
Abstract
Objective
To compare the safety and efficacy of low-power (LP) and high-power (HP) holmium laser enucleation of the prostate (HoLEP) in patients with symptomatic small-volume benign prostatic hyperplasia (BPH).
Methods
In this prospective, multicenter, single-blind, randomized controlled trial, men with symptomatic BPH (prostate volume <40 mL, peak urinary flow rate [Qmax] <10 mL/s, International Prostate Symptom Score [IPSS] ≥18) underwent either LP (24 W) or HP HoLEP (80 W). The primary outcome was IPSS at 6 months postoperatively. Secondary outcomes included the surgical duration, total laser energy, enucleated prostate weight, patient-reported outcomes, and Clavien–Dindo classification of complications at 1, 3, and 6 months after surgery.
Results
Eighty-one participants completed the study. LP HoLEP used significantly less energy (22.4 ± 10.4 kJ vs. 58.6 ± 17.8 kJ). Postoperative pain was lower in the LP group at 24 and 48 hours. Both groups displayed significant improvements in outcomes versus baseline including IPSS and Qmax. The incidence of intraoperative complications was similar, though minor capsular perforation occurred exclusively in the HP group (9.8%).
Conclusion
LP HoLEP produced comparable clinical outcomes as HP HoLEP for small-volume BPH while using less energy, supporting its use for smaller glands.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a prevalent condition in aging men that can lead to significant lower urinary tract symptoms and a diminished quality of life. 1 Although traditionally associated with larger prostate volumes, even small-volume BPH can cause substantial morbidity. 2 Surgical intervention for BPH is typically reserved for patients who do not respond adequately to medical therapy, experience severe symptoms, or develop complications such as acute urinary retention, recurrent urinary tract infections, bladder stones, or renal impairment.3,4 For these patients, holmium laser enucleation of the prostate (HoLEP) has emerged as a versatile and effective treatment option achieving efficacy across a range of prostate sizes.5–7
Historically, high-power (HP) settings have been employed during HoLEP to achieve efficient enucleation. However, recent clinical studies have investigated the potential benefits of low-power (LP) HoLEP, which might reduce perioperative morbidity while maintaining efficacy. 8 This approach is of particular interest for patients with medium-volume prostates, as emerging data suggest that it could offer an optimal balance of safety and effectiveness.9,10 However, clinical research specifically targeting small-volume BPH remains limited. Our study aimed to fill this gap by focusing on patients with small-volume BPH, specifically evaluating whether low-power HoLEP represents a safe and effective alternative to the conventional higher-power settings.
Materials and methods
Study design
This prospective, multicenter, single-blind, randomized controlled trial investigated the safety and efficacy of LP and HP HoLEP for symptomatic small-volume BPH in patients treated between January 2021 and June 2023 at Jintan Affiliated Hospital of Jiangsu University and Zhangjiagang Hospital Affiliated to Soochow University. The study followed the guidelines of the Declaration of Helsinki (revised in 2013), and the protocol was approved by the Ethics Committee of Jintan Affiliated Hospital of Jiangsu University (Ethics number: 2020004, 2020.10.15). Informed consent was obtained from each participant before enrollment. In error, we did not prospectively register this trial, but we have now registered it retrospectively at the Research Registry (https://www.researchregistry.com/, registration number 10779).
Participants
Men with symptomatic BPH requiring surgery were included. The eligibility criteria encompassed prostate volume <40 mL, peak urinary flow rate (Qmax) <10 mL/s, International Prostate Symptom Score (IPSS) ≥18, and recurrent non-responsive urinary retention. The exclusion criteria comprised prostate cancer, bladder stones, urethral stricture, and detrusor underactivity confirmed by urodynamics.
Preoperative evaluation
A thorough preoperative assessment was performed, including detailed medical and surgical history, uroflowmetry (Qmax), post-void residual urine (PVR) measurement, IPSS and Overactive Bladder Symptom Score (OABSS) questionnaires, routine laboratory tests, serum prostate-specific antigen (PSA) analysis, and transrectal ultrasound for prostate volume quantification. When indicated, prostate biopsies and urodynamic testing were conducted.
Randomization and surgical technique
The reporting of this study conforms to the CONSORT statements. 11 Eligible participants were randomized 1:1 to the LP or HP HoLEP group using computer-generated allocation. Two experienced surgeons performed all procedures under general anesthesia using the “biplanar technique” as described by Wang et al. 12 A Ho laser generator (Versapulse PowerSuite; Lumenis Ltd., Yokneam, Israel) with a 550-µm end-firing fiber (SlimLine 550; Lumenis Ltd.) was employed. The power settings were 80 W (2.0 J, 40 Hz) for HP and 24 W (1.2 J, 20 Hz) for LP. All procedures used a 26-F resectoscope with continuous irrigation (Karl Storz, Tuttlingen, Germany) and HAWK morcellator (HAWK Inc., Hangzhou, China). Following morcellation, a 20-F three-way urethral catheter was placed for continuous irrigation with saline solution.
Outcome measures
The primary endpoints were perioperative data, IPSS, and Qmax at 1, 3, and 6 months postoperatively. The secondary endpoints included patient-reported outcomes (OABSS, PVR) and the Clavien–Dindo classification of complications at 1, 3, and 6 months post-surgery.
Statistical analysis
A sample size calculation was performed to ensure sufficient statistical power to detect a clinically meaningful difference in the primary outcome, namely the IPSS at 6 months postoperatively, between the LP and HP groups. Based on previous studies, a minimum difference of 3 ± 4 points in IPSS between the groups was considered clinically significant. 13 To achieve 80% power at a significance level of 0.05, a minimum of 36 patients per group was required. Considering a potential dropout rate of 15%, the target enrollment size was 87 patients.
Baseline data were analyzed descriptively. Continuous variables were compared using Student's t-test, whereas categorical variables were analyzed using the chi-square test. P < 0.05 was considered statistically significant. Data analysis was performed using IBM SPSS Statistics for Windows, Version 27 (IBM Corp., Armonk, NY, USA).
Results
Eighty-seven patients were initially enrolled in this randomized controlled trial. However, six patients withdrew during follow-up, and the remaining 81 participants were randomized into the LP (n = 40) and HP groups (n = 41, as indicated by the CONSORT diagram in Figure 1.

The CONSORT diagram. Group HP, high-power group; Group LP, low-power group; HoLEP, holmium laser enucleation of the prostate.
Baseline characteristics
As detailed in Table 1, no significant differences in age, prostate volume, disease duration, or PSA levels were observed between the groups (P > 0.05).
Characteristics of the participants at baseline.

The results are presented as the mean ± SD.
HP, high-power group; LP: low-power group; PSA, prostate-specific antigen.
Primary outcomes
Perioperative and postoperative parameters are detailed in Table 2. The total operative time was similar between the HP (32.3 ± 5.2 minute) and LP groups (33.2 ± 5.0 min; P = 0.416). There were no significant differences between the groups regarding the hemostasis time, morcellation time, or extracted tissue volume. However, the total energy delivered was significantly lower in the LP group (22.4 ± 10.4 kJ) than in the HP group (58.6 ± 17.8 kJ; P < 0.001). Intraoperative complications, such as anatomical plane loss (HP, 16.4%; LP, 7.5%; P = 0.159), minor capsular perforation (HP, 5.5%; LP, 1.9%; P = 0.326), and bladder neck injury (HP, 3.6%; LP, 1.9%; P = 0.580), occurred at similar rates in both groups. Postoperative outcomes, including the decrease in hemoglobin levels, irrigation time, catheterization time, and hospital stay, did not differ between the groups (all P < 0.1). However, the LP group reported lower visual analogue scale (VAS) scores for pain at 24 (P = 0.002) and 48 hours after surgery (P = 0.001).
Intra- and postoperative outcomes.
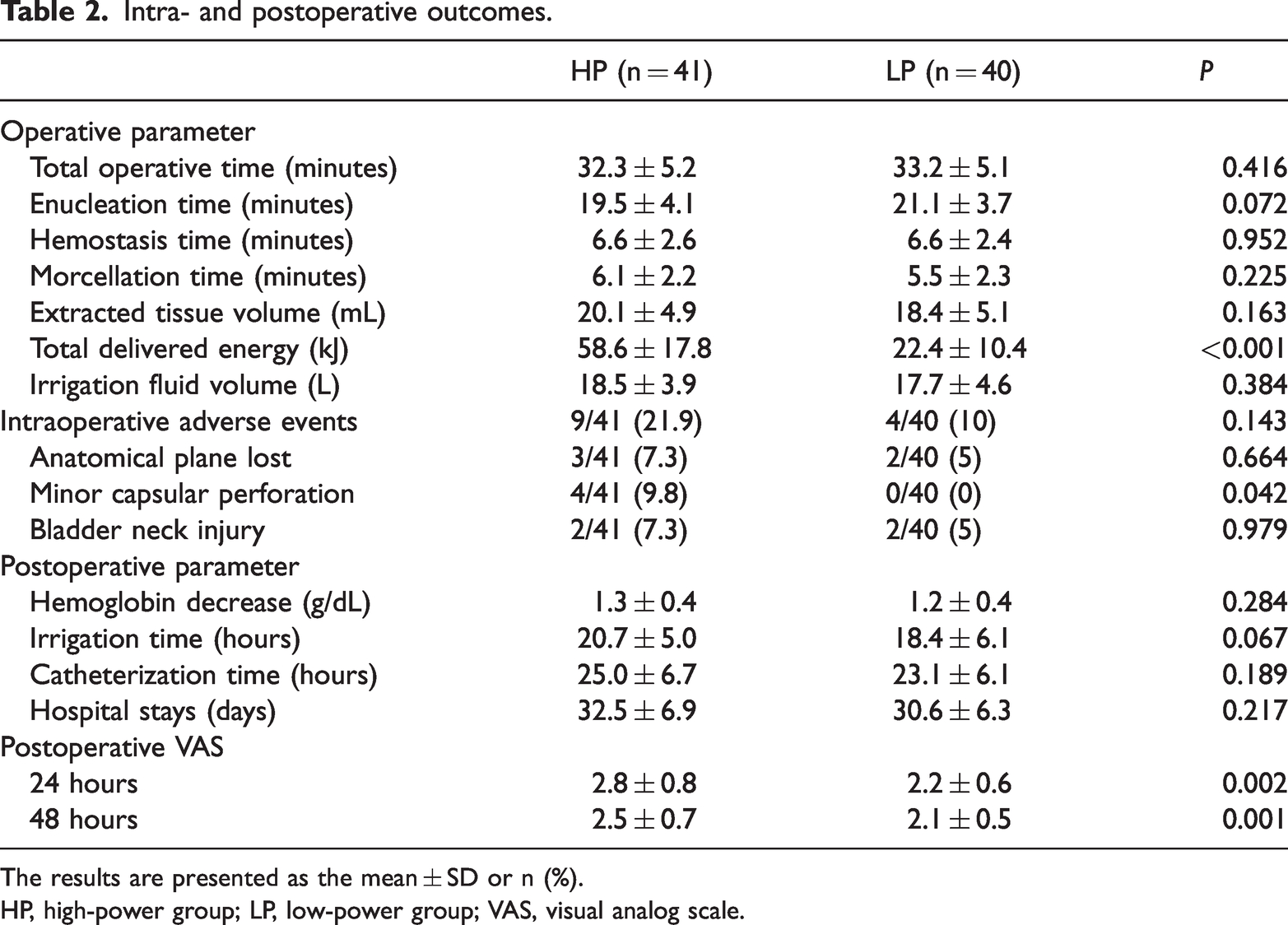
The results are presented as the mean ± SD or n (%).
HP, high-power group; LP, low-power group; VAS, visual analog scale.
At baseline, the mean IPSS was similar between the groups, At the 1-month follow-up, both groups displayed significant improvement, but the score was significantly lower in the LP group (11.4 ± 2.1) than in the HP group (12.5 ± 2.2; P = 0.023). However, at the 3- and 6-month follow-ups, there were no significant differences between the groups, with both groups exhibiting continued improvement (Figure 2(a)).
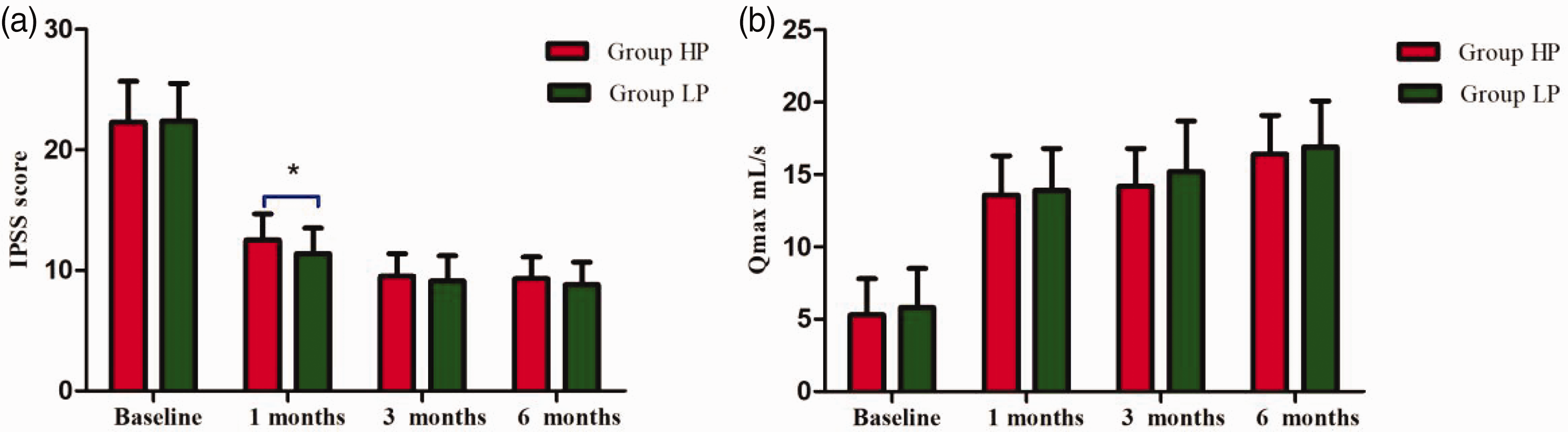
Changes in IPSS and Qmax over time changed in the two groups. (a) IPSS. (b) Qmax. The results are presented as the mean ± SD. IPSS, International Prostate Symptom Score; Qmax, peak urinary flow rate.
Similarly, Qmax was improved significantly in both groups postoperatively. At baseline, the HP group had a mean Qmax of 5.3 ± 2.5 mL/s, compared with 5.8 ± 2.7 mL/s in the LP group (P = 0.405). At 1 month after surgery, Qmax increased substantially in both groups (HP, 13.6 ± 2.7 mL/s; LP, 13.9 ± 2.9 mL/s), with no significant difference noted between the groups (P = 0.554). Improvements continued through 6 months, and the differences between groups remained non-significant (Figure 2(b)).
Secondary outcomes
The OABSS decreased over time in both groups without significant differences at any time point (all P > 0.05; Table 3). PVR also decreased significantly in both groups, with no significant intergroup differences at any time point (all P < 0.1; Table 3). Urine volume increased over the follow-up period in both groups, with no significant differences between the groups at any time point (all P < 0.1; Table 3).
Functional outcomes.
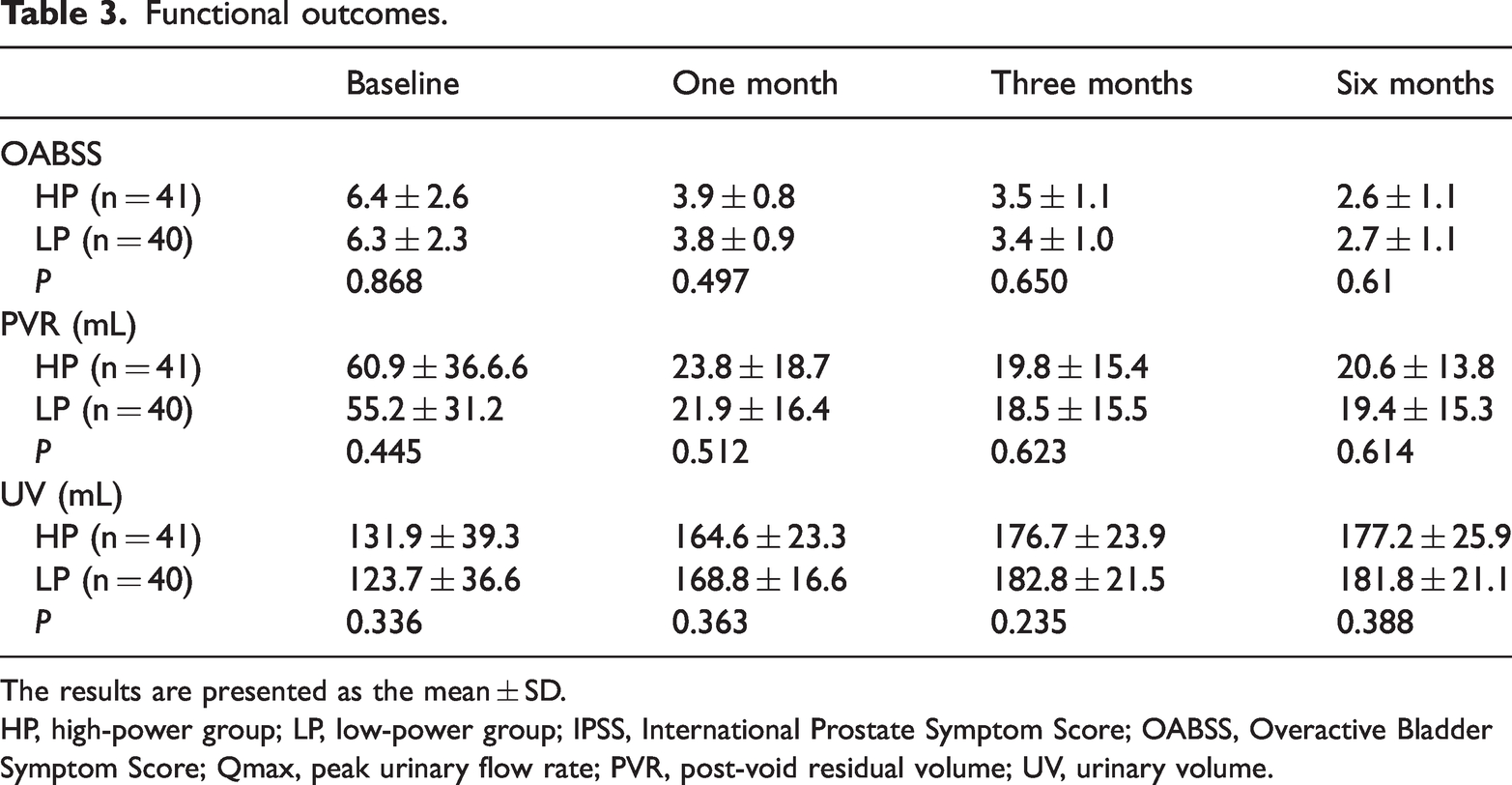
The results are presented as the mean ± SD.
HP, high-power group; LP, low-power group; IPSS, International Prostate Symptom Score; OABSS, Overactive Bladder Symptom Score; Qmax, peak urinary flow rate; PVR, post-void residual volume; UV, urinary volume.
At the 1-month follow-up, the incidence of complications was low in both groups. One patient in the HP group (2.4%) experienced transient stress urinary incontinence (SUI), classified as Clavien–Dindo grade I, versus no cases in the LP group (P = 0.320). Significant hematuria occurred in three patients, including two patients in the HP group and one patient in the LP group (P = 0.571). Urinary tract infections were equally distributed between the HP (7.3%) and LP (7.5%) groups (P = 0.975).
At 6 months, no cases of mild SUI were reported in either group. Two patients (2.5%), including one patient in each group, developed urethral strictures (P = 0.986). One patient in the HP group (2.4%) developed a bladder neck contracture, with no cases reported in the LP group (P = 0.320; Table 4).
Complications in the HP and LP groups.
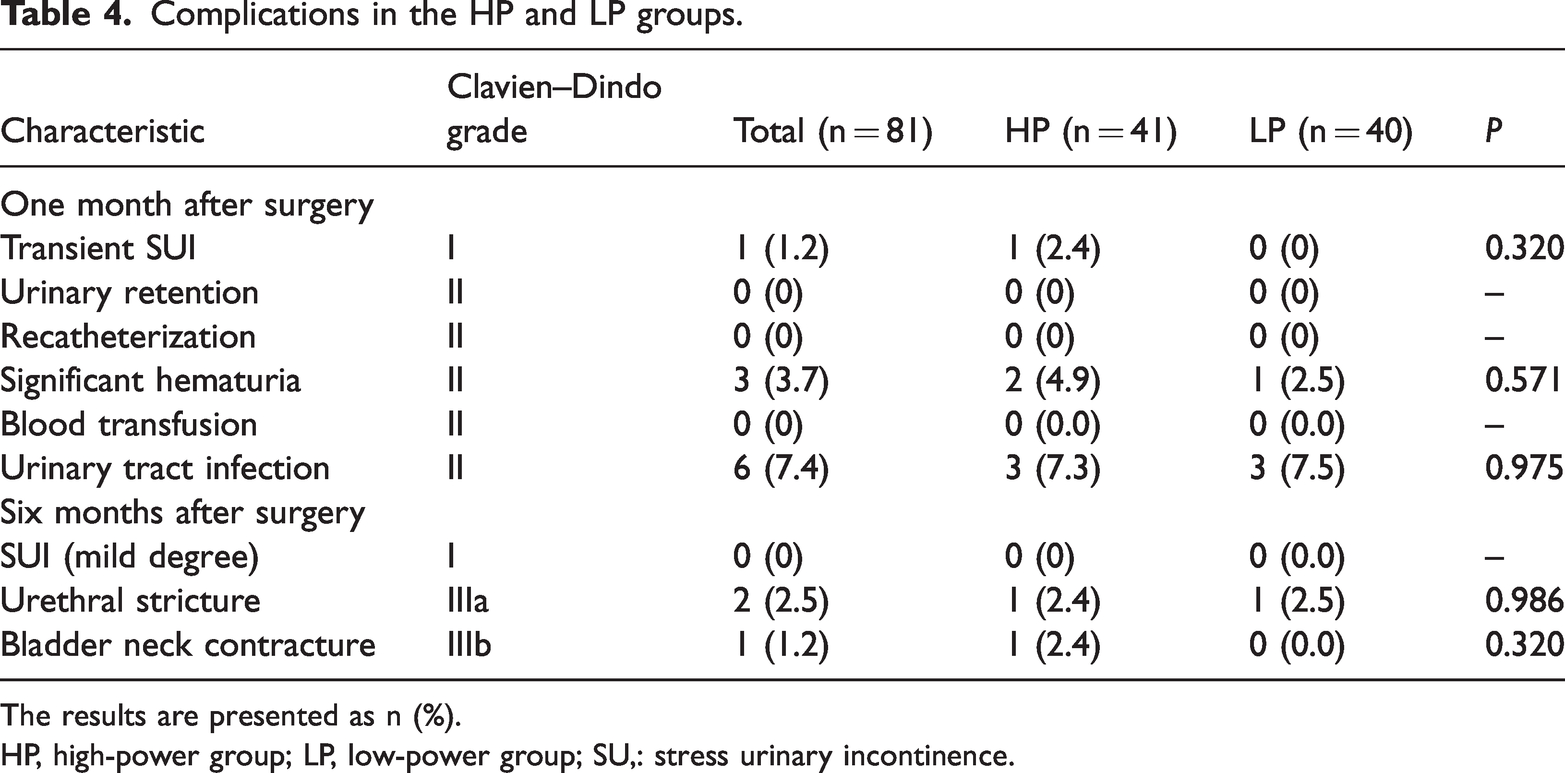
The results are presented as n (%).
HP, high-power group; LP, low-power group; SU,: stress urinary incontinence.
Discussion
Our study investigated the safety and efficacy of LP and HP HoLEP in patients with symptomatic small-volume BPH. The findings indicated that LP HoLEP, compared with HP HoLEP, does not extend the surgical duration, and it achieves similar enucleation efficiency with significantly lower energy consumption. Additionally, LP HoLEP is associated with reduced postoperative pain and favorable IPSS outcomes.
One of the primary concerns with using lower power for HoLEP is the potential increase in operative time because of the reduced laser efficacy. However, our results demonstrated no difference in operative times the LP and HP groups. This finding suggests that lower power settings do not necessarily compromise surgical efficiency.12,14 The efficient enucleation achieved with LP HoLEP can be attributed to the refinement of surgical techniques and the surgeon’s expertise, as emphasized by Becker et al. 15
A significant advantage of LP HoLEP is the reduced total energy usage. Our study revealed that the total delivered energy was substantially lower in the LP group than in the HP group. This reduction in energy consumption is beneficial, as it minimizes the potential for thermal damage to surrounding tissues, thereby enhancing patient safety.16,17 Similar findings were reported by Gazel et al., who noted that lower energy settings can achieve effective prostate tissue removal without compromising the procedure’s effectiveness. 14
Postoperative pain is a critical factor influencing patient recovery and overall satisfaction. In our study, patients in the LP group reported significantly lower VAS scores for pain at 24 and 48 hours postoperatively. Despite this observed difference, the findings cannot be conclusively attributed to the lower power settings alone. 18 Given the similar absorption properties of the holmium laser at both high and low energies, factors such as the absence of capsular perforation in the LP group might have contributed to the reduced postoperative pain. Both the LP and HP groups exhibited notable enhancements of IPSS, OABSS, Qmax, and PVR versus the baseline measurements. It is noteworthy that the LP group exhibited a slightly greater improvement in IPSS at 1 month after surgery. However, this difference was not maintained at subsequent follow-up points. These findings indicates that both LP and HP HoLEP effectively alleviate BPH symptoms and improve urinary function.19,20 This result suggests that LP HoLEP represents a long-lasting solution for patients with BPH.
The findings of our study indicated that the overall incidence of intraoperative complications was comparable between the LP and HP groups. This included events such as anatomical plane loss and bladder neck injury, which occurred at similar frequencies between the groups. However, minor capsular perforation only occurred in the HP group. This discrepancy suggests a potential advantage of LP HoLEP in mitigating the risk of capsular perforation. This observation can be attributed to the anatomical characteristics and laser settings commonly encountered in small-volume BPH cases. A smaller prostate volume is commonly associated with thinner prostatic capsules, which might render them more susceptible to laser energy penetration and potential perforation. Furthermore, the use of higher power settings in HP HoLEP might expedite the procedure but concomitantly elevate the risks of thermal damage and tissue disruption, thereby augmenting the likelihood of capsular perforation.21,22
The safety profile of LP HoLEP was further substantiated by analyzing a number of parameters, including postoperative decreases in hemoglobin levels, irrigation time, catheterization time, and the Clavien–Dindo classification of complications at 1, 3, and 6 months after surgery. No significant differences were observed between the LP and HP groups for any of the aforementioned categories. This is consistent with previous research by Elshal and Scoffone, who demonstrated that lower power settings in HoLEP do not compromise patient safety.16,23 The comparable complication rates between the groups further substantiate the safety and viability of LP HoLEP as a viable alternative to HP HoLEP.
Our study demonstrated that LP HoLEP has similar efficacy as HP HoLEP for patients with small prostates (<40 mL), with added benefits such as reduced energy usage and lower postoperative pain. However, the advantages of higher power settings might become more significant as prostate size increases. For prostates larger than 80 to 100 mL, higher power settings typically enhance the efficiency of enucleation and hemostasis, leading to shorter operative times and better control of intraoperative blood loss. Therefore, HP HoLEP might be preferable for larger prostates (>80 mL). Nonetheless, further research is necessary to define the optimal power settings for different prostate sizes, particularly in larger-volume BPH cases, in which maximizing enucleation efficiency and minimizing bleeding are crucial.
Despite these findings, several limitations must be acknowledged. First, the study was limited to patients with small prostate volumes (<40 mL), and thus, the results might not be applicable to larger prostates, for which higher power settings could offer greater benefits. Second, the follow-up period was restricted to 6 months, which is insufficient to fully assess the long-term outcomes, including symptom relief, recurrence, and potential complications such as urethral strictures or bladder neck contractures. Third, this was a single-blind trial with blinding of patients but not surgeons, which could have introduced bias in outcomes such as the operative time and surgical technique. Lastly, the study was conducted at two centers with highly experienced surgeons, potentially limiting the generalizability of the findings to less experienced surgical teams or different clinical settings. Future research should evaluate the learning curve of LP HoLEP and determine whether similar results can be achieved across various levels of surgical expertise.
Conclusions
This study demonstrated the efficacy and safety of LP HoLEP compared with HP HoLEP for the treatment of symptomatic small-volve BPH. Both power settings produced comparable improvements in urinary symptoms at 6 months. In terms of energy consumption, LP HoLEP displayed advantages over HP HoLEP. Additionally, LP HoLEP was associated with lower postoperative pain scores. Further studies with larger sample sizes and longer follow-up periods are required to confirm these findings and assess the long-term durability of treatment effects.
Footnotes
Author contributions
Zhixiang Gao, Yue Ding, and Haiyong Liu provided major contributions to completing the experiments and writing the manuscript. Follow-up was performed by Renji Du, Zhiwei Sun, and Lijuan Gu. Li Xu analyzed and interpreted the data. Rong Wang and Ping Wang designed and participated in the entire experiment. All authors read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors have declared that no conflict of interest exists.
Funding
This study was supported by the Science and Technology Project of Changzhou Health Committee (ZD202034).