed to the heterogeneity. A random-effects model was used for analysis, and the combined statistical results were as follows: MD = 2.80, 95% CI: 1.90–3.70, P < 0.00001). The outcome measure was statistically significant (P < 0.05), indicating that exercise therapy effectively corrected ATR in patients with AIS (Figure 3).

Forest plot of ATR. ATR: angulation of trunk rotation.
Effect of exercise therapy on SRS-22 scale scores in patients with AIS
A total of 4 studies (involving 249 participants, with 124 in the experimental group and 125 in the control group) reported SRS-22 scale scores before and after treatment.14–17 Differences in SRS-22 scores before and after treatment were calculated using the raw data. Heterogeneity tests revealed high heterogeneity for pain (P < 0.00001, I2 = 97%), function (P < 0.00001, I2 = 97%), self-image (P = 0.0002, I2 = 85%), mental health (P = 0.01, I2 = 73%), and satisfaction with treatment (P < 0.00001, I2 = 94%). A random-effects model was used for analysis, and the combined statistical results were as follows: pain, MD = 0.64 (95% CI: 0.10–1.19, P = 0.02); function, MD = 0.83 (95% CI: 0.20–1.45, P = 0.009); self-image, MD = 0.51 (95% CI: 0.10–0.91, P = 0.01); mental health, MD = 0.18 (95% CI: −0.13 to 0.48, P = 0.25); and satisfaction with treatment, MD = 1.36 (95% CI: 0.41–2.32, P = 0.005). The results indicated that except for mental health scores, differences in the other four scores were statistically significant (P < 0.05) (Figure 4). Subsequent exclusion of studies one by one revealed that after excluding the study by Miao and Zhang, 16 heterogeneity for SRS-22 pain scores revealed a P-value of 0.63 and I2 value of 0%; heterogeneity for SRS-22 function scores, P = 0.62 and I2 = 0%; and heterogeneity for SRS-22 mental health scores, P = 0.38 and I2 = 0%. Heterogeneity was significantly reduced, presumably due to the shorter 12-week intervention period in this study compared with that in the other studies.

Forest plot of SRS-22 scale scores. SRS-22: Scoliosis Research Society-22.
Bias and sensitivity analyses
Assessment of literature bias
The correction degree of the Cobb angle before and after treatment was used to assess publication bias. The included studies exhibited an asymmetrical distribution, indicating the presence of publication bias. This may be attributed to small sample sizes or less rigorous experimental designs (Figure 5).

Funnel plot of Cobb angle.
Assessment of literature sensitivity
Effect sizes were repeatedly switched, studies were added or removed, and the effect models were changed using RevMan 5.4. The final results showed no significant differences, indicating that the findings of this meta-analysis are robust and reliable.
Discussion
This study conducted a systematic review of the literature on the efficacy of exercise therapy for treating AIS. The results indicated that scoliosis-specific exercises effectively improved patients’ Cobb angles, corrected their ATR degrees, and positively impacted pain, functional activities, and self-image compared with other non-exercise conservative treatments, resulting in higher treatment satisfaction.
The SRS recognizes the Cobb angle as the gold standard for assessing the treatment outcomes of scoliosis. The findings of this study indicated that patients in the exercise therapy group exhibited a greater reduction in Cobb angle compared with those in the control group, with a statistically significant difference (P < 0.05). This may be attributed to the fact that exercises specifically designed for scoliosis can open the concavity of the spine, thereby correcting spinal deformities. Additionally, core stability training activates the muscles surrounding the spine, enabling interaction between the spine and paraspinal muscles, stretching concave-side muscles and ligaments, and forming a protective layer around the spine to maintain a neutral position, gradually reducing the curvature. Deformities can also be corrected by improving posture and enhancing proprioceptive training. Core muscle training strengthens the muscles surrounding the spine, stabilizing the spine and slowing the progression of spinal curvature. Patients are guided to perform chest and spinal exercises in various positions, and respiratory training is incorporated into their daily routines. This helps correct abnormal respiratory patterns in patients with AIS, resulting in a degree of reduction in Cobb angle. However, a consensus exists that a correction of ≥5° in Cobb angle is adequate. Based on this criterion, the reported effectiveness of exercise therapy for AIS varies significantly. Four studies in this review showed an average correction of ≥5° in Cobb angle with exercise therapy, whereas another four studies indicated an average correction of <5°.23–29 One study reported a Cobb angle correction of 13.2° with exercise therapy; however, its evidence level was grade IV. 30 Therefore, relying solely on the degree of Cobb angle correction to evaluate the efficacy of exercise therapy for AIS is inadequate. Furthermore, most Cobb angle measurements are conducted manually, leading to significant measurement variability, which inevitably affects research outcomes. 31
Considering the limitations and narrow focus of using Cobb angle alone to evaluate the effectiveness of exercise therapy, many scholars have incorporated ATR into the assessment system. Bunnell proposed in 1984 that a scoliometer could be used to measure ATR, aiding in the assessment of AIS severity. 32 Numerous studies have confirmed the reliability of spinal rotation measurement instruments and found a high correlation between ATR and Cobb angle, highlighting its usefulness in spinal screening.33–35 The results of this study indicated that exercise therapy effectively reduced ATR in patients, with a statistically significant difference (P < 0.05). This may be attributed to the three-dimensional correction approach adopted in the therapy, which involved expanding the chest through rotational breathing and rib cage translation, self-correcting the posture of the pelvis and scapular belt in various positions, enhancing trunk muscle strength and core stability, and correcting abnormal vertebral and rib rotation, thereby reducing ATR in patients with AIS. Bunnell initially suggested that professional consultation and treatment are necessary when ATR exceeded 5°, later raising this threshold to 7° to reduce the likelihood of false positives (12% false positives at 5° and 3% at 7°). However, a 2° change in ATR is considered significant for intra-observer measurements. In this meta-analysis, only one study reported an average ATR correction below 2°, further supporting the effectiveness of exercise therapy in reducing ATR. Additionally, Huanzhou et al. found that core stability training combined with Schroth exercises effectively corrected spinal curvature in patients with idiopathic scoliosis. This intervention reduced ATR and the prominence of the rib hump, thereby normalizing external appearance and significantly enhancing patients’ self-confidence and quality of life. 36
With advancements in modern medical technology, the latest guidelines for the Rehabilitation Diagnosis and Treatment of Adolescent Idiopathic Scoliosis prioritize the treatment goals for AIS as follows: (a) improving overall appearance; (b) enhancing quality of life; (c) preventing disability; (d) alleviating low back pain; (e) maintaining good mental health; (f) reducing the risk of deformity progression in adulthood; (g) improving respiratory function; and (h) decreasing the Cobb angle of scoliosis. 37 Deviating from the traditional focus on reducing Cobb angle, these guidelines emphasize the importance of improving overall appearance and quality of life in AIS treatment. The results of this study showed that participants in the exercise therapy group scored higher on the SRS-22 scale compared with those in the control group, with statistically significant differences in pain, functional activities, self-image, and satisfaction with treatment (P < 0.05), indicating a marked improvement in patients’ quality of life. This may be attributed to the effective improvement of scoliosis through exercise therapy, which adjusts the biomechanical balance of muscles; reduces pain; alleviates related clinical symptoms such as back pain, respiratory dysfunction, muscle contracture, and abnormal spinal deformities; and enhances functional activities. Adolescents are primarily concerned with their physical appearance, and exercise therapy helps improve deformities such as unequal shoulder height and rib humps, leading to increased satisfaction with appearance and improved self-image scores. However, no significant improvement was observed in mental health, with no statistically significant difference (P > 0.05). This may be because the patients were adolescents susceptible to external influences; their psychological pressure may have increased during the treatment process as they gradually learned about scoliosis through regular follow-ups, health education, and self-research. In summary, exercise therapy for AIS prioritizes improving patients’ overall quality of life and restoring social function. It enhances balance, improves functional outcomes, and limits scoliosis progression. This approach is easy to learn, cost-effective, and most importantly, noninvasive. It effectively increases treatment satisfaction and aligns with the contemporary concepts advocated by the International Society on Scoliosis Orthopaedic and Rehabilitation Treatment.
Currently, no consensus exists on the optimal duration of exercise therapy required to achieve satisfactory clinical outcomes. After excluding the study by Miao and Zhang, 16 in which treatment lasted only 3 months, a significant reduction in heterogeneity was observed for pain, functional activity, and mental health scores on the SRS-22 scale. This suggests that a brief treatment duration hinders the attainment of favorable clinical results. Some studies have reported that patients can achieve certain effects after only 2 weeks of exercise therapy under strict supervision of a physiotherapist.38–39 However, various studies with different levels of evidence-based support indicate that satisfactory outcomes from exercise therapy generally require a minimum duration of 6 months, with sessions lasting no less than 45 min per day.23–25 Most studies support the notion that a standardized treatment period of at least 6 months is necessary to achieve stable outcomes.40–44 A meta-analysis by Park et al., 43 which combined 15 studies and measured the pre-post effect size of Schroth exercises on idiopathic scoliosis, found that treatment duration was a crucial factor. According to Cohen’s guidelines, the method demonstrated a medium effect size (≥0.50) when applied for less than 6 months. They recommended continuing treatment for at least 6 months or longer, as it has been shown to produce a large effect size (≥0.80) on the Cobb angle. Another issue is determining when to terminate exercise therapy. Exercise therapy requires consistent adherence from patients and continuous adjustment of the treatment plan as therapy progresses, posing a challenge for both patients and their families. However, data on the appropriate timing for termination are lacking. Based on the natural history of AIS, exercise therapy should continue at least until there is no risk of scoliosis progression. 31
The limitations of this study were as follows: 1. The quality of some included studies was not high, and the implementation of allocation concealment and blinding methods was not clearly stated, reducing the reliability of the results. 2. The follow-up durations of the included studies were inconsistent, potentially introducing publication bias. 3. The included literature did not cover all types of exercise therapy, resulting in incompleteness. 4. Only published Chinese and English literature was included, potentially leading to publication and language biases.
In summary, exercise therapy effectively improved the Cobb angle, reduced ATR, and enhanced quality of life in patients with AIS compared with other conservative treatments. However, given the limitations in the number and quality of the included studies, these conclusions require further verification through additional high-quality research.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251389744 - Supplemental material for Efficacy of exercise therapy in adolescent idiopathic scoliosis: A meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605251389744 for Efficacy of exercise therapy in adolescent idiopathic scoliosis: A meta-analysis by Ziyao Ma, Song Wang and Shuai Zhang in Journal of International Medical Research
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
Ziyao Ma extracted data, reviewed all articles, and wrote the first draft. Shuai Zhang and Song Wang designed the study, reviewed the first draft, and provided valuable comments.
Availability of data and materials
The datasets generated and analyzed during the current study are available in the following repositories:
CNKI: https://www.cnki.net/ PubMed: https://pubmed.ncbi.nlm.nih.gov/ Web of Science: https://www.webofscience.com/wos/ Embase: https://www.embase.com/ Ovid: https://ovidsp.ovid.com/
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Not applicable.
Funding
This work was jointly funded by the Sichuan Natural Science Foundation (NO.2023NSFSC0333) and the Strategic Cooperation Project of Luzhou Municipal People’s Government - Southwest Medical University (NO.2024LZXNYDJ031).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.