
Abstract
Study Design
Systematic review and meta-analysis.
Objectives
The need for definitive fusion for growing rod graduates is a controversial topic in the management of Early-onset scoliosis (EOS) patients. The authors performed a systematic review and meta-analysis on the available literature to evaluate the outcomes of growing rod graduates undergoing final fusion or observation with implants in-situ.
Methods
An extensive literature search was carried out aimed at identifying articles reporting outcomes in growing rod graduates. Apart from the study characteristics and demographic details, the extracted data included Cobb’s correction, trunk height parameters, and revision rate. The extracted data was analyzed and forest plots were generated to draw comparisons between the observation and fusion groups.
Results
Of the 11 included studies, 6 were case-control and 5 were case series. The authors did not find any significant difference between the 2 groups with respect to the pre-index and final Cobb’s correction, T1-T12 or T1-S1 height gain in either over-all, or sub-analysis with case-control studies. The meta-analysis showed a significantly higher revision rate in patients undergoing a definitive fusion procedure.
Conclusion
The current analysis revealed comparable outcomes in terms of correction rate and gain in the trunk height but a lesser need of revisions in observation sub-group. The lack of good quality evidence and the need for prospective and randomized trials was also propounded by this review.
Introduction
Early-Onset Scoliosis (EOS) presents as a challenging entity for any spine surgeon to manage. Apart from ensuring adequate trunk growth, due emphasis should be given to maintaining proper alignment, balance and keeping the deformity from progressing. Distraction-based modalities such as traditional growing rods or magnetically controlled growing rods are the most widely accepted treatment modalities worldwide. These implants assume the role of an internal brace to prevent the progression of the deformity while maintaining balance and allowing trunk growth at the same time.1,2 Both the implants need to be anchored to the proximal and distal fixation points usually constituted by 2 vertebrae cranially between T2 to T4 and 2 vertebrae caudally, usually the stable or the last touch vertebra.3-6 Sub-periosteal dissection is avoided in the segments lying in between the cranial and caudal fixation points to maintain the growth potential in these segments and periodic distractions achieve the necessary lengthening of the trunk.
Growing rod “graduates” are defined as the patients who have completed their growing rod treatment. 7 Despite years of literature available on growing rods, graduation protocol for these patients is still controversial. The 3 options available for these patients include 1.) undergoing final-fusion, 2.) observation while maintaining the implants in their position, and 3.) removing the implants. 8 The available literature has a considerable lacuna in good quality evidence for the appropriate management of these patients. The authors performed a systematic review and meta-analysis of the available literature to evaluate the outcomes of growing rod graduates undergoing final fusion or observation with implants in-situ.
The authors sought the answers of the following questions from this review—1) Is observation with implants in-situ an effective alternative to definitive fusion in terms of cobb’s correction and gain in trunk height after graduation of growing rods? 2) Is observation a safer alternative to definitive fusion in terms of revision surgeries in graduates? Removal of implants with an acceptable alignment is an alternative strategy, however its discussion in literature is limited to just 1 article with poor results and subsequently has not been investigated as a part of this meta-analysis.8,9 We have included all available researches in the last 2 decades, and have followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to help improve the reporting quality of our study. For the purpose of simplicity, both the traditional and magnetic growing rods have been termed as “growing rods” in this article.
Methods
Literature Search
An extensive electronic and manual literature search was performed using PubMed, EMBASE, and Google Scholar databases by 2 independent reviewers. The search was aimed at identifying articles reporting outcomes in EOS with growing rod implants undergoing final fusion or observation after graduation published in the last 10 years. Medical subject heading (MeSH) terms used included “scoliosis/classification” and “scoliosis/treatment” while non-MeSH search terms used included “early-onset scoliosis,” “growing rod,” “graduation,” and “final fusion.” Additionally, references of the included citations were cross checked manually to include any additional articles. The authors eliminated the duplicated citations first using Zotero’s de-duplication function after merging all the references followed by manual elimination.
Study Selection
The inclusion criteria for the articles were laid down following the PICOS format. Participant—studies describing the outcomes of EOS patients with growing rod (traditional or magnetic) in-situ after graduation, Intervention—observation in graduated patients, Control—final fusion in graduated patients, Outcomes—reporting of safety and efficacy in terms of deformity correction and complication rate, Study design—all studies except case reports, or case series with a sample size of less than 4 were included. Studies reporting outcomes in languages other than English were excluded. Any disagreements between the authors were resolved by means of discussion to reach a consensus.
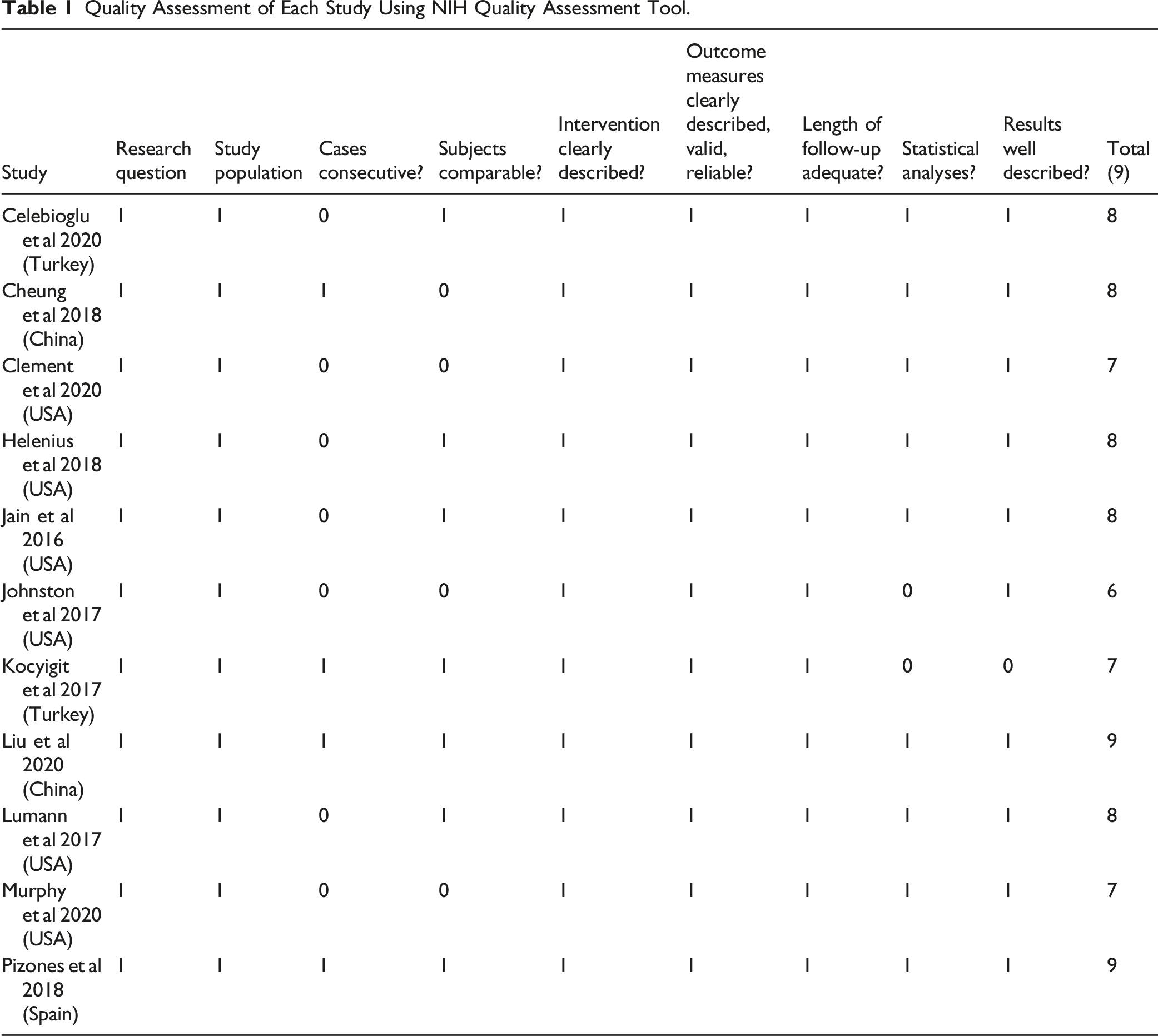
Quality Assessment
Quality Assessment of Each Study Using NIH Quality Assessment Tool.
Data Extraction
Data extraction was done from the included citations by the first 2 authors. The extracted data included the study characteristics, demographic data, and primary and secondary outcome variables. The study characteristics included the name of the first author, title, journal, year of publication, study design, level of evidence, and quality of the study. The extracted demographic information included the number of patients, mean age information on surgical constructs and the type of scoliosis (idiopathic, congenital, neuromuscular, or syndromic). The measured variables included pre-index and final Cobbs, Cobb’s correction, T1-T12, and T1-S1 height gain at the time of final follow-up, mean number of lengthening surgeries, mean follow-up duration and incidence of re-surgeries due to various complications in the follow-up period post-graduation. Once the data was extracted, the studies were classified into 2 groups for analysis—(1) undergoing final fusion after graduation and (2) undergoing observation with implants in-situ after graduation. Further, attempts were made to contact the investigators to obtain detailed data sheets if data was incomplete or unclear.
Statistical Analysis
Descriptive analysis using means, standard deviation (SD), and ranges (minimum, maximum) of the pooled data across the included studies were performed. Meta-analysis was performed using the Metafor package in R statistical software v4.0.0 (R Core Team, Vienna, 2020). Analysis was performed using a random-effects model using the DerSemonian Laird method. Forest plots were generated in order to draw comparisons between the 2 groups (Fusion and observation). Subsequently sub-group analysis was done by including only the case-control studies comparing fusion and observation. Weighted mean difference (WMD) and relative risk (RR) were used for analyzing continuous and categorical or binary data respectively. A P-value of less than .05 was considered significant, whereas any overlap within the 95% CI or P-value more than .05 was considered insignificant.
Results
The PRISMA flowchart of study selection is shown in Figure 1. After excluding duplicated and irrelevant articles from various databases, 369 articles were included for review. After reviewing abstracts, 32 articles were shortlisted for full-text review based on the pre-decided inclusion and exclusion criteria. After reviewing complete texts, 21 articles were excluded because of inadequate sample size or data, describing implant removal at graduation, publication in language other than English and inadequate data in the study. Subsequently, 11 studies were included for data extraction and final analysis (Table 2) Depiction of study format according to preferred reporting items for systematic reviews and meta-analysis format. Demographic Details of Included Studies.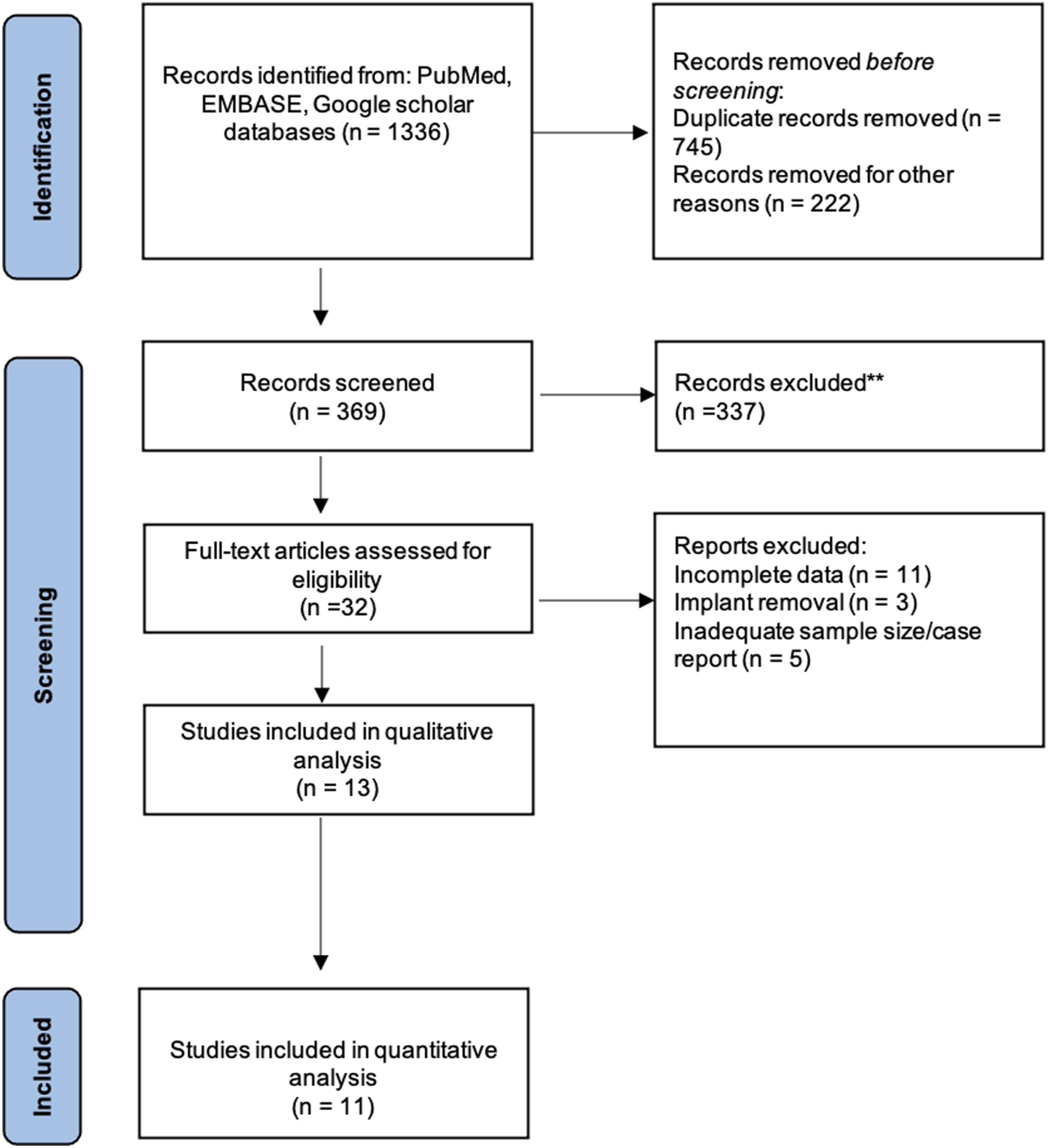
Study Characteristics
Of the 11 included studies, 5 were found to be case series11-15 (level IV evidence) whereas 6 were case-control studies8,16-20 (level III evidence). No RCTs were found in the literature. All 5 case series described the outcomes of final fusion after graduation. Of the included studies, 10 described the outcomes with traditional while 1 described the outcomes with magnetic growth rods. 13 All the studies were found to have a quality score of 6 or above out of 9 and were subsequently included in analysis(Table 1).
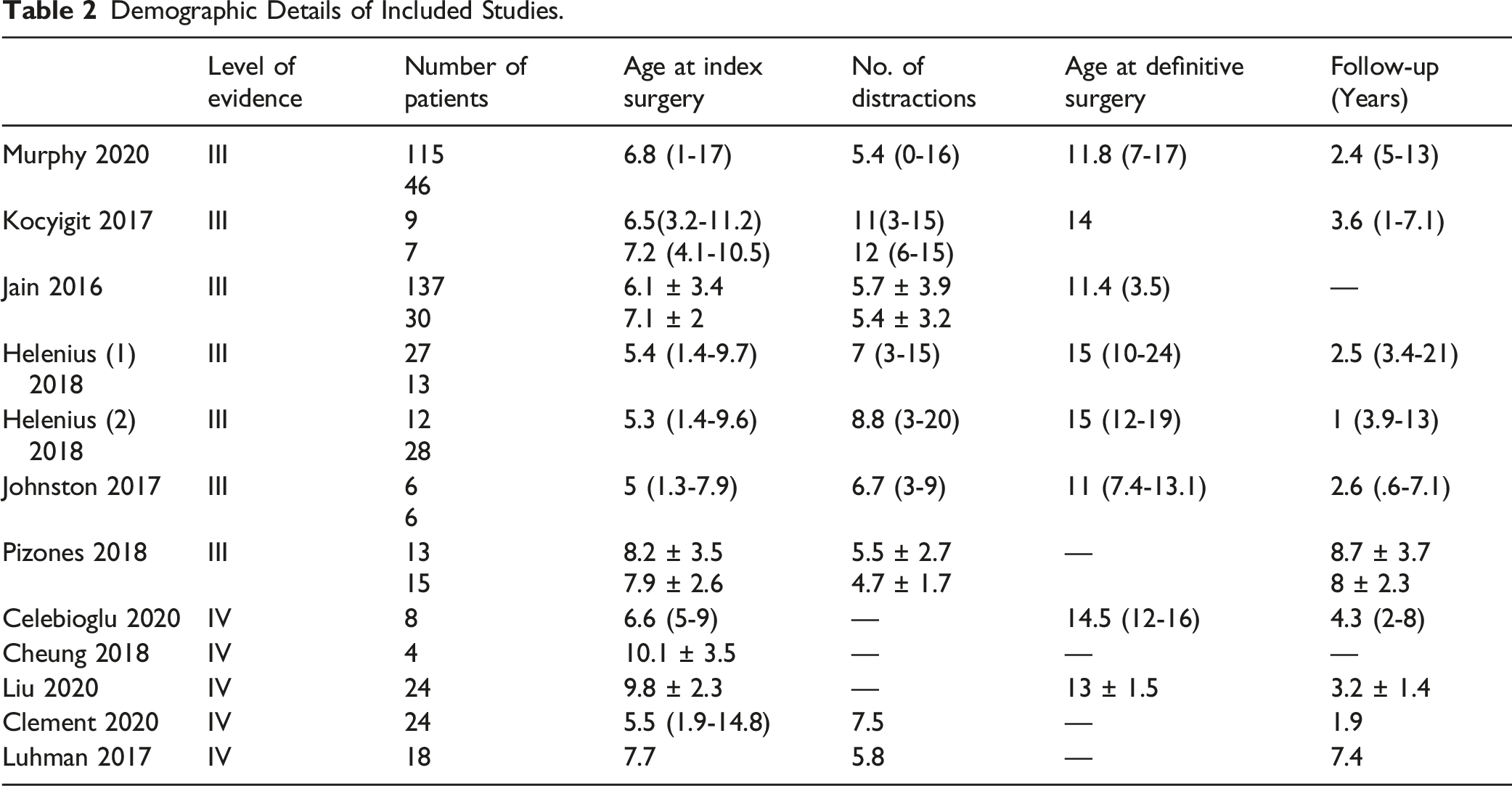
Demographic Data
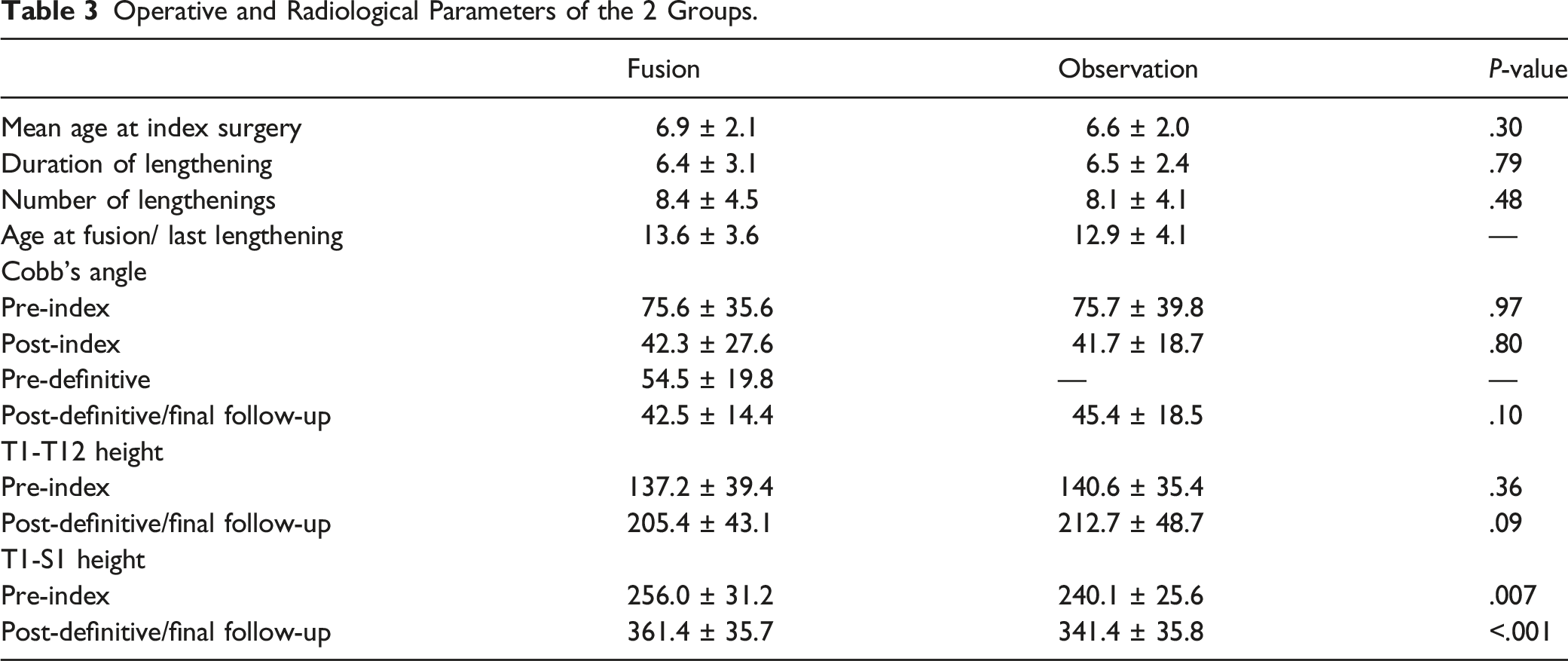
Operative and Radiological Parameters of the 2 Groups.
All the mean values described are in effect the pooled means and standard deviations of all the included studies in 1 group. Neuro-muscular was found to be the commonest etiological diagnosis in 11 of the 12 included studies which described the etiology of EOS (Figure 2). Etiology wise distribution of the included patients in all the studies.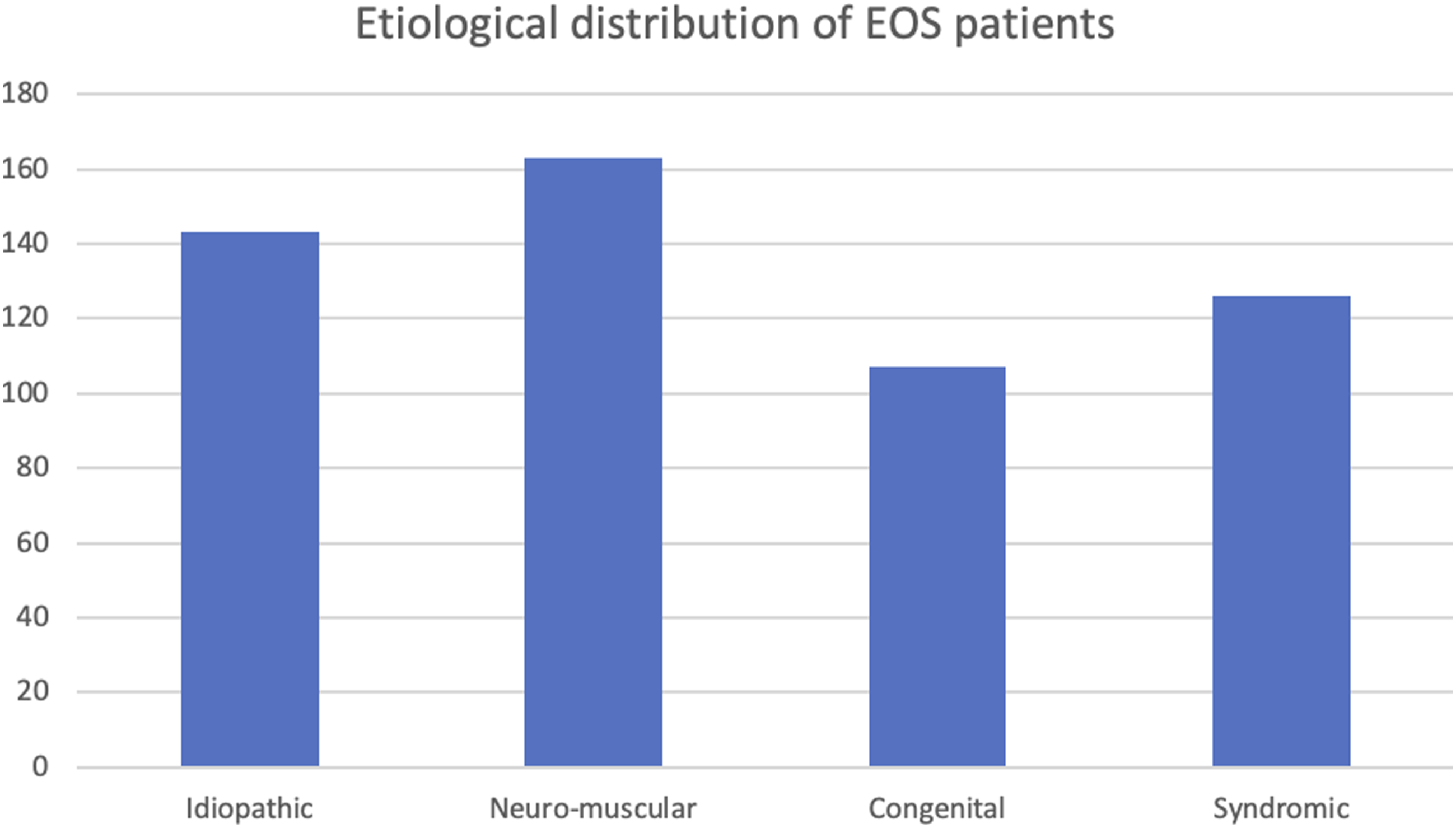
Cobb’s Correction Rate
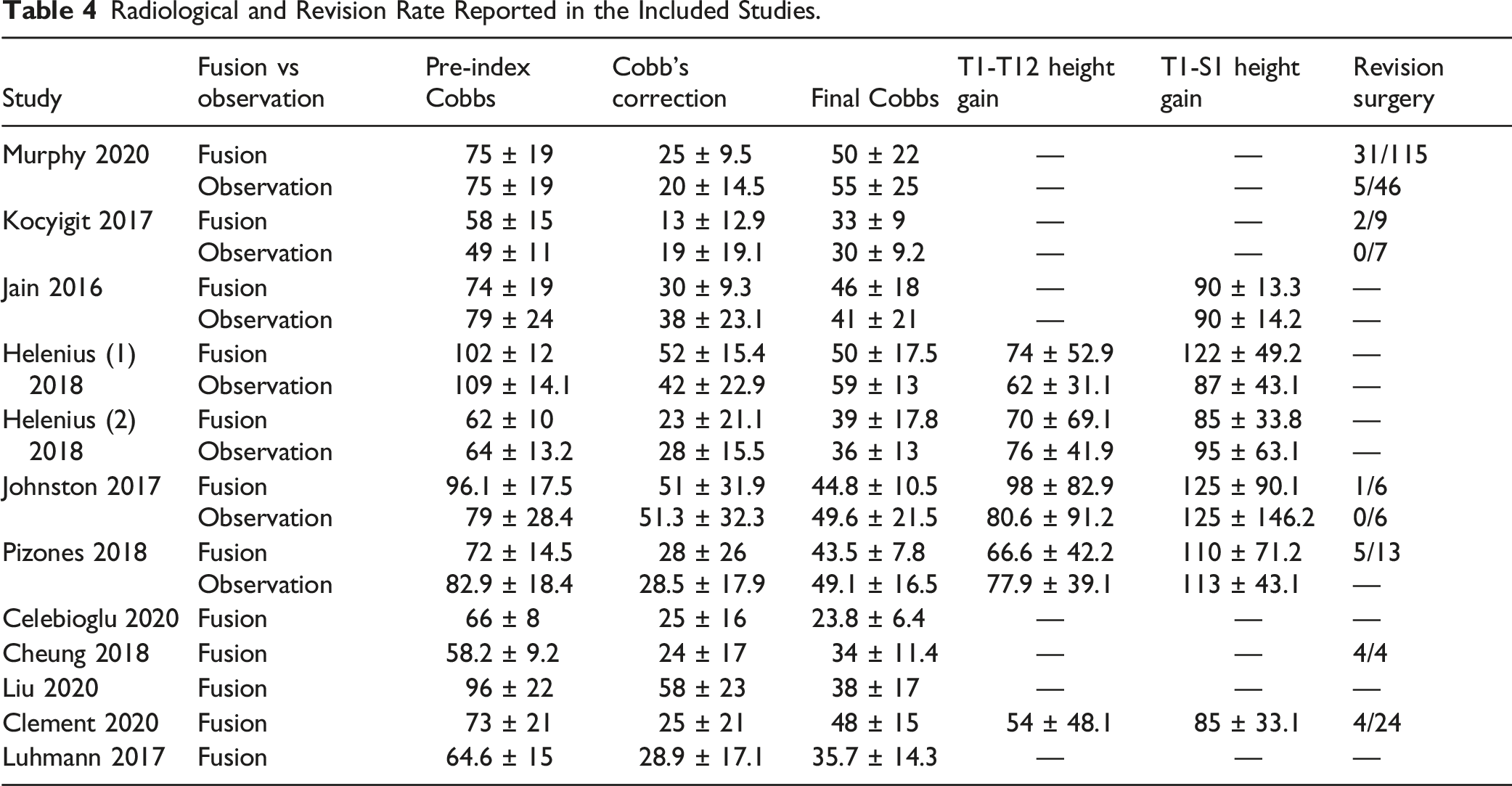
Radiological and Revision Rate Reported in the Included Studies.
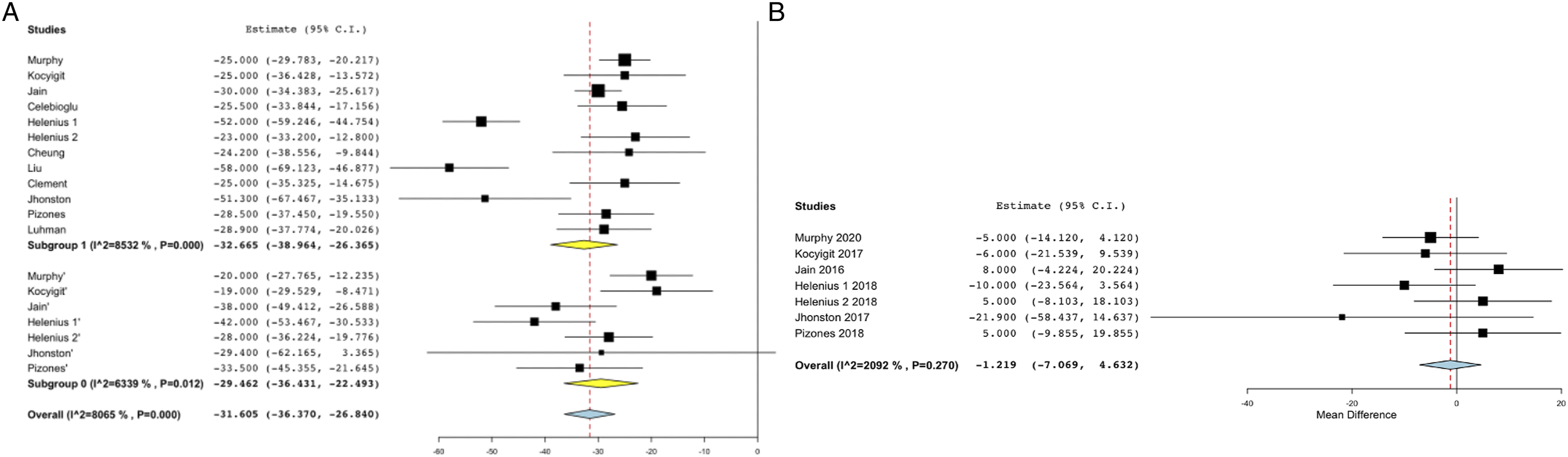
A–B. Forest plots showing Cobb’s correction between pre-index and final follow-up in A. over-all analysis B. analysis including only case-control studies.
T1-T12 and T1-S1 height gain
Pre-index and final T1-T12 height was reported in 5 studies and the difference between the 2 was used for analysis. There was no significant difference found T1-T12 height gain between the 2 groups either on over-all analysis(MD 67.97; 95% CI - 55.844, 79.75 vs MD 70.67; 95% CI – 60.47,80.86) or on sub-group analysis including only case-control studies (WMD = −.384; 95% CI -18.5, 17.7; P – .96) (Table 3 and 4; Figure 4A-B) A–B. Forest plots showing T1-T12 height gain in A. over-all analysis B. analysis including only case-control studies.
Similarly, no significant difference was observed in T1-S1 height gain in over-all analysis (MD = 98.29; 95%CI – 85.6, 110.9 vs MD = 97.93; 95% CI – 83.3, 112.5) or sub-analysis using case-control studies (WMD = 12.23; 95%CI -9.2, 33.8; p - .26). Reporting of both T1-T12 (I2 = 0%, P =.67) and T1-S1 height gain(I2 = 32.8%, P = .14) was found to be homogenous (I2 <50%, P > .05) (Table 3 and 4; Figure 5A-B). A–B. Forest plots showing T1-S1 height gain in A. over-all analysis B. analysis including only case-control studies.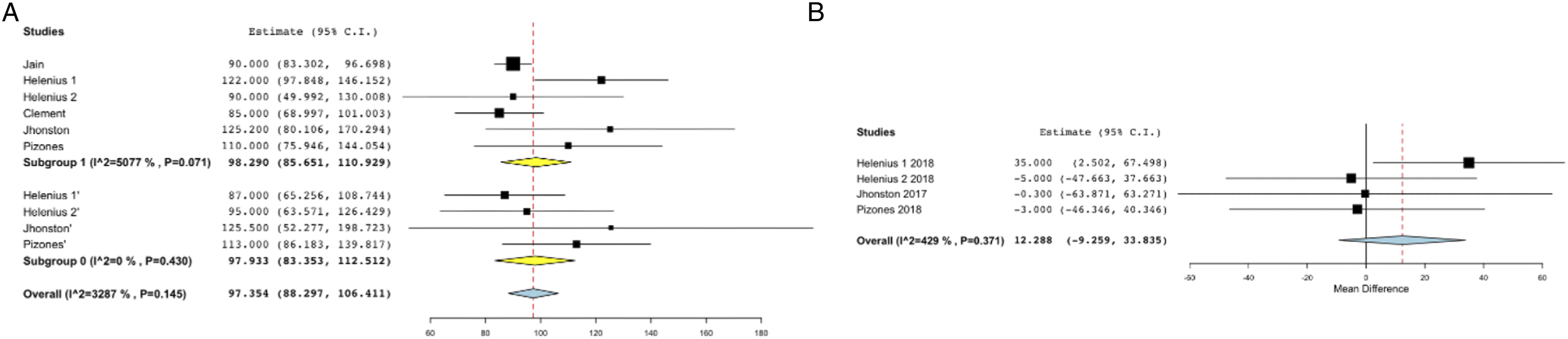
Revisions
Of the included articles, 6 described the complications after graduation. To exclude minor complications, the authors included complications requiring revision surgeries after definitive procedure or final distraction for analysis. Revisions in fusion group were found to be significantly higher than observation group (RR =.33; 95% CI – .17,0.49 vs RR =.09; 95% CI – .02,0.16). Sub-analysis including case-control studies yielded similar results (log RR = 3.19; 95% CI – 1.25, 8.10; P = .014). (Figure 6A-B). Proportional meta-analysis showing comparison of revision rates in A. over-all analysis B. analysis including only case-control studies.
Discussion
EOS is defined as onset of scoliosis before 10 years of age in a patient. Of the 3 techniques described earlier, traditional or magnetic growing rods are the most widely employed treatment strategy for EOS. At some point during the course of treatment, the patients attain skeletal maturity and are no longer candidates for distraction. Flynn has coined the term “graduates,” for such patients. He described the outcomes of series of patients who underwent definitive fusion after completion of the distraction treatment. 7 The management of these growing rod graduates is controversial and lacks good quality evidence presently.
The management of EOS is based on harnessing the growing forces of the immature spine. While braces in EOS apply corrective forces on the spine externally, growing rods apply these forces internally and guide the growth of the spine through regular distractions. Growing rods, like braces avoid long segment fusions and being closer to the spine are able to transmit stronger corrective and manipulative forces as compared to a brace. 8 Nevertheless, the similar mechanism of action of the 2 modalities has led to the theorization of implant removal or observation at graduation and avoidance of final fusion with a balanced spine and an acceptable deformity, a concept analogous to the brace discontinuation protocols after skeletal maturity. Kocyigit et al reported the outcomes of growing rod removal for the first time in a prospective study and concluded that implant removal is not a realistic strategy after graduation as they noticed worsening of deformity and a need for fusion in 9 out of 10 patients who underwent removal of their growing rods at graduation. 8 Due to the lack of adequate literature on implant removal, the authors included observation and final fusion on graduation as 2 groups for analysis.
Cobb’s angle of the curve is a direct marker for the extent of the deformity. Correction of the deformity was found to be maximum during the index surgery, that is, the implantation of growing rods. On performing meta-analysis with the Cobb’s correction between pre-index and final values, no significant difference was seen in over-all or sub-analysis using case-control studies. Additionally, at the final follow-up, the difference between the Cobb’s angles of the 2 groups was also not significant. One might expect a significantly lesser cobb’s angle in fusion group due to the application of several correction maneuvers, however, a possible explanation in this regard is that the curve correction obtained during definitive fusion was modest due to auto-fusion and spinal rigidity acquired by the spine during the distraction treatment21,22. Further, the pre-definitive Cobb’s in the fusion group was higher than the final Cobb’s in the observation group. The authors recognize this observation as a selection bias towards fusing the graduates with worse deformities as opposed to observing more modest curves. In summary, Cobb’s angle trend showed a significant correction after the index surgery followed by a steady increase over the distraction duration and a modest correction after the final fusion. A considerable amount of follow-up is important to compare the 2 treatment strategies. Breakage of implants and the worsening of the deformity are 2 theoretical concerns that arise with observation without final fusion. However, with a mean follow-up of 2.5 years after the last distraction, only 5 of the 59 patients in the observation group(3 articles in the observation group reported complications) were reported to have a revision surgery as opposed to 48 out of 186 patients in the final fusion group with a mean follow-up of 2.8 years. Sawyer et al reported a revision rate of 24% in the form of implant removal or re-revision predominantly due to hardware failure, infection or proximal junctional kyphosis 23 . Similar to their findings, Poe-Kochert et al reported a 20% rate of return to the operating room whereas Murphy et al reported a 22% revision rate in a follow-up period of 5 years16,24,25. We found a significantly higher risk of revision in fusion group as opposed to observation group. The higher risk of revisions in the fusion group could play an important role in deciding the course of action for growing rod graduates.
Thoracic spine has been defined as the posterior pillar of the thoracic cage 26 . Aberrations with the trunk height in the form of precocious arthrodesis or untreated EOS are often associated with short stature and respiratory insufficiency. Karol et al have reported a thoracic height of 18-22 cm is crucial to avoid respiratory insufficiency 27 . Similarly, Goldberg et al reported a 50% reduction in forced vital capacity if more than 60% of thoracic spine (8 thoracic vertebrae are fused) 28 . T1-T12 and T1-S1 height gain are the most commonly used parameters to determine the trunk height gained during distraction 29 . Trunk height is a surrogate marker for the increase in the thoracic volume needed for adequate lung development and the effectiveness of the distraction procedure 30 . Although the final T1-S1 height in the observation group is significantly less than the fusion group but that can be explained by the shorter pre-index surgery height of the patients who were observed. The authors in this study found no significant difference in the 2 groups with respect to the change in the trunk height in over-all or sub-analysis. Based on the results of the current analysis, it is pertinent to consider observation as a reasonable treatment option in patients with well-maintained sagittal and coronal profiles, a clinically acceptable rib-hump and truncal shift and an acceptable curvature. However, final fusion is unavoidable in graduates with poor sagittal or coronal balance, a severe rib-hump and Cobb’s angle or in cases needing revisions due to complications such as screw pullout or hook dislodgment nearing skeletal maturity.
A few drawbacks of this study need mentioning. Most of the available citations on the topic are retrospective case-control studies. There is a lack of good quality prospective studies comparing post-graduation strategies in these patients. Removal of implants at graduation may be considered as a possible treatment strategy and should be evaluated in patients with an acceptable deformity and balance at graduation. Homogeneity of the studies included in proportional meta-analysis was questionable in terms of the age, surgical techniques (rib based/spine based distractions or magnetic and traditional growing rods) and outcome measures especially the T1-T12 and T1-S1 heights. The authors have performed sub-analysis with only case-control studies to limit the heterogeneity in analysis. Further, the authors also acknowledge poorly reported functional outcomes and pulmonary function outcomes in all the citations.
Nevertheless, this is the first review with analysis comparing the outcomes of the commonly practiced graduation strategies in EOS patients managed with growing rods. The current research should help clinicians in evidence–based decision-making for EOS patients keeping the risks and benefits of various strategies in mind.
Conclusions
The available literary evidence suggests that in the presence of acceptable deformity with mild to moderate Cobb's angle and balanced spine, observation alone could be a suitable alternative to fusion surgery. The risk of revision surgeries was found to be significantly higher in patients who underwent definitive fusion. Nevertheless, the lack of good quality evidence and scarcity of literature on the topic was also propounded by this review. Prospective, randomized and multicentre RCT’s with longer follow-ups are required to establish the superiority of 1 treatment strategy over the other.
ORCID iDs
Kaustubh Ahuja https://orcid.org/0000-0003-1344-9889
Samarth Mittal https://orcid.org/0000-0003-3528-0949
Nikhil Goyal https://orcid.org/0000-0002-0387-4358
P. Venkata Sudhakar https://orcid.org/0000-0002-5976-561X
Pankaj Kandwal https://orcid.org/0000-0002-8801-6909
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, and patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
This work was performed at Indraprastha Apollo Hospital, New Delhi.