
Abstract
Study Design
An e-mail-based online survey for adult spinal deformity (ASD) surgeons.
Objective
Wound closure and dressing techniques may vary according to the discretion of the surgeon as well as geographical location. However, there are no reports on most common methods. The purpose of this study is to clarify the consensus.
Methods
An online survey was distributed via email to AO Spine members. Responses from 164 ASD surgeons were surveyed. The regions were divided into 5 regions: Europe and South Africa (ESA), North America (NA), Asia Pacific (AP), Latin America (LA), and Middle East and North Africa (MENA). Wound closure methods were evaluated by glue(G), staples(S), external non-absorbable sutures (ENS), tapes(T), and only subcuticular absorbable suture (SAS). Wound Dressings consisted of dry dressing (D), plastic occlusive dressing (PO), G, Dermabond Prineo (DP).
Results
The number of respondents were 57 in ESA, 33 in NA, 36 in AP, 22 in LA, and 16 in MENA. S (36.4%) was the most used wound closure method. This was followed by ENS (26.2%), SAS (14.4%), G (11.8%), and T (11.3%). S use was highest in ESA (44.3%), NA (28.6%), AP (31.7%), and MENA (58.8%). D was used by 50% of surgeons postoperatively. AP were most likely to use PO (36%). 21% of NA used DP, while between 0%-9% of surgeons used it in the rest of the world.
Conclusion
Wound closure and dressings methods differ in the region. There are no current guidelines with these choices. Future studies should seek to standardize these choices.
Introduction
Surgical site infections are a common and morbid complication in adult spinal deformity surgery. Infection rates remain over 3%–10% and are doubly higher in obese patients.1-3 Non-infectious wound complications are uncommon, including wound dehiscence, with rate of .5%. 4 On the other hand, it is high incidence in ASD patients with complex wound closures (23%). 5
There are many methods of wound closure and wound dressing, but there is a lack of evidence for them in the field of spine surgery. 6 Typical methods of wound closure include 2-octyl-cyanoacrylate (Glue), staples, sutures (subcuticular and external nylon skin sutures), tapes, etc. Closure methods can be compared in terms of surgical time and effect on surgical site infections (SSI). Staples can reduce surgical time as compared to sutures. 7 On the other hand, compared to staples, total wound closure using sutures demonstrates a reduced incidence of SSI and superior cosmetic outcomes in terms of scarring.8,9 Shani et al. 10 reported a higher infection rate of for staples (11.8%) in a study of posterior spinal surgery as compared to external nylon sutures (4.2%). However, one report indicates no difference in infection rates between staples and nylon sutures. 11 Glue also has the advantage of not requiring removal of stitches, wound dressing and to resist contact with water. 7 Moreover, glue has also been shown to have a much lower infection rate (0%–.43%) in reports comparing it to staples.12,13
Another possible intervention to prevent wound complications is type of dressing. In a Cochrane review for all types of clean surgery, the authors concluded that there is no particular wound dressing that may decrease SSI, although there is very low certainty evidence supporting hydrocolloid and silver-containing dressings . 14 In a network review in total joint arthroplasty, silver-containing, alginate and hydrofiber dressings were found to significantly decrease wound infections as compared to gauze. 15
There are no reports with a high level of evidence regarding the choice of wound closure or wound dressing in the spine surgery, and these are often left to the discretion of the surgeon. Few reports have investigated which methods are commonly chosen in the world, and perhaps this may vary by region and social context. The purpose of this study was to confirm expert consensus by emailing AO spine members around the world and asking questions about wound closure and wound dressing.
Material and Methods
A peri-operative spine survey was formulated by a study group within AO Spine. The study group included experts in the knowledge forum (KF) degenerative and KF deformity spine. The questionnaire included demographic information on participants and was designed to cover various aspects of peri-operative care such as wound management, antibiotics, bracing and activity instructions. An online survey was distributed via email to AO Spine users and members between March 3 and March 22, 2022. The survey was targeted at surgeons performing at least 10 cases per year using one or more of the following procedures: a) Long fusion (>5 levels) for adult spine deformity patients extending to pelvis b) Long fusion (>5 levels) for adult spine deformity patients NOT extending to pelvis c) Open 1 or 2 level fusion for adult lumbar degenerative pathologies d) MIS 1 or 2 level fusion for adult lumbar degenerative pathologies e) Open 3 to 5 level fusion for adult lumbar degenerative pathologies
It was estimated that over 6000 surgeons that were AO Spine users and members received the email. Among all those who received the email, 354 responded and 280 completed the survey. Of the surgeons who completed the survey, 164 performed adult spine deformity surgeries (procedures a and/or b) and 261 performed adult spinal degenerative surgeries (procedures c, d and/or e).
This study included 164 adult spinal deformity surgeons from 51 countries. The country of residence was divided into regions as follows: Europe and South Africa (ESA), North America (NA), Asia Pacific (AP), Latin America (LA), and Middle East and North Africa (MENA). Options for wound closure were glue, staples, external non-absorbable suture (ENS), tapes, or only subcuticular absorbable suture (SAS). In addition, the question items regarding fascial suture are the type of suture (absorbable braided suture, non-absorbable braided suture, absorbable, monofilament suture, or non-absorbable monofilament suture), whether to perform muscular layer approximation, suture method (continuous suture, interrupted suture, or both). For wound dressing, selection of postoperative dressing (dry dressing [D], plastic occlusive dressing [PO], G, incisional wound vacuum [IWV], or Aquacel Ag [AA]), timing of initial removal of dressing, and dressing after removal.
Literature Review
We conducted literature review to identify relevant articles on wound closure and wound dressings in spine surgery. We consulted PubMed. The search strategy was as follows; “skin closure” [All Fields] OR “wound closure” [All Fields] OR “wound suture” [All Fields] AND “spine surgery” [All Fields] in wound closure. On the other hand, the search strategy in wound dressings was constructed after discussion and consensus of all authors and included these terms: “wound care” [All Fields] AND “spine surgery” [All Fields] AND “dressing” [All Fields]. Two authors (GS, MG) independently inspected the bibliographic quotes and identified relevant abstracts. The full-text article was analyzed for included studies. References from the selected articles were also reviewed and added through cross reference if appropriate.
Then, eligible articles were selected and reviewed.
Results
Wound Closure
Wound Closure.
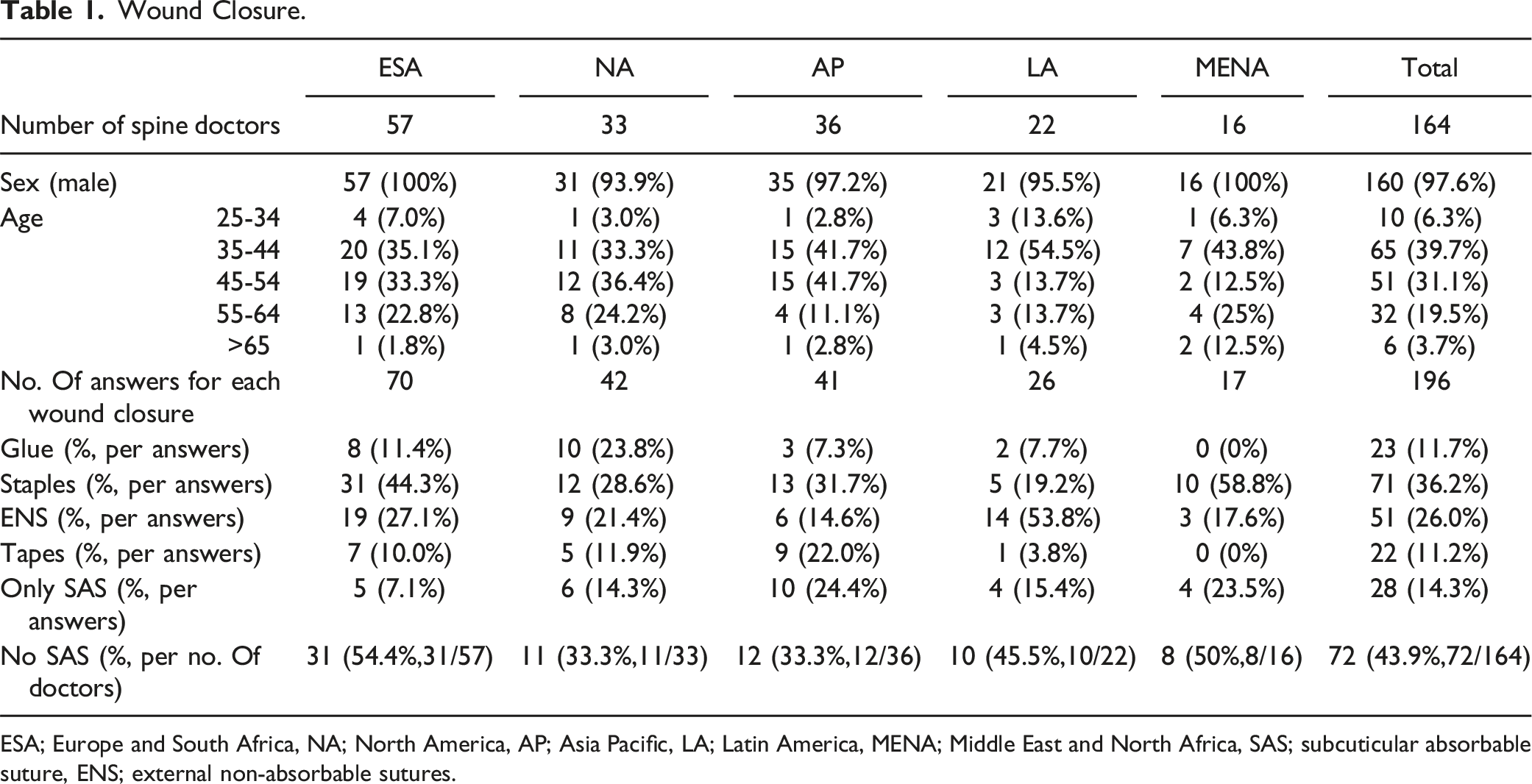
ESA; Europe and South Africa, NA; North America, AP; Asia Pacific, LA; Latin America, MENA; Middle East and North Africa, SAS; subcuticular absorbable suture, ENS; external non-absorbable sutures.
Multiple responses are possible, so the number of responses by region for wound closure was 70 in ESA, 42 in NA, 41 in AP, 26 in LA, and 17 in MENA. Staples were the most common wound closure globally (36.2%), followed by ENS (26%), Only SAS (14.3%), glue (11.7%), and finally tapes (11.2%). By region, the usage rate of staples was the highest in ESA (44.3%), NA (28.6%), AP (31.7%), and MENA (58.8%), but ENS was the most common wound closure in LA (53.8%). Glue use was low in most regions, but NA had the second highest use (23.8%). Furthermore, less than half (43.9%) of all surgeons responded that they would not perform SAS for wound closure. It was especially low at 33.3% for NA and AP.
Fascia Closure.
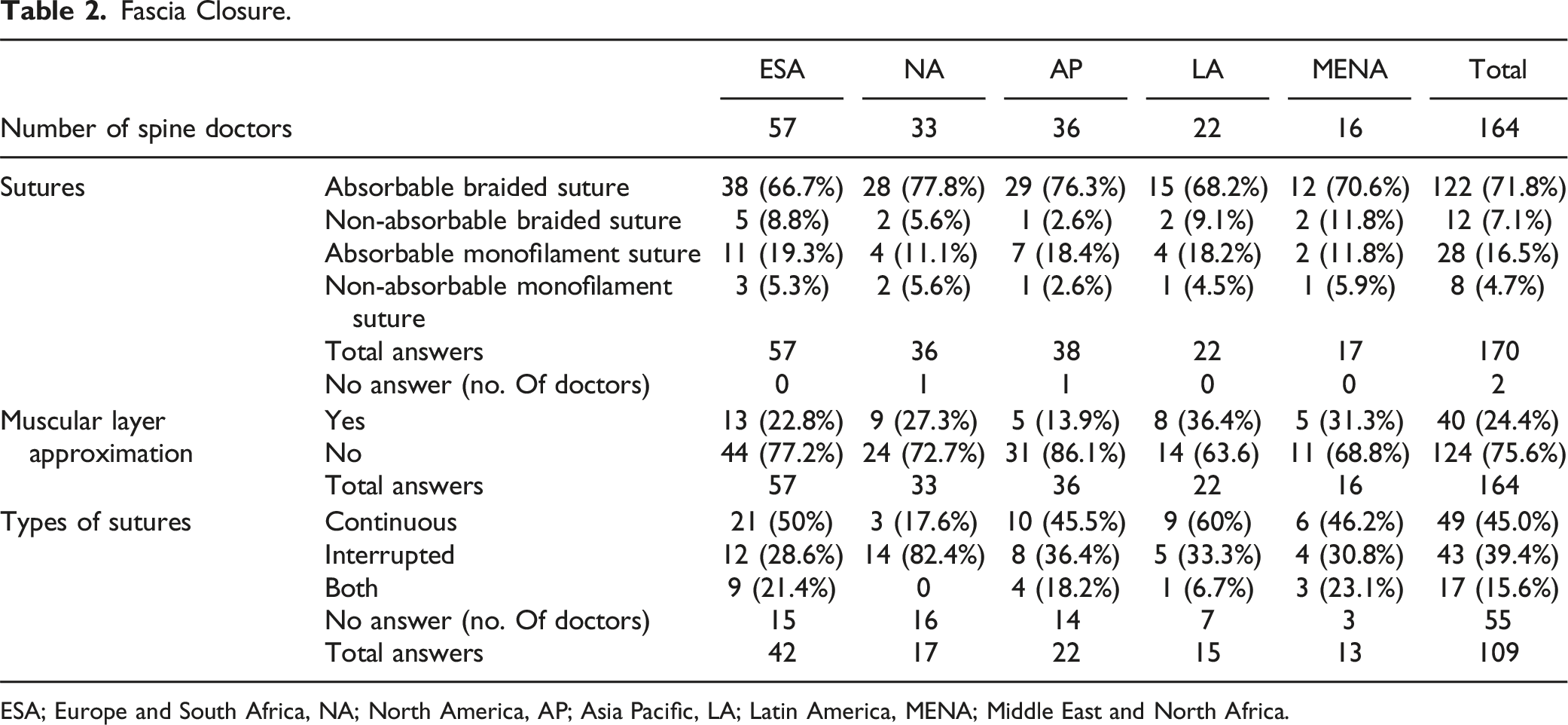
ESA; Europe and South Africa, NA; North America, AP; Asia Pacific, LA; Latin America, MENA; Middle East and North Africa.
Continuous suturing technique was slightly more popular than interrupted suture (45.0% vs 39.4%). ESA, AP, LA, and MENA tended to have more continuous sutures, while NA had the overwhelming majority of interrupted sutures (82.4% vs 17.6%).
Literature for Wound Closure
Literature Review.
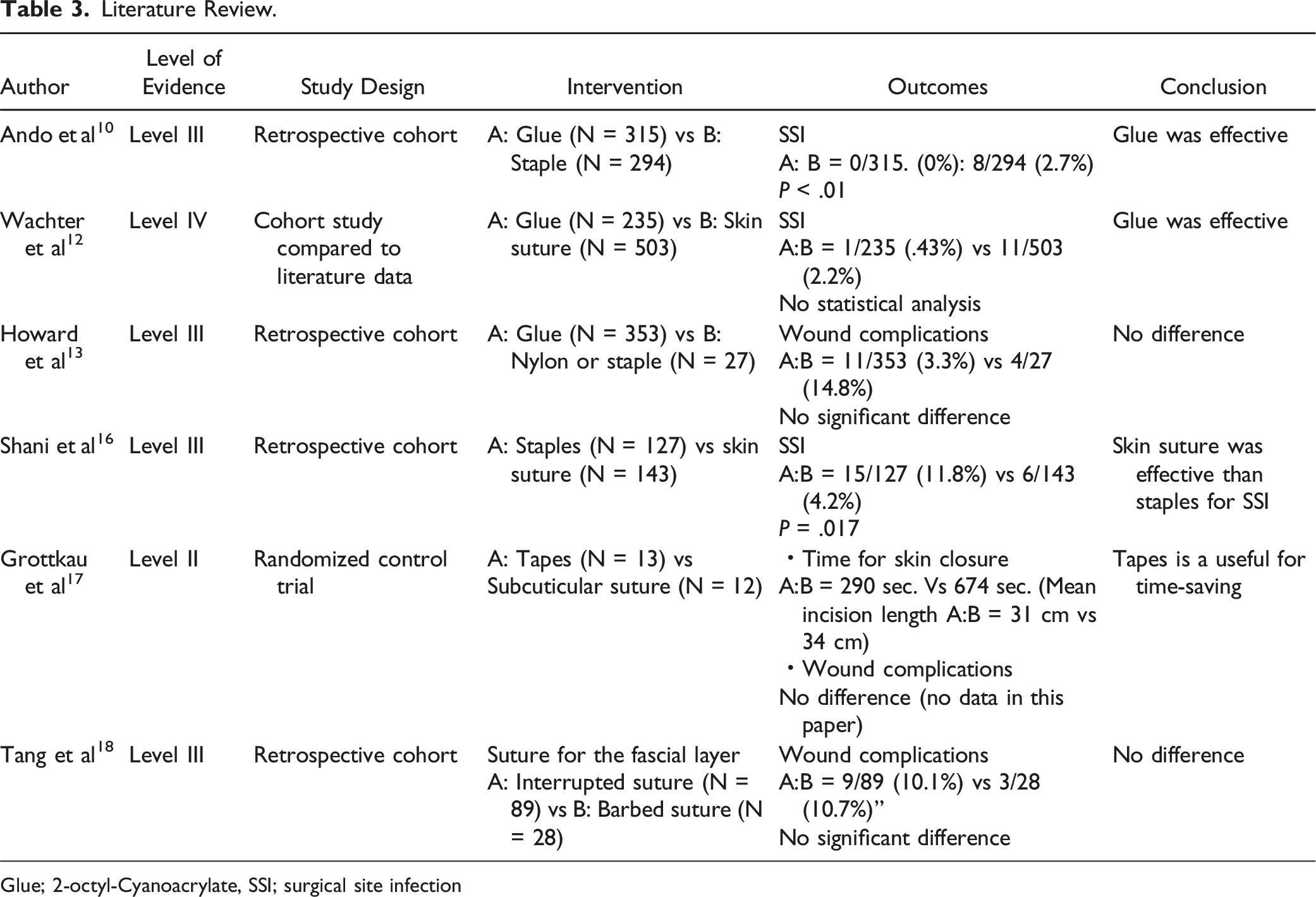
Glue; 2-octyl-Cyanoacrylate, SSI; surgical site infection
Dressings Survey Results
Initial Wound Dressing After Surgery.
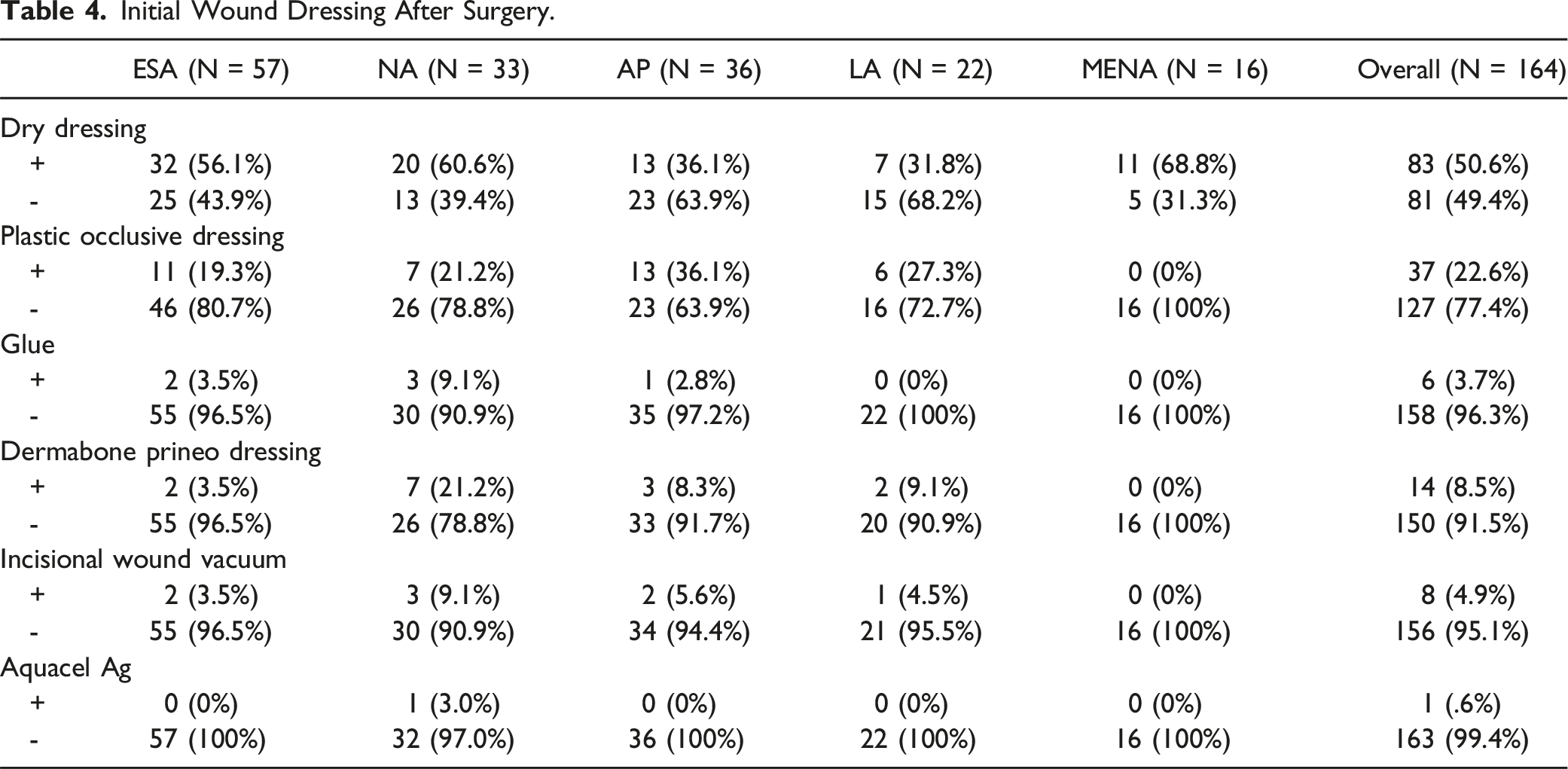
Other closure techniques were sparingly used. Glue was used by only 4% of surgeons. Dermabond Prineo dressings were used in NA, LA, and AP (21%, 9% and 8% respectively), but sparingly used in ESA and MENA. Similarly, incisional wound vacuum saw 9% NA use, 6% AP use and 5% LA use, but very little use in ESA and MENA. Only one NA surgeon used AA dressings.
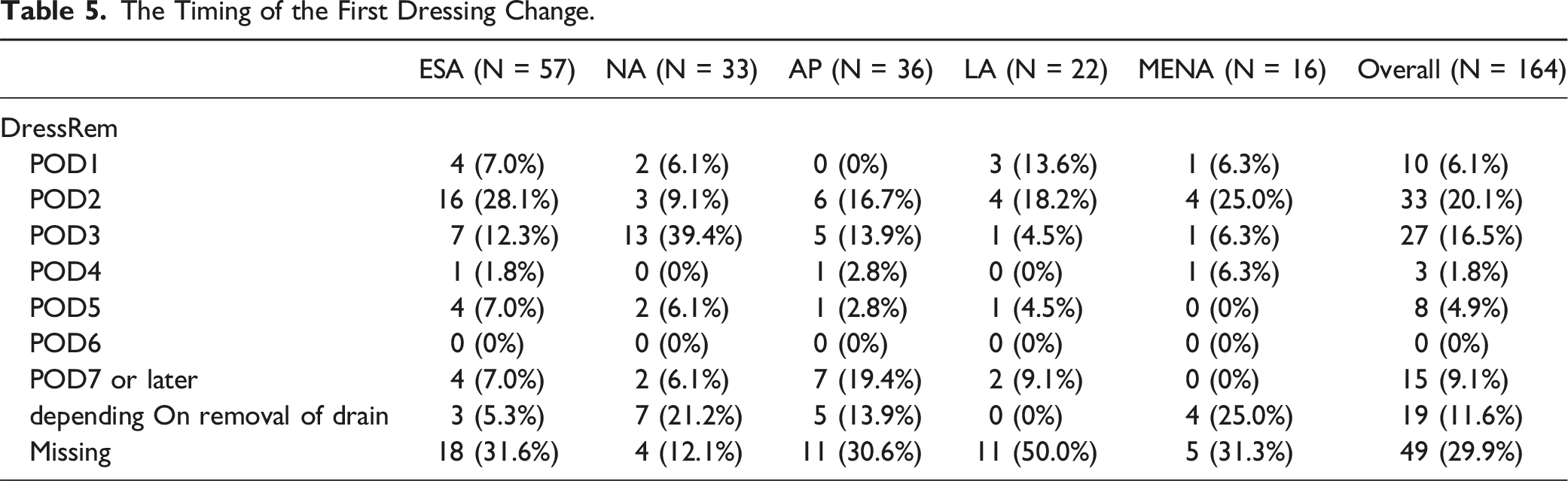
The Timing of the First Dressing Change.
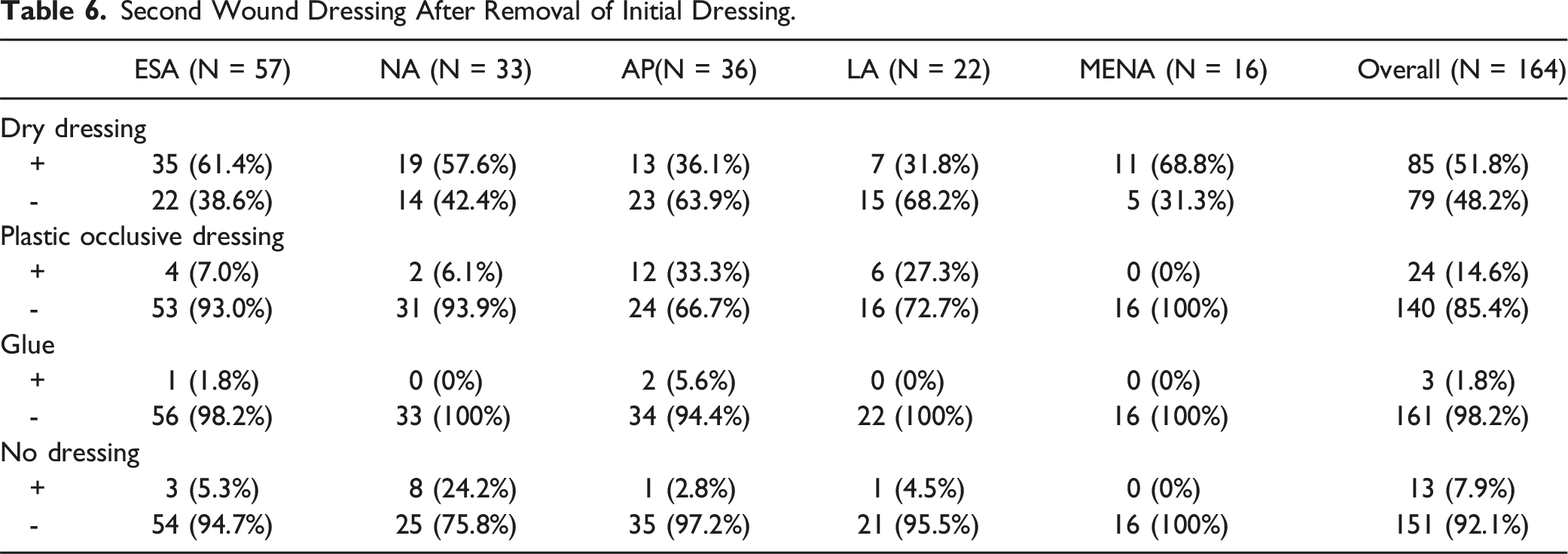
Second Wound Dressing After Removal of Initial Dressing.
Wound Care and Dressings Literature Review
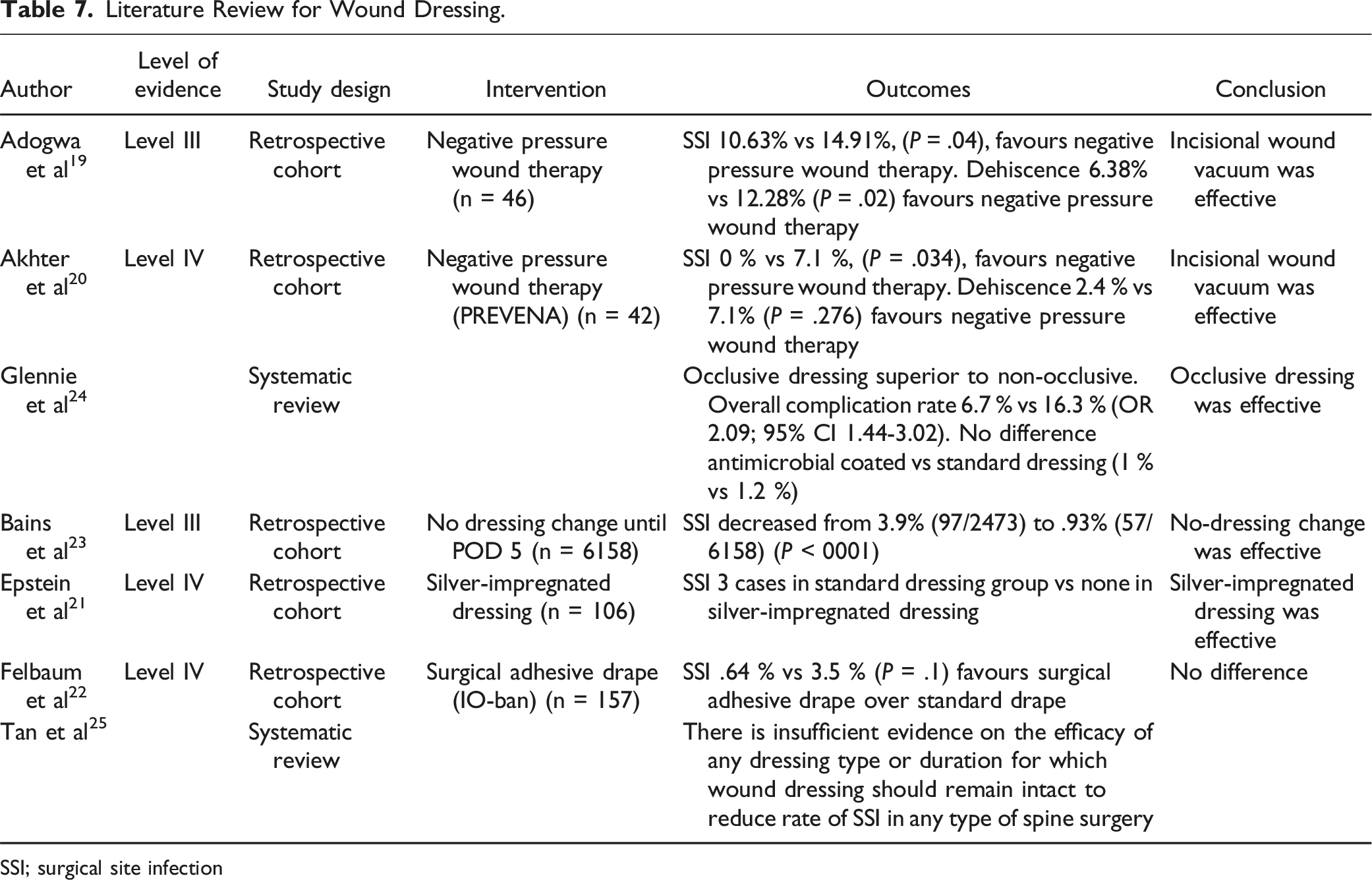
Literature Review for Wound Dressing.
SSI; surgical site infection
All papers were Level 3 or 4 evidence. There is some support for IWC being effective in ASD surgery for SSI19,20 and for dehiscence. 19 There is also some low-level evidence supporting silver-impregnated antimicrobial dressings, 21 antimicrobial film. 22 and in a no-dressing-change protocol. 23 in spine surgery, but these are not specific to ASD.
A systematic review on wound dressings in spine surgery (not specific to ASD) suggested that occlusive dressings are superior to non-occlusive. 24 In contrast, another systematic review suggested no conclusive evidence on the efficacy of any suture or dressing type. 25
Discussion
Surgeons have many choices in wound closure and dressings in ASD, but the choices have not yet been clarified. In other surgical domains, there is much interest and uncertain literature regarding choice of wound closure and impact wound infection and drainage rates.14,26,27 While the rate of ASD surgery wound complications are high, there is little literature to guide our choices. In this investigation, we document geographical variations in wound closure and dressing techniques.
Although the literature review did not find studies with a high level of evidence for wound closure, the results in Table 3 suggest that Glue may be more effective in preventing SSI than other wound closures. However, staples were the most frequently used wound closure in all regions except for LA (Table 1). This may be due to cost performance and perceived ease of use. Considered further, the cost and time required to close a 10 cm incision are US$25 for 20 s with glue, and US$38.5 for 48 s with staples, and thus glue may be superior in terms of cost performance. 13 Nonetheless, as shown in Table 1, Glue usage is low globally, except perhaps in NA. This may reflect the higher density of medical suppliers in NA, and thus newer medical supplies are more readily. The most prevalent wound closure in LA was ENS. In a survey similar to this study of neurosurgeons and orthopedic surgeons mainly in South America (mostly Mexico), 82% reported skin suture with nylon as their wound closure method, and the remaining 18% reported staples. 28
Table 2 describes the method used to suture the fascia, and absorbable sutures were overwhelmingly the most common type of suture throughout all regions. Of these, absorbable braided suture was selected by the majority of surgeons compared to absorbable monofilament suture. This may be due to the fact that many surgeons consider the difficulty of thread loosening to be more important for fascia sutures. Muscular layer approximation was also not performed by an average of 75.6% of surgeons across all regions, indicating that muscular layer approximation is not common across all regions.
In this study, in over 74% of surgeons, initial post-operative dressing choices were mostly dry dressings or plastic occlusive dressings (Table 4). In contrast, the use of glue or hydrofibre dressing (AA) were very limited. The Dermabond Prineo dressing, and the Incisional Vacuum dressing were used by 8.5% and 5% of world surgeons respectively, but with some important geographical variations, namely high use rates in NA (21% DP and 9% Incisional Vacuum). The most likely explanation for high NA use is cost, as surgical expenses in the US are generally higher than other jurisdictions. 29
New dressing technologies could improve wound healing performance. The Dermabond Prineo dressing consists of a self-adhesive mesh and traditional skin glue (2-octyl cyanoacrylate) (Ethicon, US). The purported advantages are to avoid intradermal sutures and decrease wound stress, avoid need for dressing changes, and that it forms an anti-microbial layer.30,31 There are few reports of DP use in spine surgery, and none in ASD. Stricker et al. 31 described successful use in 50 pediatric non-instrumented cases, including 45 intra-dural surgeries. They reported a very high satisfaction rate with respect to ease of use. However, while rare, allergic reactions to skin glue can occur in approximately .5% to 2% of cases. 32 and can lead to reoperations. While the effect of DP dressing on wound complications may be decreased drainage and less operating time,33,34 it is expensive as compared to DD or PO dressings.
Incisional vacuum dressings in spine have been used in the management of known surgical site infections, 35 but there is little evidence when used at the index surgical closure to prevent infection (Table 7). Adogwa et al. 19 analyzed the effect of incisional wound vacuum on wound infection and dehiscence rates in ASD surgery. A significant decrease in the incidence of wound dehiscence (6.4% vs 12.3%, P = .02) and postoperative surgical site infection (10.6% vs 14.9%, P = .04) was observed in the IWV patient cohort. The authors concluded that this therapy was related to reduced wound complications in patients undergoing deformity surgery. Dyck et al. 36 in a small series, have also reported that prophylactic use of IWV in high-risk spine wounds can decrease SSI.
The timing and type of second dressings after ASD surgery was also quite heterogeneous. Despite some evidence supporting minimizing dressing changes in spine surgery, 23 most surgeons changed the dressings by POD3.
Conclusions
A survey of surgeons performing ASD surgery revealed that although stales are common for wound closures and dry dressing is common for wound dressings, there is some regional variation in the choice. However, there are no current guidelines to help surgeons with these choices, and these data are not informative. Given high rates of wound complications in ASD surgery, there is an opportunity for high-quality trials to determine if wound closure and dressing choices can decrease complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.