
Abstract
Study Design
A retrospective study.
Objectives
To explore the relationship between K-line tilt and short-term surgical outcomes following laminoplasty in patients with multilevel degenerative cervical myelopathy (DCM), and to evaluate the potential of K-line tilt as a reliable preoperative predictor.
Methods
A retrospective analysis was performed for 125 consecutive patients who underwent laminoplasty for multilevel DCM. The radiographic parameters utilized in this study encompassed T1 slope (T1S), C2-C7 lordosis (CL), C2-C7 sagittal vertical axis (cSVA), T1 slope minus C2-C7 lordosis (T1S-CL), C2-C7 range of motion (ROM), and K-line tilt. The neurological recovery was evaluated using the Japanese Orthopaedic Association (JOA) score. Pearson correlation coefficients were calculated to assess the relationship between K-line tilt and other classical cervical parameters. Logistic regression analysis was employed to examine the association between K-line tilt and surgical outcomes.
Results
Of the 125 patients, 89 were men. The mean age of the patients was 61.74 ± 11.31 years. The results indicated a correlation between the K-line tilt and the cSVA (r = 0.628, P < 0.001), T1S (r = 0.259, P = 0.004), and T1S-CL (r = 0.307, P < 0.001). The K-line tilt showed an association with the failure of the JOA recovery rate (RR) to reach the minimal clinically important difference (MCID) and the occurrence of postoperative kyphotic deformity. We identified cutoff values for the K-line tilt which predict the failure of the JOA RR to reach the MCID and postoperative kyphotic deformity as 10.13° and 9.93°, respectively.
Conclusions
The K-line tilt is an independent preoperative risk factor associated with both the failure of the JOA RR to reach the MCID and the occurrence of postoperative kyphotic deformity in patients with multilevel DCM after laminoplasty.
Keywords
Introduction
Laminoplasty is commonly employed as a non-fusion procedure to alleviate multilevel spinal cord compression resulting from degenerative cervical myelopathy (DCM). 1 The primary objective of surgery is to relieve symptoms by posteriorly shifting the spinal cord, often referred to as the “bowstring effect”. 2 Therefore, having cervical lordosis before surgery and being able to maintain it after surgery are essential prerequisites for successful surgery. Regrettably, some patients with preoperative cervical lordosis may still experience kyphotic deformity after laminoplasty, potentially compromising the indirect decompression effect achieved through the posterior shift of the spinal cord.3,4 Therefore, identifying preoperative factors that can reliably predict cervical kyphotic deformity after laminoplasty holds significant clinical importance.
Previous studies have concluded that cervical sagittal imbalance is predictive of cervical kyphotic deformity and unsatisfactory neurologic recovery after laminoplasty.5,6 Patients with a higher T1S may necessitate increased cervical lordosis to retain a horizontal gaze. The posterior muscle-ligament complex plays a crucial role in maintaining cervical lordosis, but laminoplasty inevitably disrupts this complex. Consequently, such patients are at higher risk of developing cervical kyphosis post-laminoplasty.7,8 Additionally, patients with larger cSVA, larger T1S-CL, and smaller CL are also susceptible to postoperative kyphosis.9-11 These changes can lead to poor improvement in postoperative JOA scores.
In addition to the classical cervical sagittal parameters, Kim et al. introduced a new radiographic index, K-line tilt, to assess cervical sagittal alignment. 12 They defined the K-line tilt as the angle between the K-line and a line perpendicular to the horizon, and their findings demonstrated a positive correlation between K-line tilt and the classic cervical parameters. In terms of the relationship between K-line tilt and surgical outcomes after laminoplasty, Sakai et al. reported that patients with K-line tilt greater than 20° are more prone to developing kyphotic deformity. 13 Furthermore, Rao et al. also demonstrated that patients with higher preoperative K-line tilt experienced more significant kyphosis changes after laminoplasty. 9
The participants in the aforementioned studies were primarily ossification of the posterior longitudinal ligament (OPLL) patients. As a more comprehensive term, degenerative cervical myelopathy (DCM) encompasses both cervical spondylotic myelopathy (CSM) and OPLL, thus better capturing the degenerative nature of the condition. 14 However, to our knowledge, there are currently no reports examining the feasibility and clinical utility of K-line tilt in predicting surgical outcomes after laminoplasty in patients with multilevel DCM. Therefore, in this study, we aim to explore the association between K-line tilt and short-term surgical outcomes in multilevel DCM patients undergoing laminoplasty.
Materials and methods
Ethics Statements
This study was approved by our institutional review board (number: GDREC201793H). Written informed consent was obtained from all patients before collecting their clinical and radiological information.
Study Design and Population
The study utilized a retrospective data collection approach involving patients who underwent laminoplasty for multilevel DCM at our institution from June 2020 to February 2023. All patients were diagnosed following a comprehensive medical history interview, physical examination, and imaging. Exclusion criteria comprised: (1) patients with a history of other neurological diseases that may impact their neurological function, such as stroke, Parkinson’s disease, or poliomyelitis; (2) previous cervical surgery; (3) obvious cervical kyphosis; (4) incomplete follow-up data; and (5) unclear imaging. All patients were followed for more than 1 year. Preoperative and postoperative imaging data, in conjunction with clinical outcome measures including the Japanese Orthopaedic Association (JOA) score and numeric rating scale (NRS) for neck pain, were gathered. Comorbidities were quantified using the Charlson Comorbidity Index (CCI) score, which was derived from data extracted from each patient’s medical records.
Operative Procedure
All surgeries were performed by a senior surgeon following the laminoplasty procedure outlined in previous studies. 15 The patients were positioned in a prone neutral stance, and the laminae were exposed by dissecting the bilateral paracervical muscles through a posterior midline incision. A high-speed air-burr drill was used to create grooves at the junction of the lamina and facet joints, with 1 lamina’s ventral cortex being cut, while the ventral cortex of the other lamina was grooved to serve as a hinge. The cut lamina of the opposite side was then elevated and secured in the expanded position using titanium miniplates and screws. The laminoplasty procedure involved only plating, and no bone grafts or fusion materials were placed on the hinge or the open side.
Radiological Measurements
Preoperative plain radiographs and MRI of the cervical spine were performed in all patients. The cervical parameters measured on the standing lateral radiograph included K-line tilt, cSVA, T1S, CL, T1S-CL, and C2-C7 range of motion (ROM). These measurements were obtained using Surgimap software (New York, NY, USA). The K-line tilt was defined as an angle between the K-line (a line connecting the midpoints of the spinal canal at C2 and C7) and a line vertical to the horizon (Figure 1A).
12
The cSVA is the distance between the perpendicular line of the center of the C2 vertebral body and the posterior upper-end point of the C7 vertebral body (Figure 1B). The T1S is the angle between the upper plate of the T1 vertebral body and the horizontal line (Figure 1C). CL is the angle between the lower-end plate of the C2 and C7 vertebral bodies (Figure 1D). ROM was calculated as the difference between the CL in maximal flexion and CL in maximal extension (Figure 1E,F).
8
The kyphotic deformity was defined as a CL of less than 0° postoperatively.13,16 The patients were then categorized into subgroups of kyphosis and lordosis based on the postoperative CL. T2-weighted magnetic resonance images were evaluated to determine the presence of high signal intensity within the spinal cord. K-line tilt (A), cSVA (B), T1S (C), and CL (D) were measured in the neutral position. Flex CL (E) and Ext CL (F) were measured with the patient in maximal flexion and extension, respectively. cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; CL, C2-C7 cervical lordosis; Ext CL, CL in extension; Flex CL, CL in flexion.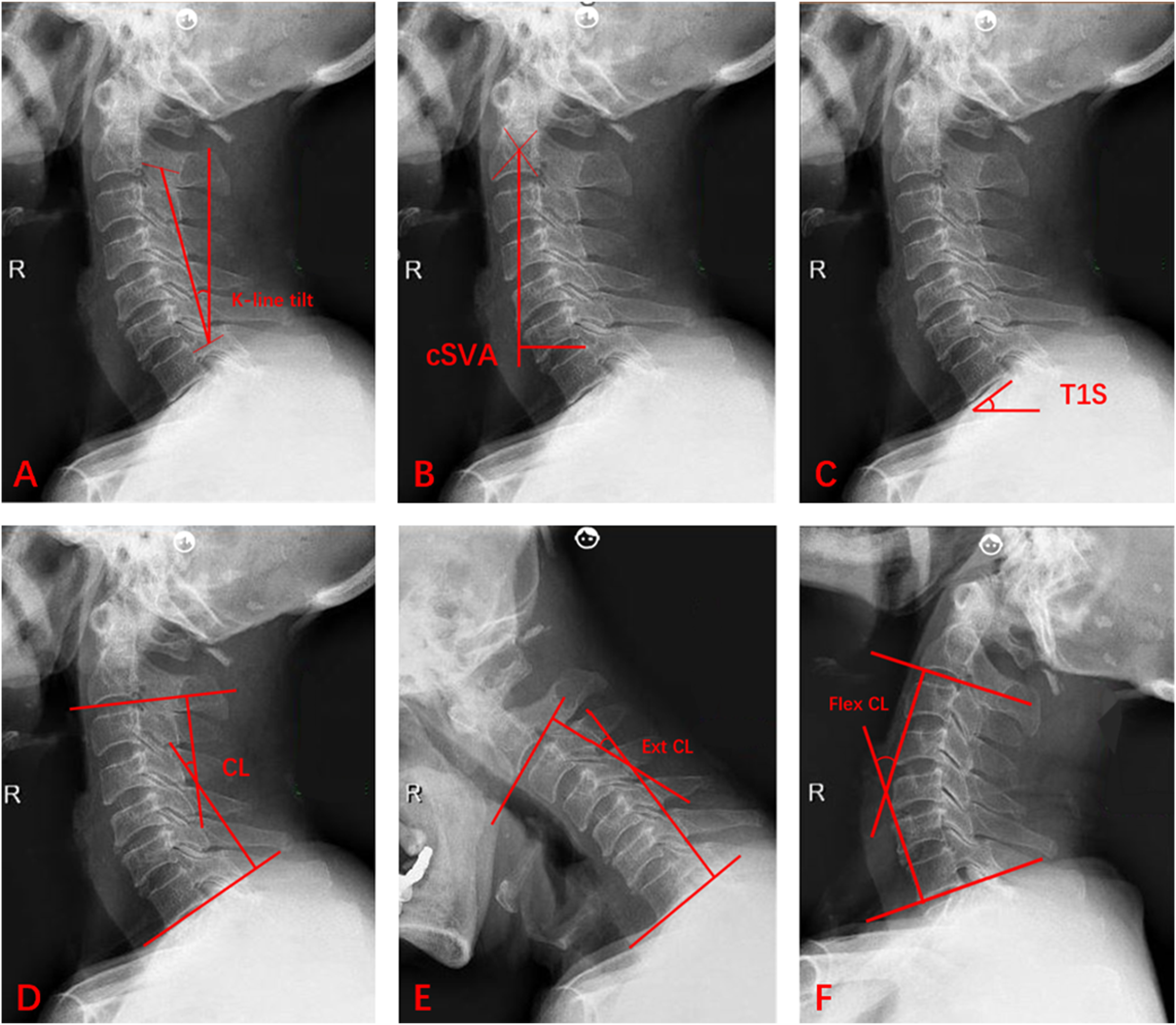
Clinical Measurements
At the last follow-up, observe the presence of cervical kyphotic deformity in the patients based on the standing lateral radiograph, and document the surgical segments. The clinical outcomes before and after laminoplasty were evaluated using the JOA score and the NRS for neck pain. The JOA recovery rate (RR) was calculated using the Hirabayashi method as follows: RR = [postoperative JOA score – preoperative JOA score]/[17 – preoperative JOA score]×100%. 17 The minimal clinically important difference (MCID) is defined as the smallest change that can be recognized as “clinically meaningful” by a patient to evaluate the success of interventions. Based on a previous study, the minimum clinically important recovery rate was found to be 52.8%. 18 In this study, 52.8% was used as a reference criterion to assess whether the changes to the JOA scores were significant enough to produce measurement clinical differences. The patients were divided into 2 groups: those who achieved MCID in the JOA recovery rate (JOA RR ≥ MCID) and those who did not achieve MCID in the JOA recovery rate (JOA RR < MCID).
Statistical Analysis
Numerical variables were presented as mean ± standard deviation (SD) or median (interquartile range, IQR), and the differences were assessed using the Student’s t-test or Mann-Whitney U test. Categorical variables were displayed as frequencies and percentages, and the differences were compared using Pearson’s chi-squared test or Fisher’s exact test. Pearson correlation coefficient was employed for correlation analyses. Multivariate logistic regression analysis with a stepwise procedure was conducted to identify potential independent preoperative risk factors associated with cervical kyphotic deformity and the failure of the JOA recovery rate (RR) to reach the MCID. Preoperative factors with a P-value less than 0.05 in univariate analysis were included in the multivariate analysis. The area under the receiver operating characteristic curve (AUC) was calculated to measure the predictive value. All statistical analyses were performed using SPSS statistical software, version 26 (IBM Corp, Armonk, NY, USA). Statistical significance was set at a P-value less than 0.05.
Results
Demographic Data
Baseline Demographic and Clinical Features of Patients.
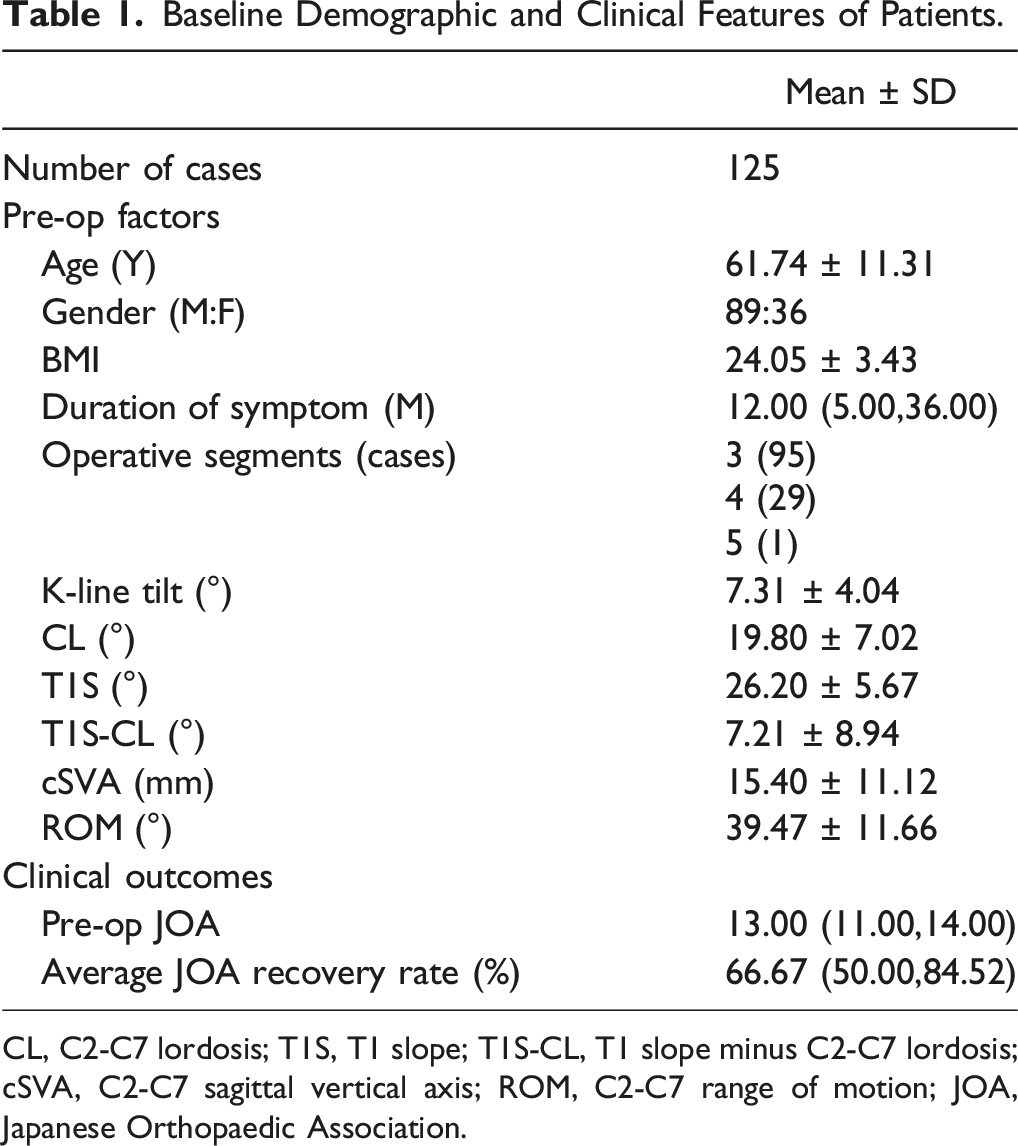
CL, C2-C7 lordosis; T1S, T1 slope; T1S-CL, T1 slope minus C2-C7 lordosis; cSVA, C2-C7 sagittal vertical axis; ROM, C2-C7 range of motion; JOA, Japanese Orthopaedic Association.
Correlation Between K-Line Tilt and Other Radiographic Parameters
The Pearson Correlation Coefficients and P Values Between Radiographic Parameters.
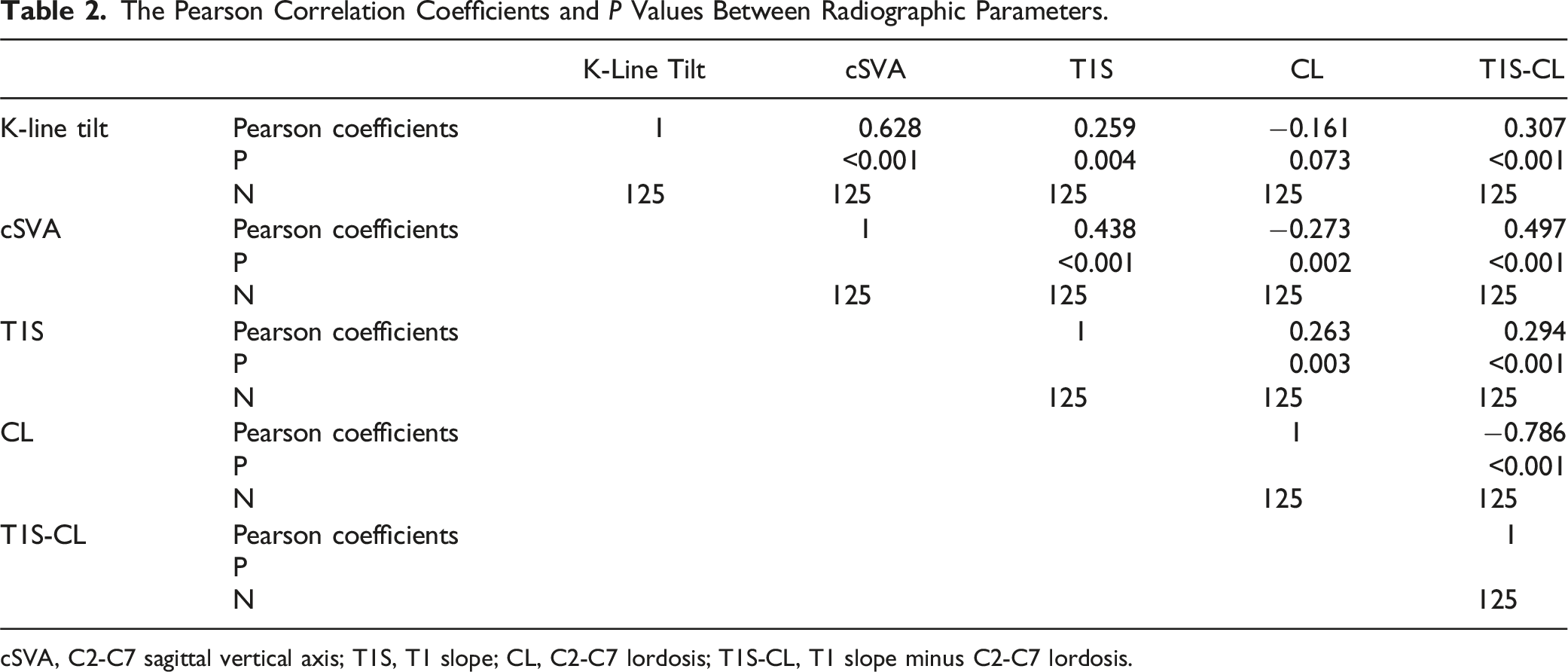
cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; CL, C2-C7 lordosis; T1S-CL, T1 slope minus C2-C7 lordosis.
Change in Radiological and Clinical Measurements
A postoperative kyphotic deformity (CL <0°) was observed in 12 patients (9.6%), and 37 patients (29.6%) did not reach the minimal clinically important difference (MCID) in their JOA recovery rate. The degree of C2-C7 lordosis significantly decreased from 19.80 ± 7.02° to 12.41 ± 10.50° at the final follow-up (P < 0.001). All clinical measurements showed improvement. JOA scores increased from 13.00 (11.00,14.00) to 16.00 (15.00,16.00), while NRS scores decreased from 2.00 (0.00,4.00) to 0.00 (0.00,1.00) (all results with P < 0.001). The average JOA RR was 66.67% (50.00, 84.52).
Comparison Between the Kyphosis and Lordosis Groups
Preoperative Factors and Clinical Outcomes in the Kyphosis and the Lordosis Groups.
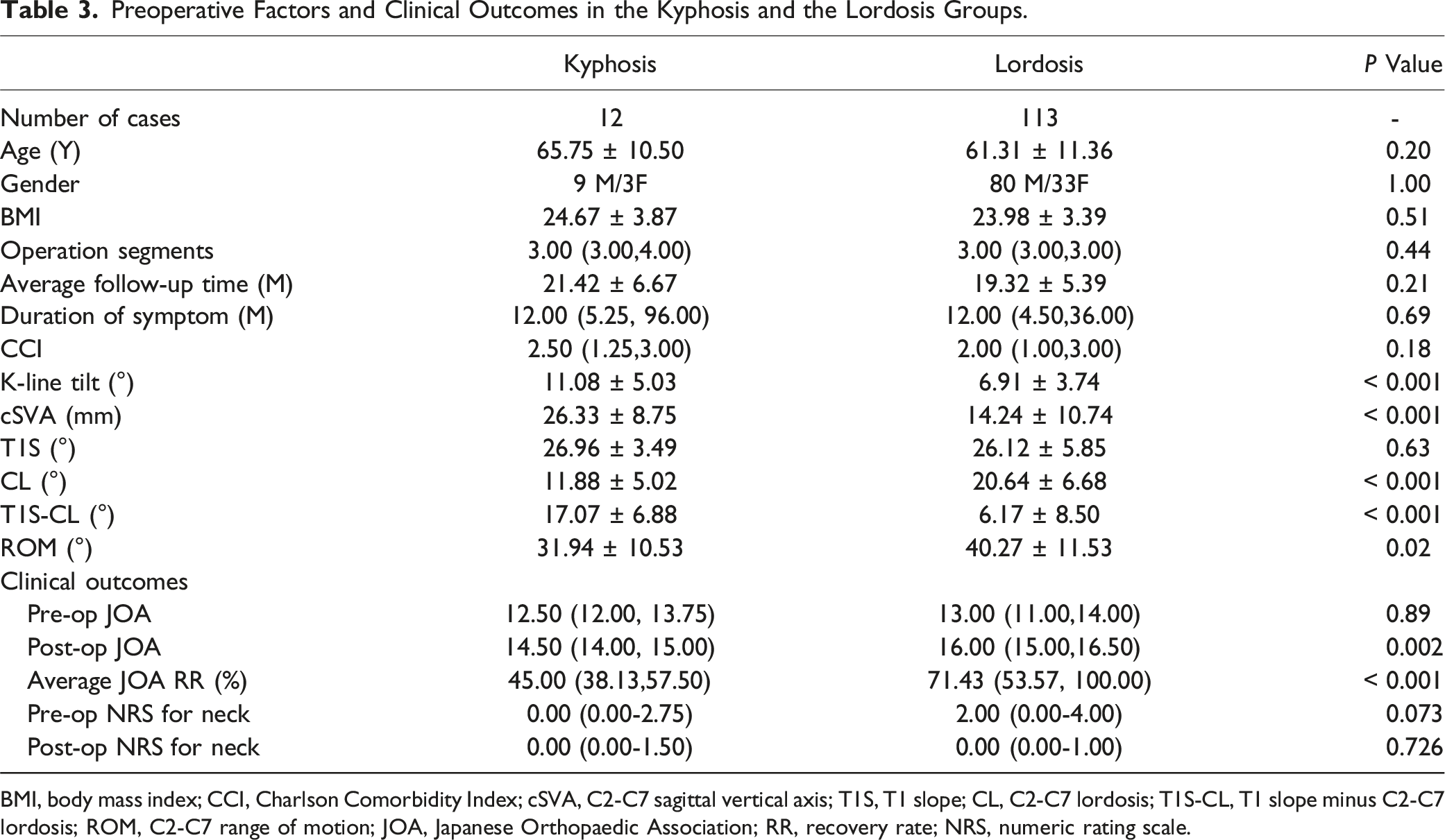
BMI, body mass index; CCI, Charlson Comorbidity Index; cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; CL, C2-C7 lordosis; T1S-CL, T1 slope minus C2-C7 lordosis; ROM, C2-C7 range of motion; JOA, Japanese Orthopaedic Association; RR, recovery rate; NRS, numeric rating scale.
Preoperative Risk Factors of Postoperative Kyphotic Deformity
Logistic Regression Analysis Results for Preoperative Risk Factors Associated With Postoperative Kyphotic Deformity (Forward, LR, a = 0.05).
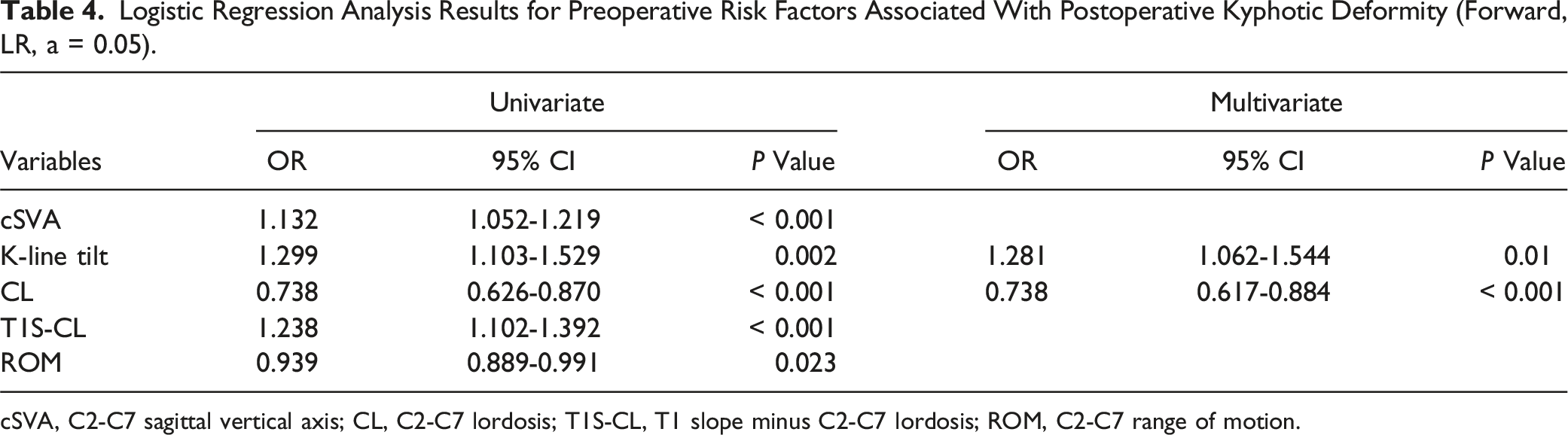
cSVA, C2-C7 sagittal vertical axis; CL, C2-C7 lordosis; T1S-CL, T1 slope minus C2-C7 lordosis; ROM, C2-C7 range of motion.
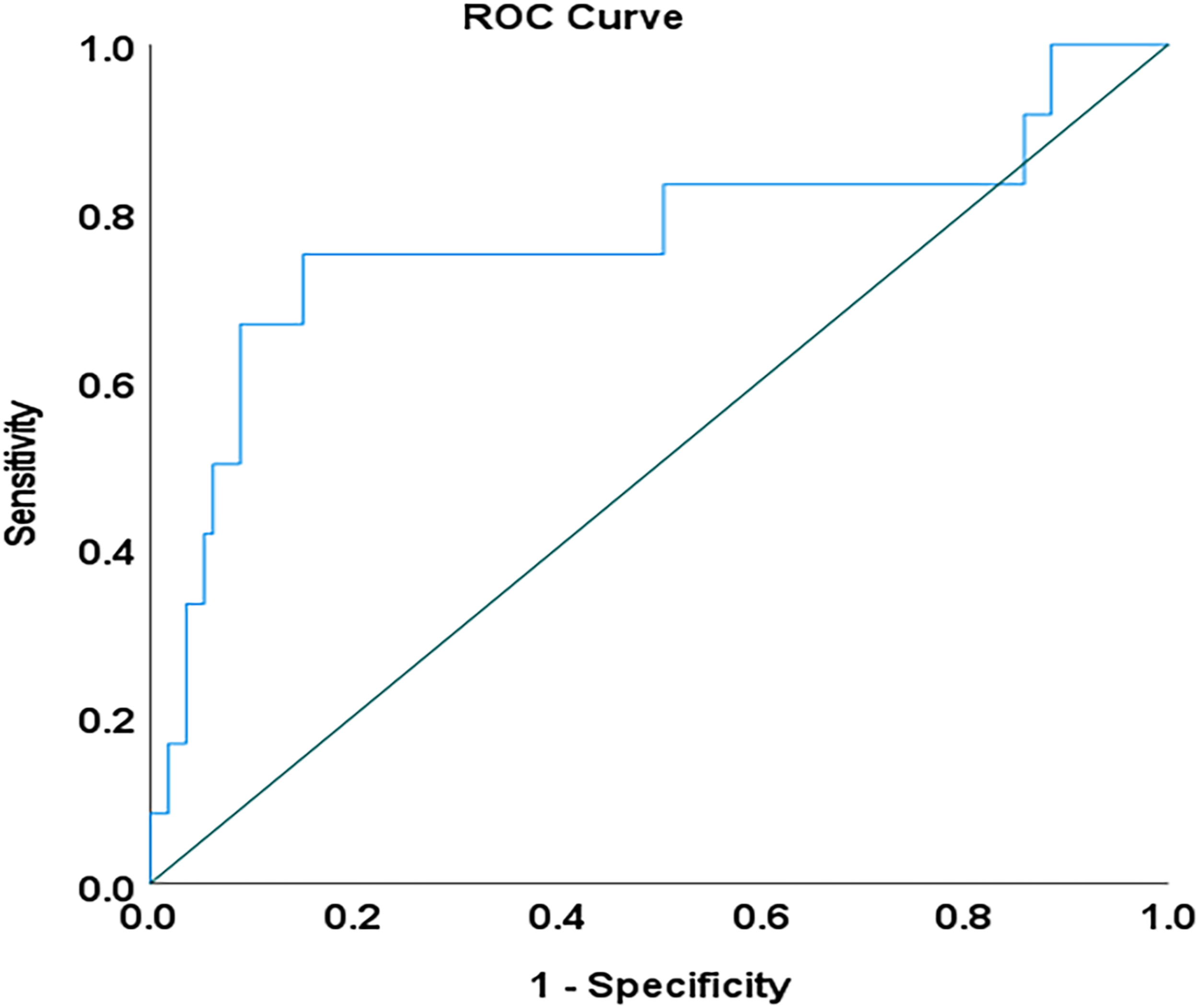
ROC curve analysis to predict postoperative kyphotic deformity. The cutoff value for K-line tilt was 10.13° (area under the curve = 0.768, P = 0.002), with a sensitivity of 75.0% and a specificity of 85.0%. ROC, receiver operating characteristic.
Comparison by JOA Recovery Rate
Comparison of Preoperative Factors and Clinical Outcomes Between Two Groups.
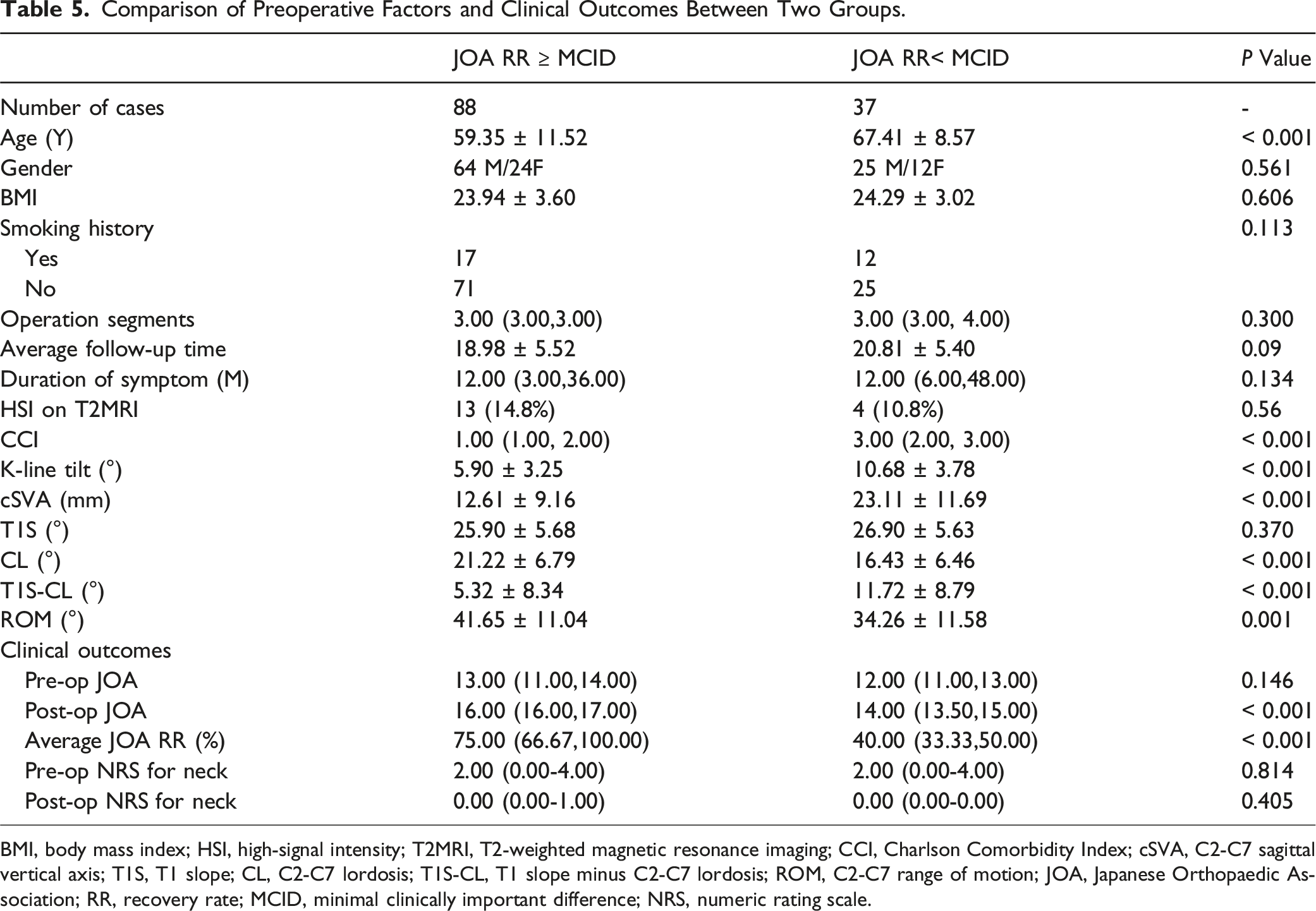
BMI, body mass index; HSI, high-signal intensity; T2MRI, T2-weighted magnetic resonance imaging; CCI, Charlson Comorbidity Index; cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; CL, C2-C7 lordosis; T1S-CL, T1 slope minus C2-C7 lordosis; ROM, C2-C7 range of motion; JOA, Japanese Orthopaedic Association; RR, recovery rate; MCID, minimal clinically important difference; NRS, numeric rating scale.
Preoperative Risk Factors of JOA RR Not Achieving the MCID
Logistic Regression Analysis Results for Preoperative Risk Factors Associated With JOA RR Not Achieving the MCID (Forward, LR, a = 0.05).
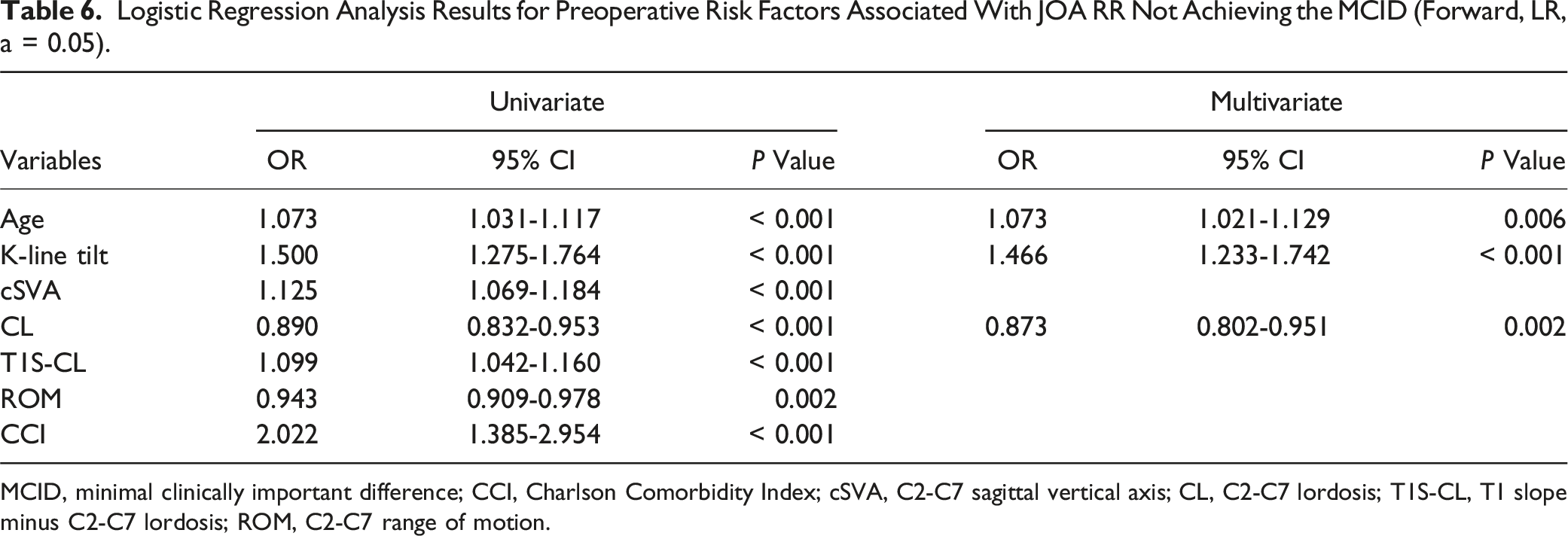
MCID, minimal clinically important difference; CCI, Charlson Comorbidity Index; cSVA, C2-C7 sagittal vertical axis; CL, C2-C7 lordosis; T1S-CL, T1 slope minus C2-C7 lordosis; ROM, C2-C7 range of motion.
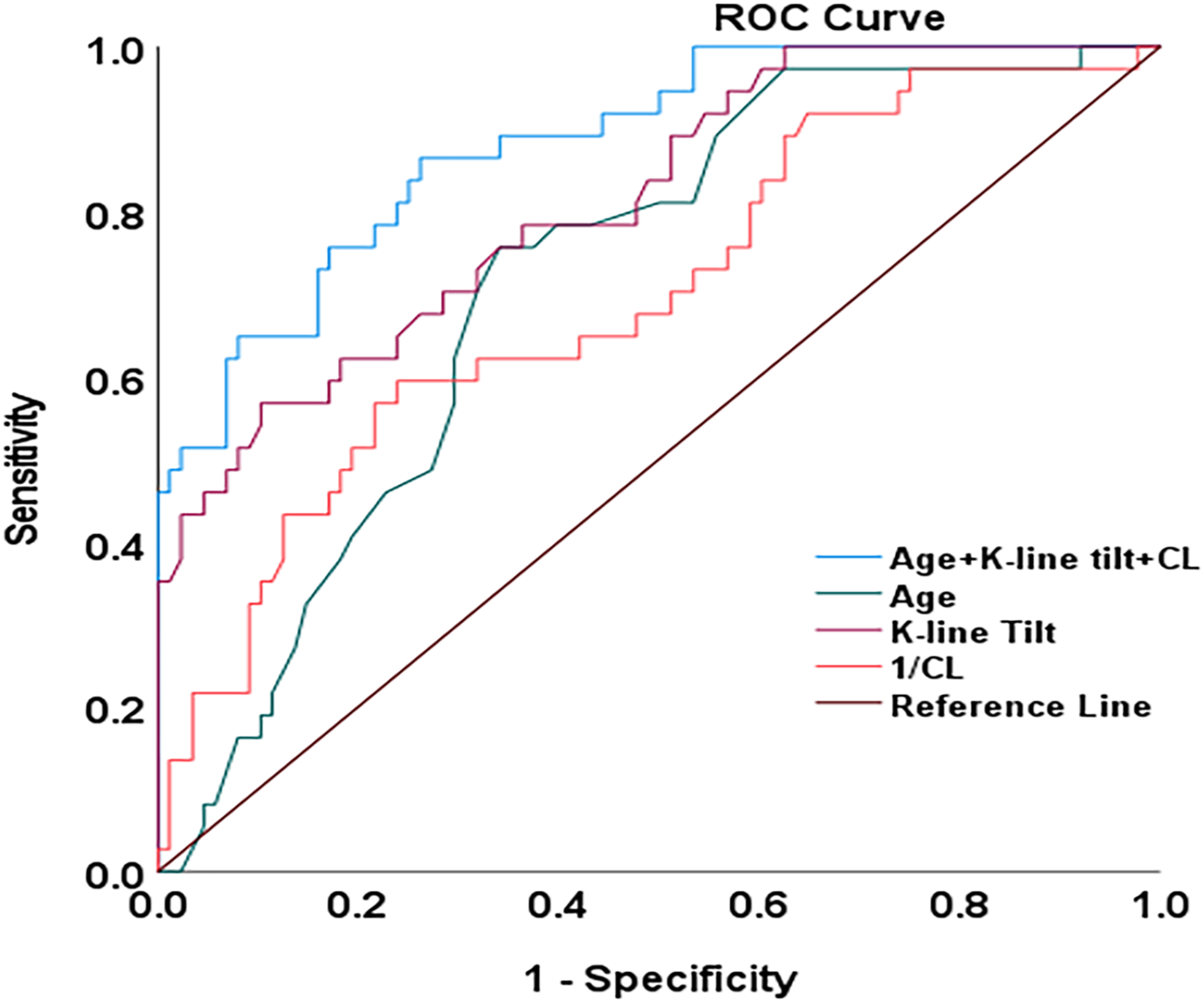
ROC curve analysis to predict JOA RR < 52.8%. The cutoff value for K-line tilt was 9.93° (area under the curve = 0.813, P < 0.001), with a sensitivity of 56.8% and a specificity of 89.8%. The combined use of multiple preoperative indicators, including age, K-line tilt, and CL, demonstrated greater accuracy in predicting the likelihood of JOA RR<52.8%, compared to using the K-line tilt alone (AUC: 0.882 vs 0.813). ROC, receiver operating characteristic; JOA, Japanese Orthopaedic Association; RR, recovery rate; CL, C2-C7 lordosis.
Discussion
Subsequent to the introduction of K-line tilt, numerous studies have reported its association with the development of kyphotic deformity following laminoplasty in patients with ossification of the posterior longitudinal ligament (OPLL). However, the correlation between preoperative K-line tilt and short-term surgical outcomes after laminoplasty in patients with multilevel degenerative cervical myelopathy (DCM) remains to be fully elucidated. The present study has shown that K-line tilt can be used as a valuable radiographic parameter to evaluate cervical sagittal alignment. Importantly, it has been established that K-line tilt is a significant preoperative risk factor for predicting the inability of the JOA RR to achieve the minimal clinically important difference (MCID) and postoperative kyphotic deformity.
Laminoplasty is the primary method employed to achieve indirect decompression through the posterior shift of the spinal cord in patients with multilevel degenerative cervical myelopathy (DCM). Prior investigations have confirmed the safety and efficacy of laminoplasty for multilevel DCM in both short-term and long-term observations. 3 To achieve adequate indirect decompression by moving the spinal cord away from problematic anterior pathologies, it is crucial to possess cervical lordosis before surgery and maintain it after surgery. Despite this, observations have revealed instances where patients with adequate preoperative cervical lordosis developed kyphotic deformity after laminoplasty. The occurrence of postoperative kyphotic deformity can impede backward drifting of the spinal cord, resulting in the loss of the desired indirect decompression effect. Therefore, it is imperative to ascertain the risk factors associated with kyphotic deformity and to take preventative measures to mitigate its occurrence following laminoplasty.
A variety of preoperative factors may be linked to kyphotic deformity after laminoplasty in patients with DCM who do not have preoperative cervical kyphosis. These factors encompass cervical foraminal stenosis, ROM, cervical posterior muscle status, disc degeneration, thoracolumbar sagittal balance, and preoperative cervical sagittal alignment.16,19-21 Of these, preoperative cervical sagittal alignment stands out as a significant concern. According to Kim et al, patients with higher T1S preoperatively are at risk for postoperative kyphosis. 22 Furthermore, other studies have also suggested an association between preoperative T1S and the development of postoperative kyphosis.8,11 These studies have also indicated that cSVA, CL, and T1S-CL may also be linked to post-laminoplasty kyphosis.
The above research findings indicate a relationship between post-laminoplasty kyphosis and preoperative cervical sagittal parameters. In addition to the aforementioned classic cervical parameters, the utility of K-line tilt as a parameter, similar to cSVA and T1S-CL, in assessing cervical sagittal alignment has been confirmed. 12 Our study also validated a positive correlation between K-line tilt and classical cervical parameters such as cSVA, T1S, and T1S-CL. Regarding the clinical significance of the K-line tilt, Sakai et al. showed that a large K-line tilt (>20°) is a risk factor for cervical kyphotic deformity after laminoplasty in patients with OPLL. 13 In addition, Rao et al. also discovered that patients with a greater preoperative K-line tilt were at higher risk of developing cervical kyphotic deformity following laminoplasty. 9 Consistent with these findings, our study results also indicate that K-line tilt is an independent preoperative risk factor for developing postoperative kyphotic deformity, with a greater K-line tilt associated with a higher likelihood of postoperative kyphotic deformity.
We further investigated the association between preoperative factors and neurological function recovery. Based on the univariate analysis, we observed that patients who did not reach the minimally clinically important difference (MCID) in JOA RR tended to have higher age, larger K-line tilt, larger cSVA, larger T1S-CL, smaller CL, smaller ROM, and more severe comorbidities. These findings are consistent with the results of comparable studies.23-26 To explore the independent preoperative risk factors associated with failing to reach the minimally clinically important difference (MCID) in JOA RR, we conducted a multivariate logistic regression analysis with a stepwise procedure. The analysis revealed that K-line tilt was a significant factor (OR, 1.466; 95% CI, 1.233 - 1.742; P < 0.001). This study established a cutoff value of 9.93° for the K-line tilt. It indicates that when the K-line tilt is ≥9.93°, there is an increased likelihood that the JOA RR will not achieve the MCID.
We hypothesize a potential mechanism that may elucidate why a large K-line tilt increases the risk of JOA RR not reaching the MCID and postoperative kyphotic deformity. Our study revealed a positive correlation between K-line tilt and preoperative cSVA and T1S, indicating that a larger K-line tilt corresponds to larger T1S and cSVA. Patients with a larger preoperative T1S may necessitate a greater cervical lordosis to maintain a horizontal gaze, which entails the action of the posterior muscle ligament complex. Similarly, a larger cSVA results in the increased forward tilt of the cervical spine, demanding greater tension from the posterior muscle-ligament complex. However, laminoplasty inevitably damages the posterior muscule-ligament complex. Consequently, patients with a large K-line tilt are predisposed to postoperative loss of cervical lordosis. Our results showed that the C2-C7 lordosis (CL) was smaller in the group with a K-line tilt of ≥9.93° compared to the group with a K-line tilt of <9.93° at the final follow-up (6.82° ± 10.13° vs 14.18° ± 10.02°; P < 0.001). The group with a K-line tilt of ≥9.93° also exhibited a significantly greater postoperative CL change (9.69° ± 7.27° vs 6.66° ± 6.27°; P = 0.028) compared to the group with a K-line tilt of <9.93°. As a result, the efficacy of indirect decompression through the posterior shift of the spinal cord will be negatively affected, ultimately hindering the postoperative recovery of neurological function. Additionally, age and CL were also identified as independent preoperative risk factors associated with failure to achieve the MCID in the JOA recovery rate. The identified cut-off value for the age, indicating the failure to achieve the MCID in JOA RR, was 63.5 years. The analysis revealed that compared to patients with age <63.5, patients with age ≥63.5 often had more severe comorbidities (Z = −9.107, P < 0.001). This discovery implies that the impaired neurological function recovery following laminoplasty is likely linked to the presence of more severe comorbidities in elderly patients. Therefore, we conducted a ROC curve analysis using a combination of 3 indicators (age, CL, and K-line tilt). The analysis results demonstrated that the combined use of these indicators was more accurate in predicting the JOA RR not achieving the MCID compared to using a single indicator, the K-line tilt (AUC: 0.882 vs 0.813, Figure 3). Therefore, we recommend that clinicians should holistically consider the impact of preoperative indicators on postoperative neurological recovery to improve prediction accuracy.
Our study is subject to several limitations. Firstly, this was a single-center retrospective study and some unintended biases could exist. Secondly, the sample size in our study was relatively small; however, it still exceeds the sample size of several previous similar studies. Thirdly, the follow-up duration of our study was relatively shorter compared to earlier similar studies. This limited follow-up duration may impact the ability to fully assess the long-term effects and outcomes. Hence, it is imperative to conduct a multicenter prospective study with larger sample sizes and longer follow-up durations to validate and strengthen the reliability of our findings.
Conclusion
In patients with multilevel degenerative cervical myelopathy (DCM) undergoing laminoplasty, a higher preoperative K-line tilt may correlate with inferior neurological recovery and postoperative kyphotic deformity. Our findings indicate that a preoperative K-line tilt of ≥9.93° signifies a likelihood of suboptimal neurological recovery, whereas a preoperative K-line tilt of ≥10.13° indicates a likelihood of postoperative kyphotic deformity.
Footnotes
Acknowledgments
We thank Ke’er Wang for contributing to the data collection.
Author contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Qifei Duan, Jianxiong Zhuang, and Shuaihao Huang. The first draft of the manuscript was written by Qifei Duan and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Guangdong Province (2022A1515012557).
Ethical Review Committee Statement
The Research Ethics Committee of the institute approved this investigation [No.GDREC2017293H] and all investigations were conducted in conformity with ethical principles of research.
Data Availability Statement
The datasets utilized and/or analyzed during the current study are available from the corresponding author upon reasonable request.