
Abstract
Study Design
A retrospective study.
Objectives
This study aimed to investigate the impact of cervical kyphosis on patients with cervical spondylotic myelopathy (CSM) following selective laminectomy (SL) regarding posterior spinal cord shift (PSS), and a number of SLs.
Methods
We evaluated 379 patients with CSM after SL. The patients with kyphosis (group K) were compared with those without kyphosis (group L). Moreover, groups K and L were divided into subgroups KS and KL (SLs ≤ 2) and LS and LL (SLs ≥ 3), respectively, and analyzed. Receiver operating characteristic (ROC) curve analysis was performed to determine the cut-off value of the C2–C7 angle for satisfactory surgical outcomes, which was defined as a Japanese Orthopaedic Association (JOA) recovery rate of ≥50% in group KS.
Results
The average PSS (mm) in group K was smaller than that in group L (.8 vs 1.4; P < .01), but the JOA recovery rate was comparable between the 2 groups. Meanwhile, the mean PSS and JOA recovery rate (%) in group KS was lower than those in group KL, respectively (.3 vs 1.0; P < .01, 35.1 vs 52.3; P = .047). Moreover, the average PSS of group KS (.6) was smaller than those of other subgroups ( < .01). In addition, the ROC curve analysis showed that the C2–C7 angle of −14.5° could predict satisfactory surgical outcomes in group KS.
Conclusion
Selective laminectomy is not contraindicated for patients with kyphosis, but a larger number of SLs may be indicated for the patients with C2–C7 angles of ≤ −14.5°.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is essentially caused by age-related degeneration, which leads to spinal cord dysfunction and impairment.1,2 Because CSM is thought to be a progressive disease, patients with moderate or severe CSM frequently require surgical interventions.1,2 Among them, cervical posterior decompression surgeries without fixation, including open-door laminoplasty, 3 double-door laminoplasty, 4 and selective laminectomy (SL) with muscle preservation, 5 are widely used because of satisfactory surgical outcome with simple surgical procedure.
In contrast, several studies indicated that preoperative cervical kyphosis worsens outcomes of posterior decompression surgery by (1) insufficient decompression at the anterior aspect of the spinal cord with reduction of posterior spinal cord shift (PSS)6,7 and (2) vulnerable nature of the spinal cord by increased intramedullary pressure8-10 and reduced artery filling. 11 However, the clinical impact of preoperative cervical kyphosis on neurological recovery after posterior decompression surgery has been controversial and is at least partially due to the smaller number of subjects in previous studies.6,7,12-14 Meanwhile, SL is reported to limit a number of decompression laminae to reduce invasion of the posterior structure, 5 but the limitation may worsen surgical outcomes with a reduction in the amount of PSS especially for the patients who have kyphosis.7,15 Nevertheless, to the best of our knowledge, no studies investigated the clinical feature of preoperative cervical kyphosis in patients with CSM after SL. Thus, we conducted a retrospective study on 379 patients with CSM who underwent SL to identify the impact of preoperative kyphosis on myelopathy; this has been the largest series investigating the clinical impact of kyphosis after decompression surgeries reported to date.
This study aimed to analyze the impact of cervical kyphosis on surgical outcomes for patients with CSM after SL.
Materials and Methods
Patient Population and Selection
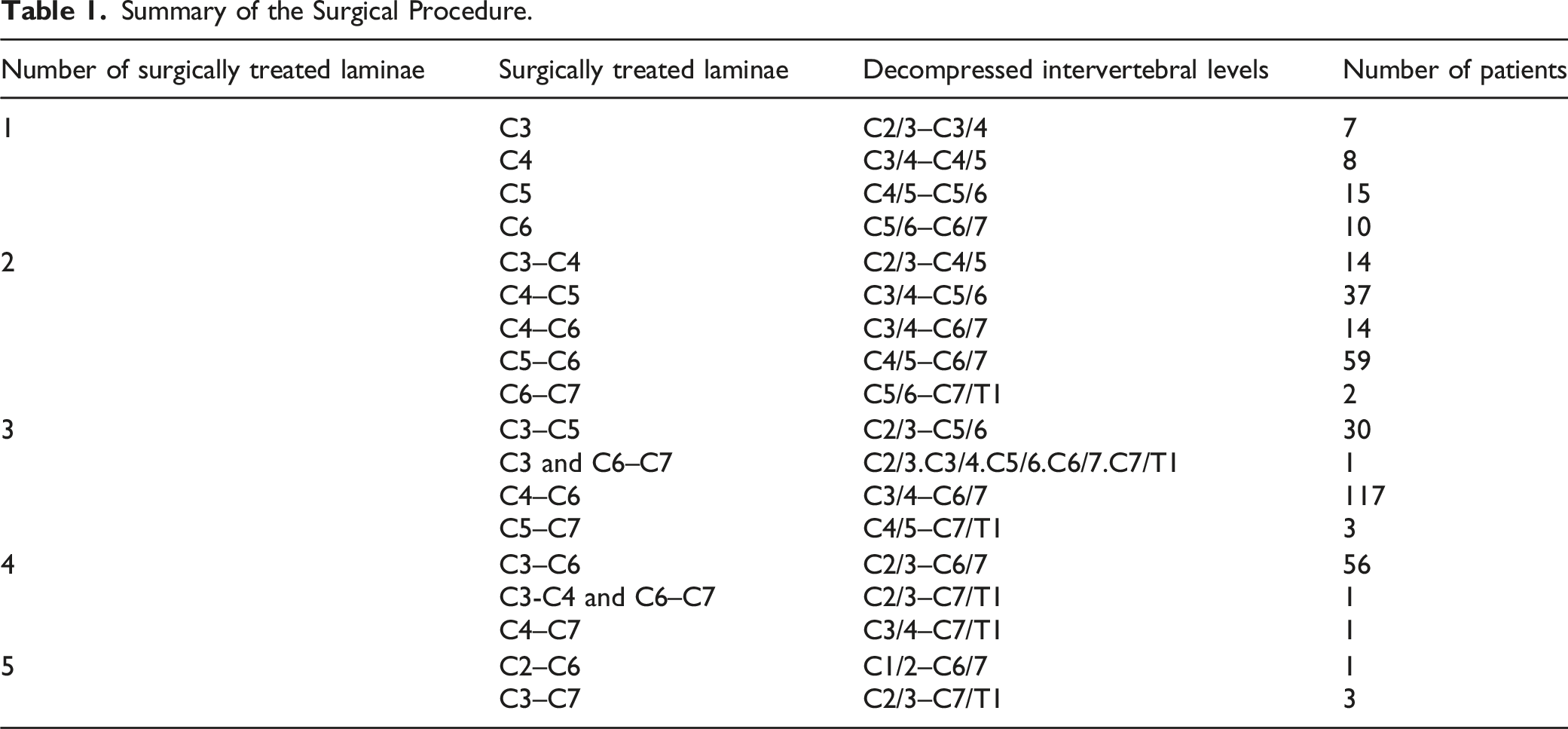
Summary of the Surgical Procedure.
Surgical Procedure
Before surgery, decompression levels were established via complete obstruction of the subarachnoid space using preoperative magnetic resonance imaging (MRI) or computed tomography following myelography. 16 Surgical technique of the procedure is described elsewhere.5,16 An operating microscope was used throughout the SL. The surgical technique used for C4–C5 SL was as follows: The nuchal fascia was divided in line with the midline skin incision. Subsequently, the C3/4, C4/5, and C5/6 interlaminar spaces were exposed. Using a high-speed drill, the C4 and C5 spinous processes were split longitudinally and divided at the base without disturbing the bilateral deep extensor muscles. The C4 and C5 laminae, upper half of the C6 lamina, and yellow ligament of the ventral aspect of the C3 lamina were removed. Thus, decompression was accomplished in 3 adjacent levels (C3/4, C4/5, and C5/6).
Patient Demographics and Clinical Assessment
Patients’ demographics, including sex, age, and body mass index, preoperative symptom duration, and presence of diabetes mellitus were investigated. Preoperative neurologic statuses were evaluated using the Japanese Orthopaedic Association (JOA) scoring system. Postoperative neurologic statuses were also evaluated using the JOA score at the final follow-up period, and neurological recovery was assessed by the JOA scoring system, which was calculated as follows: recovery rate (%) = (postoperative JOA score–preoperative JOA score) × 100/(17–preoperative JOA score). 18
Radiographic Assessment
The following radiographic parameters were measured in the neutral position on a standing lateral radiograph (Figure 1)19,20: (1) C2–C7 angle, which was the Cobb angle from the lower endplate of C2 to the lower C7; (2) C2–C7 sagittal vertical axis (C2–C7 SVA), which was the distance between a plumb line dropped from the centroid of C2 and posterior superior aspect of C7; and (3) C7 slope, which was the angle between the superior end plate of C7 and horizontal line. Among the described radiographic parameters, the C2–C7 angle was measured in flexion and extension and in neutral position. The range of motion was defined as the difference in C2–C7 angle at flexion and extension. The kyphosis was defined as preoperative C2–C7 angle <0° in neutral position.6,21-24 The presence of preoperative spinal cord signal change was evaluated using T2-weighted sagittal MRI.
6
The magnitude of PSS was determined as the difference between the preoperative and final follow-up posterior disc to anterior border of the spinal cord distances at C4/5 using postoperative T2-weighted sagittal MRI.
16
Meanwhile, 20 cases (5.3%) did not include C4/5 level among decompression levels; therefore, they adopted other levels closed to C4/5 level among decompression levels, such as C3/4 level (N = 7) and C5/6 level (N = 13), to measure PSS. Illustration of radiographic parameters: (A) C2–C7 angle, (B) C2–C7 sagittal vertical axis, and (C) C7 slope.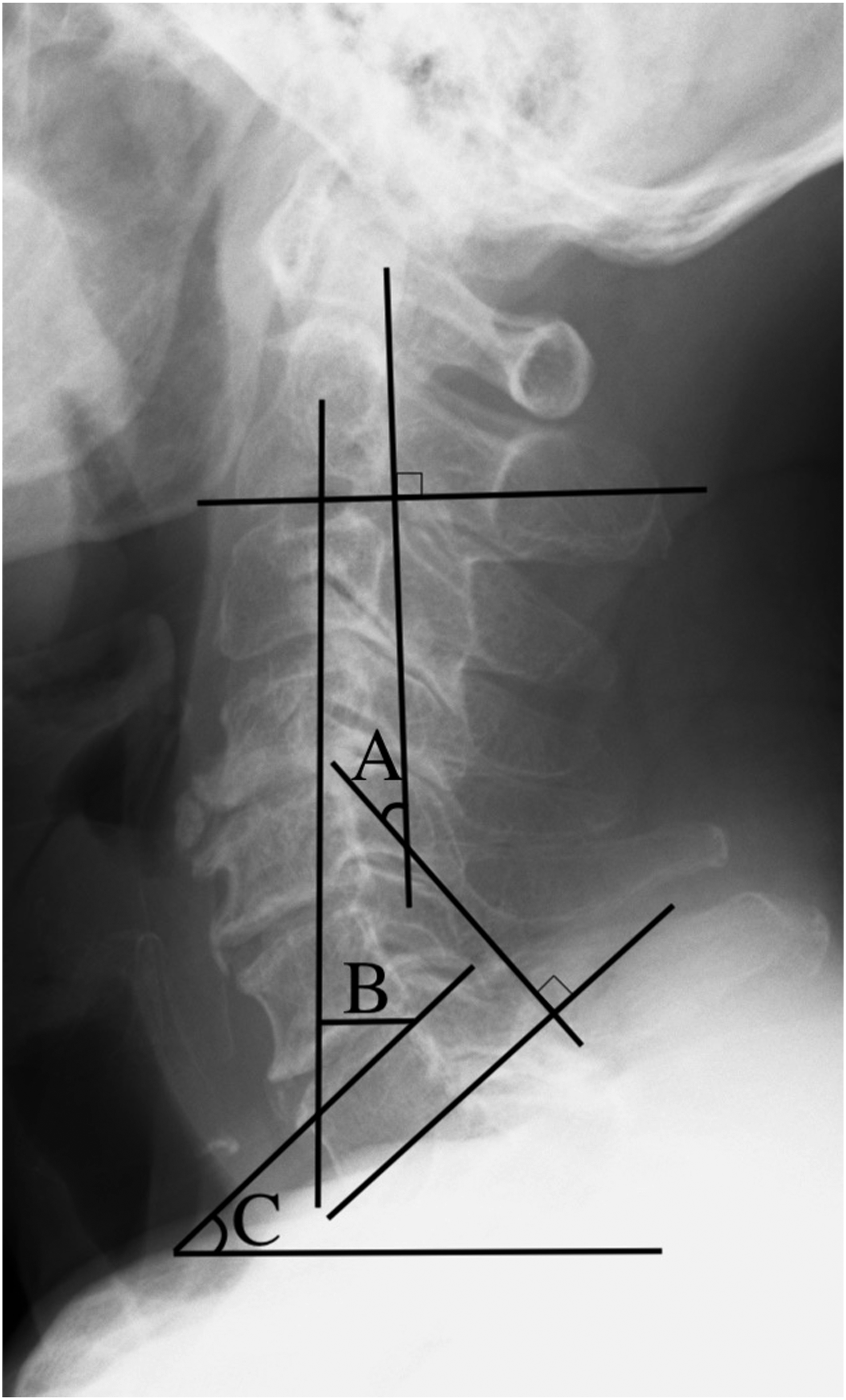
Comparative Analyses
Enrolled patients who had and did not have kyphosis were assigned to groups K and L, respectively. Moreover, two other groups were created with regard to a number of laminectomies in groups K and L, respectively. In group K, patients who underwent a smaller number of SLs, such as one and two, and those who underwent a larger number of SLs, such as three, four, and five, were assigned to groups KS and KL, respectively. Similarly, in group L, patients who underwent a smaller number of laminectomies, such as one and two, and those who underwent a larger number of laminectomies, such as three, four, and five, were assigned to groups LS and LL, respectively. Comparison analyses of demographic, radiographic, and clinical variables were performed between groups K and L, groups KS and KL, and groups LS and LL. In particular, to exclude confounders between groups KS and KL, univariate and multivariate logistic regression analyses were performed for the two groups.
Receiver Operating Characteristic Curve Analysis
A receiver operating characteristic (ROC) curve analysis was performed to investigate a surgical indication for a smaller number of laminectomies (1 or 2) so that patients having cervical kyphosis can obtain satisfactory surgical outcomes. A satisfactory surgical outcome was defined as a JOA recovery rate exceeding 50%. 6
Statistical Analysis
SPSS Statistics version 22.0 (IBM Corp, Armonk, New York) was used to perform statistical analyses. Student’s t-test and chi-square test were performed for univariate analysis between the two groups. One-way analysis of variance (ANOVA) was used to determine the statistical differences of the amount of PSS among groups KS, KL, LS, and LL. Factors with P < .25 in the univariate logistic regression analysis were then included in the multivariate logistic regression analysis. Differences were considered statistically significant at P < .05. In addition, for the ROC curve analysis, cut-off values of the C2–C7 angle to predict satisfactory surgical outcomes and the area under the ROC curve area under the receiver operating characteristic curve (AUC) were analyzed.
Results
Features of Patients Considering the Presence of Preoperative Kyphosis
Comparative Analysis Between Patients With Cervical Kyphosis and Those Without Cervical Kyphosis.
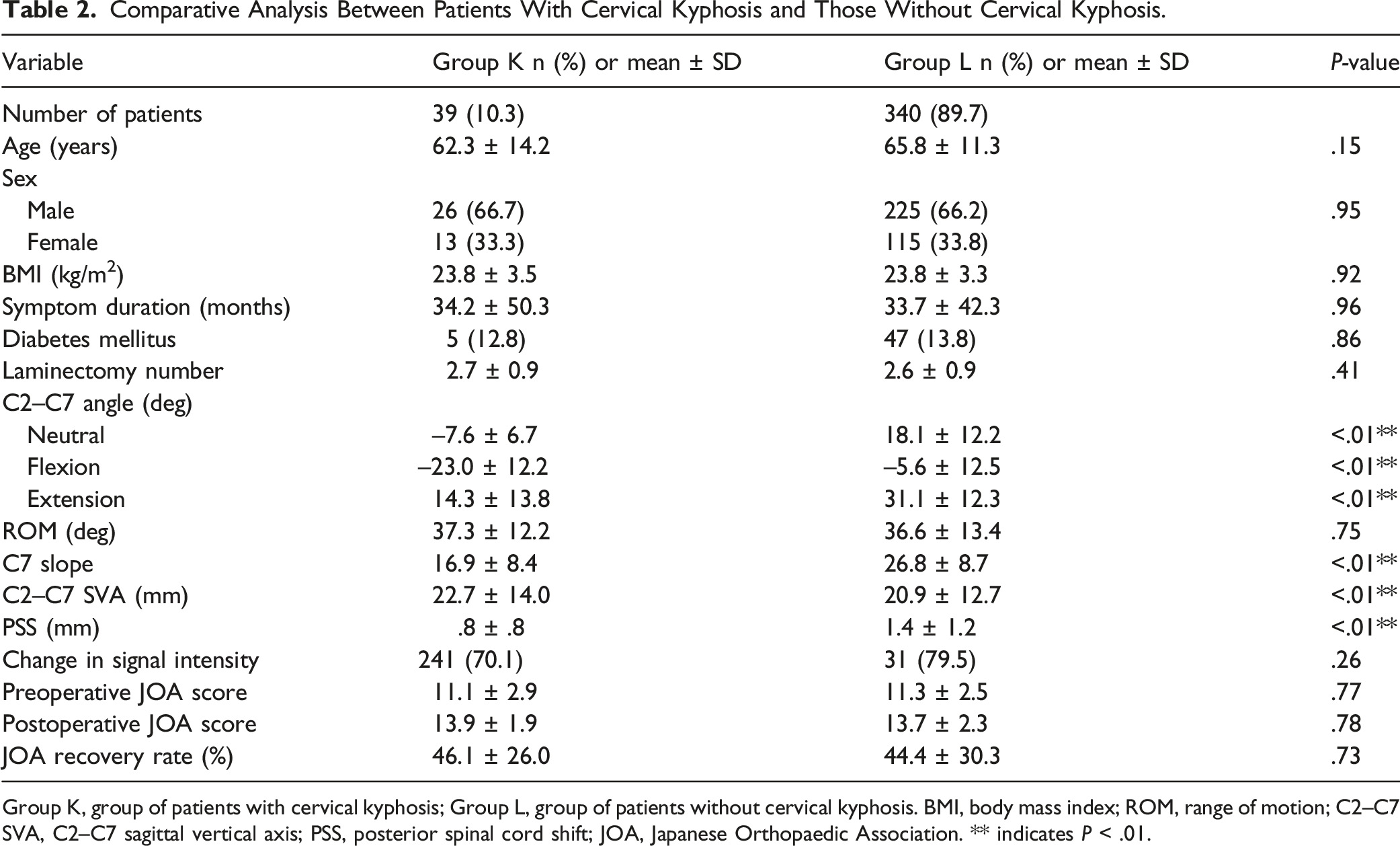
Group K, group of patients with cervical kyphosis; Group L, group of patients without cervical kyphosis. BMI, body mass index; ROM, range of motion; C2–C7 SVA, C2–C7 sagittal vertical axis; PSS, posterior spinal cord shift; JOA, Japanese Orthopaedic Association. ** indicates P < .01.
Features of patients considering the presence of preoperative kyphosis and a number of laminectomies
Comparative Analysis of Patients With Cervical Kyphosis Considering a Number of Laminectomies.
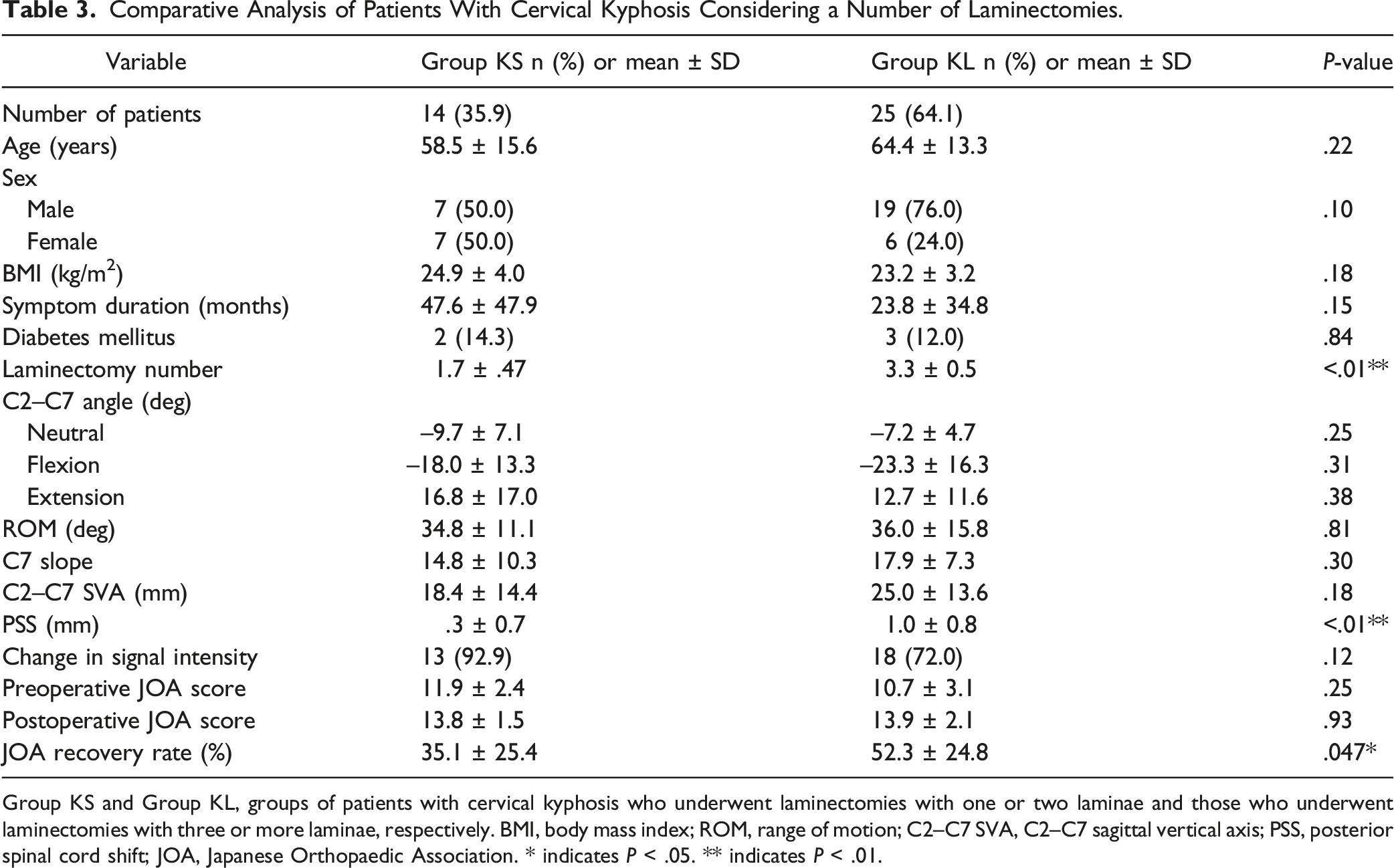
Group KS and Group KL, groups of patients with cervical kyphosis who underwent laminectomies with one or two laminae and those who underwent laminectomies with three or more laminae, respectively. BMI, body mass index; ROM, range of motion; C2–C7 SVA, C2–C7 sagittal vertical axis; PSS, posterior spinal cord shift; JOA, Japanese Orthopaedic Association. * indicates P < .05. ** indicates P < .01.
Comparative Analysis of Patients Without Cervical Kyphosis Considering a Number of Laminectomies.
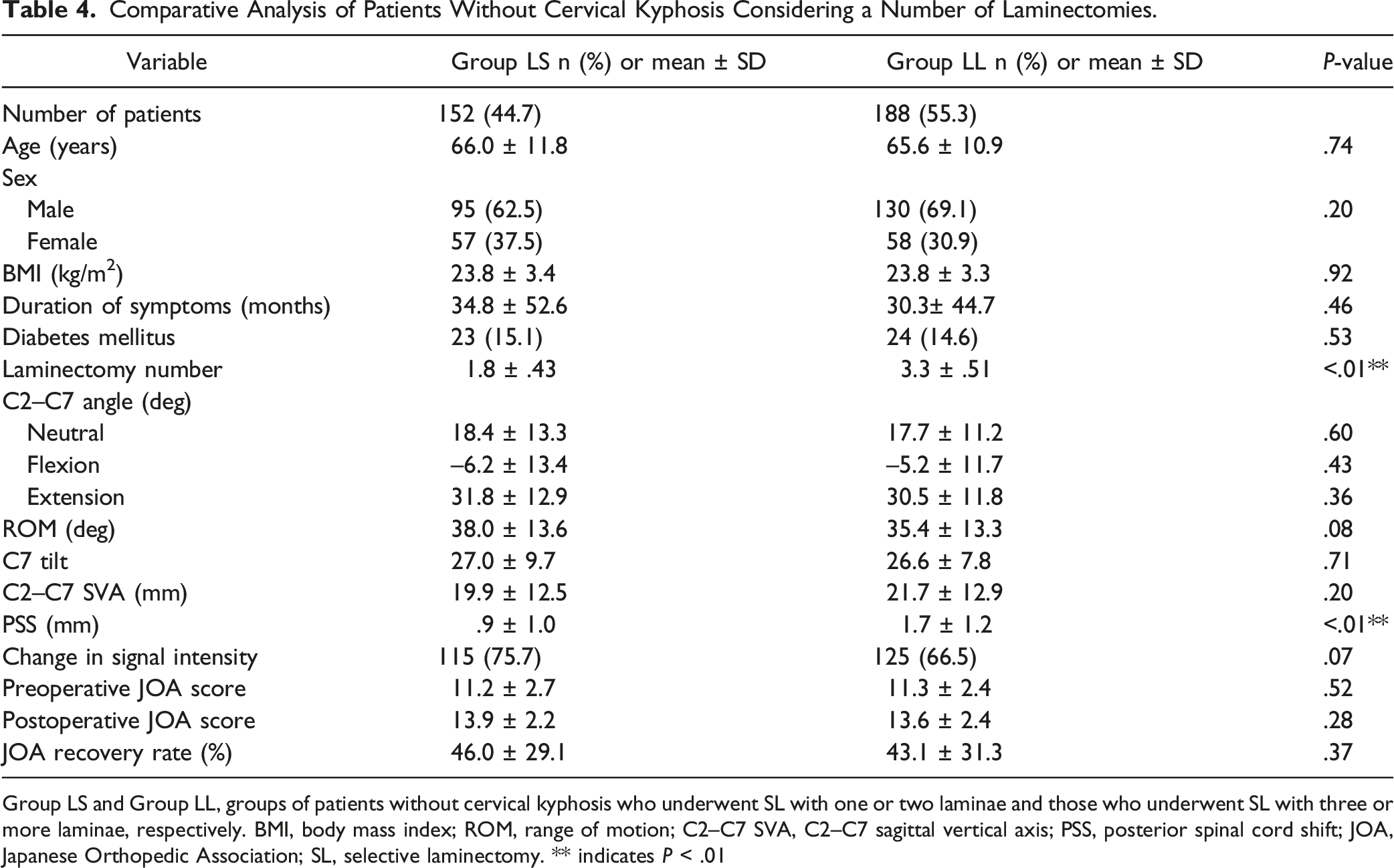
Group LS and Group LL, groups of patients without cervical kyphosis who underwent SL with one or two laminae and those who underwent SL with three or more laminae, respectively. BMI, body mass index; ROM, range of motion; C2–C7 SVA, C2–C7 sagittal vertical axis; PSS, posterior spinal cord shift; JOA, Japanese Orthopedic Association; SL, selective laminectomy. ** indicates P < .01
Multivariate Logistic Regression Analysis Between the Groups KS and KL
Univariate and Multivariate Logistic Regression Analyses Between Groups KS and KL.
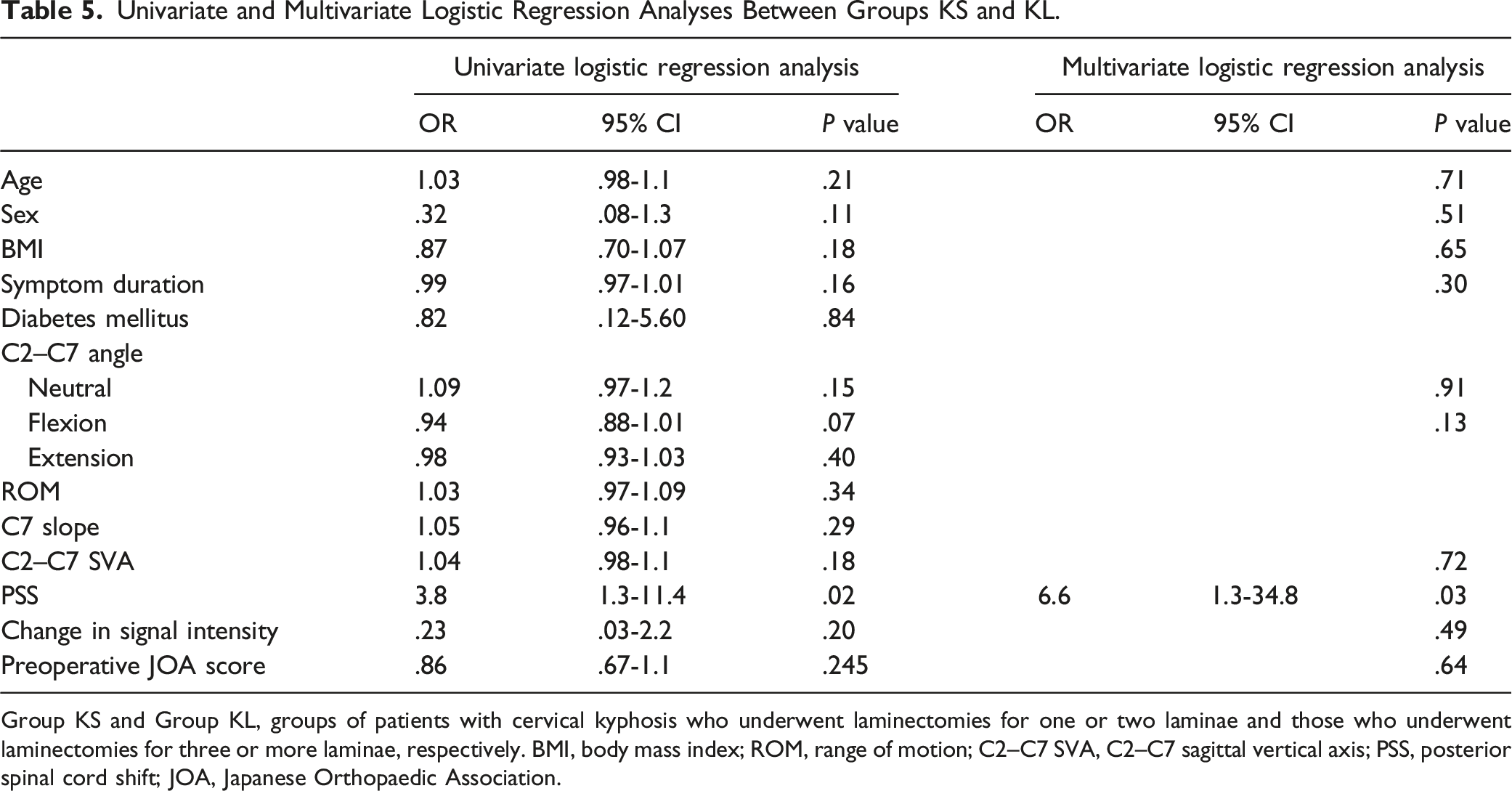
Group KS and Group KL, groups of patients with cervical kyphosis who underwent laminectomies for one or two laminae and those who underwent laminectomies for three or more laminae, respectively. BMI, body mass index; ROM, range of motion; C2–C7 SVA, C2–C7 sagittal vertical axis; PSS, posterior spinal cord shift; JOA, Japanese Orthopaedic Association.
Posterior spinal cord shift Considering Cervical Alignment and a Number of Laminectomies
The amounts of PSS (mm) were as follows: for group KS, .6 ± .7; for group KL, .9 ± 1.0; for group LS, 1.4 ± .8; and for group LL, 1.6 ± 1.2 (Figure 2). The amount of PSS in group KS was significantly smaller than those in other groups. Comparative analysis of posterior spinal cord shift, with consideration of the presence of cervical kyphosis and the number of laminectomies. Group KS and Group KL consisted of patients who had preoperative kyphosis and underwent laminectomies for one or two laminae and for three or more laminae, respectively. Group LS and Group LL consisted of patients who did not have preoperative kyphosis and underwent laminectomies for one or two laminae and for three or more laminae, respectively. PSS, posterior spinal cord shift. *P < .05. **P < .01.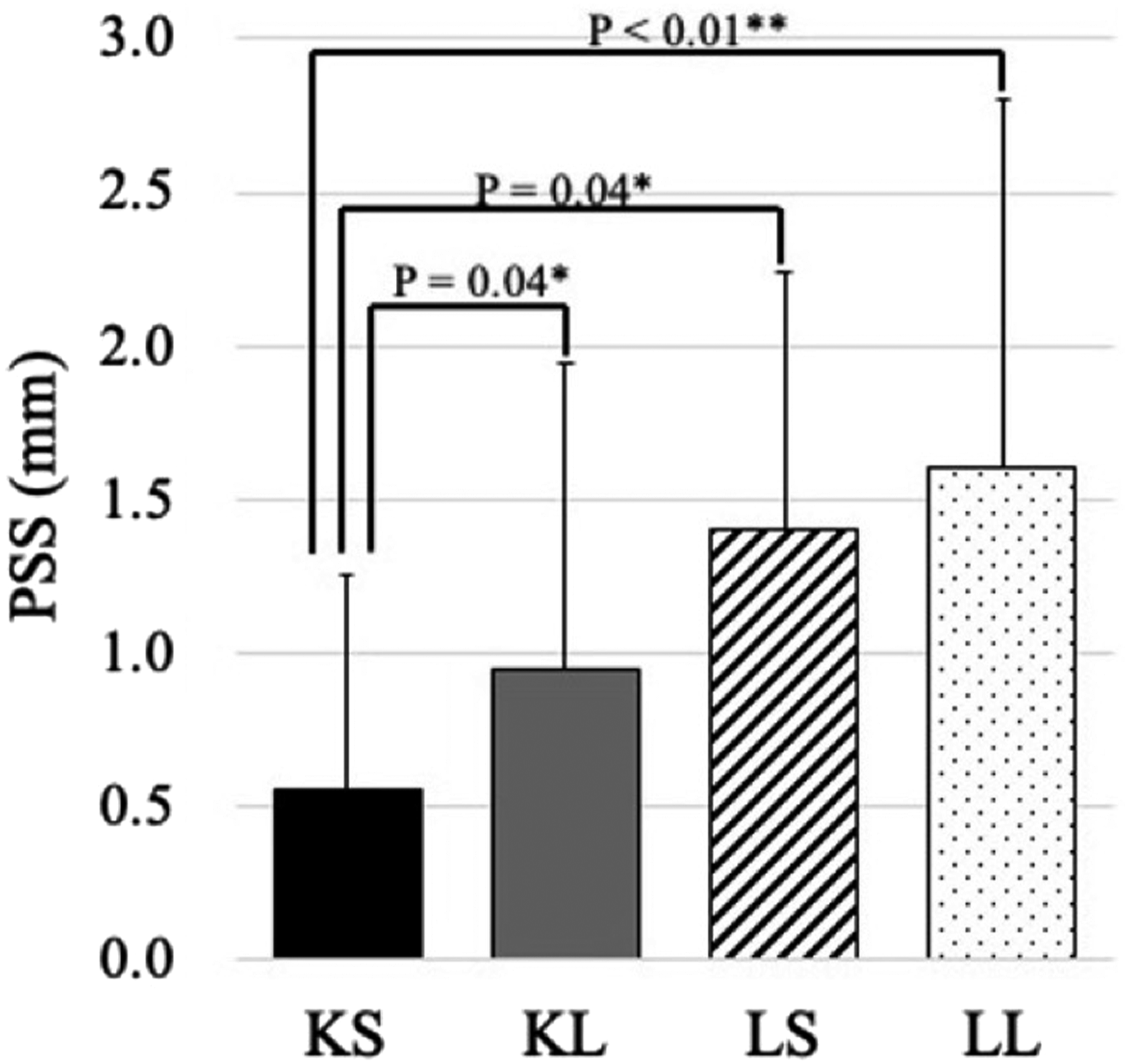
Receiver Operating Characteristic Curve Analysis
Among the patients with preoperative kyphosis who underwent fewer laminectomies (eg, 1 or 2), ROC curve analysis showed that −14.5° was considered the optimal cut-off value of the C2–C7 angle to predict satisfactory surgical outcomes, with an AUC of .70 (Figure 3). Receiver operating characteristic curve of preoperative C2–C7 angles to predict Japanese Orthopaedic Association recovery rate among the patients with kyphosis after fewer laminectomies (e.g., one or two). The area under the curve was .70.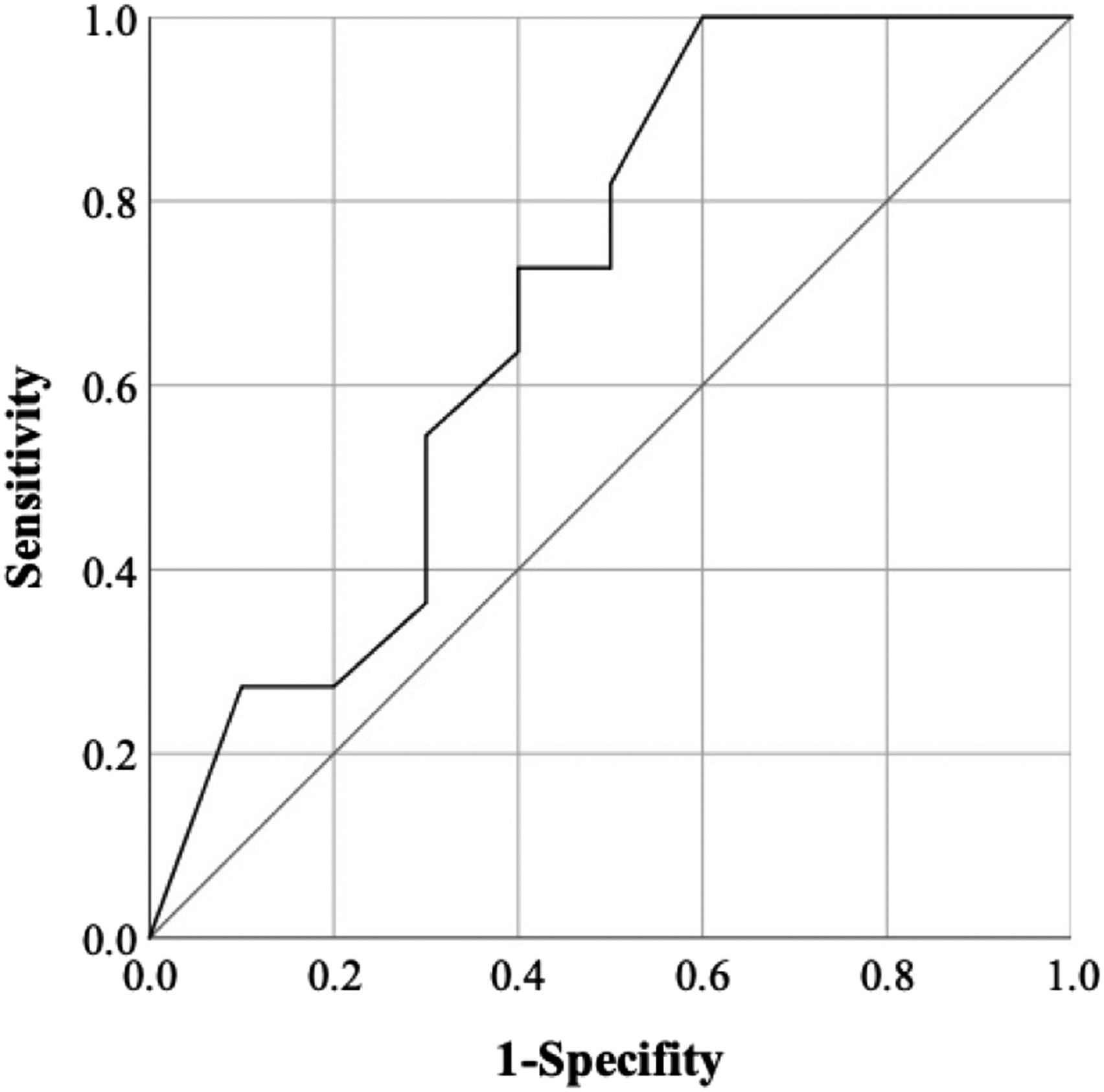
Case Presentation
Representative cases of patients in groups KL and KS are shown in Figure 4. A 68-year-old woman with a C2–C7 angle of −5° underwent a C4-6 SLs (group KL; Figure 4A1). The JOA recovery rate was 100% (14→17) with PSS of 2.3 mm (Figure 4A2). A 43-year-old man with a C2–C7 angle of −16.8° underwent C5-6 SLs (group KS; Figure 4B1). The JOA recovery rate was 20% (12→13) with PSS of .0 mm (Figure 4B2). Illustration of patients who have kyphosis with respect to the number of laminectomies. (A1) A 68-year-old woman with C2–C7 angle of −5° underwent a larger number of C4-6 SL (group KL). (A2) The JOA recovery rate was 100% (14→17) with PSS of 2.3 mm (arrow). (B1) A 43-year-old man with C2–C7 angle of −16.8° underwent a C5.6 SL (group KS). (B2) The JOA recovery rate was 20% (12→13) with PSS of .0 mm (arrowhead). SL, selective laminectomy; JOA, Japanese Orthopaedic Association; PSS, posterior spinal cord shift.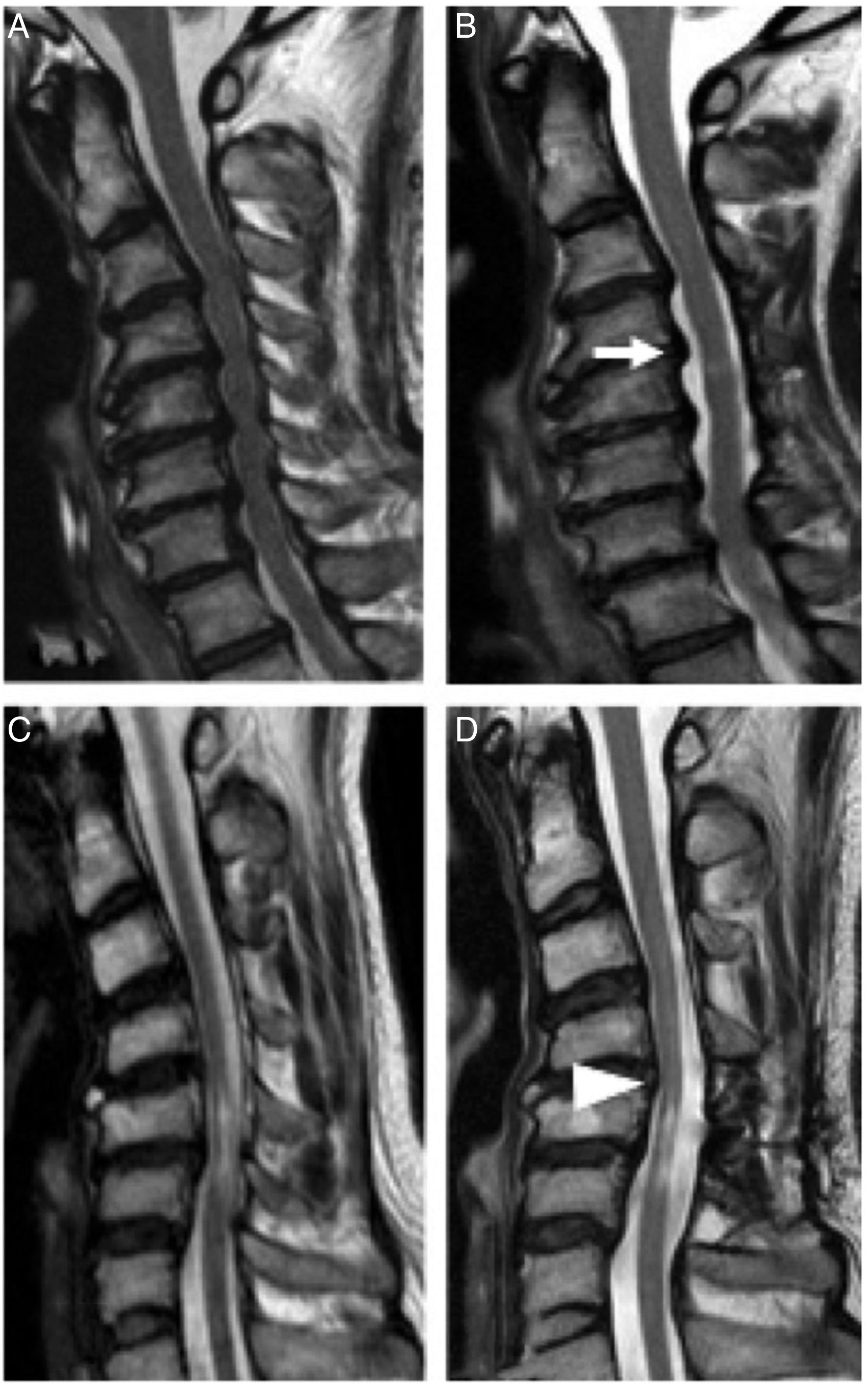
Discussion
This study retrospectively investigated the clinical impact of preoperative kyphosis on patients who underwent SL for CSM, especially considering PSS and laminectomy number with the largest number of patients (N = 379) among similar previous studies. The results showed that the mean magnitude of PSS in group K was significantly smaller than that in group L, but JOA recovery rate was comparable between the 2 groups. Moreover, the results of multivariate regression analysis and one-way ANOVA suggested that lower magnitudes of PSS associated with smaller number of laminectomies decreased the JOA recovery rate in group K. Interestingly, nevertheless, a smaller number of laminectomies was significantly correlated to a smaller amount of PSS but not with JOA recovery rate in group L. Meanwhile, the ROC curve analysis indicated that the cut-off value of preoperative C2–C7 angle for predicting satisfactory surgical outcomes was −14.5° in group KS.
Several studies reported that preoperative cervical kyphosis worsened surgical outcomes of posterior decompression among patients with CSM.6,14 The adverse effect of preoperative cervical kyphosis on surgical outcomes can be explained by 2 mechanisms. 6 First, a decrease in PSS associated with kyphosis may interfere anterior indirect decompression and result in poor postoperative neurological recovery.7,15 Second, fragility of the spinal cord related to cervical kyphosis may worsen surgical outcomes. An increase in intramedullary pressure associated with kyphosis may make the spinal cord more fragile, causing neuronal loss and demyelination.8-10 Furthermore, one study indicated that a reduction in blood supply to the cervical spinal cord in kyphotic spine or flex position may also gradually injure the spinal cord. 11
However, preoperative cervical kyphosis did not significantly worsen surgical outcomes after SL in the current study. Similarly, Chiba et al. 12 investigated 70 patients with CSM who underwent laminoplasty and reported that cervical kyphosis was not a contraindication for laminoplasty. Moreover, Jain et al. 13 compared characteristics of patients with CSM who underwent laminectomy without instrumentation between those with kyphosis (N = 32) and those without kyphosis (N = 36) and indicated that kyphosis did not influence the surgical results. In contrast, Suda et al. 6 evaluated 114 patients with CSM who underwent laminoplasty and demonstrated that the presence of local kyphosis with >13° was a risk factor of poor surgical results. Additionally, Miyamoto et al. 14 investigated outcomes of posterior surgery for the patients with CSM considering the presence of cervical kyphosis. The authors compared surgical results among patients with kyphosis who underwent laminoplasty alone (N = 30), those with kyphosis who underwent laminectomy with instrumentation (N = 30), and those without kyphosis who underwent laminoplasty alone (N = 30). As a result, posterior instrumentation surgery was significantly correlated to larger postoperative increase in C2–C7 angle and better surgical outcomes. Although the reasons of discordant clinical effects of cervical kyphosis on outcomes of posterior decompression surgery in previous studies are unclear, we have several speculations to explain the discordance. First, radiographic definition of cervical kyphosis differs in previous studies and may contribute to the disagreement: (1) different measurement methods were used, such as C2–C7 angle,7,20-24 local kyphosis,14,25 or both of them, 6 and (2) different degrees of cervical angle were adopted as a minimum degree of kyphosis, such as 0°,6,21-24 5°,6,7,14,20 or 10°. 25 Moreover, several studies did not demonstrate the definition of kyphosis.12,13 In this study, we used C2–C7 angle <0° as a definition of cervical kyphosis because this definition may be most commonly used,6,21-24 and the measurement method is reported to be associated with higher accuracy and reliability. 26 Second, previous studies investigating clinical features of kyphosis included relatively smaller number of patients (N; 43-114),6,7,12-14,21-25 and some studies comprised other diagnoses than CSM, such as OPLL7,24 and cervical spondylotic radiculopathy. 25 In contrast, our study included the largest number of patients (N = 379) among similar studies investigating clinical roles of preoperative cervical kyphosis and comprised only CSM as a diagnosis, which may provide a more reliable analysis. Third, different surgical indications and skills among surgeons may have diverse clinical impacts of kyphosis in the literature. For example, several studies demonstrated that preoperative grade of myelopathy affects surgical outcomes, but preoperative grade of myelopathy to consider a surgery varies among surgeons.1,27 Besides, cervical kyphosis was significantly associated with smaller C7 slope and larger C2–C7 SVA in this study. These results were in accordance with the previous studies possibly to maintain cervical balance.8,19
Moreover, a correlation between cervical kyphosis and amount of PSS was contentious in the literature. 28 In this study, we showed that patients with preoperative kyphosis had significantly smaller degree of PSS than those without preoperative kyphosis. Similarly, Sodeyama et al. 7 analyzed 65 patients with cervical myelopathy after laminoplasty and showed that smaller magnitudes of PSS were observed at C3/C4, C4, and C5, where anterior compression was most commonly presented, among patients who had kyphosis and S-shaped alignment. Furthermore, Baba et al. 15 investigated 55 patients who had cervical myelopathy undergoing open-door laminoplasty and found a positive correlation between degree of PSS and cervical lordosis. In contrast, Hatta et al. 29 investigated 51 patients with CSM who underwent posterior decompression surgery: 26 cases of SL and 25 cases of open-door laminoplasty. Consequently, they found no correlations between the amount of PSS and preoperative cervical curvature index among patients who underwent SL and those who underwent open-door laminoplasty. In addition, Shiozaki et al. 30 evaluated PSS among 19 patients with CSM undergoing laminoplasty and demonstrated that PSS at 24 h postoperatively did not correlate with preoperative C2–C7 angle. The causes of equivocal clinical correlations between PSS and cervical kyphosis and myelopathic grade are unclear, but we have some explanations for the controversy. First, various definitions of PSS in previous studies may affect the controversies; the PSS was measured from posterior vertebral body or disc to (1) anterior margin of the spinal cord,13,16,29,31 (2) middle of the spinal cord,15,30 and (3) posterior margin of the spinal cord. 7 Moreover, investigated spinal levels are different in the literature; they evaluated an amount of PSS at C3 level, 15 C4/5 level, 16 C5 level,13,29 and every level of cervical spine.7,30,31 In the current study, we measured the distance from the posterior aspect of C4/5 disc to anterior margin of the spinal cord to evaluate PSS for some reasons: (1) strong accuracy and reliability of that measurement were reported with interclass correlation coefficient (2, 1) >.8 in the previous study, 16 (2) decompression cases most commonly included the C4/5 level, 16 and (3) the PSS around this level is usually the greatest following posterior decompression surgery.7,16 Second, other similar studies included relatively smaller number of patients (N; 19-162),7,13,15,16,26,30 and some of preceding studies comprised different diagnoses other than CSM, such as OPLL.7,15 In contrast, our study included the largest number of patients (N = 379) among studies investigating the clinical features of PSS after posterior decompression surgery and comprised only CSM, which may provide a more reliable analysis. Third, technical differences of posterior decompression surgery in previous studies may affect the controversy. For instance, the width of laminectomy is reported to influence the amount of PSS, but the width depends on each surgeon’s preference and skill. 31
Among surgical methods of cervical posterior decompression, SL has a feature of minimizing a number of decompression laminae to preserve the posterior structure, and the feature is reported to be associated with smaller amount of PSS.5,16 Moreover, although still controversial, 28 correlations between magnitude of PSS, surgical outcomes, and preoperative kyphotic alignment are described in several previous studies.7,15
These previous studies reminded us of a clinical question in which a smaller number of SLs for the patients who have kyphosis may further decrease the amount of PSS and worsen surgical outcomes. However, to the best of our knowledge, there have been no studies that investigated the clinical question. Thus, we performed comparative analyses with patient groups generated by a presence of kyphosis and a number of laminectomies. As a result, PSS was the only significant variable; the others did not differ significantly between groups KS and KL in the multivariate logistic regression analysis, which suggested that a lower amount of PSS in association with a smaller number of laminectomies worsens surgical outcomes in patients having cervical kyphosis. Interestingly, in contrast, a smaller number of laminectomies was significantly correlated to a smaller amount of PSS but not to JOA recovery rate among patients who did not have preoperative kyphosis. Although the reason that clinical roles of a laminectomy number on JOA recovery rate depended on the presence or absence of preoperative kyphosis was unknown, we speculated the reason as below (Figure 5). A satisfactory surgical outcome and sufficient amount of PSS are obtained in group LL (A). Moreover, although a magnitude of PSS decreases, posterior decompression surgery still provides satisfactory outcomes for group LS (B) and KL (C). However, a degree of PSS further decreased in group KS with statistical significance (D). Combined with fragile nature of spinal cord due to increased intramedullary pressure and reduced artery filling associated with kyphosis, neurological recovery was interfered in group KS. In addition, to investigate which C2–C7 angle could provide satisfactory outcomes of a smaller number of SLs among the patients with kyphosis, we performed ROC curve analysis. The results showed that a C2–C7 angle of −14.5° was an optimal cut-off value for predicting satisfactory outcomes after a smaller number of SLs. Therefore, a number of laminectomies should be considered for the patients with kyphosis to obtain a sufficient amount of PSS and its related satisfactory surgical outcomes. In particular, in patients who have kyphosis with a C2–C7 angle of less than −14.5°, a larger number of SLs may be indicated. Posterior spinal cord shift with respect to the presence of cervical kyphosis and a number of selective laminectomies. (A) Larger amount of PSS without kyphosis, and a larger number of SLs. (B) Moderate amount of PSS without kyphosis, and a smaller number of SLs. (C) Moderate amount of PSS with kyphosis, and a larger number of SLs. (D) Smaller amount of PSS with kyphosis, and a smaller number of SLs. PSS, posterior spinal cord shift; SL, selective laminectomy.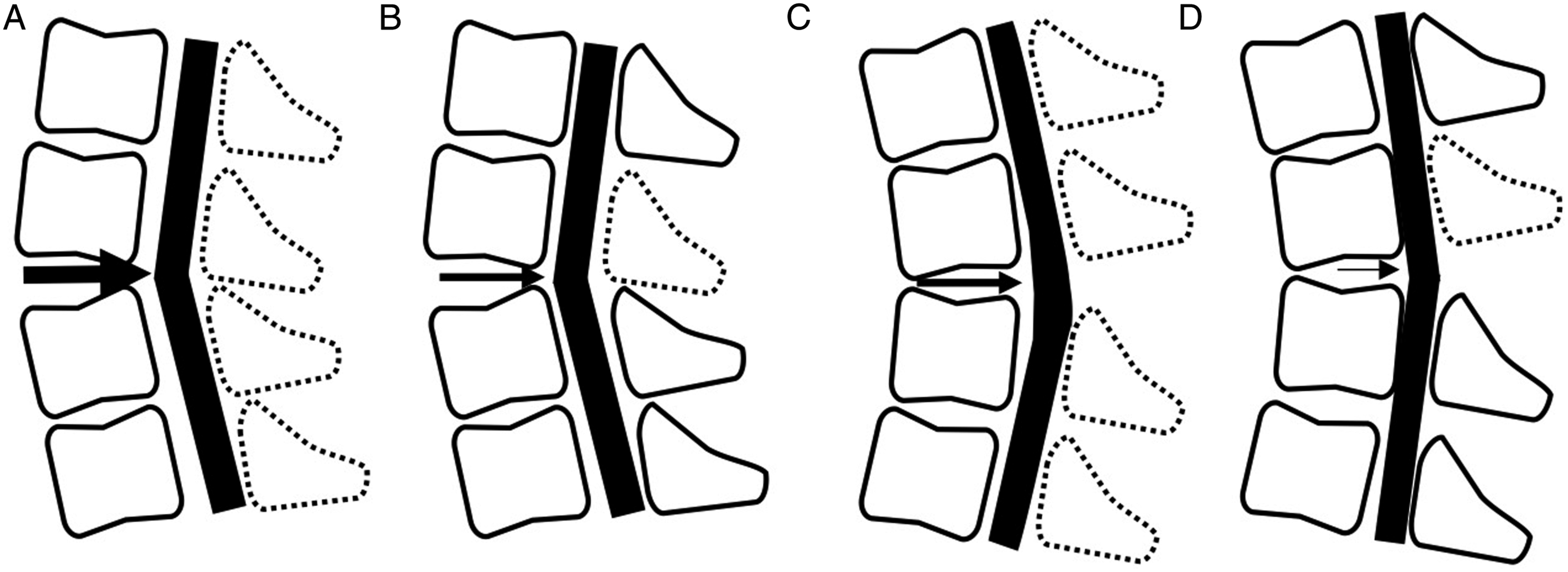
Some limitations must be considered when interpreting the present results. First, this is a retrospective study and thus sample and control biases are difficult to control. Second, several procedures of the study may have led to biases. The patients’ data were collected from two hospitals, which could have led to bias, although the surgeons faced a common surgical indication and had comparable surgical skills for SL. In addition, the magnitude of PSS was investigated at mainly C4/5, but in 20 cases (5.3%), levels other than C4/5 were adopted because the C4/5 level was not included among the levels of decompression. Third, symptomatic patients who have severe kyphosis are more likely to undergo anterior or posterior decompression with fixation surgery; however, such cases were excluded in the current study. To address these limitations, further prospective investigation is needed with a longer follow-up period.
In summary, we conducted a retrospective study to find the impact of preoperative cervical kyphosis on surgical outcomes of SL for CSM with the largest number of patients among studies investigating clinical features of cervical kyphosis. Our results showed that kyphosis was significantly associated with a smaller degree of PSS but not with JOA recovery rate. Meanwhile, among the patients who had preoperative kyphosis, a smaller number of laminectomies was significantly associated with a smaller amount of PSS and lower JOA recovery rate. In contrast, among the patients who did not have preoperative kyphosis, a smaller number of laminectomies was significantly correlated to a smaller amount of PSS but not to JOA recovery rate. In addition, we performed ROC curve analysis to investigate which C2–C7 angle could provide satisfactory outcomes of a smaller number of SLs among the patients with kyphosis, and found that a C2–C7 angle of −14.5° was an optimal cut-off value for predicting satisfactory outcomes after a smaller number of SLs. We speculate that an insufficient anterior indirect decompression effect by further decrease of PSS and fragile nature of spinal cord associated with kyphosis worsens neurological recovery among patients with kyphosis who underwent smaller number of SLs. Taken together, the current study suggested that SL is not contraindicated for patients who have kyphosis, but for patients who have kyphosis with a C2–C7 angle of less than −14.5°, a larger number of SLs may be indicated.
Footnotes
Acknowledgments
We would like to thank Keiichi Sakuma for data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.