
Abstract
Study Design:
Retrospective multicenter study.
Objectives:
To evaluate the outcomes of posterior cervical decompression for cervical spondylotic myelopathy (CSM) when performed by board-certified spine (BCS) or non-BCS (NBCS) surgeons.
Methods:
We reviewed outcomes for 675 patients who underwent surgery for CSM, were followed at least 1 year after surgery, and were assessed preoperatively and at final follow-up by Japanese Orthopaedic Association (JOA) scores and by the visual analog scale (VAS) for the neck. Cervical alignment was assessed on radiographs by C2-C7 angles, and range of motion (ROM) by extension minus flexion C2-C7 angles. We compared outcomes for BCS surgeons, who must meet several requirements, including experience in more than 300 spinal surgeries, and for NBCS surgeons.
Results:
BCS surgeons performed 432 of 675 laminoplasties. NBCS surgeons were primary in 243 surgeries, of which 187 were directly supervised by a BCS surgeon. BCS surgeons required significantly less time in surgery (98.0 ± 39.5 vs 108.1 ± 49.7 min; P < .01). BCS and NBCS surgeons had comparable perioperative complications rates, and preoperative-to-postoperative changes in JOA scores (2.9 ± 2.1 vs 3.1 ± 2.3; P = .40) and VAS (−1.5 ± 2.9 vs −1.4 ± 2.5; P = .96). Lordotic cervical alignment and ROM were maintained after operations by both groups.
Conclusions:
Surgical outcomes such as functional recovery, complication rates, and cervical dynamics were comparable between the BCS and NBCS groups. Thus, posterior cervical decompression for CSM is safe and effective when performed by junior surgeons who have been trained and supervised by experienced spine surgeons.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is a common degenerative disorder that causes spinal cord compression and neurological deterioration. The prevalence of CSM is expected to increase as the population ages. 1 The standard treatment for CSM is surgical decompression, which can halt neurological deterioration and improve the patient’s function and quality of life. 2 Of the various decompression techniques, laminoplasty of the cervical spine 3 –6 effectively recovers neurological function and is also remarkably cost-effective, since it eliminates the need for instrumentation for fixation. 7,8
With regard to spinal surgery as a whole, numerous studies have investigated how the participation of junior surgeons affects surgical outcomes and perioperative complications. 9 –18 Results vary; some studies report comparable outcomes regardless of the involvement of young surgeons (residents or fellows), 9,14,15,18 and others report that the participation of junior surgeons increases the risks for surgical site infections, displaced pedicle screws, and insufficient correction of scoliosis. 10,11,16 For the cervical spine specifically, there is limited evidence as to how the involvement of inexperienced surgeons affects outcomes following surgery. 12,13,17 Two studies found that in anterior cervical discectomy and fusion, the involvement of a resident as primary surgeon had no negative effect on surgical outcomes or perioperative complications, despite longer operation times and a higher estimated blood loss. 12,17 Another study found that the participation of a resident in posterior cervical fusion surgery was a significant predictor for blood transfusion, operative time, and length of hospital stay. 13 Although these studies clarify some of the issues associated with inexperienced surgeons, they dealt with a variety of diagnosed diseases and lacked detailed analyses, such as neurological function and imaging.
Therefore, to investigate the impact of surgeon experience on CSM treatment outcomes, here we conducted a multicenter study of patients with a diagnosis of CSM who were treated by posterior decompression without fixation. We compared and evaluated the functional and radiographic outcomes between surgeries performed by board-certified (BCS) and non-BCS (NBCS) spine surgeons in Japan.
Materials and Methods
Subjects
This study included 675 patients with clinically and radiographically confirmed CSM who were treated at 17 Japanese institutions between January 2012 and December 2014. All investigators were experienced orthopedic spine surgeons. This study was approved by the review board at each institution involved.
Subjects had to meet the following criteria to be included in the study: (1) they presented with at least one clinical sign of myelopathy, (2) there was evidence of cervical spinal cord compression on magnetic resonance (MR) imaging or computed tomography (CT), and (3) there was no previous cervical spine surgery. Patients were excluded if they were asymptomatic or were diagnosed with active infection, neoplastic spinal disease, rheumatoid arthritis, ankylosing spondylitis, ossification of the posterior longitudinal ligament, cervical kyphosis, or concomitant lumbar stenosis.
Indication and Surgical Technique
The patients included in this study were seen at an outpatient clinic before surgery by the doctor who would be the primary surgeon for the operation, regardless of whether a BCS or NBCS surgeon actually performed the surgery. The indication for surgery, technique, and range of decompression levels were decided by a spine team at each institute. Three different surgical techniques were used in this study: expansive open-door laminoplasty (OD), double-door laminoplasty (DD), or selective laminectomy with muscle preservation (SL). 3,5,6 OD, DD, and SL were conducted at 12, 7, and 9 institutions, respectively. In general, these techniques were indicated by multisegmental spondylosis in the presence of a narrow spinal canal without kyphotic cervical alignment.
Data Collection
We retrospectively collected demographic information, medical history, symptomology, imaging, the surgical summary, and other data for all subjects. All subjects were followed at least 1 year after surgery. Neurological status was assessed prior to surgery and at the final follow-up, and functional status was evaluated prior to surgery and at the final follow-up using Japanese Orthopedic Association (JOA) scores and the visual analog scale (VAS) for the neck. All surgery-related events that occurred within 30 days of the operation were defined as perioperative complications.
In Japan, becoming BCS surgeon requires that the surgeon (1) be authorized as a Spine Specialist Approved by the JOA; (2) be a member of the Japanese Society for Spine Surgery and Related Research (JSSR); (3) have surgical experience in more than 300 spine and spinal cord operations, including experience in more than 200 operations as the primary surgeon, and in more than 20 operations involving the cervical spine and 60 cases involving the lumbar spine; (4) have participated in at least 2 annual meetings of the JSSR within the past 5 years; and (5) have published at least 5 clinical papers related to the spine and spinal cord disorders.
In Japan, less-experienced NBCS surgeons train to become BCS surgeons by performing at least 200 spine surgeries. In this study, 21 NBCS surgeons were included. At the start of this study (the first patient registration), the NBCS surgeons’ mean age and practice time as an orthopedic surgeon were 32.2 ± 3.5 and 7.4 ± 3.1 years, respectively. Their average duration of practicing surgery at a spine training center was 1.5 ± 1.6 years. Over their career, they had conducted an average of 391.3 ± 221.2 orthopedic-related surgeries, and 79.9 ± 93.0 spine surgeries. In addition, members of this group who performed the surgery without direct BCS supervision had performed an average of 182.6 ± 163.5 spinal surgeries at that point.
In contrast to the North American medical educational system, the training period for physicians in Japan does not include resident or fellow grades. Spine surgeons in Japan are only classified as BCS or NBCS.
Imaging
The stenotic levels in CSM were assessed from T2-weighted sagittal MR images. Cervical alignment was assessed by measuring the intermittent C2-C7 angles from plain radiographs in the neutral position using the Cobb technique; the angles were determined by tangential lines on the posterior edge of the target vertebral bodies. The cervical range of motion (ROM) was calculated by subtracting the flexion from the extension C2-C7 angles.
Statistical Analysis
Continuous variables and frequencies were presented as means ± standard deviation, and categorical variables as percentages. Baseline demographics, preoperative scores, scores at final follow-up, and surgical characteristics in the two groups were compared by unpaired t test for continuous variables and by chi-square test for categorical variables. A P value less than .05 was considered statistically significant.
Results
Demographics and Imaging
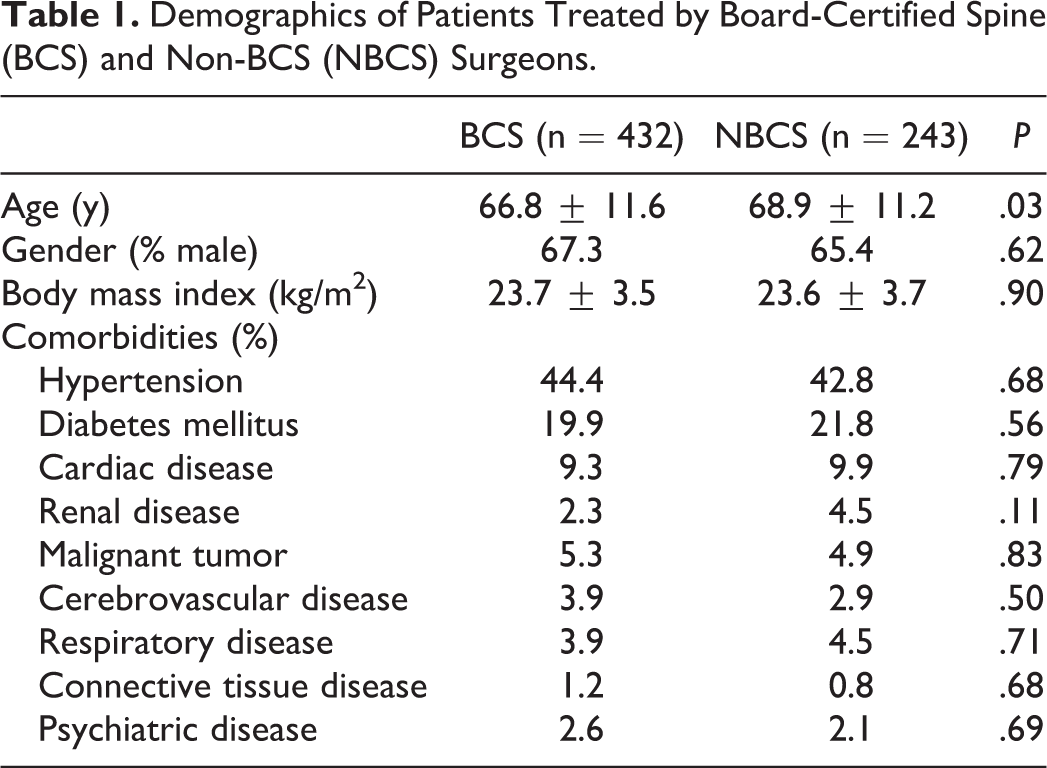
Table 1 summarizes the demographics for 675 subjects who underwent posterior cervical decompression for CSM. Of these operations, 432 were performed by BCS surgeons (64.0%) and 243 by NBCS surgeons (36.0%). The average duration of surgical experience was significantly longer in the BCS group rather than the NBCS group (18.9 ± 7.9 vs 9.2 ± 2.6 years; P < .01). In the NBCS group, 187 operations (77.0%) were performed under the direct supervision of a BCS surgeon. In these cases, the BCS surgeon was directly involved during the surgery, and personally instructed the junior NBCS surgeon in anatomy and technique. Patients in the BCS group were significantly younger (mean age 66.8 ± 11.6 years) than those in the NBCS group (68.9 ± 11.2 years; P = .03), but the 95% confidence interval partially overlapped between the groups (BCS, 65.7-67.9; NBCS, 67.4-70.3). There was no difference between the 2 groups in gender ratio (% male 67.3 vs 65.4; P = .62), BMI (23.7 ± 3.5 vs 23.6 ± 3.7 kg/m2; P = .90), or frequency of comorbidities. The mean follow-up period was 23.1 months in the BCS group and 21.3 months in the NBCS group.
Demographics of Patients Treated by Board-Certified Spine (BCS) and Non-BCS (NBCS) Surgeons.
MR images were available for 396 subjects in the BCS group and for 224 in the NBCS group. The level of the most severe stenosis was C4/5 in the BCS group (35.1%) and C5/6 in the NBCS group (38.8%) (Table 2). The difference in distribution of stenosis severity did not differ significantly between the groups (P = .81).
The Most Severe Stenotic Level, Revealed by Magnetic Resonance Imaging.
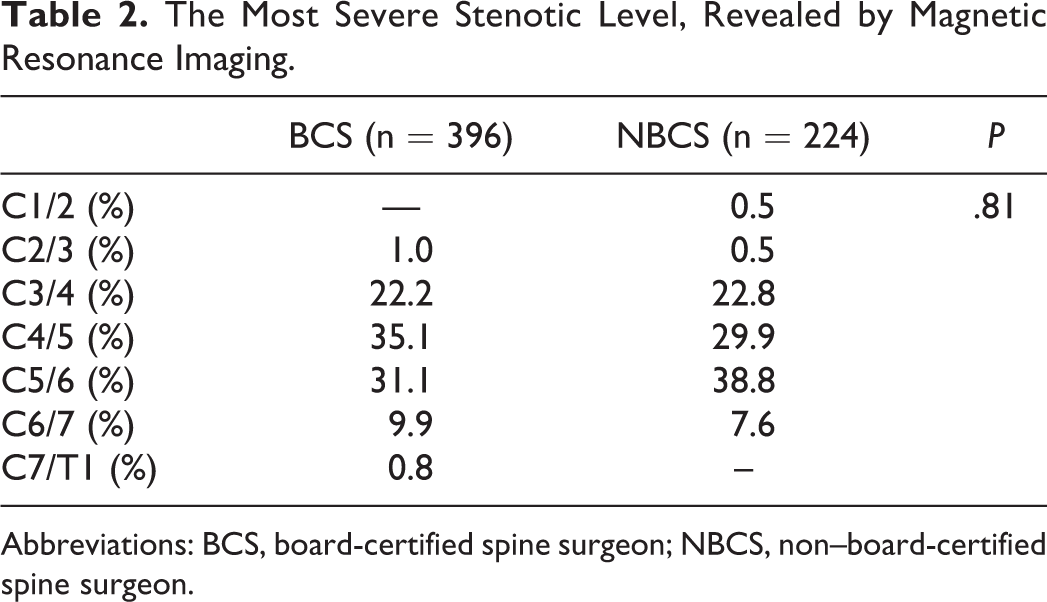
Abbreviations: BCS, board-certified spine surgeon; NBCS, non–board-certified spine surgeon.
Surgical Summary and Perioperative Complications
In the BCS group, DD (38.9%) was performed most frequently, while the frequencies of OD (30.8%) and SL (30.3%) were almost equal. In the NBCS group, OD was the most frequent surgical technique (53.5%; Table 3), followed by SL (34.2%) and DD (12.4%). The difference in surgical methodology between the 2 groups was significant (P < .01).
Surgical Factors and Perioperative Complications.
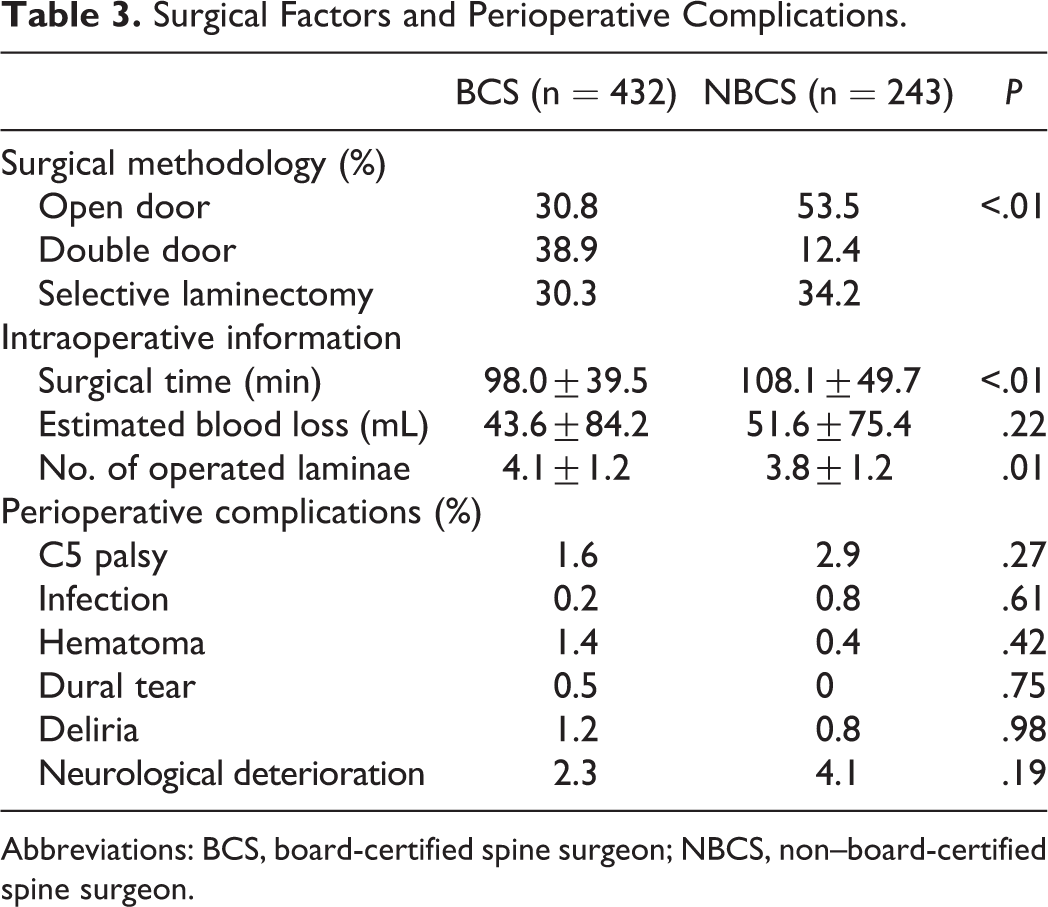
Abbreviations: BCS, board-certified spine surgeon; NBCS, non–board-certified spine surgeon.
Surgical times were significantly shorter in the BCS than in the NBCS group (98.0 ± 39.5 vs 108.1 ± 49.7 min; P < .01), whereas there was no significant difference in estimated blood loss (43.6 ± 84.2 vs 51.6 ± 75.4 mL; P = .22; Table 3). The number of operated laminae was significantly larger in the BCS group (4.1 ± 1.2 vs 3.8 ± 1.2; P = .01). The number of perioperative complications per subject was comparable between the groups (0.05 ± 0.23 vs 0.04 ± 0.21; P = .51). As shown in Table 3, detailed analysis showed no significant difference in complication rates for C5 palsy (1.6% vs 2.9%; P = .27), surgical site infection (0.2% vs 0.8%; P = .61), hematoma (1.4% vs 0.4%; P = .42), dural tear (0.5% vs 0.0%; P = .75), deliria (1.2% vs 0.8%; P = .98), or neurological deficit (2.3% vs 4.1%; P = .19) between the BCS and NBCS groups. The occurrence of these complications was also statistically insignificant when comparing rates between BCS-supervised and BCS-unsupervised surgeries within the NBCS group (0.08 ± 0.31 vs 0.16 ± 0.41; P = .12). There was no revision surgery in any subject after the initial posterior cervical decompression. The number of complications was also comparable between the BCS and NBCS groups within each surgical technique (OD, 0.14 ± 0.38 vs 0.15 ± 0.42, P = .83; DD, 0.08 ± 0.29 vs 0.03 ± 0.18, P = .42; SL, 0.07 ± 0.28 vs 0.05 ± 0.22, P = .57).
Surgical Outcomes
As shown in Table 4, the baseline JOA scores prior to surgery showed significantly better function in patients in the BCS group (11.1 ± 2.7) than those in the NBCS group (10.6 ± 2.7; P = .03). However, this difference became insignificant in the postoperative JOA scores at final follow-up between the BCS and NBCS operations (14.0 ± 2.1 vs 13.6 ± 2.2; P = .06). In fact, the changes in JOA scores were comparable between the 2 groups (2.9 ± 2.1 vs 3.1 ± 2.3; P = .40), and were also comparable between NBCS surgeries with or without a participating BCS surgeon (3.2 ± 2.3 vs 2.6 ± 1.9; P = .11).
Surgical Outcomes.
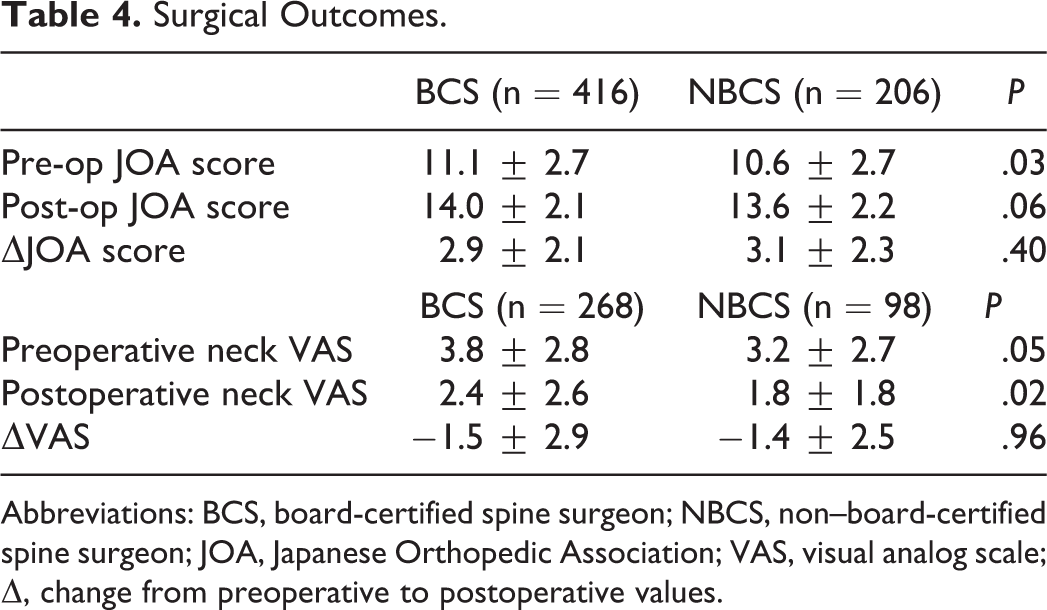
Abbreviations: BCS, board-certified spine surgeon; NBCS, non–board-certified spine surgeon; JOA, Japanese Orthopedic Association; VAS, visual analog scale; Δ, change from preoperative to postoperative values.
With regard to the outcomes in each surgical technique, the changes in JOA scores did not show statistical significance between the BCS and NBCS groups in OD (3.4 ± 1.8 vs 3.1 ± 2.7; P = .25), DD (2.9 ± 2.2 vs 3.4 ± 1.8; P = .40), and SL (2.4 ± 2.1 vs 2.9 ± 2.3; P = .14).
The VAS analysis for the neck showed that patients in the BCS group had more severe pain prior to surgery (3.8 ± 2.8) than those in the NBCS group (3.2 ± 2.7; P = .05). The VAS at final follow-up was significantly worse in the BCS group (2.4 ± 2.6) than in the NBCS group (1.8 ± 1.8; P = .02). However, when evaluating changes in VAS, the results between the 2 groups were comparable (−1.5 ± 2.9 vs −1.4 ± 2.5; P = .96).
Evaluation of Cervical Alignment
Radiographic analyses of the C2-C7 angle showed a more lordotic preoperative alignment of the cervical spine in patients in the NBCS group (14.5° ± 12.9°) than in patients in the BCS group (12.7° ± 13.7°; P = .09; see Table 5). At final follow-up, this lordotic curvature was slightly reduced in both the BCS (12.3° ± 14.3°) and NBCS (13.5° ± 13.9°) groups, with no significant difference between the groups (P = .31). With regard to the ROM of the cervical spine, there was no significant difference between the BCS and NBCS groups in the preoperative (35.3° ± 13.8° vs 35.1° ± 13.2°; P = .84) or postoperative (29.9° ± 12.3° vs 31.1° ± 13.3°; P = .28) ROM.
Preoperative and Postoperative Imaging.
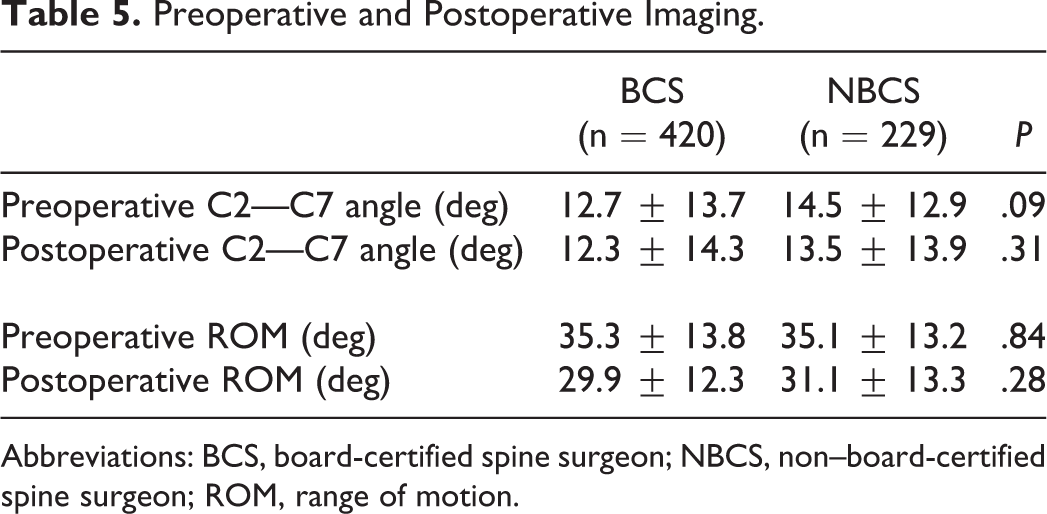
Abbreviations: BCS, board-certified spine surgeon; NBCS, non–board-certified spine surgeon; ROM, range of motion.
Discussion
This is the first multicenter study to examine the impact of unexperienced surgeons on surgical outcomes after posterior decompression for CSM, and our study has the largest sample size to date. Although NBCS surgeons required significantly more time in surgery despite a smaller number of operated laminae, there was little influence on surgical outcomes as assessed by changes in JOA scores or VAS for the neck, perioperative complications, or changes in postoperative ROM or spinal alignment. These findings indicate that decompressive surgery for CSM is equally safe and effective when conducted by a BCS or NBCS surgeon. Therefore, if predominantly supervised by experienced surgeons, less-experienced surgeons can achieve results comparable to those of BCS surgeons when performing posterior cervical decompression for CSM patients.
In the present study, the surgical techniques for cervical decompression varied significantly between the 2 groups. Patients in the NBCS group were treated more frequently by OD and less frequently by DD than patients in the BCS group. The reason for this difference was that more than half of the participating institutes mainly performed OD, while DD was specifically conducted at 3 high-volume institutes that had few NBCS spine surgeons. Although this technical variation could have affected the surgical outcomes, previous comparisons of OD and DD clinical outcomes revealed comparable postoperative JOA scores and recovery rates. 19 –22 In addition to neurological function, a recent meta-analysis of postoperative complications and radiographic parameters showed no advantage of one technique over the other. 23 Thus, our study is consistent with previous reports in finding that the neurological recovery and complication rates were favorable despite differences in surgical technique, regardless of whether a BCS or NBCS surgeon performed the surgery. Although further studies are needed to compare the outcomes from SL with those from other procedures, the methodological differences did not affect the surgical outcomes or complications in this study.
NBCS surgeons required significantly more surgical time than BCS surgeons despite having fewer operating laminae, although the difference was only 10 minutes (108.1 ± 49.7 vs 98.0 ± 39.5 min). This is not difficult to explain, since surgeons who are not used to performing decompression surgery are less familiar with the technique and anatomy, and require more time for instruction and supervision during the operation. Even so, surgical times for the NBCS group were within the range of mean operation times reported for laminoplasty, from 90 to 168.8 min. 5,19 –21 Moreover, the estimated blood loss and rate of perioperative complications were similar for both groups despite the difference in operation time. Thus, the longer surgical time required by junior surgeons did not negatively affect the perioperative outcomes.
The different number of operated laminae between the groups was probably due to a change in surgical philosophy over time. C3-C7 laminoplasty has been performed since this technique was developed. 3 However, one of our authors later proposed the novel concept of selective laminoplasty, 24 which is less invasive and reduces axial symptoms and segmental motor paralysis. This concept has been gradually adopted by younger surgeons, whereas senior surgeons are more likely to hold onto the original philosophy. This history may have led to the significant difference in the decompressive ranges between the BCS and NBCS surgeons.
A previous study showed that maintaining a lordotic cervical alignment after laminoplasty does not increase axial pain. 21 Patients in our study had a postoperative lordotic alignment despite a slight loss of curvature, but still experienced a reduction in pain. Cervical ROM is known to decrease after the laminoplasty, 19,20,22 and ROM was reduced in our study as well. However, our study found a postoperative ROM of about 30°, which is larger than the range of 16° to 26° reported in previous studies. 19,20,22 Therefore, the preservation of cervical ROM in the present study might improve functional outcomes after surgery. Notably, postoperative cervical alignment and ROM were well maintained in the NBCS group, indicating that posterior decompression performed by less experienced surgeons does not negatively affect the dynamics of the cervical spine.
When evaluating outcomes of operations conducted by NBCS surgeons, it is important to consider whether an experienced attending surgeon participated in the operation and directly instructed the less experienced surgeon. In the present study, BSC surgeons attended in approximately 77% of the operations in which an NBCS surgeon was primary. The postoperative functional outcomes and complication rates were comparable in operations performed by NBCS surgeons with or without supervision by a BCS surgeon. This is not surprising, since a NBCS surgeon is expected to have some degree of surgical experience before performing operations without a supervising BCS surgeon, and the surgical outcomes in the NBCS group were similar whether a BCS instructor was present or not. These results indicated that laminoplasty or selective laminectomy can be effective even when performed by inexperienced surgeons if supervised by an experienced surgeon.
With regard to the patient age at surgery, the 95% confidence interval was 65.7 to 67.9 in the BCS group and 67.4 to 70.3 in the NBCS group, so the intervals partially overlapped between the groups. Therefore, although there was a statistically significant difference between the groups, it could have been due to the large sample size, and was probably not clinically meaningful.
Several limitations in this study should be noted. First, this is a retrospective study, which inevitably carries a low evidence level. Further prospective studies should be conducted to validate these results. Second, there was no standardized educational protocol for residents or fellows among the various institutions, and decisions about surgical methods and the number of decompression levels were made at the discretion and preference of the surgeons. Third, the postoperative rehabilitation for CSM patients was not consistently defined and was likely to differ among institutions.
In conclusion, although the surgical time was longer in the NBCS group, postoperative functional recovery, the rate of perioperative complications, and changes in cervical dynamics on radiographs were comparable in the NBCS and BCS groups. These results suggest that posterior cervical decompression is a safe technique that is effective even when performed by young surgeons under the supervision of experienced spine surgeons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.