
Abstract
Study Design
Prospective, randomized controlled double-blinded study.
Objective
To compare the relative efficacy of ultrasound-guided ESPB and CEB for postoperative analgesia after a single-level lumbar fusion surgery and compared it with conventional multimodal analgesia.
Methods
81 patients requiring single-level lumbar fusion surgery were randomly allocated into 3 groups (ESPB group, CEB group, and the control group). Demographic and surgical data (blood loss, duration of surgery, perioperative total opioid consumption, muscle relaxants used) were assessed. Postoperatively, the surgical site pain, alertness scale, satisfaction score, time to mobilization, and complications were recorded.
Results
The total opioid consumption in the first 24 hours was significantly lower in both the block groups than in the control group (103.70 ± 13.34 vs 105 ± 16.01 vs 142.59 ± 40.91mcg; P < .001). The total muscle relaxant consumption was also significantly less in block groups compared to controls (50.93 ± 1.98 vs 52.04 ± 3.47 vs 55.00 ± 5.29 mg; P < .001). The intraoperative blood loss was significantly less in both the block group (327.78 ± 40.03 mL, 380.74 ± 77.80 mL) than the control group (498.89 ± 71.22 mL) (P < .001). Among the block groups, the immediate postoperative pain relief was better in the CEB group, however, the ESPB group had a longer duration of postoperative pain relief.
Conclusion
Both ESPB and CEB produce adequate postoperative analgesia after lumbar fusion however the duration of action was significantly longer in the ESPB group with relatively shorter surgical time and lesser blood loss compared to the CEB group.
Keywords
Introduction:
Lumbar fusion is a major surgery resulting in significant acute post-operative pain which in turn is one of the key factors to influence the outcomes postsurgically.1,2 Achieving adequate postoperative pain relief encourages early mobilization and optimal rehabilitation thereby reducing pulmonary, and thromboembolic complications and chronic pain syndromes.3,4
Multimodal analgesia, which acts on various pain signaling mechanisms, is increasingly used as the standard of care to produce additive or synergistic benefits. Opioids are the mainstay of perioperative analgesia; however, the current trend in perioperative pain management has moved the emphasis to non-opioids, which constitute the majority of the multimodal analgesic regimen, in order to reduce opioid-related adverse effects.5,6 Furthermore, the ongoing rise in spine surgery warrants future research into the clinical and financial burden of pain management to improve functional outcomes.7,8
The role of preemptive analgesia in preventing central sensitization and postoperative morbidity in patients undergoing spine surgery has been well documented by previous studies.9,10 Sekar et al highlighted that in lumbosacral spine procedures, medications given in the caudal block before to surgical incision provide effective preemptive analgesia by adhering to the nerve roots, inhibiting CNS plasticity, and extending analgesia 10 A novel technique of regional anesthesia known as the erector spinae plane (ESP) block involves injecting local anesthetics into the space between the vertebral transverse process and the deep fascia of the erector spinae muscle. This block may affect the dorsal rami of spinal nerve, and it is a desirable regional anesthesia technique for spinal fusion surgery since it is secure and simple to carry out while using ultrasound to identify bone landmarks. It was initially used in spinal fusion surgery as a component of a multimodal anesthetic regimen, and it was found to reduce or even completely remove the requirement for opioids. A recent RCT by Goel et al highlighted the beneficial effects of ESPB block in patients undergoing lumbar fusion surgery. They reported a significant reduction in postoperative total opioid consumption for the first 24 hours in patients who had blocks compared to those without blocks. 11
Studies have shown that both caudal epidural block (CEB) and erector spinae plane block (ESPB) are effective in lowering pain and opioid consumption after lumbar surgery. To the best of our knowledge, there are no studies comparing these two blocks. So, we conducted a double-blinded randomized controlled trial to compare the postoperative opioid consumption as well as postoperative analgesics efficacy of these two blocks.
Materials and Methods:
This study was conducted in a tertiary spine care center following the approval of the institutional review board (Ganga Medical Centre & Hospital Pvt Ltd Institutional Review; IRB Application No: 2022/07/12) and the study has been registered in the clinical trial registry (CTRI/2022/08/045117). It is a prospective, randomized controlled double-blinded study, where written consent was obtained from all the patients included in the study. Patients more than 20 years of age undergoing single-level lumbar fusion surgery (TLIF) for degenerative listhesis/lytic listhesis or lumbar canal stenosis with instability were included in the study. Patients with a bleeding disorder, local/systemic infection, lumbar spine injury, tumors, revision spine surgery, and those patients who refused to give consent were excluded from the study.
Based on the exclusion criteria 4 were excluded out of 85 patients and the remaining 81 patients were randomized using computer-generated numbers into the ESPB group, CEB group, and the control group. The allocation details of the study have been represented using the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting randomized trials (http://www.consort-statement.org/) - [Figure. 1]. All patients were given 75 mg Pregabalin and 1 gm Acetaminophen the previous night of surgery and induction for surgery was done by standard general anesthesia technique CONSORT flow diagram.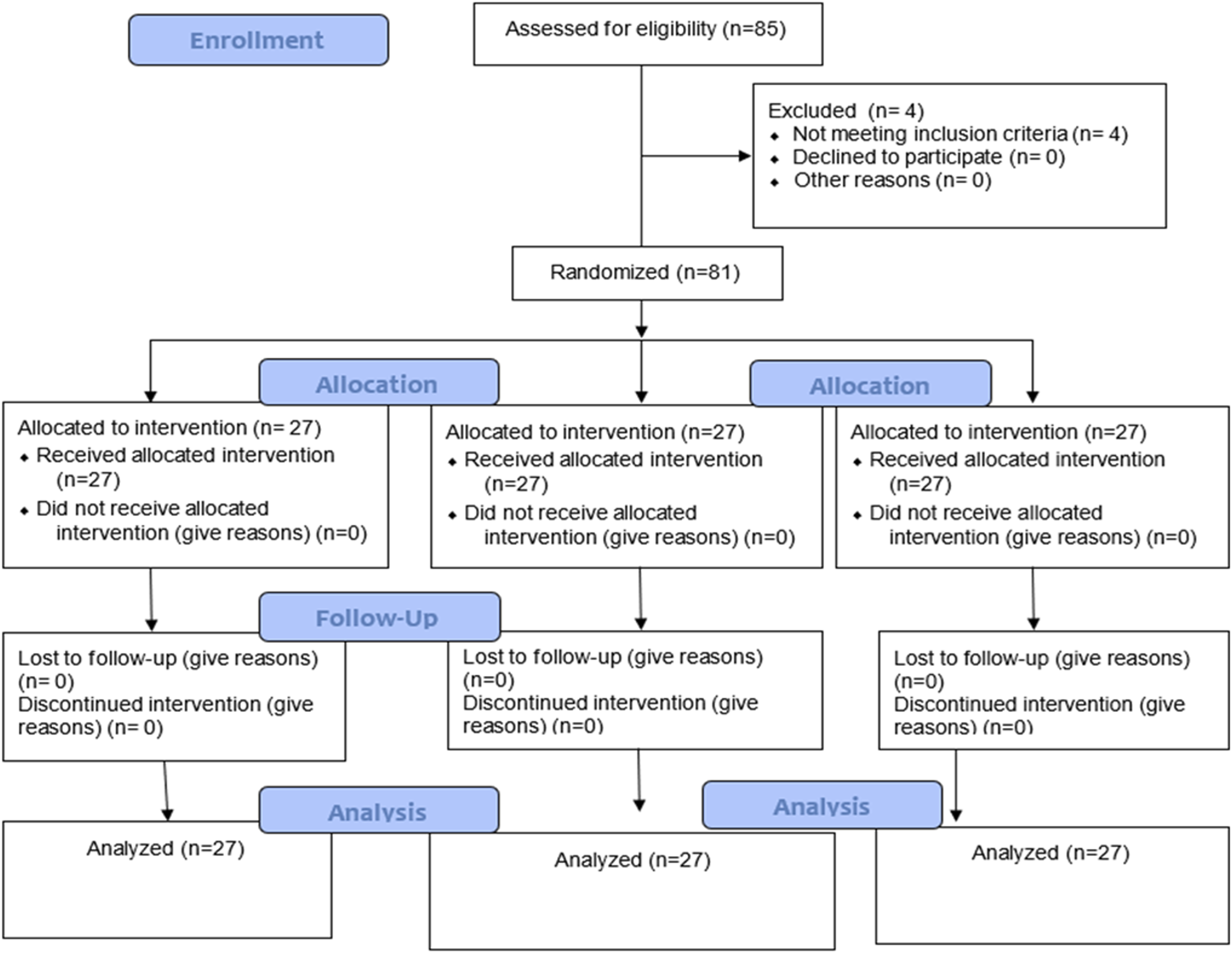
Patients were randomly allocated to one of the 3 groups. Senior anesthetists with more than 5 years of experience performed the blocks.
After skin preparation and draping, the surgery was performed in standard fashion by a single senior spine surgeon with 25 years of experience in performing spine surgeries. The total consumption of Fentanyl and muscle relaxant (Rocuronium) was documented throughout the surgery. Intraoperative opioid and muscle relaxant consumption, amount of blood loss as well as the duration of surgery were documented
All of the patients received postoperative analgesia in the form of 1g paracetamol administered intravenously every 8 hours and 75 mg of pregabalin taken once daily. A fentanyl infusion was given for breakthrough pain, and the total amount of Fentanyl administered was recorded. Postoperative parameters such as Numeric Rating Scale, Modified observer's alertness/sedation score (MOASS) [Appendix 1], mobilization time, the total opioid consumed (TOC), and all complications were recorded by two fully trained physician assistants unaware of the randomization. The total satisfaction score was obtained for all the patients at the end of 72 hours post-surgery (Appendix 2).
Statistical Analysis
The sample size was calculated based on the assumption that the drug Fentanyl had at least 70 percent analgesic effect on the testing population and >95% effect on the general population. With 95% CI; 80% power, the ratio of unexposed/exposed 1:1, with odd’s ratio of 2.5 and risk of 1.7, the sample size estimated for this trial was 60 with 20 patients in each group. To improve the strength of the study and to compensate for potential dropouts, we evaluated 30% more patients in each group. Data were analyzed using SPSS v21. Unpaired t-tests were used to analyze continuous variables and the Chi-square test or Fisher’s exact test was used to analyze categorical variables. One-way ANOVA test was used as the test of significance for comparison between groups for continuous data and LSD test was used for post-hoc analysis. P-value <.05 was considered significant statistically.
Results:
Demographic and Clinical Characteristics of the Groups.
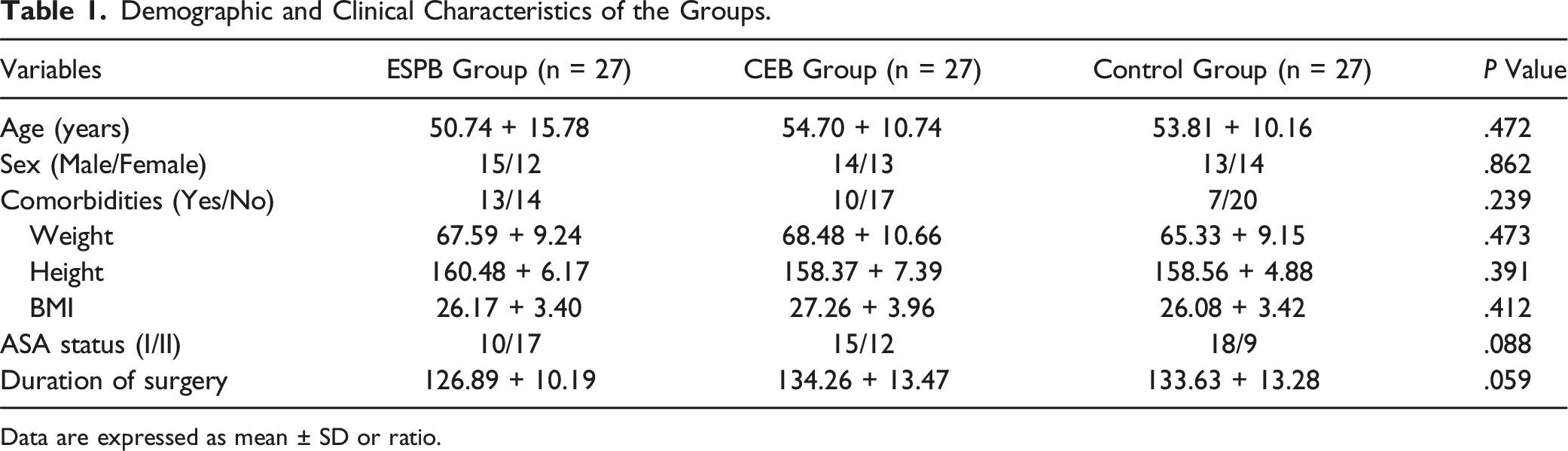
Data are expressed as mean ± SD or ratio.
Intra-operative Parameters:
Primary and Secondary Outcome Parameters.
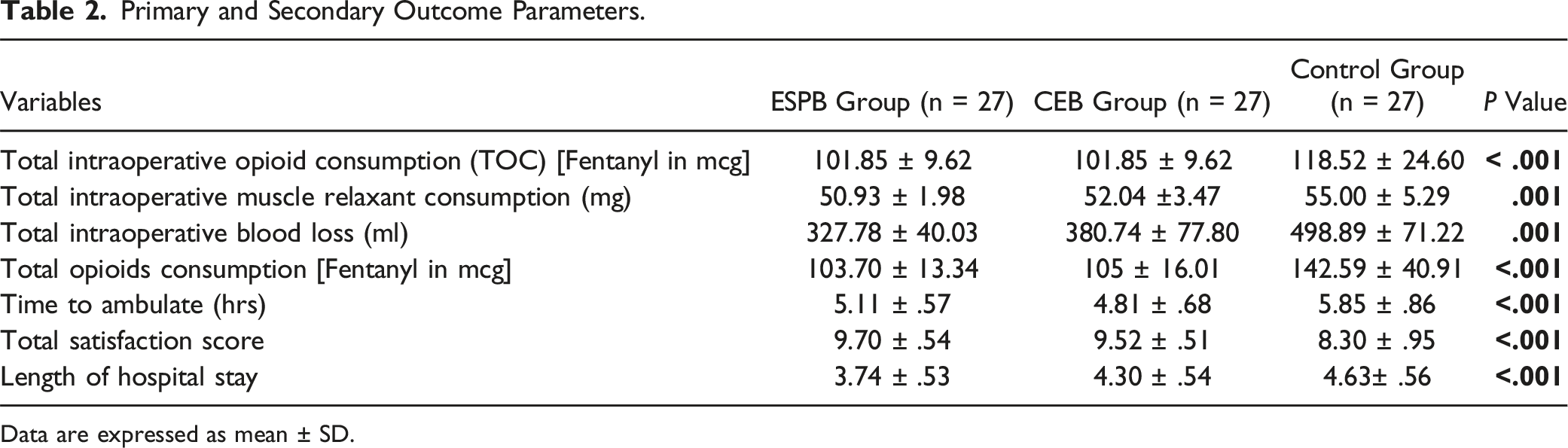
Data are expressed as mean ± SD.
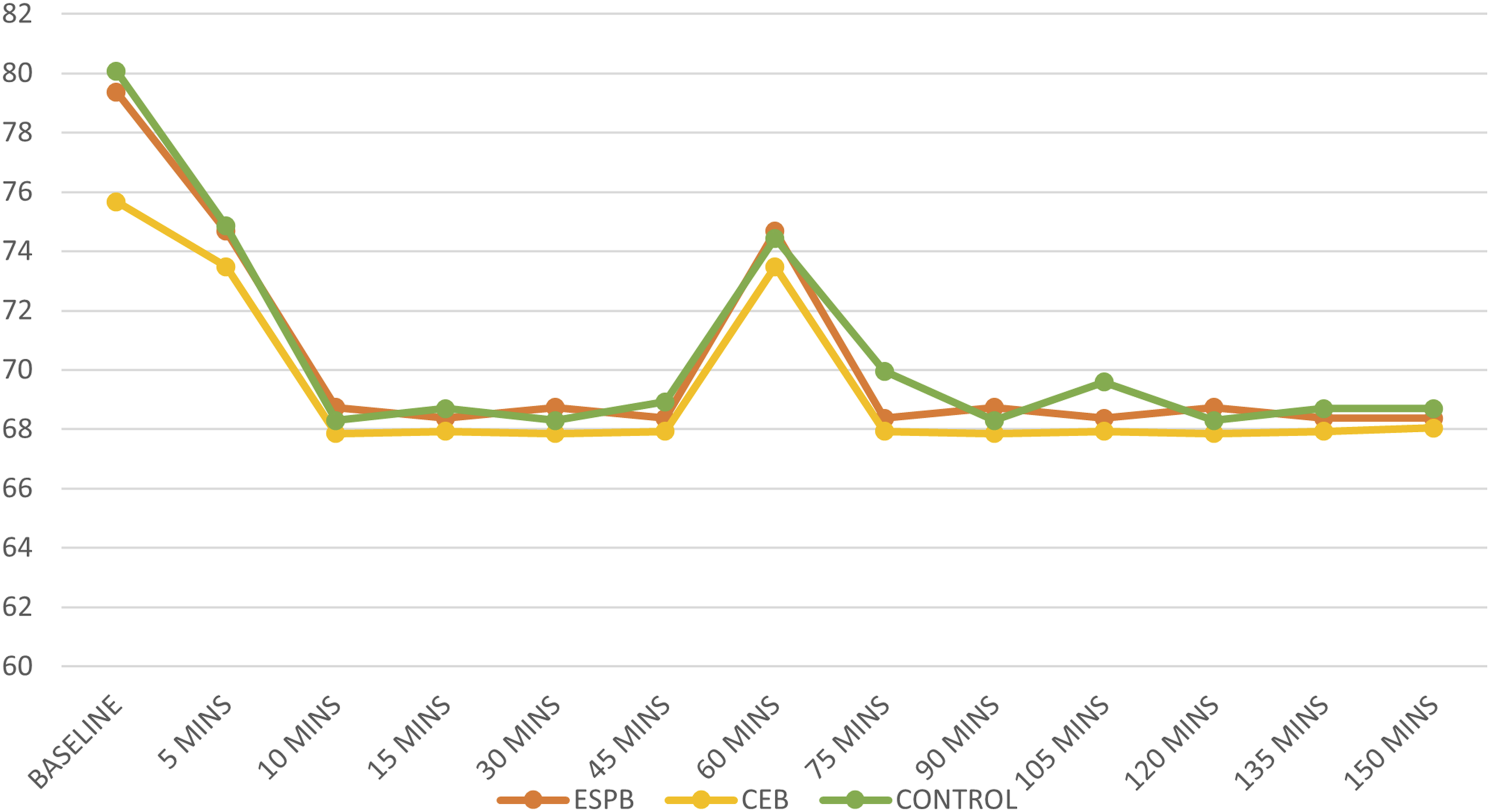
Comparison of intraoperative heart rate between 3 groups.
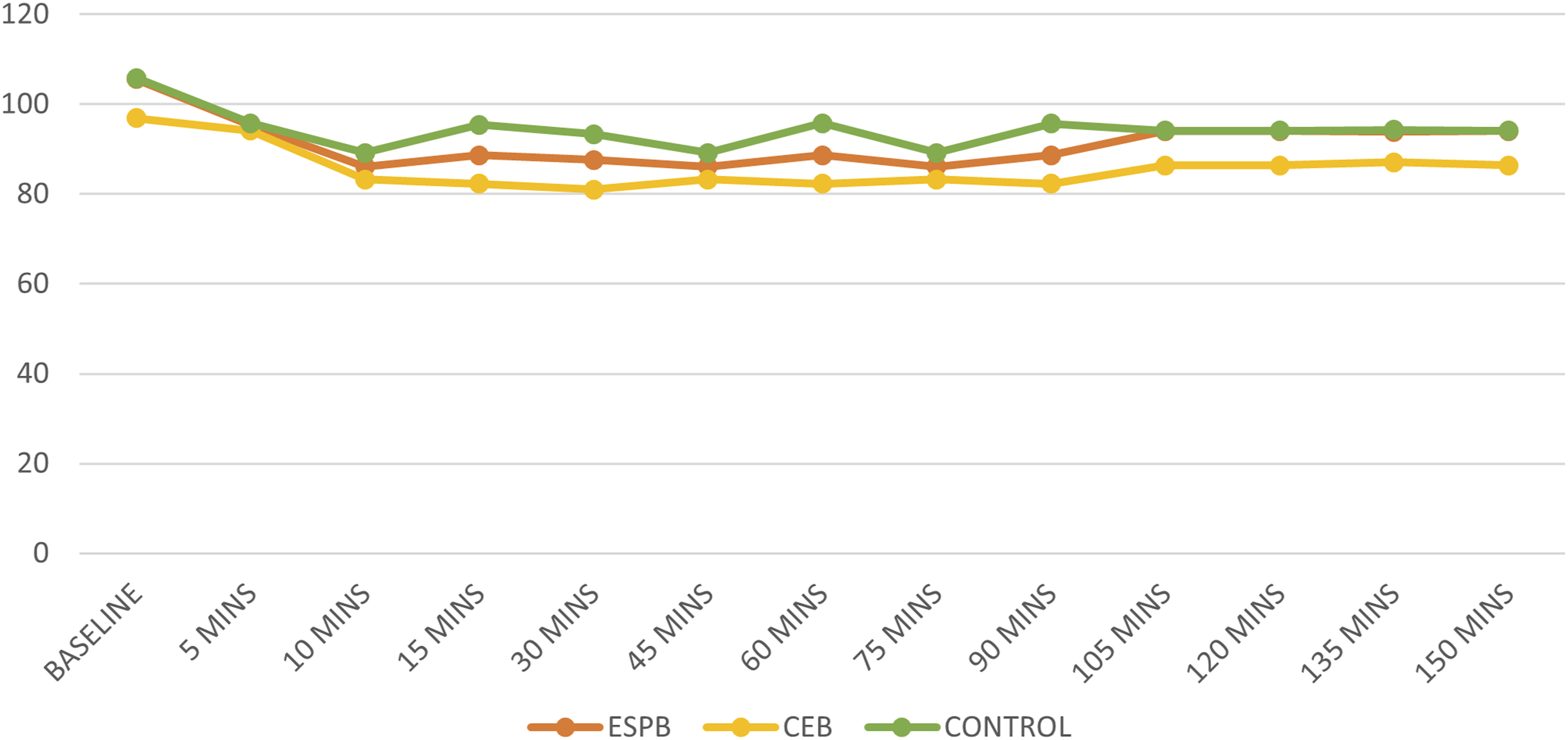
Comparison of intraoperative mean arterial pressure between 3 groups.
Post-operative Parameters:
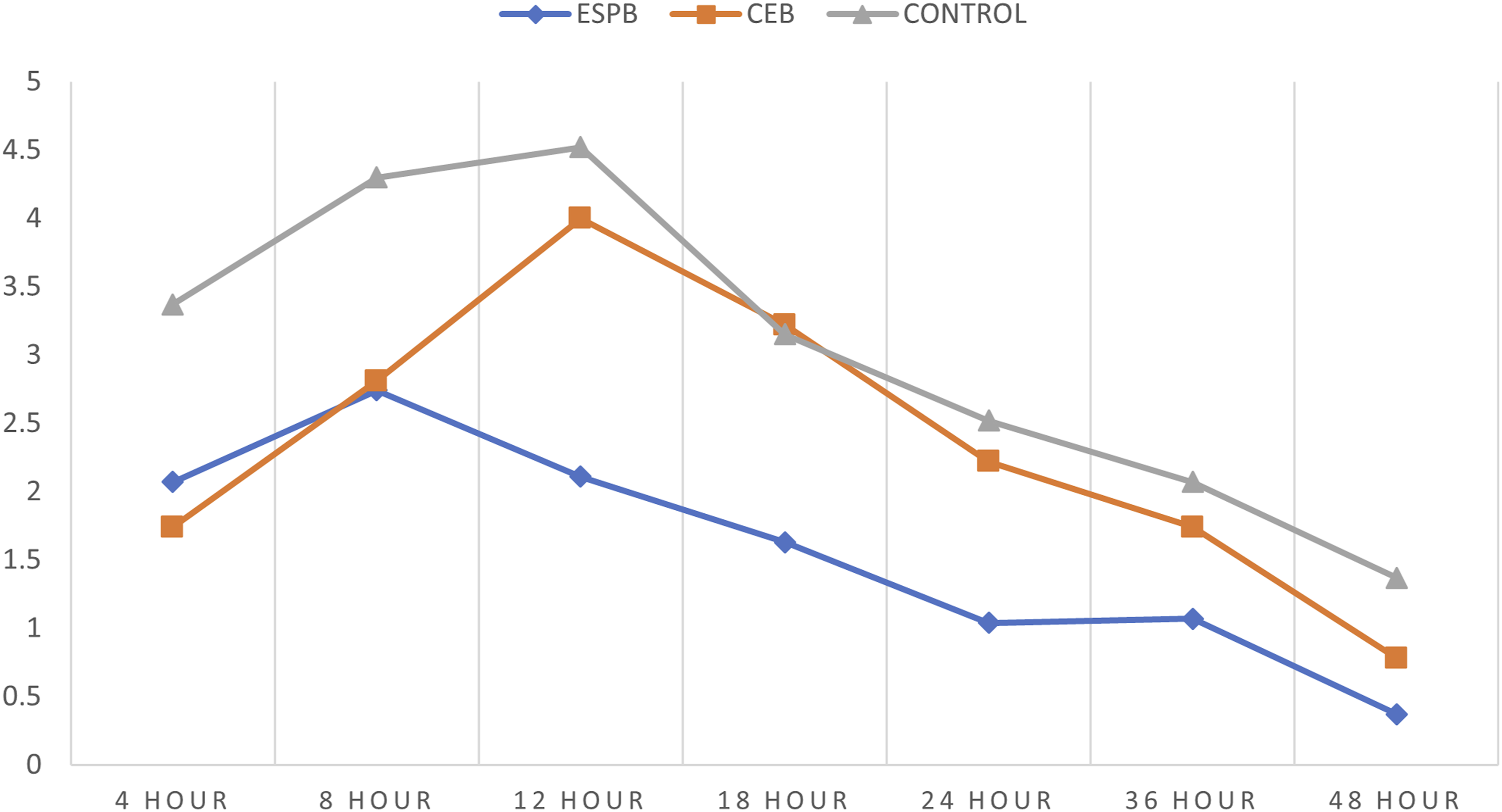
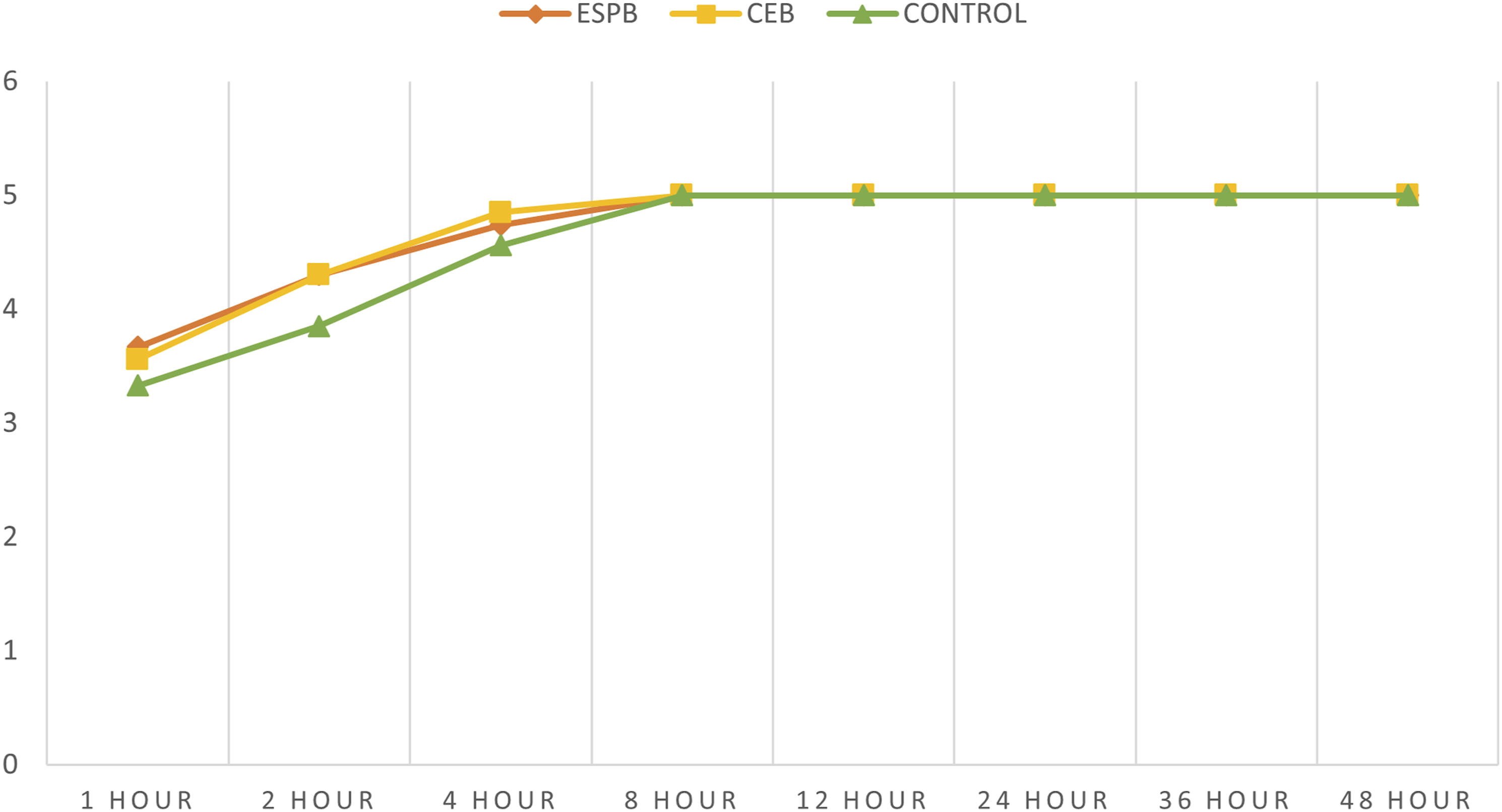
In the first 48 hours after surgery, the control group had a considerably greater postoperative pain score (NRS) compared to the block groups (Figures 4,5). Among the block groups, the immediate postoperative pain relief was better in the CEB group than the ESPB group. However, the ESPB group had a longer duration of postoperative pain relief than the CEB group. The MOASS score at 1,2 and 4 hours was significantly less in the control group when compared to the block groups indicating decreased alertness presumably due to higher opiate usage in controls (Figure 6). Comparison of NRS (at rest) between the 3 groups. Comparison of NRS (at movement) between the 3 groups. Comparison of MOASS between the 3 groups.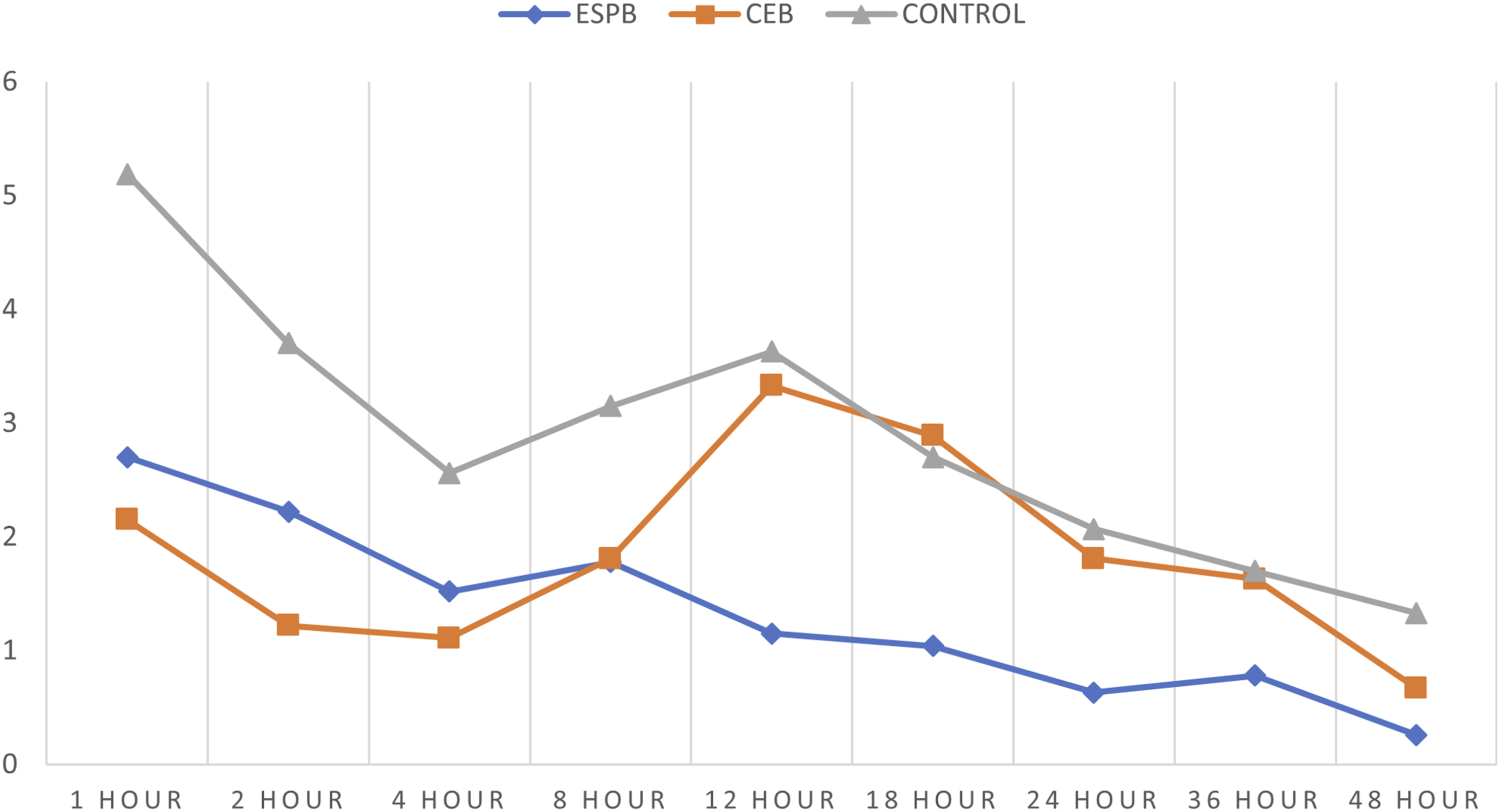
The mean time required to ambulate was 5.11 ± .57 hrs (ESPB group) and 4.81 ± .68 hrs (CEB group) whereas, in controls, it was 5.85 ± .86 hrs respectively (P < .001). The satisfaction score in the ESPB group (mean value of 9.70 ± .54) and CEB group (mean value of 9.52 ± .51) was significantly better when compared to controls (mean value of 8.30 ± .95) at the end of 72 hrs. Similarly, the mean length of hospital stay in the ESPB group (3.74 ± .53 days) and CEB group (4.30 ± .54 days) was significantly less when compared to the control group (4.63 ± .56 days) (Table 2).
Seven patients in the control group developed severe nausea and vomiting, whereas only 2 patients in the block groups developed nausea and vomiting requiring medication. Postoperative urinary retention requiring bladder catheterization was clinically comparable in all groups (3 in ESPB, 3 in CEB, and 4 in controls). We did not encounter any block-related complications in any of our patients
Discussion:
To the best of our knowledge, our study is the first randomized controlled double-blinded trial comparing the relative efficacy of the ESPB and CEB for postoperative analgesia in patients undergoing single-level lumbar fusion surgery. Our study highlights that the total opioid consumption was significantly reduced by both blocks in the initial 24 hrs following surgery. Also, both block groups had considerably lower postoperative pain scores than the control group.
In a large cohort study, involving 115,775 individuals who underwent 179 different surgical procedures, spinal fusion surgery patients experienced the most severe postoperative pain. 12 Hence effective postoperative pain management promotes early mobilization and patient satisfaction, prevents the onset of pulmonary and thromboembolic complications, and lowers postoperative mortality and morbidity. As per the literature, the most commonly used method for the management of postoperative pain following lumbar fusion surgery is opioid-based patient-controlled intravenous analgesia. 13 However, the adverse effects of opioids range from minor ailments like nausea, vomiting, and hypotension to severe side effects like unconsciousness and respiratory depression. Therefore, in terms of analgesic planning, regional applications are more rational than a drug that can have systemic effects. This goal has been served by the use of epidural, spinal, and the recently popular plane blocks.
The role of the pre-incisional caudal epidural block as preemptive analgesia in lumbar spine surgery was studied by Kakiuchi et al where the author reported significantly less analgesics requirement in the initial 12 hours in patients with CEB. 14 Similar to the previous study, Sekar et al demonstrated that the caudal epidural block with the combination of bupivacaine and tramadol provides a relatively pain-free postoperative period following lumbar discectomy. 10 The prone position used for the lumbar fusion surgery is the best one to access the caudal epidural region. The precise placement of the hypodermic needle in the caudal epidural space can be successfully confirmed by using ultrasound or image intensifiers, which are easily accessible at the time of these surgeries.15,16
Targeted fascial plane nerve blocks have recently been shown to improve peri-operative analgesia in posterior spine procedures. Anatomically, the dorsal rami of nerve roots at each spinal segment supply the pain-producing nociceptors in the posterior surgical site, including the skin, fascia, paraspinal muscles, and periosteum. The dorsal rami, which emerges from the neural foramen, travels through the transverse process and enters the erector spinae to innervate the pain generators of the posterior spine. 17 The erector spinae plane block (ESPB) involves injecting a significant volume of long-acting local anesthetic solution into the fascial plane between the transverse process and erector spinae to block the dorsal rami. Effective perioperative analgesia for lumbar and thoracic spine surgeries has been made possible by ESPB, which was first developed to treat chronic thoracic neuropathic pain. 18
The results of this study highlight that the regional anesthesia technique (ESPB and CEB) results in much longer postoperative analgesia and significantly lower total opioid use in the first 24 hours after surgery. The study results highlighted that among the block groups, immediate postoperative pain relief during the first 4 hours of post-surgery was better in the CEB group than the ESPB group. However, the ESPB group had a longer duration of postoperative pain relief than the CEB group. This can be substantiated by the fact that the caudal epidural block involves the injection of a local anesthetic drug into the epidural space through the sacral hiatus. Drugs injected act directly on spinal nerves and receptors in the spinal cord due to diffusion across the dura and CSF thereby effectively preventing the perception of a nociceptive stimulus. Later as the drug enters systemic circulation the action of CEB wanes out. Moreover, we preferred only .25% ropivacaine without any adjuvants which might also be contributing factor for the shorter duration of action. A 20-30 mL caudal injection of local anesthetics (bupivacaine and ropivacaine, .166% to .376%) with or without adjuvants has been shown to greatly reduce the need for postoperative analgesics in lumbar fusion surgery. However, adjuvants such as buprenorphine (.1 mg), tramadol (50 mg), ketamine, dexamethasone (8 mg), and dexmedetomidine (1 g/kg) have been reported to have good beneficial effects19-21 In ESPB, injecting the local anesthetic deep into the erector spinae prevents the washout of the drug during the surgical procedure unlike in CEB, which improves the quality and length of analgesia for a longer duration of time. Multiple studies have shown that injected local anesthetics used in ESPB reach the paravertebral spaces, leading to blockage of the dorsal rami, ventral rami, and sympathetic chain.22,23 This could be a contributing factor to the longer action of the ESPB.
Our study's findings show that the ESPB group's surgical time (126.89 ± 10.19 min) and blood loss (327.78 ± 40.03 mL) were significantly less than those of the CEB group (134.26 ± 13.47 mins, 380.74 ± 77.80 mL) and the control group (133.63 ± 13.28 mins, 498.89 ± 71.22 mL). In the ESPB group, ropivacaine that is injected in the erector spinae plane spreads to block the sympathetic chain, dorsal rami, and ventral rami. A local anesthetic injected into the dorsal rami blocks the transmission of pain signals from the skin and the posterior nociceptors. This allows the surgeon to execute a precise dissection without having to provide a large dose of opioids or a deep anesthetic plane. Hemodynamic stability is another benefit of reduced nociceptive stimulus. Intraoperative blood loss has been demonstrated to be lower in the ESPB group, which may be attributable to the combination of sympathetic blockade and pre-emptive analgesia given before to real tissue damage. Hence the clean surgical field and hemodynamic stability may have contributed to the reduction in surgical time.
The fact that our study is a prospective, randomized, double-blinded clinical trial with a robust methodology of randomization into 3 groups that have comparable demographic and surgical features is one of its main strengths. Additionally, our study has addressed intra-operative factors such as blood loss, muscle relaxant dosage, and operation time. We were also able to precisely assess the intraoperative and postoperative study parameters due to strict adherence to anesthetic and pain management protocols with no deviations. Moreover, we did not observe any block-related complications in our study groups.
The study has a few limitations. First, the sample size is relatively small, and hence a larger sample with longer follow-up would strengthen the results and enhances the clinical findings of the study. There is a chance of intrinsic performance bias because the anesthesiologist who gave the block was not blind to the two groups While we did see a statistically shorter surgical time (incision to closure), the additional 10-15 minutes needed to execute the block should be taken into account by the surgical team.
Conclusion:
Both ESPB and CEB produce adequate postoperative analgesia following lumbar fusion surgery and may be utilised as adjunctive arms in multimodal analgesia. However, the duration of the postoperative analgesic effect was significantly longer in the ESPB group with relatively shorter surgical time and lesser blood loss compared to the CEB group.
Supplemental Material
Supplemental Material - Comparison Between Relative Efficacy of Erector Spinae Plane Block and Caudal Epidural Block for Postoperative Analgesia in Lumbar Fusion Surgery- A Prospective Randomized Controlled Study
Supplemental Material for Comparison Between Relative Efficacy of Erector Spinae Plane Block and Caudal Epidural Block for Postoperative Analgesia in Lumbar Fusion Surgery- A Prospective Randomized Controlled Study by Yogin Patel, Karthik Ramachandran, Ajoy Prasad Shetty, Sekar Chelliah, Rishi Mugesh Kanna, and Rajasekaran Shanmuganathan
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.