
Abstract
Study Design
Systematic review.
Objective
Degenerative cervical myelopathy (DCM) is a common spinal cord disorder necessitating surgery. We aim to explore how effectively diffusion tensor imaging (DTI) can distinguish DCM from healthy individuals and assess the relationship between DTI metrics and symptom severity.
Methods
We included studies with adult DCM patients who had not undergone decompressive surgery and implemented correlation analyses between DTI parameters and severity, or compared healthy controls and DCM patients.
Results
57 studies were included in our meta-analysis. At the maximal compression (MC) level, fractional anisotropy (FA) exhibited lower values in DCM patients, while apparent diffusion coefficient (ADC), mean diffusivity (MD), and radial diffusivity (RD) were notably higher in the DCM group. Moreover, our investigation into the diagnostic utility of DTI parameters disclosed high sensitivity, specificity, and area under the curve values for FA (.84, .80, .83 respectively) and ADC (.74, .84, .88 respectively). Additionally, we explored the correlation between DTI parameters and myelopathy severity, revealing a significant correlation of FA (.53, 95% CI:0.40 to .65) at MC level with JOA/mJOA scores.
Conclusion
Current guidelines for DCM suggest decompressive surgery for both mild and severe cases. However, they lack clear recommendations on which mild DCM patients might benefit from conservative treatment vs immediate surgery. ADC’s role here could be pivotal, potentially differentiating between healthy individuals and DCM. While it may not correlate with symptom severity, it might predict surgical outcomes, making it a valuable imaging biomarker for clearer management decisions in mild DCM.
Introduction
Degenerative cervical myelopathy (DCM) is the most prevalent spinal cord disorder resulting in significant neurologic dysfunctions and is a leading cause of cervical spine surgical procedures.1,2 Despite progress in medical knowledge, there remains a critical need for non-invasive, reliable measures for evaluating the condition of the spinal cord in patients with DCM.3,4 While magnetic resonance imaging (MRI) is the established imaging technique for diagnosing DCM and aids in guiding treatment strategies, it predominantly identifies anatomical compression factors like the intervertebral disc, ligamentum flavum, vertebral osteophytes, facet joints, and ossification of the posterior longitudinal ligament. 5 It also detects T2-weighted hyperintensity within the spinal cord. However, MRI’s efficacy is limited by its inability to consistently align with clinical symptoms, as it often fails to reveal microscopic changes in the spinal cord, which are crucial in DCM. 6
Emerging in the field of neuroimaging, diffusion tensor imaging (DTI) has offered new insights into the pathology of the central nervous system disorders, particularly in DCM. 7 DTI’s ability to trace water molecule diffusion at microscopic scales provides for the assessment of spinal cord microstructure. DTI has revealed significant variations in the cervical spinal cord at the point of maximal compression in DCM cases. 8 A key measurement in DTI is Fractional Anisotropy (FA), which ranges from 0 to 1, indicating the directionality of water diffusion. 9 High FA values in a healthy spinal cord suggest a uniform direction of axonal paths, similar to aligned straws. In contrast, conditions like DCM disrupt this uniformity, leading to decreased FA. 9 DTI also tracks other indices such as Mean Diffusivity (MD), Apparent Diffusion Coefficient (ADC), Axial Diffusivity (AD), and Radial Diffusivity (RD). These indices measure the average rate and direction of water diffusion in tissue.
Although initial studies have linked DTI parameters to preoperative clinical evaluations, the full diagnostic potential of DTI in differentiating between DCM patients and healthy individuals remains largely uncharted. Recent studies highlight the significance of preoperative FA in correlating with postoperative myelopathy severity measured by the Japanese Orthopedic Association (JOA) or modified JOA (mJOA) scores, particularly in older individuals and those with longer follow-up periods. 10 Notably, recovery rates showed a substantial correlation with ADC across various age groups. Nevertheless, no significant correlations were identified between other DTI parameters (MD, AD) and postoperative outcomes.
This systematic review and meta-analysis was designed to explore these areas. The goal is to define the effectiveness of DTI to distinguish DCM from healthy individuals and to assess the relationship between DTI metrics and symptom severity, as indicated by JOA and mJOA.
Methods
Protocol Registration and Compliance
The protocol for this systematic review was formally registered with PROSPERO, the International Prospective Register of Systematic Reviews, under the identifier CRD42023417303. Details of the protocol are accessible via the PROSPERO database (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023417303). Adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines was maintained throughout the study to ensure a rigorous and transparent methodology.
Literature Search Strategy
A methodical and comprehensive literature search was conducted across several electronic databases, namely PubMed, Web of Science, and EMBASE, to identify relevant studies. The search, performed in December 2023 by author FF, was not limited by language constraints. The search strategy was meticulously designed using specific keywords such as “degenerative cervical myelopathy”, “cervical spondylotic myelopathy”, “diffusion tensor imaging”, and “fractional anisotropy”. Each database search was customized with a unique combination of these terms to maximize retrieval efficiency. Additionally, manual searches were conducted within the reference lists of key articles to uncover further applicable studies.
Inclusion and Exclusion Criteria
The systematic review encompassed primary studies of any design. For inclusion in this systematic review, manuscripts needed to meet the following eligibility criteria: (1) Enrolment of adult patients diagnosed with DCM who have not undergone any form of decompressive surgery for the condition, (2) Evaluation of the impact of DTI parameters on patient symptoms or comparing them to healthy subjects, (3) Reporting symptom severity by JOA or mJOA, (4) Implementation of any correlation analysis between DTI parameters and severity, or comparing them between healthy and DCM (5) Reporting of a correlation coefficient or mean and P-value or 95% CI for it. Studies failing to adhere to these specifications were excluded. No restrictions on the publication dates of the potential studies were imposed.
Study Selection Process
The study selection was executed via a systematic and rigorous approach. Initially, 2 independent reviewers, MM and FR, conducted a preliminary screening by examining titles and abstracts, thereby eliminating unrelated studies. Subsequently, these reviewers performed a detailed assessment of the full texts against the predefined inclusion and exclusion criteria. Discrepancies were resolved through discussion or, if necessary, consultation with a third reviewer, FF, to reach a consensus.
Data Extraction Methodology
Data extraction was independently carried out by 2 reviewers (FF and MM), using a pre-tested, standardized template in MS Excel. EndNote software facilitated reference management. Extracted data encompassed demographic information, radiographic data including DTI measures, MRI protocols, clinical or radiographic measurements, JOA or mJOA scores, diagnostic accuracy data (e.g., AUC, specificity, sensitivity), and correlation or comparison metrics. Discrepancies in data extraction were addressed through discussion and consensus.
Risk of Bias Assessment
The QUADAS-2 tool, recommended for bias assessment in systematic reviews of diagnostic accuracy studies, was employed. This tool evaluates 4 domains: patient selection, index test, reference standard, and flow and timing. Two researchers (FF and FR) independently applied this tool to each study, with their assessments exhibiting complete agreement, underscoring the consistency of the evaluation process.
Data Analysis Techniques
A variety of statistical methods were employed for data synthesis. Initially, pooled mean and mean difference meta-analyses were conducted to compare various DTI parameters between DCM patients and healthy controls. For correlation data between DTI parameters and JOA/mJOA scores, Spearman and Pearson correlations were first transformed to z-scores using the inverse variance method to calculate pooled effect sizes and then back-transformed for reporting. We acknowledge the distinction between Spearman and Pearson correlations in assessing different types of relationships, yet both measures quantify the strength and direction of associations between variables. By integrating both Spearman and Pearson correlations, we aimed to capture a wider range of associations and provide a more nuanced understanding of the underlying relationships within the dataset.
To pool diagnostic accuracy data (sensitivity, specificity, AUC) for DTI parameters distinguishing between healthy and DCM subjects, a proportional meta-analysis was initially performed. Additionally, for AUC analysis, pooled means and 95% confidence intervals of DTI parameters were utilized, especially when direct diagnostic accuracy tests were less prevalent in the studies. This analysis assumed a binormal distribution for DTI parameters, with pooled standard errors reflecting the combined variability in control and DCM groups. Z-scores were calculated to quantify the distinction between the mean DTI values of both groups, and subsequently transformed into AUC values using the standard normal distribution’s cumulative distribution function.
All meta-analyses were also subgrouped based on levels used for DTI indices measurements and based on age. An age of 65 was used as the cut-off point for the age subgroup as this age defines the elderly subgroup, and we wanted to see if DTI indices could be valuable in both age groups. 10 Heterogeneity among studies was quantified using the I2 statistic. The pooled effect size is reported as a pooled correlation coefficient with a 95% confidence interval. All statistical analyses were conducted using R version 4.2.3.
Results
Literature Search
With our initial search, 1115 records were identified, of which 302 duplicates were removed. Then, after screening titles and abstracts, 715 were further excluded. After reviewing full texts an additional 41 articles were excluded. Finally, 57 eligible studies were used for data extraction and quality assessment (Figure 1). PRISMA flow chart for this review.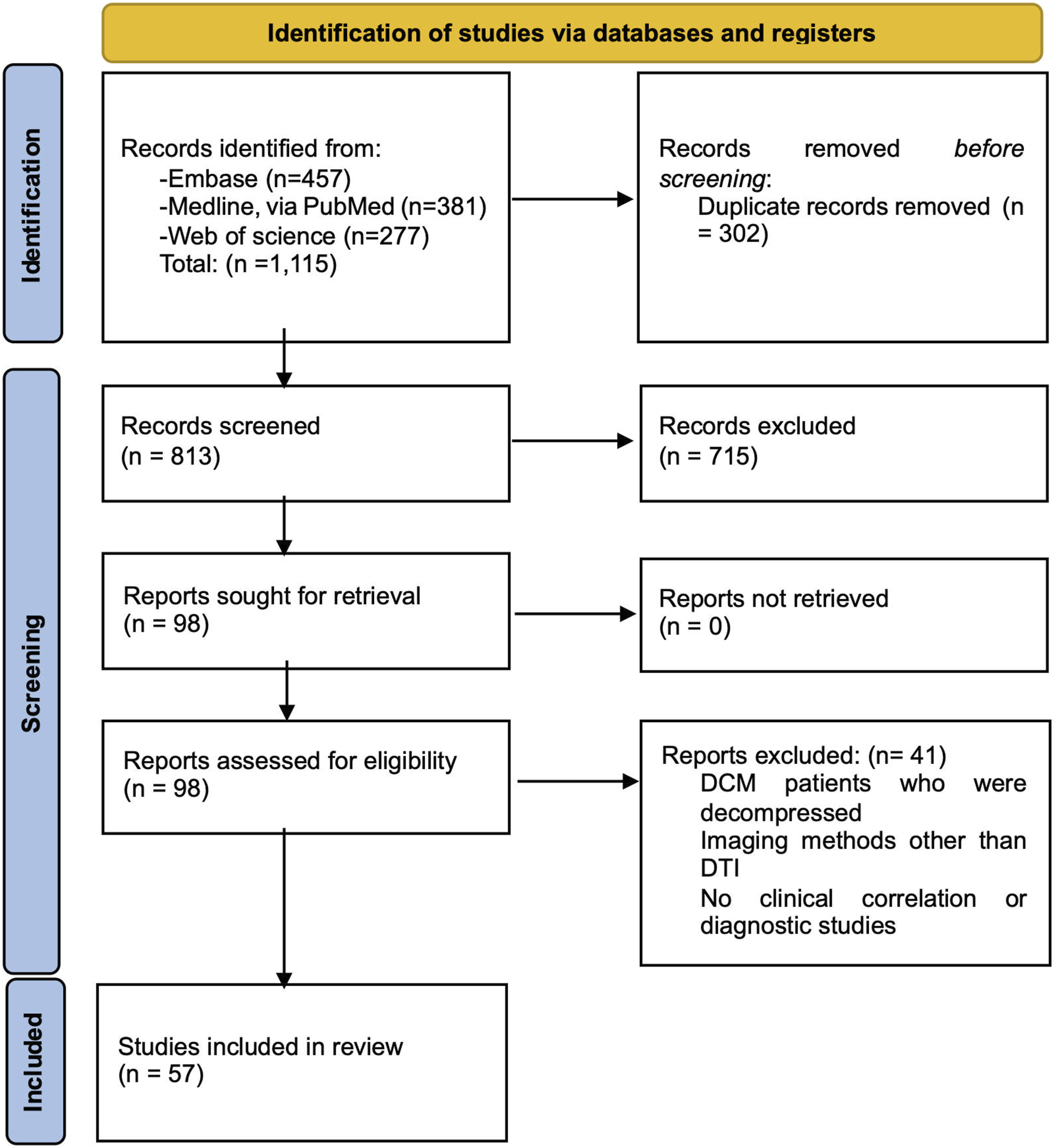
Quality Assessment
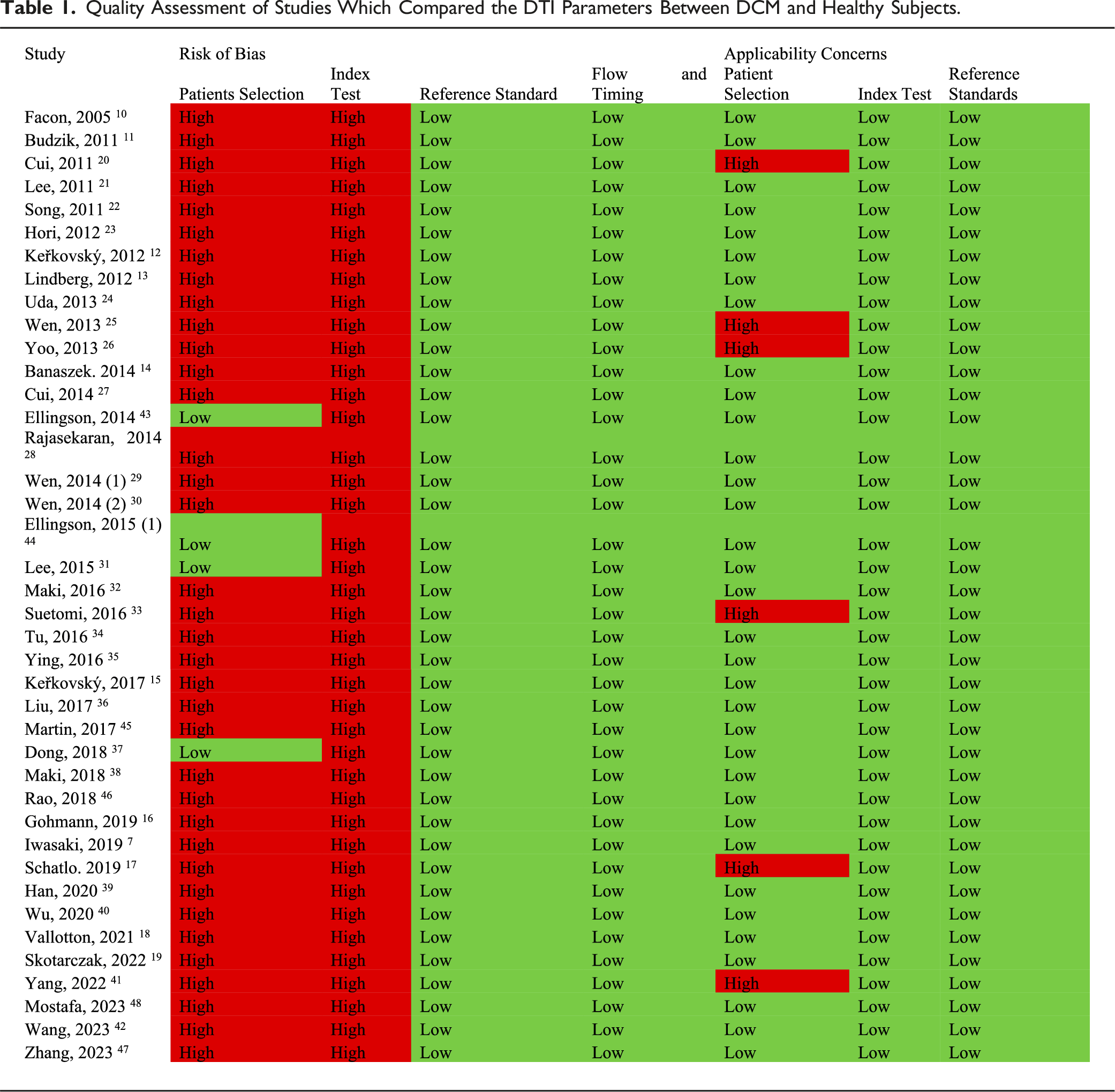
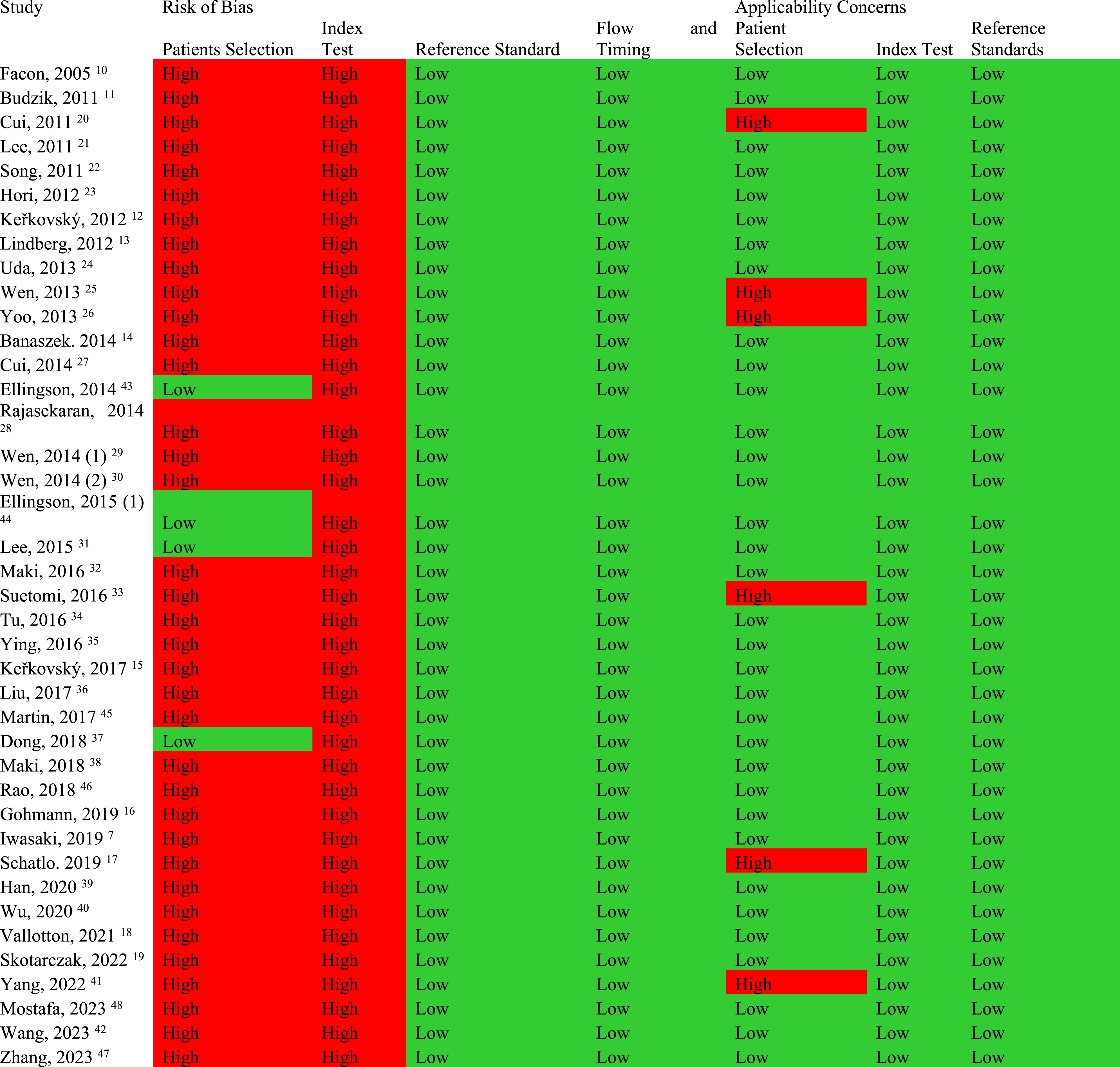
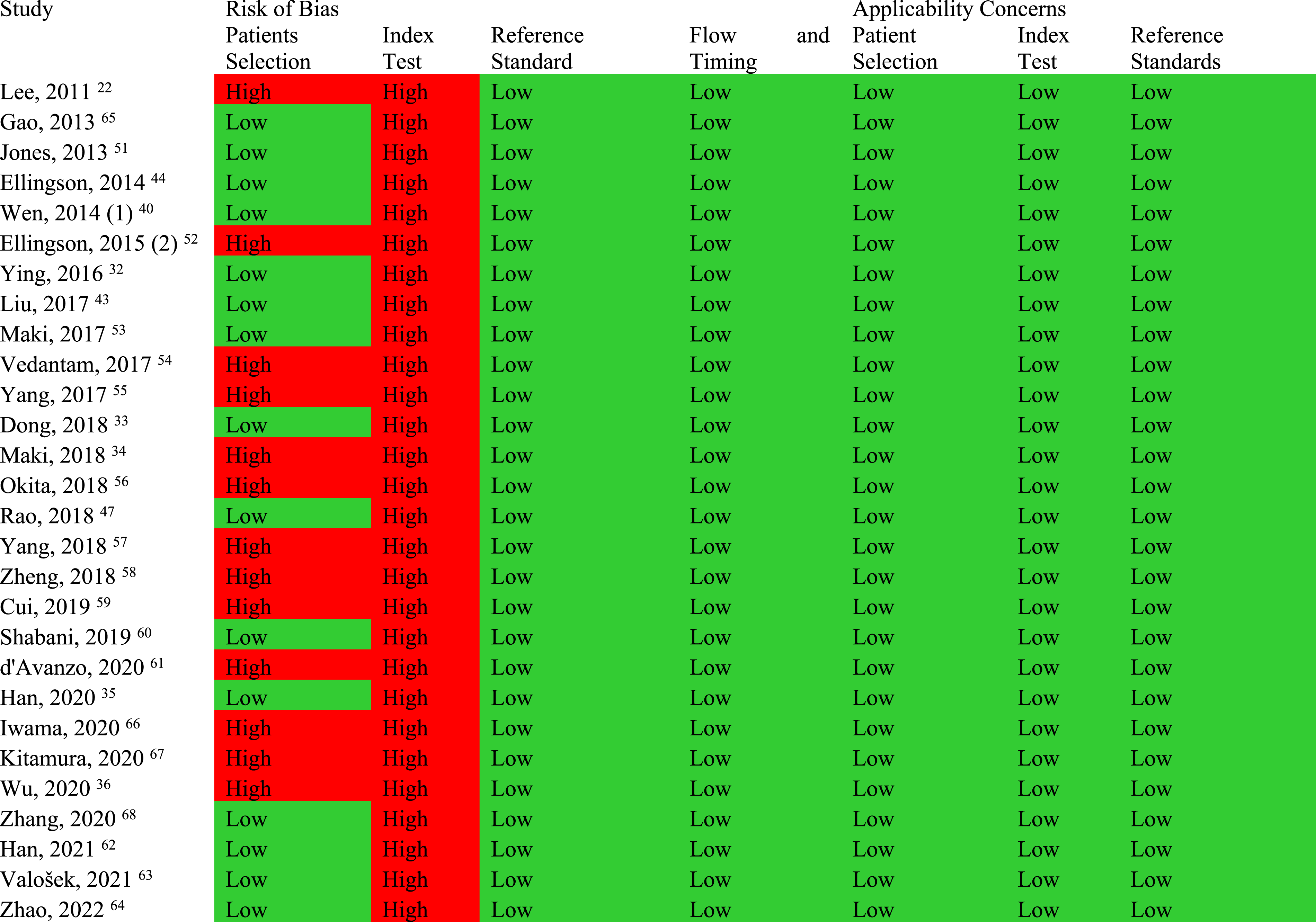
Quality Assessment of Studies Which Compared the DTI Parameters Between DCM and Healthy Subjects.
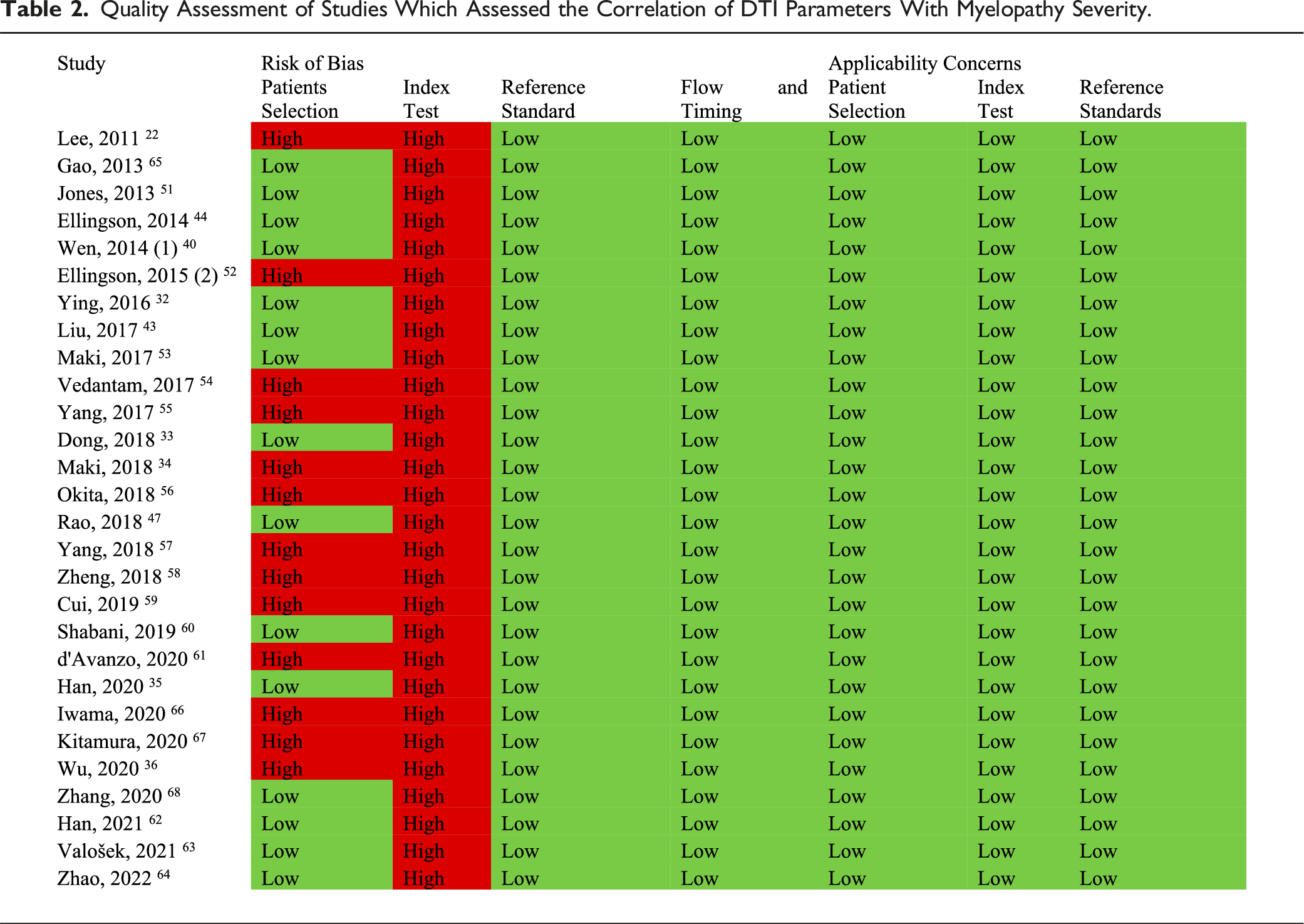
Quality Assessment of Studies Which Assessed the Correlation of DTI Parameters With Myelopathy Severity.
Comparison of DTI Parameters Between DCM and Healthy Subjects
Study Characteristics of Studies Which Compared the DTI Parameters Between DCM and Healthy Subjects.
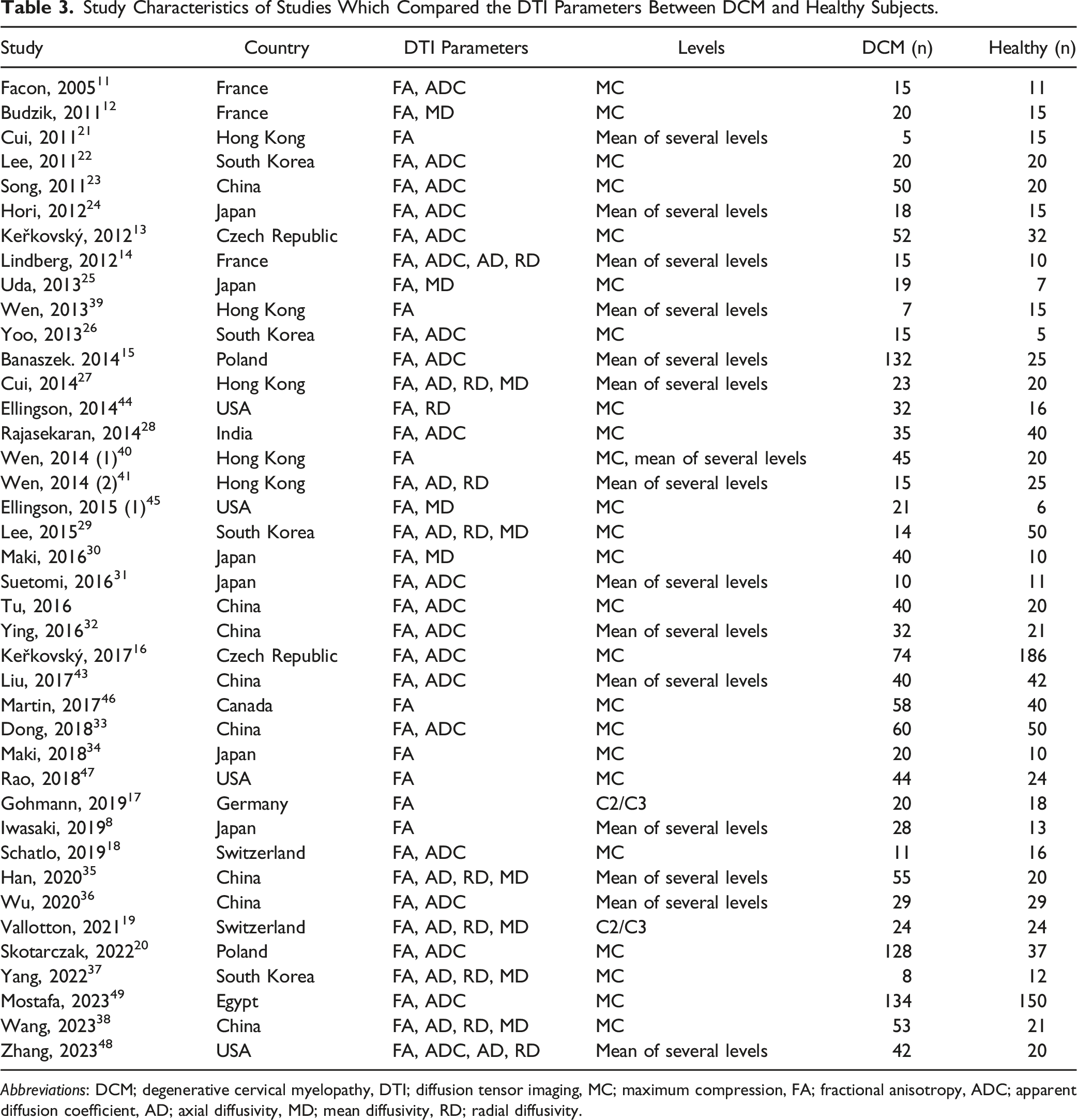
Abbreviations: DCM; degenerative cervical myelopathy, DTI; diffusion tensor imaging, MC; maximum compression, FA; fractional anisotropy, ADC; apparent diffusion coefficient, AD; axial diffusivity, MD; mean diffusivity, RD; radial diffusivity.
The DTI parameters analyzed included FA, ADC, AD, RD, and MD. FA and ADC were the most frequently measured parameters. Among these studies, 24 utilized DTI parameters from the maximal compression level of the cervical spine (MC),11-13,16,18,20,22,23,25,26,28-30,33,34,37,38,40,42,44-47,49 15 calculated the mean DTI values from several cervical spine levels,8,14,15,21,24,27,31,32,35,36,39-41,43,48 and 2 focused on the C2/C3 level.17,19
We performed a meta-analysis to compare the mean differences in FA values between DCM patients and healthy subjects. This analysis was conducted separately for studies measuring FA at MC,11-13,16,18,20,22,23,25,26,28,30,33,34,37,38,40,42,44-47,49 and for those assessing the mean across several levels.8,14,15,21,24,27,31,32,35,36,39-41,43,48 The results, depicted in Figure 2 forest plots, indicate that FA values are significantly lower in DCM patients at both MC and the averaged levels. Subgroup analysis for elderly (aged 65 years and older) and non-elderly populations showed significant differences in both subgroups (Figure 2). Meta-analysis for comparison of FA between DCM and healthy subjects. (A) Mean differences in FA at maximum compression level, grouped by age. (B) Mean differences in mean FA of all levels, grouped by age.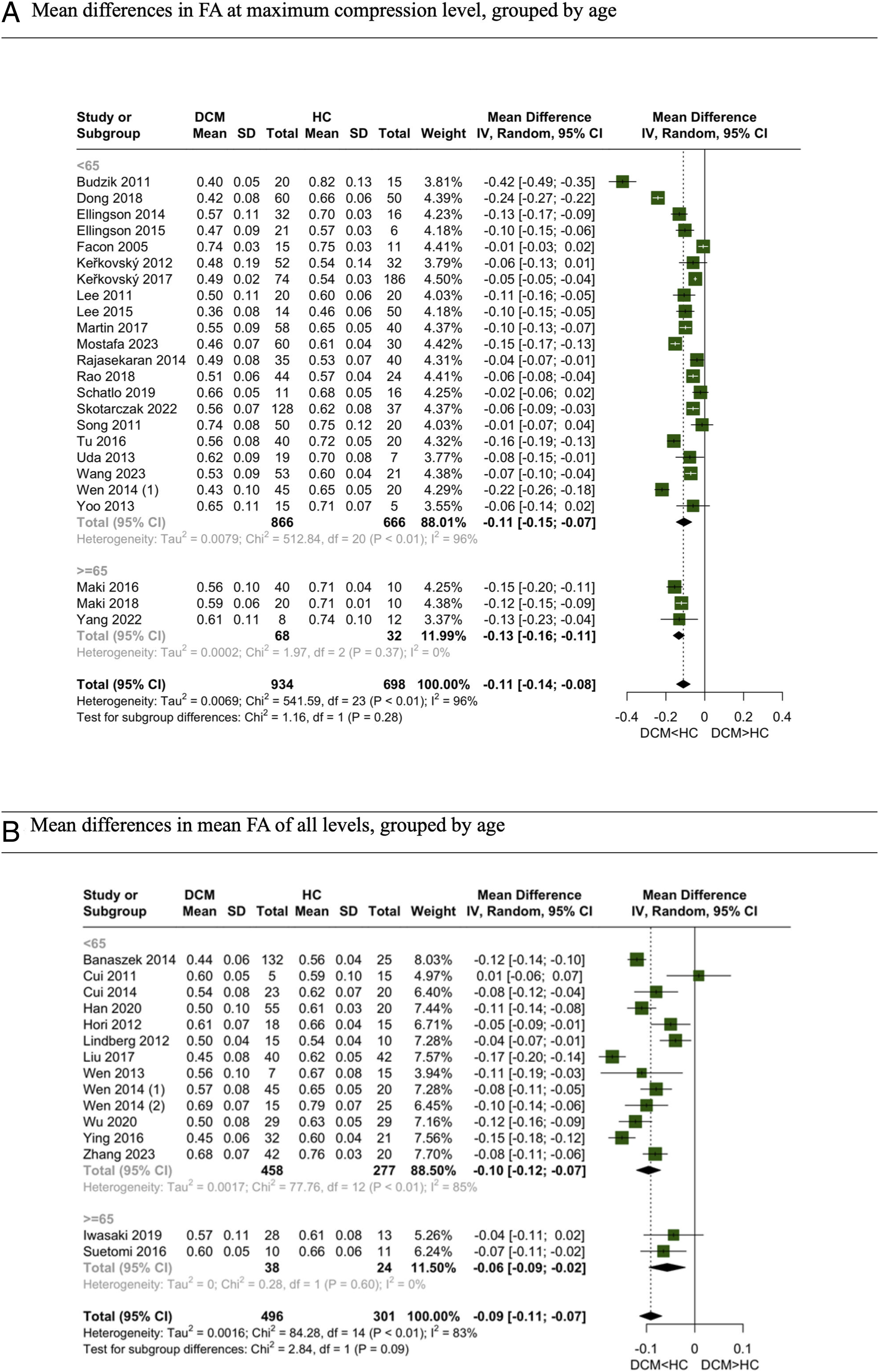
ADC was the second most studied DTI parameter. Meta-analyses were conducted separately for studies examining ADC values at MC11,13,16,18,20,22,23,26,28,33,42,49 and those averaging across multiple levels.14,15,24,31,32,36,43,48 In both analyses, ADC values were significantly higher in DCM patients compared to healthy controls. However, nearly all studies, except 1, included participants with a mean age below 65 years; thus, we could not report pooled results for the elderly subgroup (Figure 3). Meta-analysis for comparison of ADC between DCM and healthy subjects. (A) Mean differences in ADC at maximum compression level, grouped by age. (B) Mean differences in mean ADC of all levels, grouped by age.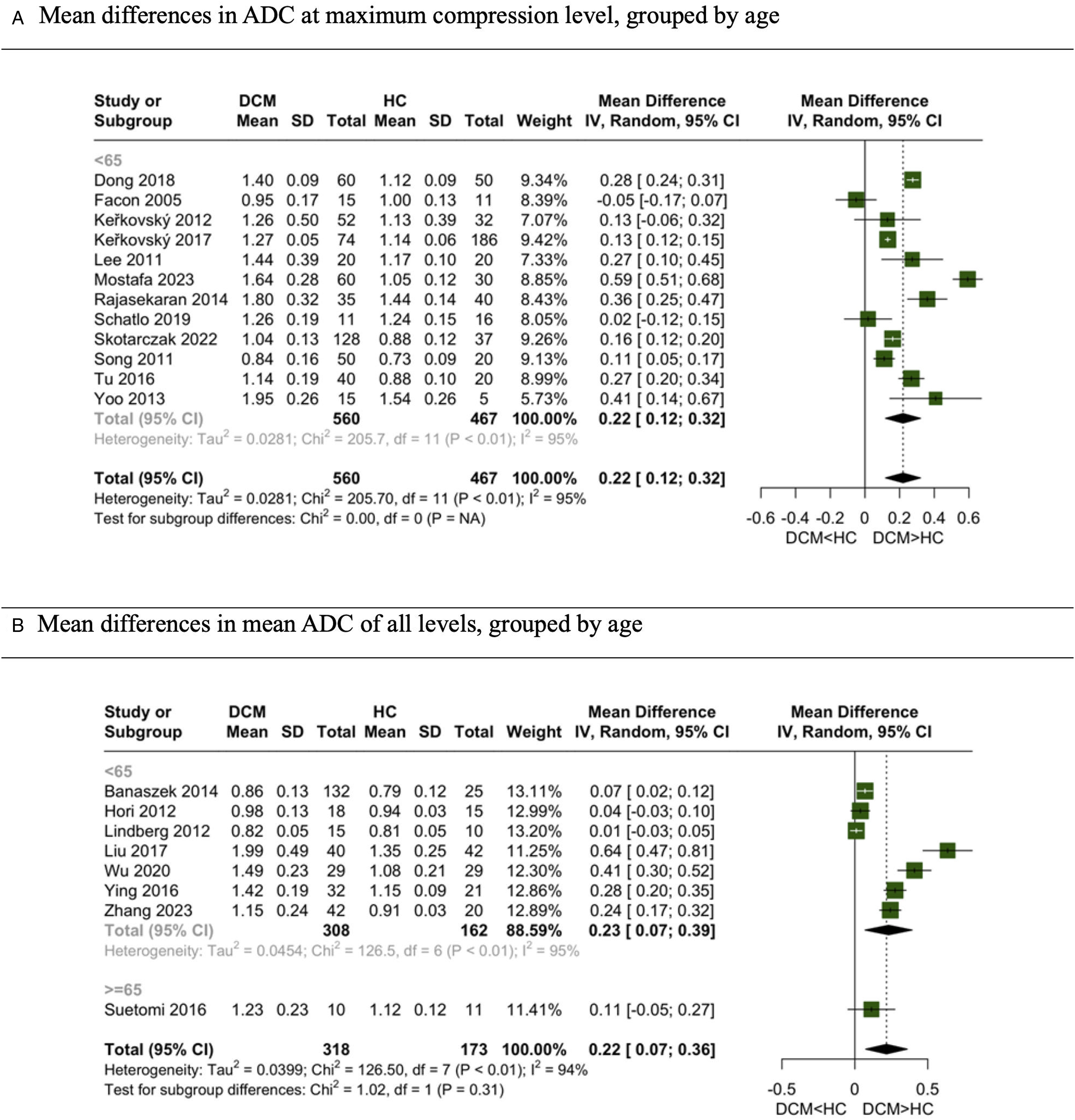
For MD, AD, and RD, separate meta-analyses were conducted for MC and averaged levels. The meta-analysis for MD, focusing on studies at MC,12,25,29,30,37,38,45 revealed higher MD values in DCM patients in both elderly and non-elderly subgroups. However, only 2 studies compared MD as an average of several levels, rendering the pooled results less reliable due to their limited number and it’s not reported here. AD, when pooled, included more studies that assessed the average of several levels14,27,35,41,48; however, no significant difference was found between DCM and healthy groups. Pooled results on AD difference in MC levels are also not reported here as the number of studies was limited. Conversely, RD, which also had a greater number of studies assessing averages,14,27,35,41,48 showed a significantly higher mean in DCM patients in both meta-analyses and age subgroups (Figure 4). Meta-analysis for comparison of MD, AD and RD between DCM and healthy subjects. (A) Mean differences in MD at maximum compression level, grouped by age. (B) Mean differences in mean AD of all levels, grouped by age. (C) Mean differences in RD at maximum compression level, grouped by age. (D) Mean differences in mean RD of all levels, grouped by age.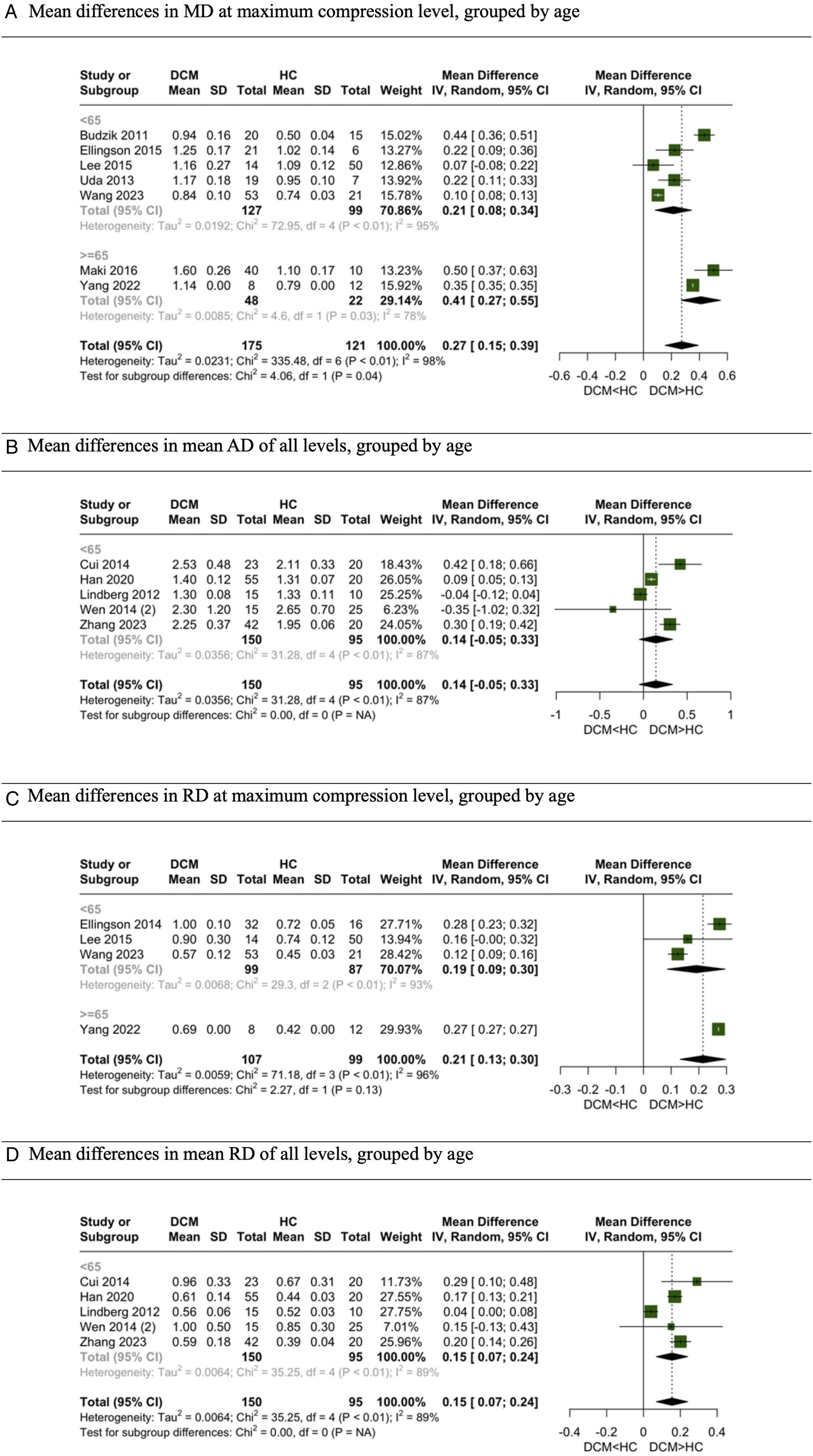
We also explored the pooled results of studies investigating either MC or the average of several levels as the measurement points for DTI parameters. The mean difference in FA between the 2 groups was −.11 (95% Confidence Interval [CI]: −.14 to −.08) in MC studies, −.09 (95% CI: −.11 to −.07) in averaged level studies, and −.10 (95% CI: −.12 to −.08) when all studies were pooled. For ADC, the mean differences were .22 (95% CI: .12 to .32) in MC studies, .22 (95% CI: .07 to .36) in averaged level studies, and .22 (95% CI: .14 to .30) when pooled. The mean differences in MD were .27 (95% CI: .15 to .39) in MC studies, .27 (95% CI: −.02 to −.55) in averaged level studies, and .25 (95% CI: .16 to .35) when pooled. For AD, the mean differences were .14 (95% CI: −.05 to .33) in MC studies, .18 (95% CI: .04 to .40) in averaged level studies, and .15 (95% CI: .04 to .26) when pooled. Lastly, the mean differences in RD were .15 (95% CI: .07 to .24) in MC studies, .21 (95% CI: .13 to .30) in averaged level studies, and .18 (95% CI: .12 to .23) when pooled (Figure 5). Meta-analysis for comparison of DTI parameters of different levels between DCM and healthy subjects. (A) Mean differences in FA, grouped by level of DTI assessment. (B) Mean differences in ADC, grouped by level of DTI assessment. (C) Mean differences in MD, grouped by level of DTI assessment. (D) Mean differences in AD, grouped by level of DTI assessment. (E) Mean differences in RD, grouped by level of DTI assessment.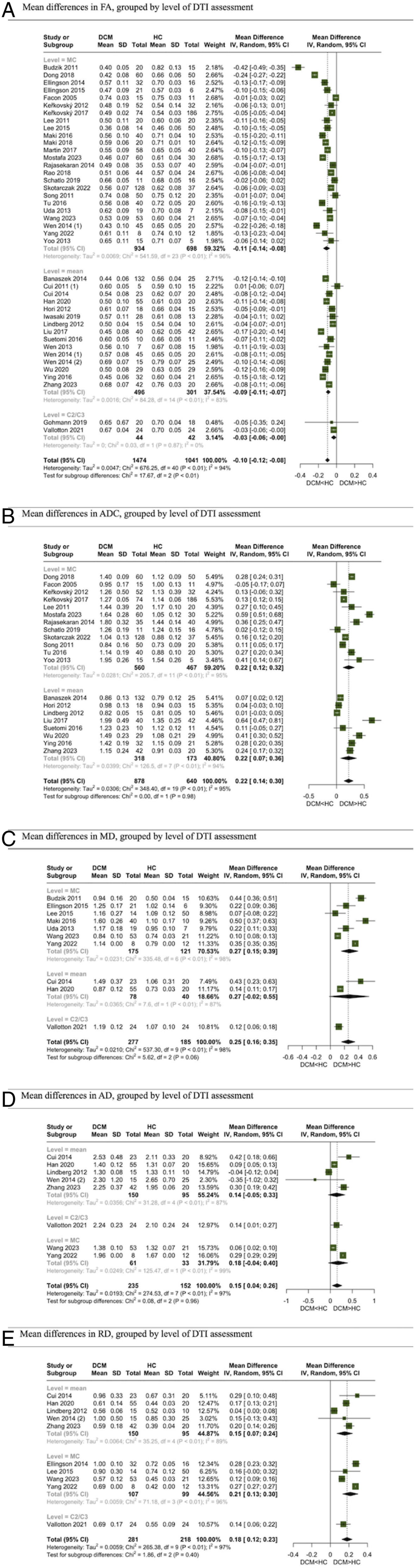
Diagnostic Ability of DTI for DCM
Diagnostic Ability of DTI for DCM.
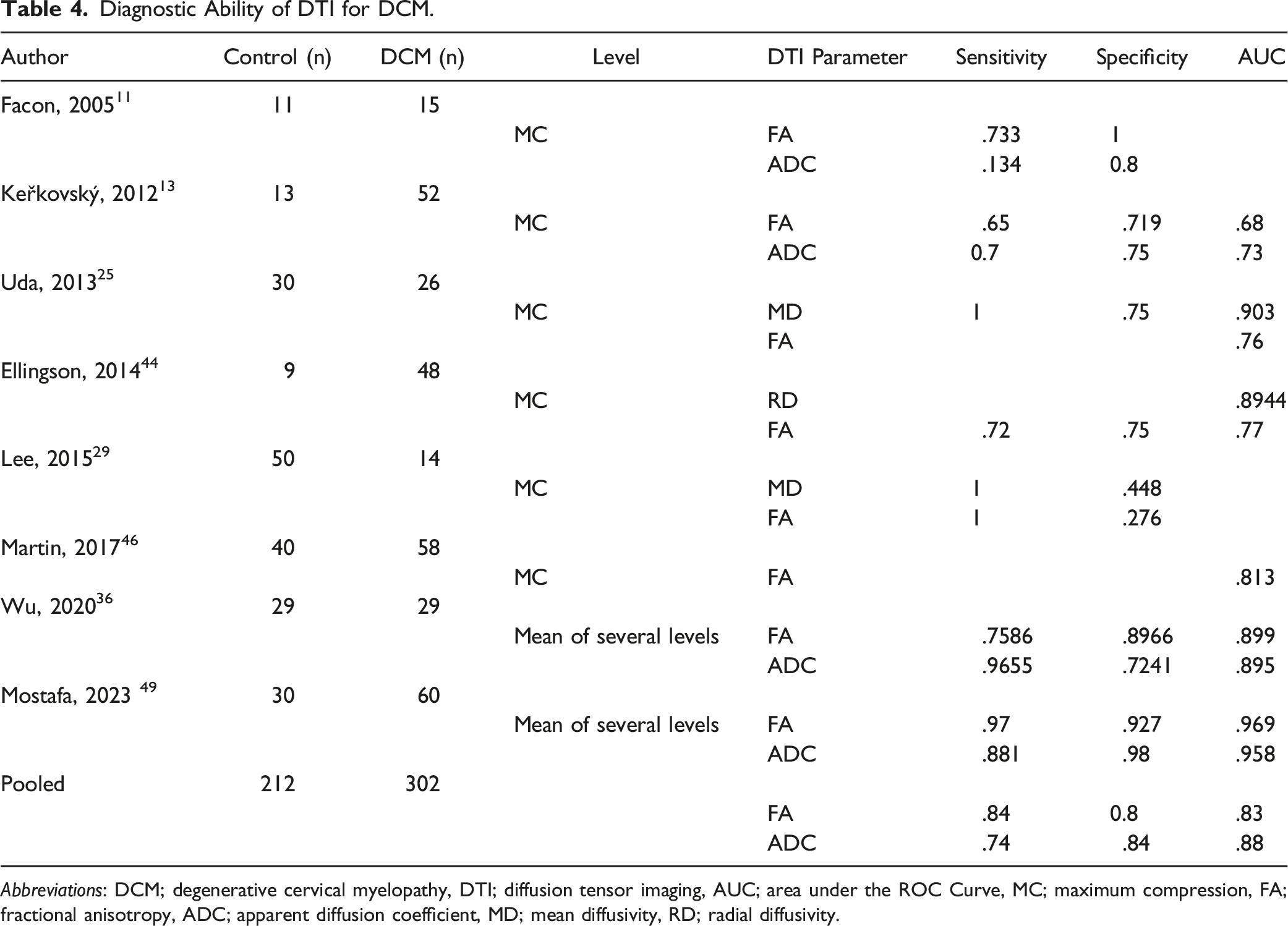
Abbreviations: DCM; degenerative cervical myelopathy, DTI; diffusion tensor imaging, AUC; area under the ROC Curve, MC; maximum compression, FA; fractional anisotropy, ADC; apparent diffusion coefficient, MD; mean diffusivity, RD; radial diffusivity.
Pooled AUC Calculated by Using the Pooled Mean of DTI Parameters.
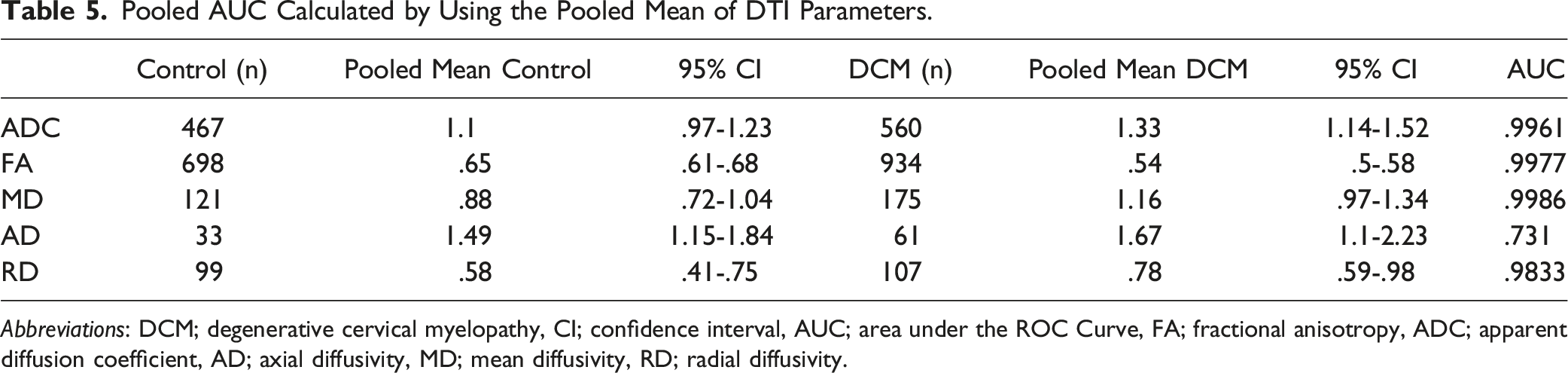
Abbreviations: DCM; degenerative cervical myelopathy, CI; confidence interval, AUC; area under the ROC Curve, FA; fractional anisotropy, ADC; apparent diffusion coefficient, AD; axial diffusivity, MD; mean diffusivity, RD; radial diffusivity.
Correlation of DTI Parameters with Myelopathy Severity Based on JOA or mJOA
Study Characteristics of Studies Which Assessed the Correlation of DTI Parameters With Myelopathy Severity.
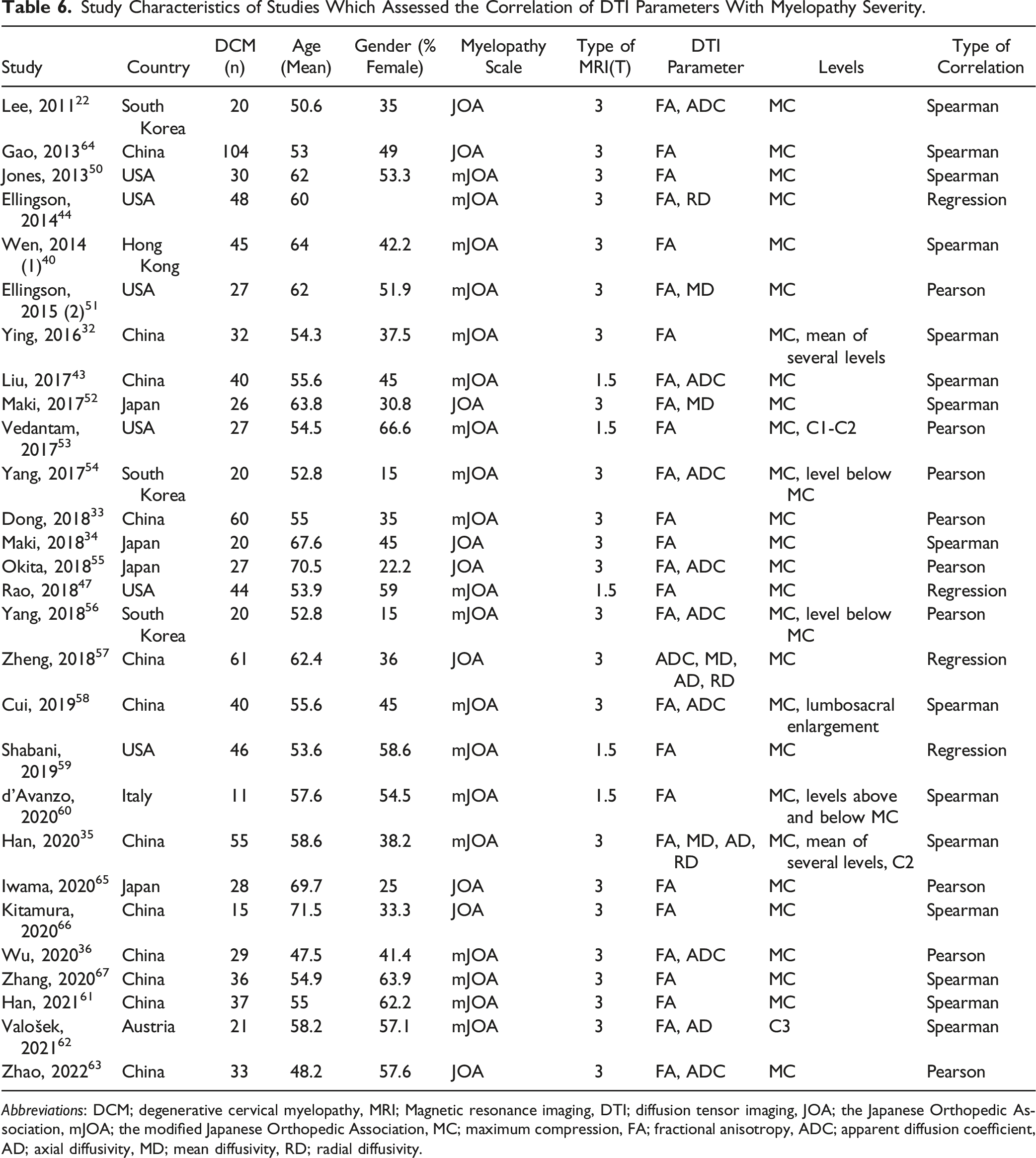
Abbreviations: DCM; degenerative cervical myelopathy, MRI; Magnetic resonance imaging, DTI; diffusion tensor imaging, JOA; the Japanese Orthopedic Association, mJOA; the modified Japanese Orthopedic Association, MC; maximum compression, FA; fractional anisotropy, ADC; apparent diffusion coefficient, AD; axial diffusivity, MD; mean diffusivity, RD; radial diffusivity.
For correlation studies, our analysis was limited to pooling results for MC level DTI parameters due to the scant number of studies at other levels. FA was again the predominant measure used and demonstrated a significant correlation with JOA/mJOA across all subjects and in both age subgroups r = .53 (95% CI: .40-.65). Although ADC was the second most commonly used parameter, it did not exhibit a notable correlation with JOA/mJOA. The sole study focusing on ADC, conducted on a group with an average age of 65, reported an r = −.11 (95% CI: −.31 to .10). Similarly, MD, another parameter for which sufficient data was available for meta-analysis, did not show a significant pooled correlation r = −.23 (95% CI: −.55 to .14). Due to the limited number of studies, results for AD could not be pooled. However, the correlation between RD and JOA/mJOA, analyzed from 3 studies involving samples with an average age below 65 years, revealed a notable correlation r = −.20 (95% CI: −.37 to −.01) (Figure 6). Meta-analysis for Correlation of DTI Parameters with Myelopathy Severity Based on JOA or mJOA at maximum compression level. (A) Correlation of FA with Myelopathy Severity (JOA or mJOA) at maximum compression level. (B) Correlation of ADC with Myelopathy Severity (JOA or mJOA) at maximum compression level. (C) Correlation of MD with Myelopathy Severity (JOA or mJOA) at maximum compression level. (D) Correlation of RD with Myelopathy Severity (JOA or mJOA) at maximum compression level.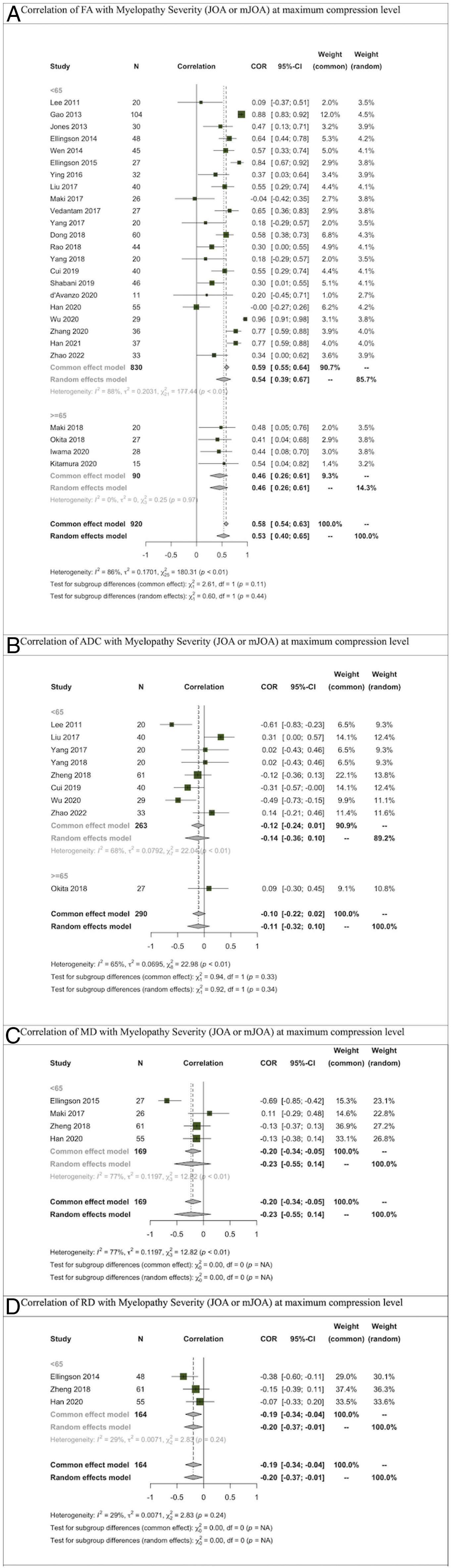
Discussion
This systematic review and meta-analysis synthesize the literature and offer an advancement in understanding DTI’s role in diagnosing and evaluating DCM. A total of 57 studies were included that involved more than 1000 DCM patients, providing a comprehensive assessment of the utility of DTI parameters for diagnosis and correlation with severity. Our findings underscore DTI’s diagnostic reliability, particularly through FA and ADC parameters. The consistent observation of lower FA and higher ADC values in DCM patients across various study populations and methodologies highlights DTI’s potential as a diagnostic tool. This shows promise for clinical use in DCM, where traditional imaging often is limited in early and accurate detection. The high diagnostic accuracy, indicated by aggregated sensitivity, specificity, and AUC values, illustrates the consistent findings and accuracy of DTI and supports the greater integration of DTI into clinical practice.
Studies comparing DTI parameters between healthy individuals and DCM patients assessed these parameters through MC, an average across several levels, or at the C2/C3 space. We aimed to subgroup the mean difference meta-analyses of different parameters based on whether they were measured at MC or averaged across multiple levels (Figure 5). The objective was to determine which measurement type (MC or average of several levels) leads to a larger mean difference when comparing DTI indices between healthy individuals and DCM patients, potentially making it a superior choice for differentiating between healthy and DCM subjects. Upon subgrouping the pooled results by these measurement levels, the pooled difference between healthy and DCM patients indicated that the difference for almost all DTI parameters is equivalent or nearly so across different levels. This significant finding suggests that both methods might possess comparable diagnostic capabilities when differentiating between healthy and DCM subjects or employing DTI for DCM diagnosis.
The correlation between DTI parameters, especially FA, and myelopathy severity assessed by JOA or mJOA scores, is noteworthy. This correlation justifies using DTI not just for diagnosis but also for assessing disease progression and treatment efficacy. Given that the JOA and mJOA assessments have numerous limitations on assessing severity, such as being subjective, non-linear, coarse, and easily confounded by other physical disabilities, DTI offers the distinct advantage of providing a direct measure of spinal cord tissue injury and has potential use in future guidelines to help more accurately quantify severity. However, the lack of significant correlation in other parameters like ADC and MD suggests a more complex interaction between DTI metrics and myelopathy, warranting a multifaceted approach in future studies.
An intriguing finding is the significant correlation between FA and RD, calculated at MC, with JOA/mJOA. While the number of studies investigating RD is still limited, the pooled results show FA’s significant correlation with symptom severity. The number of studies on ADC, the second most studied parameter, indicates it did not correlate with symptom severity. These findings are interesting because another recent systematic review and meta-analysis investigating the correlation between preoperative DTI parameters and decompressive surgery outcomes based on myelopathy severity like JOA/mJOA showed FA significantly correlated with outcomes in some age subgroups but not all. In contrast, ADC was correlated with surgery outcomes across different age groups and all age groups together. 10
The findings of this review, which investigates the correlation of DTI parameters with disease severity in patients who have not undergone surgery, and the previous review that examined the correlation between preoperative DTI parameters and decompressive surgery outcomes, shed light on the complex association between DTI metrics and myelopathy. 10 These findings suggest that FA might be a good indicator of symptom severity, but not necessarily of decompressive surgery outcomes. The complex association of FA with preoperative severity and decompression outcomes is also evident in studies included in this review that investigated the correlation of DTI parameters in both preoperative and postoperative periods.33,35,40,47,50,53,55,56,59,61,65,66 Most of these studies focus primarily on FA and reveal complex results. They mostly show that FA can be correlated with preoperative disease severity, but not all studies were able to demonstrate a correlation between FA and postoperative disease severity or recovery rate.47,53,55,59,65 This again suggests that while FA may be better used for assessing disease severity, it may not always be a reliable indicator of decompression outcomes.
Conversely, ADC seems to correlate with decompressive surgery outcomes but not preoperative symptom severity. From a surgical standpoint, these findings are significant. They suggest that patients with higher FA might have more severe myelopathy symptoms, but it’s unclear if the severity improves post-surgery. For predicting improvement after surgery, ADC might be a more reliable DTI parameter. Not only does it show no uniform correlation with symptom severity, but other systematic reviews also indicate its correlation with postoperative outcomes in DCM patients. 10
The findings of this systematic review on preoperative symptom severity and DTI, coupled with the recent study on postoperative outcomes and DTI in DCM patients, 10 could significantly impact patient selection for decompressive surgery. Current guidelines for DCM suggest decompressive surgery for both moderate and severe cases. 68 However, there is a lack of precise recommendations for mild DCM ranging from non-operative treatment such as physical therapy to immediate surgery. ADC’s role here could be pivotal, potentially differentiating between healthy and DCM patients. While it may not correlate with symptom severity, it might predict surgical outcomes, making it a valuable imaging biomarker for future management decisions in mild DCM.
Limitations
This review, while comprehensive, does highlight several significant research gaps and limitations that must be acknowledged. Firstly, the prevalent risk of bias, especially in patient selection and the absence of uniform diagnostic thresholds, is a critical concern that requires immediate attention in future research endeavors. The small sample sizes and the geographical concentration of studies, primarily in Asia, potentially limit the broader applicability and generalizability of our findings.
Additionally, a notable limitation of this study is the pooling of the diagnostic ability of DTI parameters across the entire myelopathy severity spectrum. This approach raises questions about the specificity of DTI parameters in differentiating between healthy individuals and patients with mild DCM. The ability of DTI to distinguish between these 2 groups is crucial, as it directly impacts clinical decision-making, particularly in the early stages of the disease. Therefore, further investigation is needed to determine whether DTI parameters can effectively differentiate between healthy and mild DCM cases.
Furthermore, the variability in measuring DTI parameters across different cervical spine levels poses a significant challenge. This inconsistency hampers the development of a standardized diagnostic approach and complicates the interpretation of results across studies.
Future Directions
Addressing these limitations is imperative in future research. Future studies should aim for larger, more diverse cohorts with harmonized DTI measurement protocols, enhancing the generalizability and applicability of DTI in diagnosing and monitoring DCM. Establishing clear, evidence-based diagnostic cut-offs will be crucial for improving diagnostic accuracy and reliability. Additionally, further research should focus on the specific diagnostic capabilities of DTI parameters in differentiating mild DCM from healthy states. Integrating advanced data analysis techniques, such as machine learning, could provide significant insights and refine the diagnostic capabilities of DTI.
Conclusion
In conclusion, while this systematic review and meta-analysis provide valuable insights into the utility of DTI in DCM, the highlighted limitations underscore the need for continued and focused research to fully understand and leverage DTI’s potential in clinical practice, particularly in early-stage DCM diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.