
Abstract
Study design
Prospective, randomized controlled study.
Objective
To assess the safety and efficacy of an ultrasound-guided ISP block for postoperative analgesia in posterior cervical laminectomy.
Methods
88 patients requiring posterior cervical laminectomy were randomized into two groups, those who underwent ISP block with multimodal analgesia (ISPB group) and those with only multimodal analgesia (control group). Demographic details, intraoperative parameters (blood loss, duration of surgery, perioperative total opioid consumption, muscle relaxants used), and postoperative parameters (numeric rating scale, satisfaction score, mobilization time, and complications) were recorded.
Results
The total opioid consumption (128.41 + 39.65vs 284.09 + 140.92mcg; P < .001), muscle relaxant usage (46.14 + 6.18 mg vs 59.32 + 3.97 mg; P < .001), surgical duration (128.61 + 26.08/160.23 + 30.99mins; P < .01), and intra-operative blood loss (233.18 + 66.08 mL vs 409.77 + 115.41 mL; P < .01) were significantly less in the ISPB group compared to the control. In the postoperative period, the control group’s pain score was significantly higher (P < .001) in the initial 48 hours. The Modified Observer Alertness/Sedation Score (MOASS) score and satisfaction scores were significantly better in the ISPB compared to the control (P < .001). The mean time required to ambulate was statistically less in ISPB (4.30 + 1.64hours) when compared to controls (9.48 + 3.07hours) (P < .001).
Conclusion
In patients undergoing posterior cervical laminectomy, ISP block is a safe and effective technique with better outcomes than standard multi-modal analgesia alone, in terms of reduced intra-operative opioid requirements and blood loss, better postoperative analgesia, and early mobilization.
Keywords
Introduction
Posterior cervical laminectomy is the standard surgical treatment for patients presenting with myelopathy resulting from multilevel cervical degeneration or ossification of the posterior longitudinal ligament. 1 From a surgical standpoint, these are typically extensive surgeries that necessitate more opiate use perioperatively, delayed anaesthetic recovery, and result in post-operative morbidity, especially in elderly patients. 2 Ineffective pain management in elderly patients results in delayed mobilisation and a longer stay in the hospital, with added complications like pneumonia, myocardial ischemia, and venous thrombosis. 3
Postoperative pain management in elderly patients is complicated by factors such as preexisting pain and chronic analgesic and/or opioid usage, which alter their pain perception. 4 Due to increased opioid sensitivity and the risk of postoperative delirium, respiratory depression and postoperative pain management are of particular importance in elderly patients. In addition, the use of NSAIDs carries a higher risk of GI bleeding, perforation, and renal impairment. 5
With very limited options available, the scope of regional anaesthesia using targeted nerve root blocks like the erector spinae plane (ESP) block, the multifidus cervicis plane (MCP) block, and the intersemispinal plane (ISP) block is rapidly expanding in cervical spine surgery. 6 Regional pain control using ultrasound-guided ESP block, which involves delivering the local anaesthetic agent close to the origin of the doral rami at the transverse level, has been proven to have a promising role in controlling postoperative pain in posterior cervical spine surgery. 7 However, this block is technically challenging at the cervical level, which demands an expert’s hand for proper block execution.
Ultrasound-guided cervical paraspinal block techniques include the multifidus cervicis plane (MCP) block and the intersemispinal plane (ISP) block, which involve the injection of the local anaesthetic agent into one of the fascial planes of the paraspinal muscles. 8 The MCP block is analogous to the thoracolumbar interfascial plane (TLIP) block, intended for the cervical spine, which was described by Ohgoshi et al. MCP block is relatively a deeper plane block, which has a potential risk of violation into thecal space or perforation of vessels accompanying the dorsal rami. The ISP block is a more superficial block that involves the injection of the anaesthetic agent between the semispinalis capitis and semispinalis cervicis. 9
This study is a randomized controlled study of ISP block in patients undergoing posterior instrumented cervical laminectomy. The primary outcome measures of the study were to determine the perioperative total opioid consumption and postoperative pain score, whereas the secondary outcome measures were to determine the intraoperative requirement of muscle relaxant, amount of blood loss, surgical duration, ambulatory time, and duration of stay in hospital.
Materials and Methods
This study is a prospective, randomized controlled study conducted from November 2022 to November 2023. The trial was registered with the clinical trial registry (CTRI/2022/11/060284) following the institutional review board approval. Consent was obtained from all patients included in the study.
Inclusion and Exclusion Criteria
The inclusion criteria was patients older than 20 years diagnosed with cervical compressive myelopathy (spondylotic/ossified posterior longitudinal ligament) and were going to have an elective multi-level instrumented cervical laminectomy. Patients who had a bleeding disorder, poor skin condition or local infection, cervical spine injury, systemic infection, tumours, or who refused to provide consent were excluded. Among a total of 92 patients, 4 were excluded based on exclusion criteria, and the rest (n = 88) were randomized using computer-generated numbers and allocated into an ISPB group (bilateral ISPB with multimodal analgesics) or a control group (multimodal analgesics only). The allocation details of the study have been represented using the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting randomized trials (https://www.consort-statement.org/). [Figure. 1]. Patients in both groups were administered 75 mg of pregabalin and 1 g of acetaminophen on the night before surgery, and the standard technique of general anaesthesia was used. CONSORT flow diagram.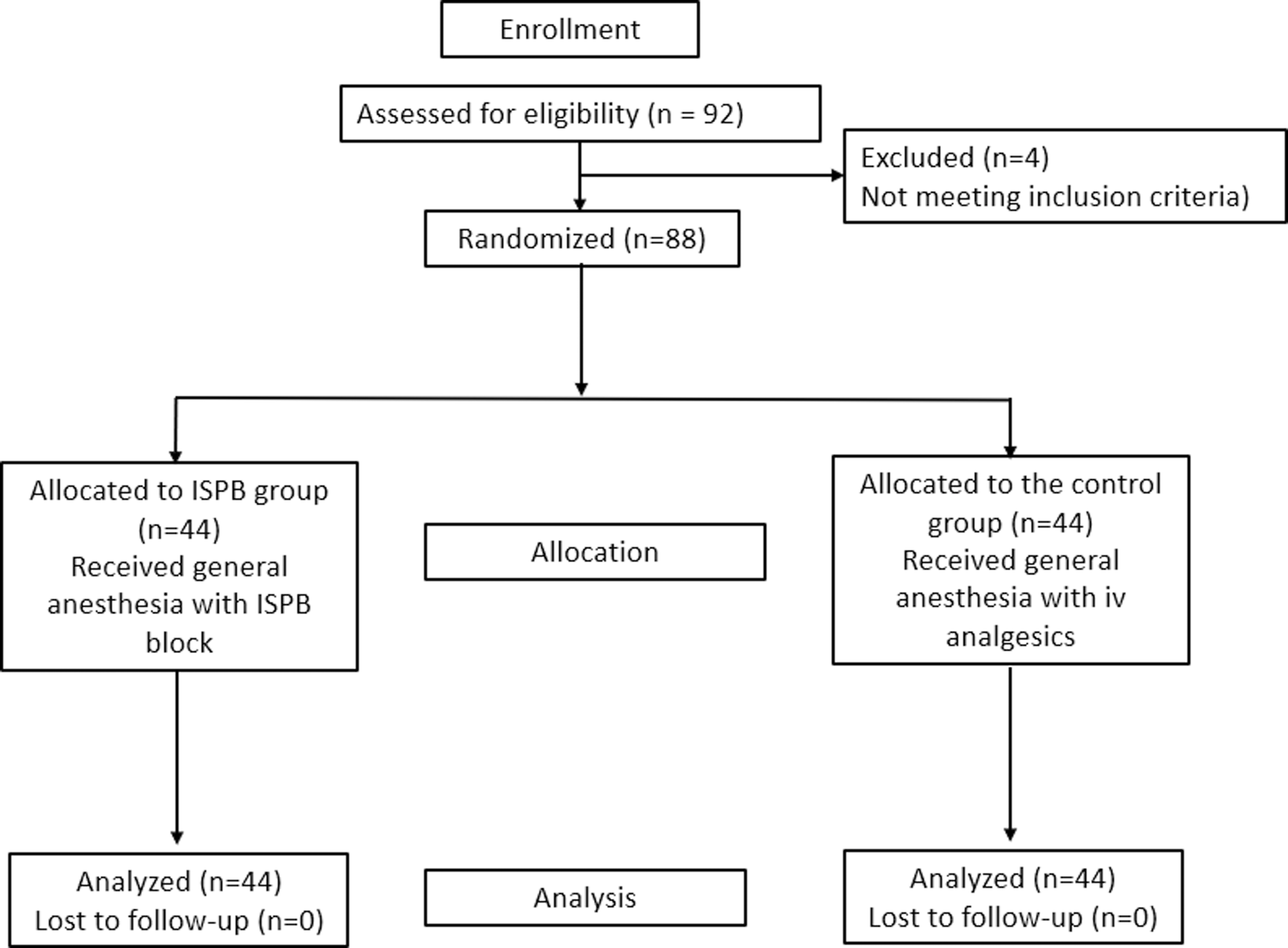
Technique of Ultrasound-Guided ISP Block
After induction, patients were placed prone on bolsters with the neck in neutral alignment. The case group was administered bilateral ISP blocks, while the control group did not receive any blocks. Only a single senior anesthesiologist, experienced in ISP blocks, performed the blocks. After disinfecting the skin, a 2-5 MHz linear probe orientated in the transverse plane (SonoSite Edge II, Bothell, WA, USA) was used to identify the five-layered posterior cervical muscles at the level of C5. By sliding the probe cranially, we were able to count the fifth cervical spine from the C7 spinous process. A 23 G 90 mm Quincke’s spinal needle (B Braun, Melsungen, Germany) was inserted in-plane through the skin and advanced into the fascial plane between the semispinalis cervicis and semispinalis capitis muscles under continuous ultrasound guidance. The correct needle tip position under the semispinalis capitis was confirmed by hydrodissection using 1 mL of normal saline, followed by injection of a mixture containing 15 mL of Inj. Bupivacaine .25% and Dexamethasone 8 mg. Correct drug placement was confirmed by the linear spread of the local anaesthetic drug, which separated the semispinalis capitis and semispinalis cervicis muscles. The spread of the drugs proximally and distally was confirmed through ultrasound. A similar mixture was administered on the other side too (Figure 2). The ISP block was administered by an experienced anesthetist who regularly does USG-guided block. Hence the time taken to administer the ISP block in our study patients was 15 minutes. After skin preparation and draping, a C3 to C6 instrumented cervical laminectomy with lateral mass screws was performed in a standard manner. Throughout the surgery, the cumulative consumption of fentanyl and a muscle relaxant (rocuronium) was recorded. Demonstration of US-guided ISP block.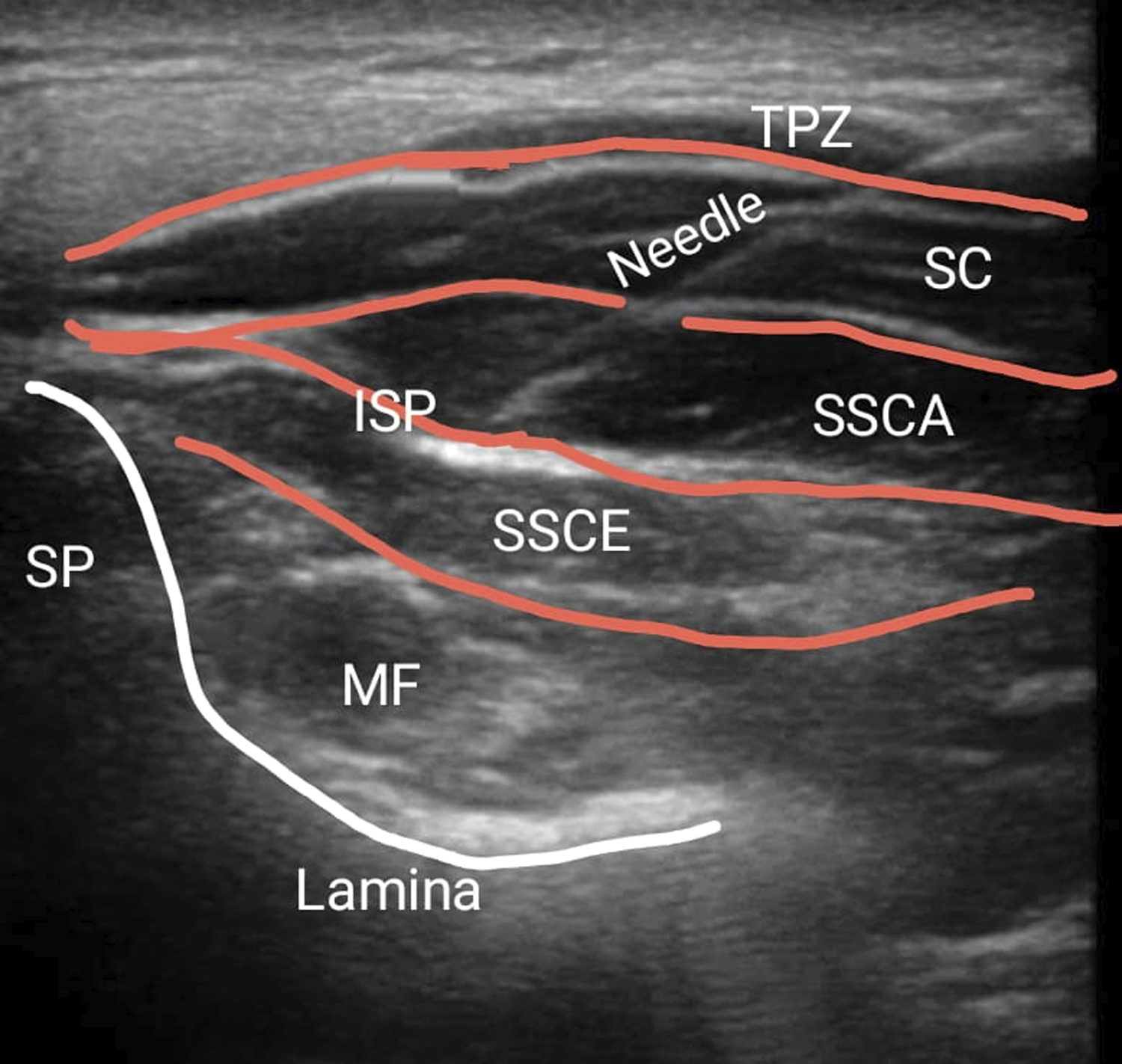
Outcome Parameters
Intra-operative parameters, namely the amount of blood loss and duration of surgery, opioid usage, and amount of muscle relaxants, were noted. Standard post-operative analgesia was provided with 1g Paracetamol IV (8th hourly) and Pregabalin 75 mg once a day. For breakthrough pain, a fentanyl infusion was administered, and the amount of fentanyl used was documented. In the first 72 hours, the Numeric Rating Scale for pain score for surgical site pain, Modified observer’s alertness/sedation score (MOASS) (Appendix 1), time to ambulate, total amount of opioids consumed (TOC), and all the complications were documented. The information was documented every 2 hours in the first 8 hours and then 12-hourly until 72 hours by two independent physician assistants. All the patients filled out a 10-point questionnaire (total satisfaction score) (Appendix 2) at the end of 72 hours postoperatively.
Statistical Analysis
The sample size was calculated based on the assumption that the drug fentanyl had at least 70 percent analgesic effect on the testing population and >95% effect on the general population. With a 95% CI of 80% power and a ratio of unexposed to exposed of 1:1, with an odd’s ratio of 2.5 and a risk of 1.7, the sample size estimated for this trial was 60, with 30 patients in each group. To improve the strength of the study and to compensate for potential dropouts, we included 30% more patients in each group. The data were analysed using SPSS v21. For continuous variables, we used an unpaired t test; for categorical ones, we used either Fisher’s exact or a Chi-square test. For continuous data, the one-way ANOVA test was utilized for significance testing when comparing groups, and for post hoc analysis, the LSD test was used. Statistical significance was determined by a P-value less than .05.
Results
Demographic and Clinical Characteristics of Both Groups.
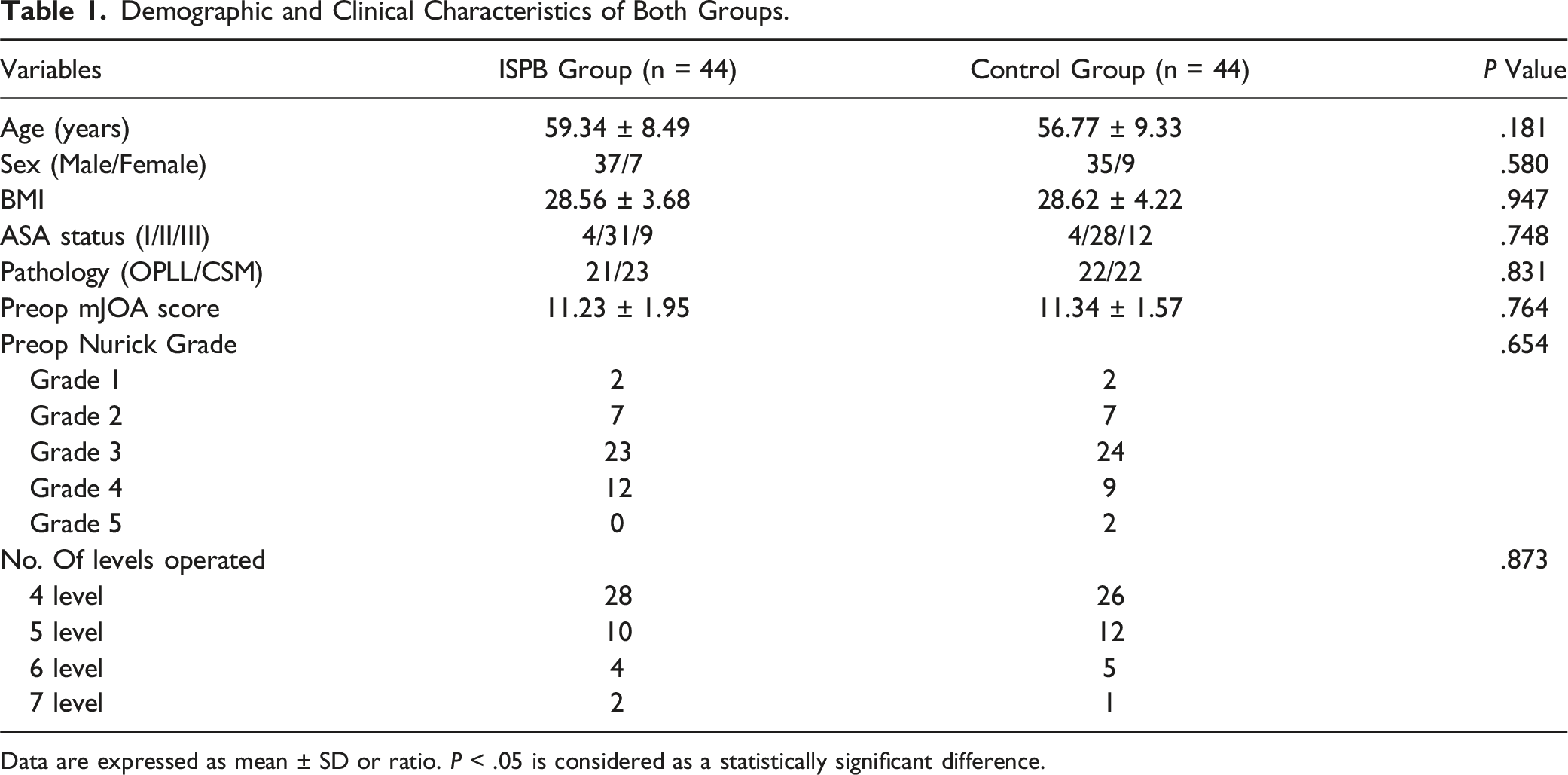
Data are expressed as mean ± SD or ratio. P < .05 is considered as a statistically significant difference.
Intra-operative Parameters
Primary and Secondary Outcome Parameters.
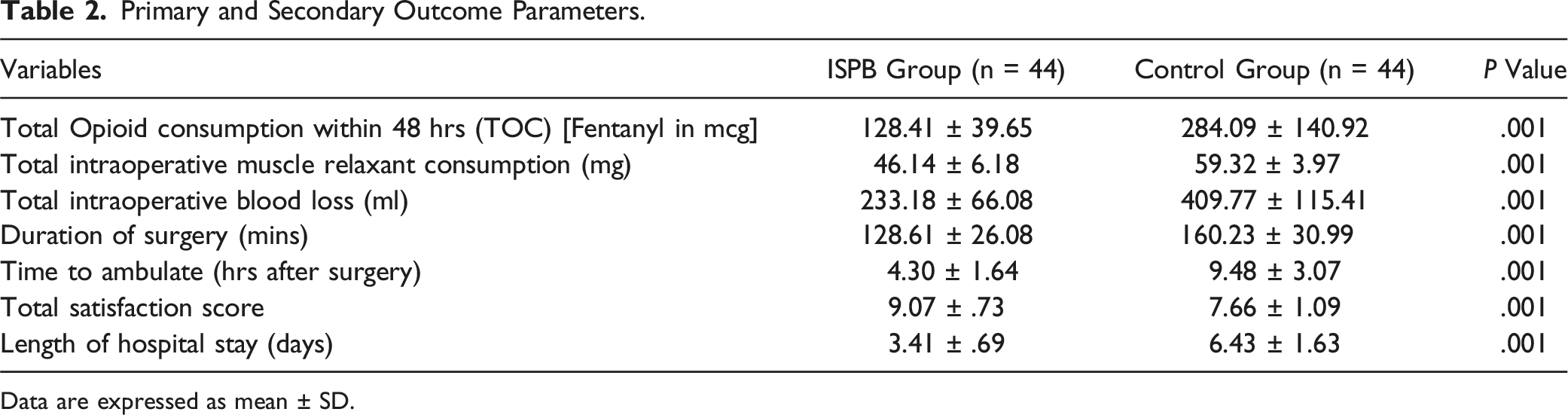
Data are expressed as mean ± SD.
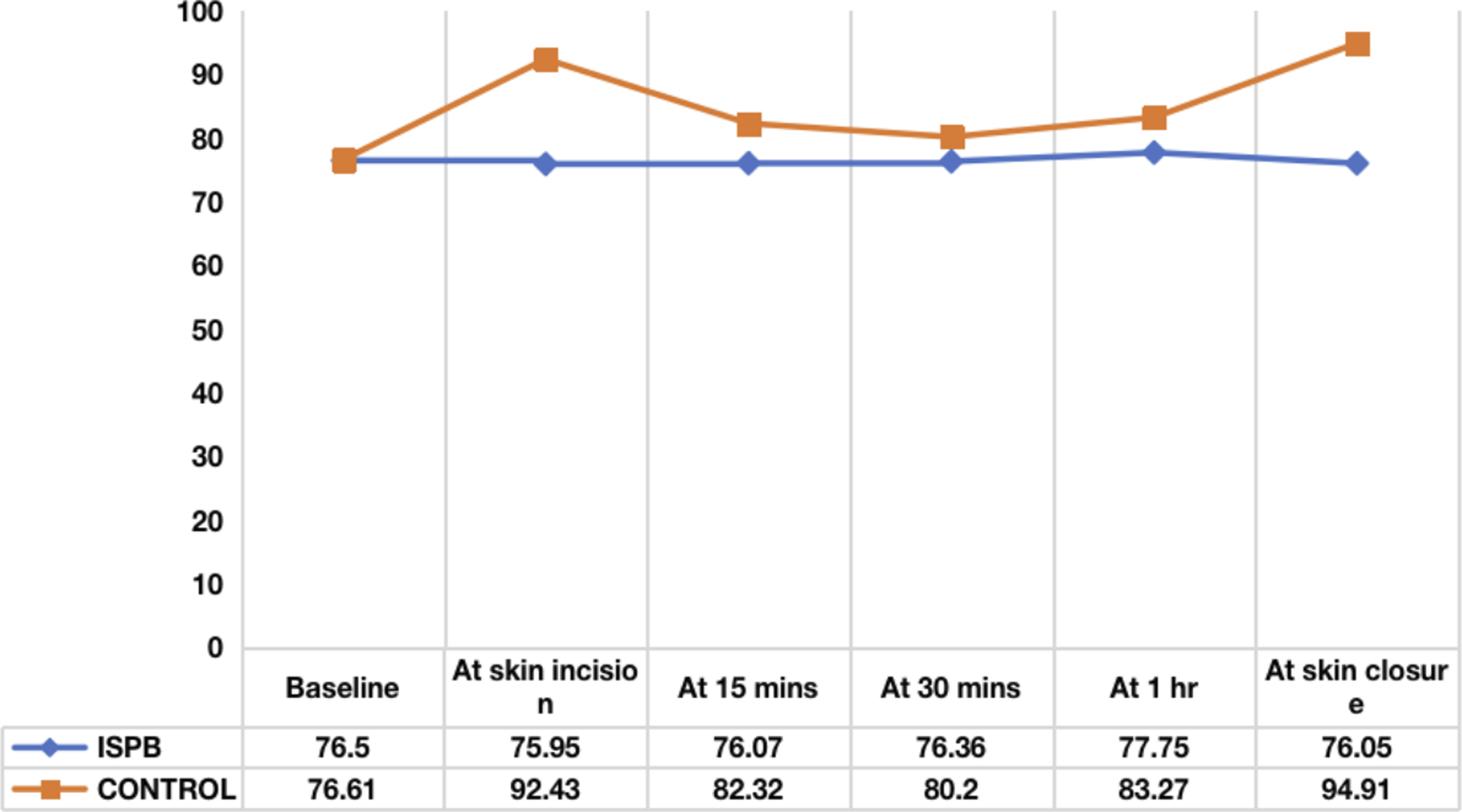
Mean heart rate distribution between two groups at various time intervals.
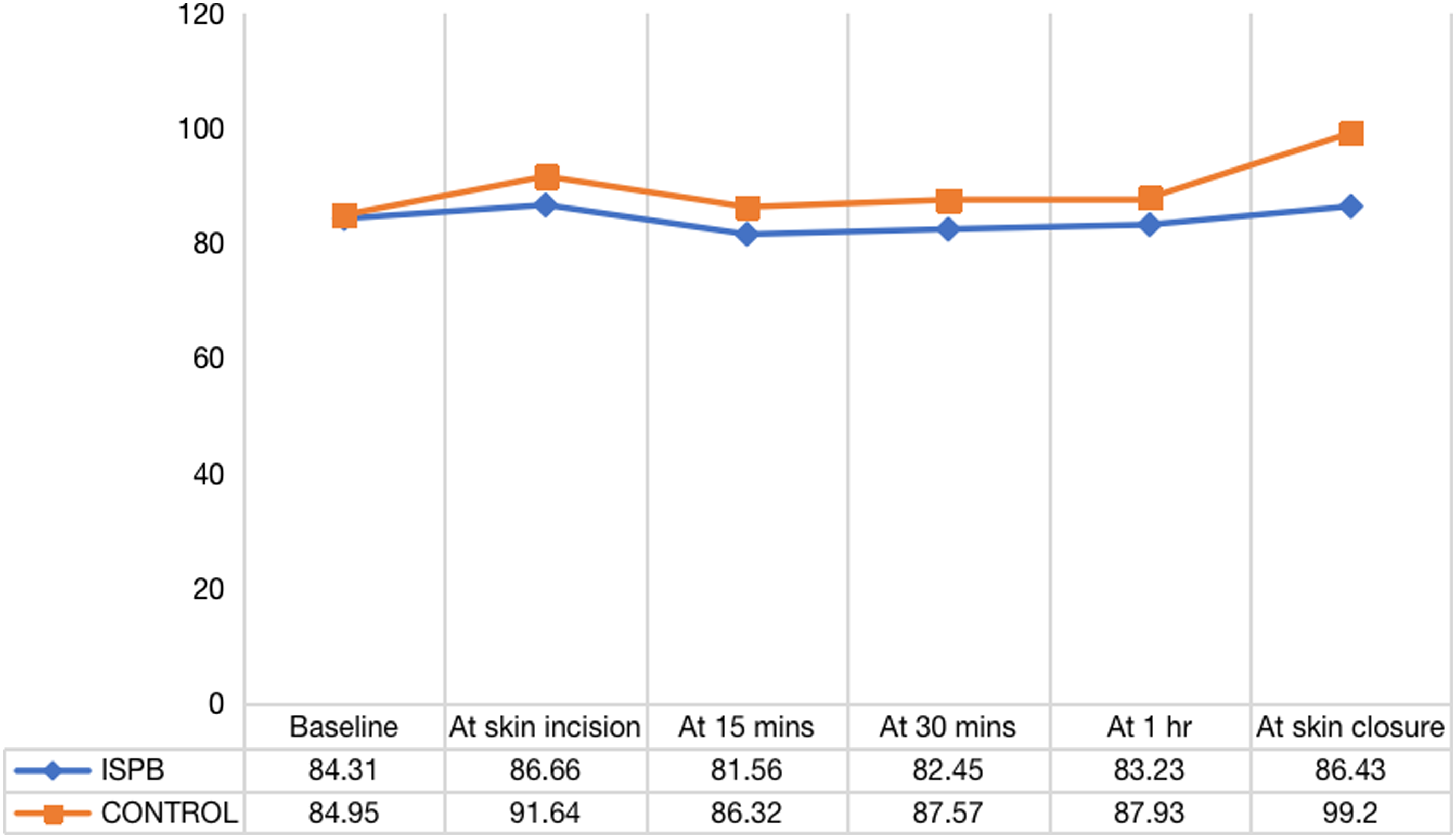
Mean arterial pressure distribution between two groups at various time intervals.
Post-operative Parameters
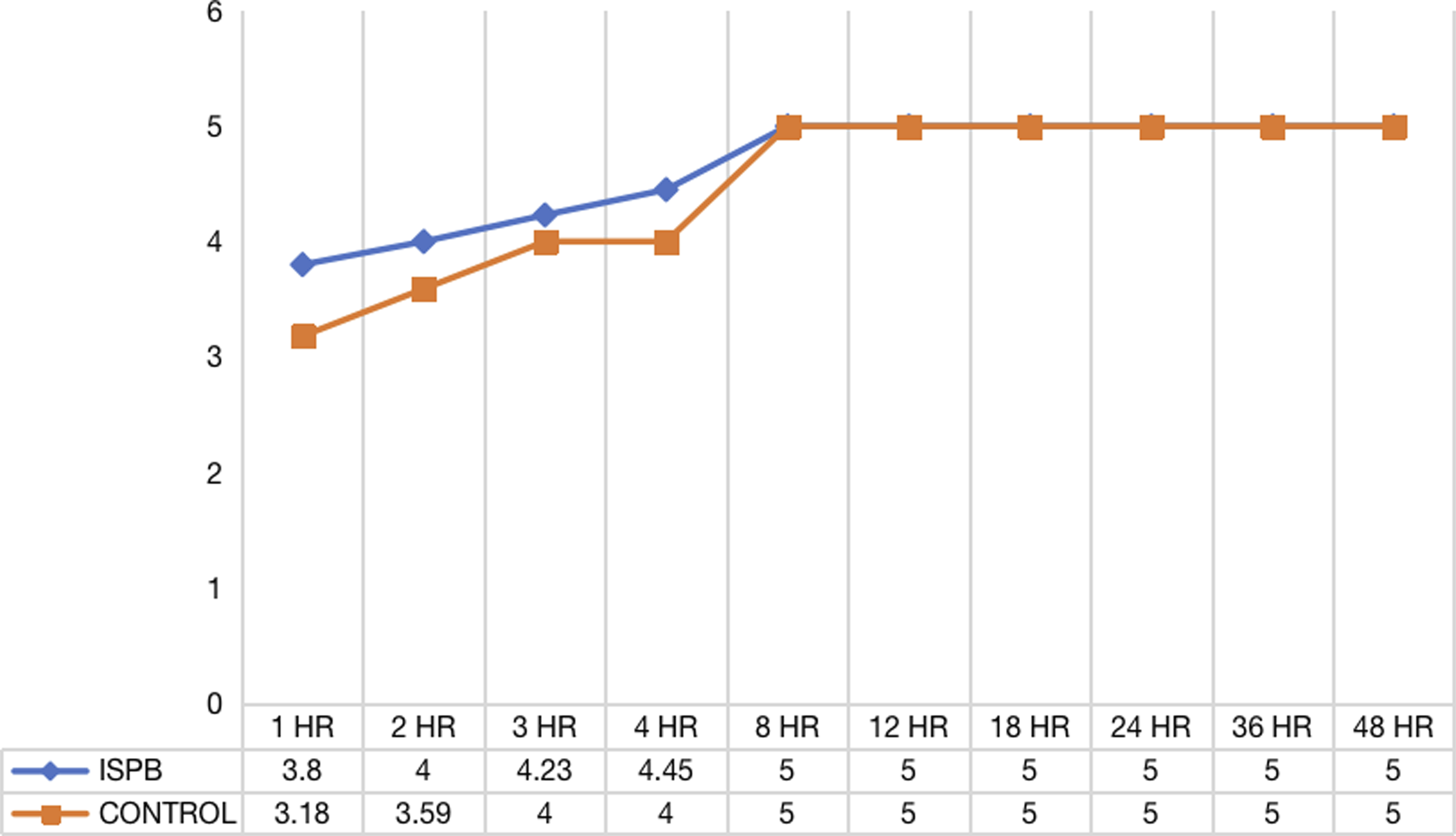
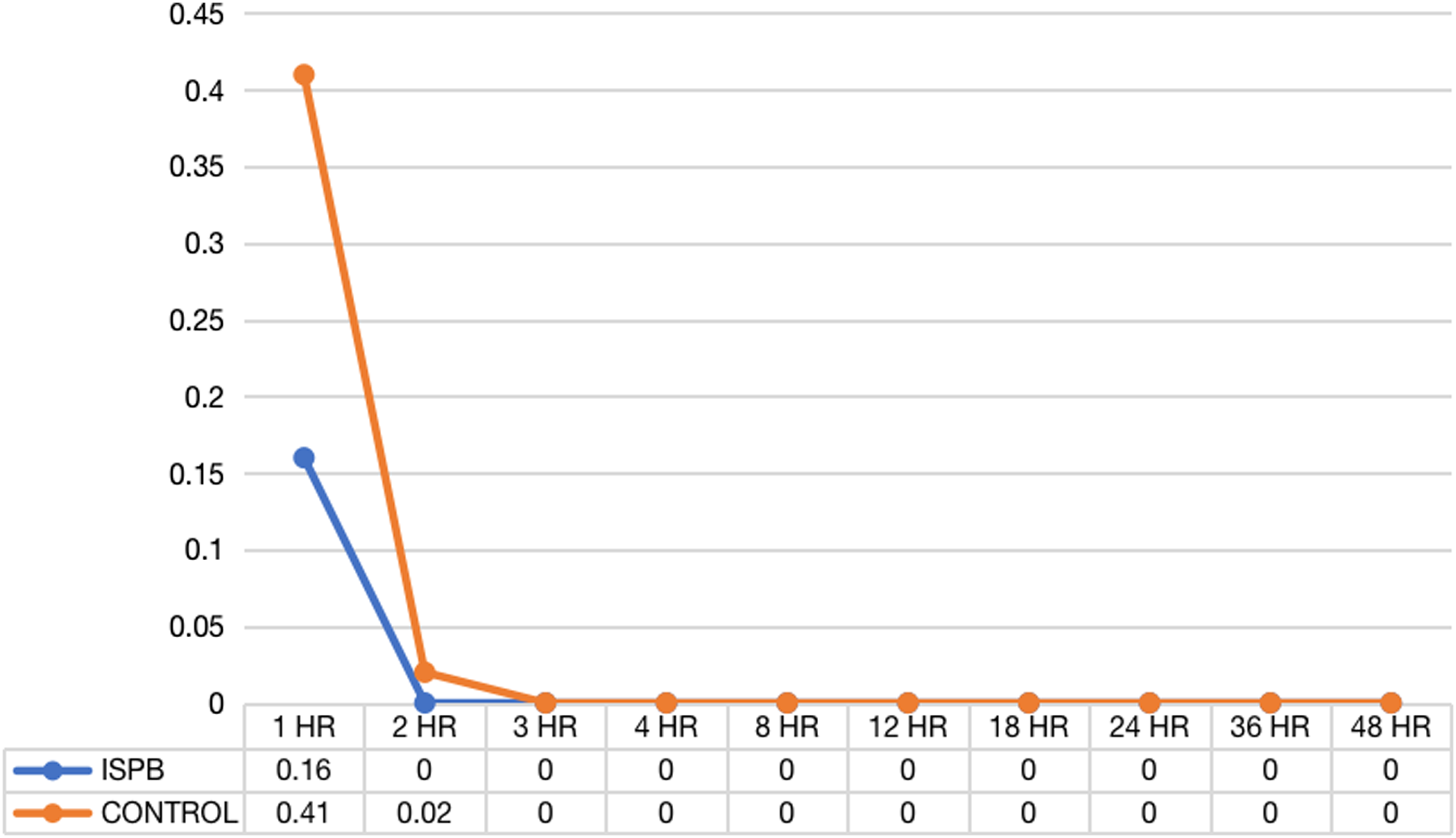
Compared to the ISPB group, the control group’s pain scoring (NRS) was significantly higher in the initial 72 hours postoperatively at all time scales of assessment when compared to the controls (Figure 5). The MOASS score at 1, 2, 3, and 4 hours was significantly lower in the control group (3.18, 3.59, 4, 4) when compared to the ISPB group (3.8, 4, 4.23, 4.45) indicating decreased alertness, presumably due to higher opiate usage in controls (Figure 6). After 8 hours, the scores matched in both groups. Similarly the PONV score was higher in the control group in the immediate postoperative period when compared to the ISPB group (Figure 7). Average NRS between two groups at various time intervals. Average MOASS score between two groups at various time intervals. Average PONV score between two groups at various time intervals.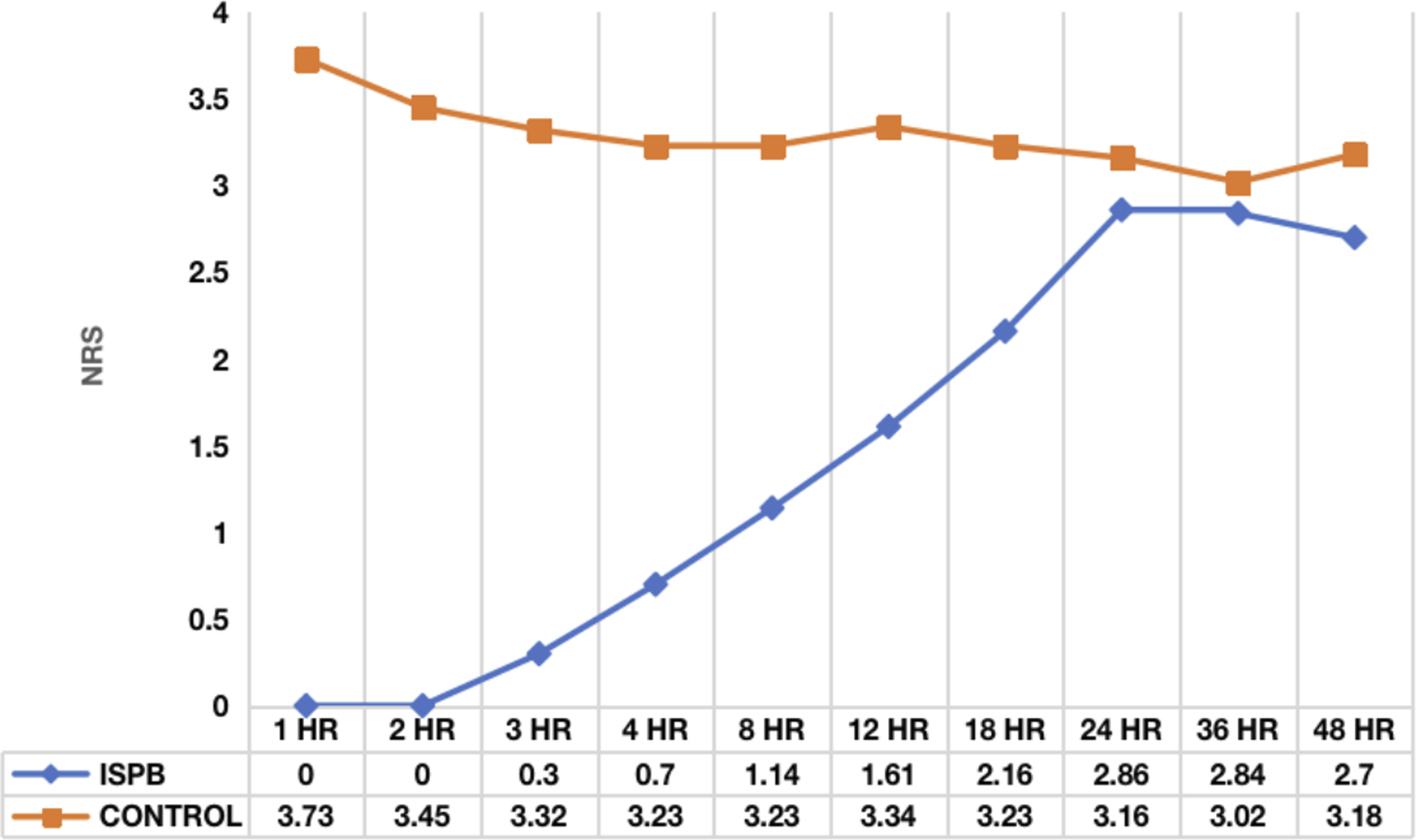
All patients were mobilized as soon as possible based on Grade 4/5 muscle power in both lower limbs. The mean time required to ambulate in neurologically normal cases (42 patients) was 4.30 ± 1.64 hrs, whereas in controls (41 patients), it was 9.48 ± 3.07 hrs, respectively (P < .001). The satisfaction score in the cases (mean value of 9.07 ± .73) was significantly better when compared to the controls (mean value of 7.66 ± 1.09) at the end of 72 hours. Similarly, the mean length of hospital stay in the case group (3.41 ± .69 days) was significantly less when compared to the control group (6.43 ± 1.63 days) (Table 2). Twelve patients in the control group developed severe nausea and vomiting, whereas only two patients in the case group developed nausea and vomiting requiring medication. Postoperative urinary retention requiring bladder catheterization was clinically comparable in both groups (3 in cases and 4 in controls). In all our patients, the block was given by an experienced anesthetist who was quite familiar in all cervical paraspinal blocks. Hence we didnt have any block-related complications in our study population.
Discussion
Our study results highlight that the ISP block provides better postoperative pain relief and is a relatively safe paraspinal cervical block that can be given to elderly patients undergoing cervical laminectomy. In addition, ISP block patients had relatively stable hemodynamic parameters in the intraoperative period, which resulted in less blood loss and hence a shorter surgical time. The total opioid consumption and muscle relaxant used were relatively less in patients who had ISP block intraoperatively.
Postoperative pain following complex spine procedures like cervical laminectomy is generally inadequately treated, with nearly 80% of them experiencing significant postoperative pain, and <50% report having appropriate pain management following surgery. 10 Inadequate postoperative pain management can lead to an increased risk of morbidity and chronic postsurgical pain, as well as longer hospital stays and higher healthcare costs. 11 Postoperative pain management is a laborious endeavour because a variety of patient factors influence the onset and intensity of postoperative pain, with age being among the most significant.12–13
The primary objective of pain management in the elderly is to maximise pain control while minimising the use of opioids, which may lead to adverse outcomes such as postoperative delirium and functional decline in this vulnerable group. 14 Though studies have shown that effective postoperative pain management leads to increased patient satisfaction, early mobilization, decreased complications, shorter hospital stays, and fewer cases of chronic pain syndrome, there is a severe dearth of reliable and efficient analgesic techniques for cervical spine procedures. 15
Multimodal analgesia is considered the ideal approach to controlling postoperative pain following complex spine surgeries, among which epidural analgesia is an important component. 16 Epidural analgesia has proven promising results in thoracic and lumbar spine surgery. In a meta-analysis of 17 randomized controlled studies, Meng et al concluded that epidural analgesia is an effective method for pain relief and can significantly reduce opioid consumption on the first day after surgery when compared to intravenous analgesia. 17 However, studies have demonstrated that neuraxial procedures significantly increase the likelihood of motor block, which might have detrimental effects on postoperative neurological recovery. Moreover, in the cervical spine, there are chances of dural puncture and epidural catheter-related complications such as blockage, displacement, and infection, which may produce drastic consequences.17,18 As a result, its role in cervical spine surgery is uncertain because the accompanying complications and risks outweigh the benefits.
Regional anaesthesia in the form of paraspinal fascial plane block is gaining popularity as a technique of choice for cervical spine surgeries. Since its introduction to clinical practice, the erector spinae plane (ESP) block has been an integral component of multimodal analgesia for a wide variety of thoracic and lumbar spine procedures.19,20 In cervical spine, a recent RCT in 86 patients undergoing posterior cervical spine surgery highlighted that the cervical ESP block can be used as a safe and effective regional technique with good postoperative pain control in elderly patients. 7 However, Elsharkawy et al and Diwan et al have demonstrated that the local anaesthetic drug used in the cervical ESP block has the potential to spread to the phrenic nerve. This can lead to diaphragmatic paralysis, which highlights the possible risk that is associated with the block.21,22
The application of other cervical paraspinal fascial blocks, namely the multifidus cervicis plane (MCP) block and intersemispinal plane (ISP) block, in cervical spine surgery was broadened by Ohgoshi et al. 8 MCP block, a considerably deeper block, entails injecting the local anesthetic agent between the multifidus cervicis and the semispinalis cervicis. On the other hand, ISP block involves injecting the local anesthetic agent in a superficial plane between two semispinalis muscles (S.capitis and S. cervicis). Because the semispinalis capitis fascia limits the craniocaudal extension of spread, an ISP block selectively blocks the medial branches of the dorsal rami of spinal nerves from C4 to T4 without affecting the brachial plexus or the phrenic nerve.23,24 Ohgoshi et al compared the analgesic effects, area of sensory loss, and duration of ISP block vs MCP block in eight healthy volunteers and reported that the ISP block provided effective cervicothoracic analgesia, with the upper border of the anaesthetic area at the C2-C3 level and the lower limit ranging from T1 to T4 level. 9
The main advantage of the ISP block is that, being a superficial plane block, it can be easily mastered and more accurately administered, even in patients with a short neck and a large amount of nuchal pad fat. Moreover, the chances of perforation of the vessels that accompany the dorsal rami branches of cervical nerves are relatively less when compared to the MCP block. As the block is limited by the S. capitis fascia, the cranial extent of the block to the greater occipital and third occipital nerves is relatively rare. Moreover, the lack of action of ISP block on the sympathetic chain and on the phrenic nerve helps to maintain a stable mean arterial pressure and heart rate, as evident in our study results. This has relatively reduced the total surgical time to 128.61 ± 26.08 min in ISPB patients when compared to 160.23 ± 30.99 min in the controls. Hence, the need for additional intraoperative opioids to maintain sedation was drastically reduced, resulting in early postoperative recovery in the ISPB group.
In our study we preferred the use of dexamethasone as an adjuvant to prolong the action of the local anesthetic agent. Dexamethasone induces a degree of vasoconstriction, so that the drug acts by reducing local anaesthetic absorption. Moreover, dexamethasone increases the activity of inhibitory potassium channels on nociceptive C-fibres (via glucocorticoid receptors), thus decreasing their activity and prolonging the duration of analgesia.25,26 Though the optimal dose of dexamethasone as adjuvant is still debatable, we preferred 8 mg, which is the commonly preferred dosage for regional blocks. 27
Though similar studies on ISP block have been published recently, they are limited by the relatively small sample size and lack of data on intraoperative parameters like blood loss, duration of surgery, postoperative mobilization status, and satisfactory score.28,29 The results of our study highlight that ISPB group patients had relatively less blood loss (233.18 ± 66.08 mL) and, in turn, less operative time (128.61 ± 26.08 min) due to stable hemodynamic parameters that were maintained throughout the surgical time. Also, ISPB patients were mobilised earlier, with a mean time of 4.30 ± 1.64 hours following surgery, than the control group due to less postoperative pain and improved alertness. Hence, this cumulative effect of low postoperative pain and early mobilization in our ISPB group resulted in a better satisfactory score and a shorter hospital stay when compared to the controls.
The study has a few limitations. First, the anesthesiologist who administered the block was not blinded to the two groups, incurring the possibility of inherent performance bias. However, the key observations in the operating room were objective measurements (blood loss, surgical duration, and use of opioids). Also, the post-operative documentation of pain and sedation scores was performed by a blind observer. Hence, the risk of observer bias is negligible. Second, the learning curve of this block depends on the experience of the anesthesiologist in regional anesthesia. As the ISP block is a superficial plane block, the time required to expertise this block is relatively less when compared to other deep plane blocks like the erector spinae plane (ESP) block, the multifidus cervicis plane (MCP) block. In our centre, the ISPB block was performed by an experienced anesthesiologist who was quite familiar in all cervical paraspinal blocks. However its safety needs to be addressed in untrained hands. Third, we preferred the use of dexamethasone along with bupivacaine to prolong the analgesic effect of the block which acts by inducing vasoconstriction, as well as by increasing the activity of inhibitory potassium channels on nociceptive C-fibres. Though the optimal dose of dexamethasone is still unclear, we preferred 8 mg, which is the commonly preferred dosage for regional blocks. 27 However the possible adverse effects in terms of infection risk and pseudoarthrosis should be taken into consideration.
Conclusion
We conclude that in patients undergoing cervical laminectomy, USG-guided bilateral ISP block causes a considerable reduction in total opioid consumption during the perioperative period as well as sustained postoperative pain relief. Also, the significant reduction in intraoperative surgical time and total blood loss during surgery makes it an ideal option among cervical paraspinal blocks. Undoubtedly, ISP block can be used as an additional arm in the multimodal analgesic strategy for elderly patients undergoing cervical laminectomy because of its proven safety and efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Appendix
Score
Sedation level
Responsiveness
Speech
Facial expressin
Eyes
5
Alert
Responds readily to name
Normal
Normal
Clear, no ptosis
4
Light
Lethargic response to name
Mild slowing
Mild relaxation
Glazed or mild potsis
3
Moderate
Response only after name is called loudly
Slurring or prominent slowing
Marked relaxation
Glazed and marked ptosis
2
Deep
Response only after mil shaking
Few recognizable words
-
-
1
Deep sleep
Response only after
-
-
-
S.no
Questions
Points
1
Whether pain is tolerable?
1
2
Able to get a sound sleep?
1
3
Interest in social talks with attendants?
1
4
Difficulty in taking oral liquids and solids?
1
5
Nausea and vomiting?
1
6
Difficulty in passing urine?
1
7
Difficulty in passing stools?
1
8
Difficulty in mobilization?
1
9
Feeling positive about the recovery?
1
10
Overall satisfaction is there or not?
1
Total score
10