
Abstract
Study design
Narrative Literature review.
Objective
To provide a general overview of important molecular markers and targeted therapies for the most common neoplasms (lung, breast, prostate and melanoma) that metastasize to the spine and offer guidance on how to best incorporate them in the clinical setting.
Methods
A narrative review of the literature was performed using PubMed, Google Scholar, Medline databases, as well as the histology-specific National Comprehensive Cancer Network guidelines to identify relevant articles limited to the English language. Relevant articles were reviewed for commonly described molecular mutations or targeted therapeutics, as well as associated clinical outcomes, and surgery-related risks.
Results
Molecular markers and targeted therapies have dramatically improved the survival of cancer patients. The increasing importance of prognostic molecular markers and targeted therapies provides rationale for their incorporation into clinical decision-making for patients diagnosed with metastatic spine disease. In this review, we discuss the molecular markers/mutations and targeted therapies associated with the most common malignancies that metastasize to the spine and provide a framework that the surgeon can utilize when evaluating patients for potential intervention. Finally, we provide case examples that highlight the importance of molecular prognostication and therapies in surgical decision-making.
Conclusion
An integrated understanding of the implications of surgery, radiation, molecular markers and targeted therapies that guide prognostication and treatment is warranted in order to achieve the most favorable outcomes for patients with metastatic spine disease.
Keywords
Introduction
Survival of patients with metastatic spine disease has significantly improved in the last 20 years. 1 Advances in surgical approaches and the use of stereotactic body radiation therapy have allowed for decreased treatment complications and the ability to improve neurologic outcome and local tumor control.2-6 However, most of the survival benefit for patients with disseminated cancer has resulted from advancements in the molecular understanding of cancer and the development of targeted therapies for patients harboring key mutations.7,8 Thus, for the spine surgeon evaluating these patients, a balanced understanding of the implications of surgery, radiation, molecular markers and targeted therapies that guide prognostication and treatment is warranted in order to achieve the most favorable outcomes for patients with metastatic spine disease.
The NOMS framework (neurologic, oncologic, mechanical, and systemic) is perhaps the most commonly used functional algorithm for surgeons treating metastatic spine disease. 9 Within this framework, the assessment of the oncologic status can be one of the most complex pillars of surgical assessment, given the rapid advancements in treatment options. It is only within the last decades that we have recognized that certain genetic markers are able to better predict overall survival or even drug candidacy, while certain treatments can either obviate the need for surgical intervention or be considered a direct contraindication to surgical intervention.9,10 Developments of new systemic treatments such as immunotherapy or targeted therapies have resulted in far greater progression-free survival, overall survival, and overall response rates for many cancers that have traditionally thought to be associated with poor outcomes.7,8 Conversely, patients undergoing treatment with certain targeted therapies such as antiangiogenic agents (VEGFR inhibitors) can have severe wound-healing complications following surgery. 11 Thus, the evolving landscape of molecular advances and targeted therapeutics has created an increased need for the surgeon to be aware of these factors and how best to incorporate them into their decision-making.
The purpose of this article is to provide the spine surgeon with a general overview of important molecular alterations and targeted therapies for some of the most common solid neoplasms (lung, breast, prostate, and melanoma) that metastasize to the spine, as well as guidance on how to best incorporate them in the clinical setting.
Molecular Marker and Targeted Treatment by Primary Tumor Histology
Lung Cancer
Lung cancer is the leading cause of cancer death worldwide and is broadly grouped into 2 categories: small cell lung cancer (SCLC) and NSCLC. Approximately 70% of patients diagnosed with lung cancer will present with locally advanced or metastatic disease at diagnosis, including bone and spine metastases.12-14 Traditionally, the prognosis of patients with spinal metastases has been poor, particularly for patients with cord compression, with a median survival of 2 – 4 months.15-18
SCLC usually responds well to chemotherapy and radiation with further improvements realized by immunotherapies; however, diagnosis is commonly made at advanced stages and so prognosis tends to be worse than NSLC. 17 Given the responsiveness and urgency to initiate systemic therapy, the role of surgery for spinal metastases tends to be when urgent intervention is needed to palliate mechanical instability or for neurologic recovery.
Common molecular targets and systemic treatments for the most common primary tumors associated with spine metastases.
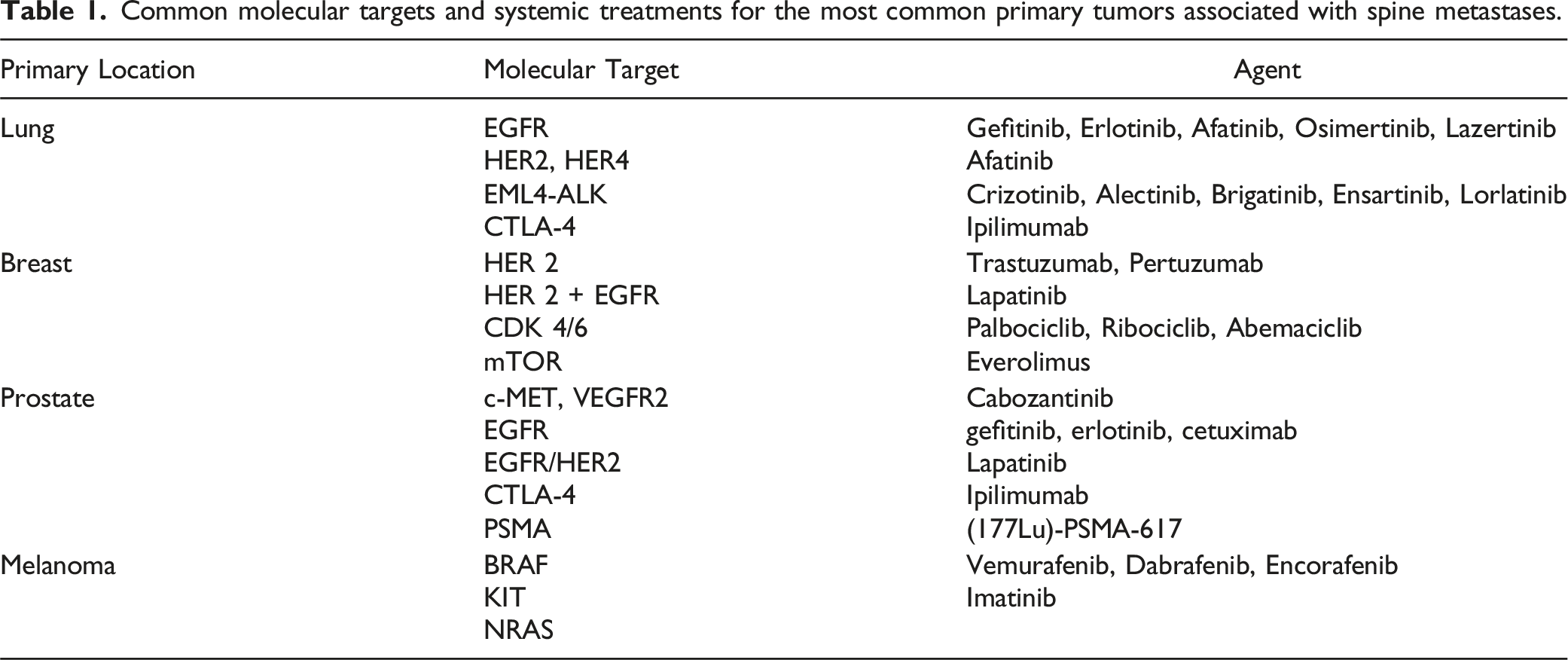
Other important actionable mutations include echinoderm microtubule-associated protein-like 4-anaplastic lymphoma kinase (EML4-ALK) mutations which can be treated with crizotinib, alectinib, brigatinib, ensartinib or lorlatinib and have shown encouraging results in patients with advanced disease.22,23 Both KRAS (Kirsten rat sarcoma virus) and BRAF mutations can also be found in patients with NSCLC. When targeted inhibitors to these mutations (Sotorasib, recently approved for patients with KRAS p.G12C-mutated advanced NSCLC 24 or Dabrafenib, a BRAF V600 E inhibitor) are combined with a MEK inhibitor (trametinib), patients with NSCLC have improved outcomes. BRAF has been historically difficult to target given that patients tend to develop resistance, but recent trials have also shown promising results. 25 Immune checkpoint inhibitors are routinely used as standard of care and have substantially increased overall survival for patients diagnosed with lung cancer. A study of 26 patients with NSCLC and spinal metastases found that for patients harboring mutations in ALK, MET, ROS1, EGFR and/or KRAS who underwent spine surgery, overall survival was significantly improved compared to patients who did not harbor a mutation. 26
Breast Cancer
Breast cancer is one of the most common cancers to metastasize to bone, with studies estimating an occurrence of almost 80%. Prognostic factors in breast cancer include patient age, histologic grade, hormone receptor (HR) status (i.e. estrogen receptor (ER) and progesterone (PR)), human epidermal growth factor receptor (HER2) status, and Ki-67 index, among others. From an immunohistochemical standpoint, breast cancer can be divided into several categories: 1) luminal A (HR+), 2) luminal B (HR+/HER2+), 3) HER2 enriched (HER2+), and 4) triple-negative (HR-/HER2-). From a prognostic standpoint, a study of patients with spinal metastases found the 12-month postoperative survival rate to be 63%, 83%, 0%, and 12%, respectively (P < .001). 27
HER2 is a proto-oncogene that is overexpressed in 15%–20% of breast cancer patients. A specific gene copy amplification results in hyperproliferative cancer cells and poor prognosis. However, the development of targeted therapy with trastuzumab revolutionized treatment of metastatic HER2 + breast cancer [Table 1]. In combination with chemotherapy, trastuzumab allows for significant benefits in progression-free survival and overall survival. 28 Since the initial FDA approval of trastuzumab, many other HER2 targeted therapies have been tested in the setting of metastatic breast cancer, including Lapatinib and Pertuzumab. 29 A multi-center study of 556 patients with breast cancer and spinal metastases found that HER2+ was an independent prognostic factor for survival, independent of patient age and histological grade. 30
ER positive tumor cells can sometimes develop resistance to endocrine therapy via several pathways. For example, Rb phosphorylation by CDK 4/6 promotes the G1-to-S phase transition and is upregulated in endocrine-resistant cells. Targeted inhibition of CDK 4/6 with palbociclib combined with fulvestrant resulted in longer progression-free survival than fulvestrant alone in a landmark trial published in 2015. 31 Inhibitors of mTOR (everolimus) are another form of targeted therapy. mTOR enhances the efficacy of hormonal therapy via activation of the ER. The BOLERO 2 trial showed that in patients with ER positive metastatic breast cancer resistant to anastrozole and letrozole, exemestane plus everolimus extended the progression-free survival from 4 to 10 months. 32 Many advances continue to evolve including use of immunotherapy in triple negative patients.
Prostate Cancer
The spine is the most common anatomic location of prostate cancer metastases. Symptomatic cord compression can sometimes be the presenting manifestation of the disease, and in that urgent situation a markedly elevated serum Prostate Specific Antigen (PSA) can make the diagnosis without need for tissue sampling. Prostate cancer cells are driven by androgens, and for the past 70 years they have been treated with androgen deprivation targeted therapies (ADT) including luteinizing hormone-releasing hormone antagonists and anti-androgens. More recently, novel androgen therapies in the form of androgen axis-receptor targeted (ARAT) therapies are furthering survival outcomes. In newly diagnosed patients with metastatic disease not requiring urgent surgical intervention, initiation of ADT can rapidly induce the patient castrate and stabilize the disease. At that point, radiation can be considered as opposed to surgery.
While most patients with newly diagnosed and metastatic hormone sensitive prostate cancer (HSPC) respond well to ADT, eventually tumors become resistant. Castrate resistant prostate cancer (CRPC) patients that present with symptomatic cord compression are typically treated first with surgical decompression with or without stabilization. HSPC metastases to the spine respond more favorably to SBRT compared to CRPC in terms of local control, and patients also have higher rates of 12- and 24-month survival. 33
New developments are changing the medical therapy for prostate cancer. Targeted therapies for prostate cancer are still limited, but have included cabozantinib (MET and VEGFR2 inhibitor), gefitinib, erlotinib, and cetuximab targeting EGFR, lapatinib targeting EGFR/HER2, olaparib (PARP inhibitor), and ipilimumab (anti-CTLA4).5,34 PSMA (prostate-specific membrane antigen) is highly expressed in metastatic CRPC, and targeted therapy has been recently developed aimed at this antigen. Lutetium-177 (177Lu)-PSMA-617 is a radioligand therapeutic agent that delivers radiation to PSMA-expressing cells and has resulted in improved progression-free and overall survival compared to standard of care. 35
Melanoma
Metastatic melanoma has historically been associated with limited survival, with patients harboring spinal metastases having a median survival of approximately 4 months. 36 One of the most studied pathways for targeted therapy in melanoma is the mitogen-activated protein kinase (MAPK) pathway. This pathway is frequently activated in melanoma and plays a critical role in the growth and survival of these cells. Several drugs have been developed that target different components of the MAPK pathway, including BRAF and MEK inhibitors.
BRAF targeted therapy is amongst the most common, given up to two-thirds of melanoma cancers have this mutation. 37 Agents targeting BRAF V600 E include vemurafenib, dabrafenib, and encorafenib. Several landmark trials showed superiority to chemotherapy in terms of progression-free survival, overall survival, and overall response rate. 8 Nevertheless, 15% of patients had initial resistance to BRAF targeted therapy, and studies found that eventually resistance developed in 50% of patients. 38
KIT mutations are less common, but treatment with imatinib can result in some response in a small subset of patients. 39 NRAS-mutant melanoma comprises 15%–20% of all melanomas and tends to be more aggressive compared to non-NRAS mutant melanoma. There are limited available therapies compared to BRAF-mutant melanoma, but use of MEK inhibitors and PI3k-AKT inhibitors appear to be of some benefit. Immunotherapy regimens are considered standard of care given the robust effects on survival and their benefit is agnostic to checkpoint ligand or receptor positivity unlike lung cancers.
Surgical Considerations with Targeted and Non-Targeted Systemic Therapies
A wide array of other targeted and non-targeted therapies exist for each histology type, however, review of all therapies is beyond the scope of this review. In this section, we focus on common therapies that should warrant critical appraisal of the patient with spine metastasis, given their mechanism of action, risk profile, and general consideration in the natural history/treatment course for a given patient.
The vascular endothelial growth factor (VEGF) pathway is involved in angiogenesis and therefore cell growth and proliferation; mutations are found in gliomas, NSCLC, colorectal cancer, hepatocellular carcinoma, renal cell carcinoma, and some gastrointestinal tumors. 40 One of the most common agents utilized for this is bevacizumab (e.g. Avastin), and a study of 18 subjects undergoing spinal radiation for metastatic disease found that patients taking this therapy did not have any unexpected complications from use of this drug. 41 However, for patients indicated for surgery, bevacizumab can lead to increased risk of hypertension, and severe bleeding, as well as severe wound-healing complications depending on the washout period prior to the index procedure, as well as. 42 Similarly, tyrosine kinase inhibitors, such as cabozantinib and sutent, are suggested to be held at minimum 3-4 weeks prior to a surgical procedure given the similar risk profile. Caution should be observed prior to proceeding with surgical intervention for a patients on these drugs, as the potential for wound-related complications and bleeding can be high, even after a sufficient washout period of 4-6 weeks. Multi-disciplinary management with plastic surgery should also be highly considered.
For chemotherapeutic agents, retrospective studies have demonstrated that patients who have received chemotherapy within 3 weeks of surgery are more likely to require a wound-related revision surgery.43,44 Antineoplastic drugs such as capecitabine, (breast), plant alkaloid based therapies such as cisplatin, and anti-metabolite therapies that interfere with DNA, such as 5-fluorouracil can be held 1-3 weeks prior to surgery depending on physician preference. Given the mechanisms of action (these agents are shown to induce myelosuppression and interfere with fibroblast function), the risk of impaired wound healing or infection is considerably higher. 44
Androgen therapies such as tamoxifen, pertuzumab, transtuzumab, androgen deprivation targeted therapy (ADT) such as bicalutamide, flutamide, or abiraterone and immunotherapies such as Pembroluzimab, nivolumab, ipilumumab, appear safe in the perioperative setting, involving multiple different types of surgery, and likely do not need to be stopped in the perioperative setting. 45 Caution needs to be applied in general with novel agents when safety profiles are evolving such as CDKN2A inhibitors, and generally to hold drug 2-4 weeks post operatively, until the wound is healed, is reasonable practice.
Questions to Ask
Does the Patient Have Favorable or Actionable Mutation or Molecular Marker that Has an Associated Targeted Therapy?
Broadly speaking, patients harboring tumors with mutations amenable to targeted therapy will tend to have longer survival and progression-free survival. For patients with metastatic spine disease, harboring these mutations would generally make a patient more suitable for surgical intervention, given that expected postoperative survival is used to determine surgical candidacy in most centers. The potential responsiveness to targeted therapy also suggests that patients have options for the postoperative period to control the systemic disease and that this would allow for sufficient time to recover from surgical intervention. Conversely, certain targeted therapies can negate the need for surgical intervention because the treatment can rapidly stabilize the disease and allow for other potential treatments. (See prostate cancer section above).
Conversely, the corollary to the above question
What Line of Medical Therapy is the Patient Currently Receiving?
The specific line of therapy may be difficult to discern as each histology has its own unique treatment regimen and within each histology there are variations in specific drug treatments based on molecular markers, risk profile, presence or absence of metastatic disease on presentation, etc. For instance, patients with newly diagnosed cancers that have not received treatment, usually have an abundance of options, and the likely benefit from surgical intervention is high. Conversely, for patients on their fourth or fifth line of systemic therapy (i.e. patients who have undergone multiple drug regimens), the potential for further systemic options may be limited or there may be no option at all. Thus, surgeons should carefully weigh the indications for surgery, the proposed surgical approach/expected recovery, the patient’s frailty/ability to tolerate surgery and the risk of morbidity and mortality against the treatment options available for a patient.46-50 In either case, a multi-disciplinary approach with medical oncology consultation is usually best to gain clarity on where a patient is currently in the natural history of their cancer. (See case examples).
Is the Patient on a Targeted Therapy, Drug or Treatment that Could Dramatically Increase the Risk Profile or is Associated with Severe Wound-Related Complications, Hemorrhage, or Thrombocytopenia (i.e. Tyrosine Kinase Inhibitor, Bevacizumab, Chemotherapy, etc.)?
Although surgical intervention may be warranted based on other indications (i.e. instability, neurologic compromise, etc.), this should be weighed against the potential complications that can ensue based on the approach. Patients should be appropriately counseled about these risks, and steps should be taken to minimize potential morbidity and mortality as much as possible. For patients on targeted therapies with increased risk for wound-related complications, consider consultation with a plastic surgeon, particularly, if treatment was received within 4-6 weeks of the proposed surgical intervention.51-53 (See Other Targeted and Non-Targeted Systemic Therapies Section Above).
Implementation into Clinical Practice
The most common and accepted decision-making framework or algorithm for management of spinal metastases is the NOMS (Neurologic, Oncologic, Mechanical, and Systemic) framework. Historically, the oncologic component of this framework assesses the tumor responsiveness to radiation. Tumors are stratified as radiosensitive or radioresistant/previously radiated; the former would signify the patient receives radiation and the latter that the patient receives separation surgery. In the context of the molecular landscape, the treating surgeon should incorporate responsiveness to chemotherapies and targeted therapeutics into the NOMS framework when deciding the most optimal treatment approach. Nevertheless, implementation into clinical practice can be challenging, especially in patients presenting with acute spinal cord compression from a radioresistant tumor and neurologic deficits. In such patients, it may be difficult to negate surgical decompression solely based on the type of mutations the primary tumor harbors. To aid in clinical decision-making, we suggest the following questions that can be asked by the surgeon to assess the relative benefit/risk ratio of a surgical procedure from the oncologic (i.e. molecular and targeted therapeutic) standpoint, that can be combined with the other components of the NOMS framework. (Figure 1) When asked to evaluate a patient with metastatic spine disease, these questions should be asked from the oncologic standpoint.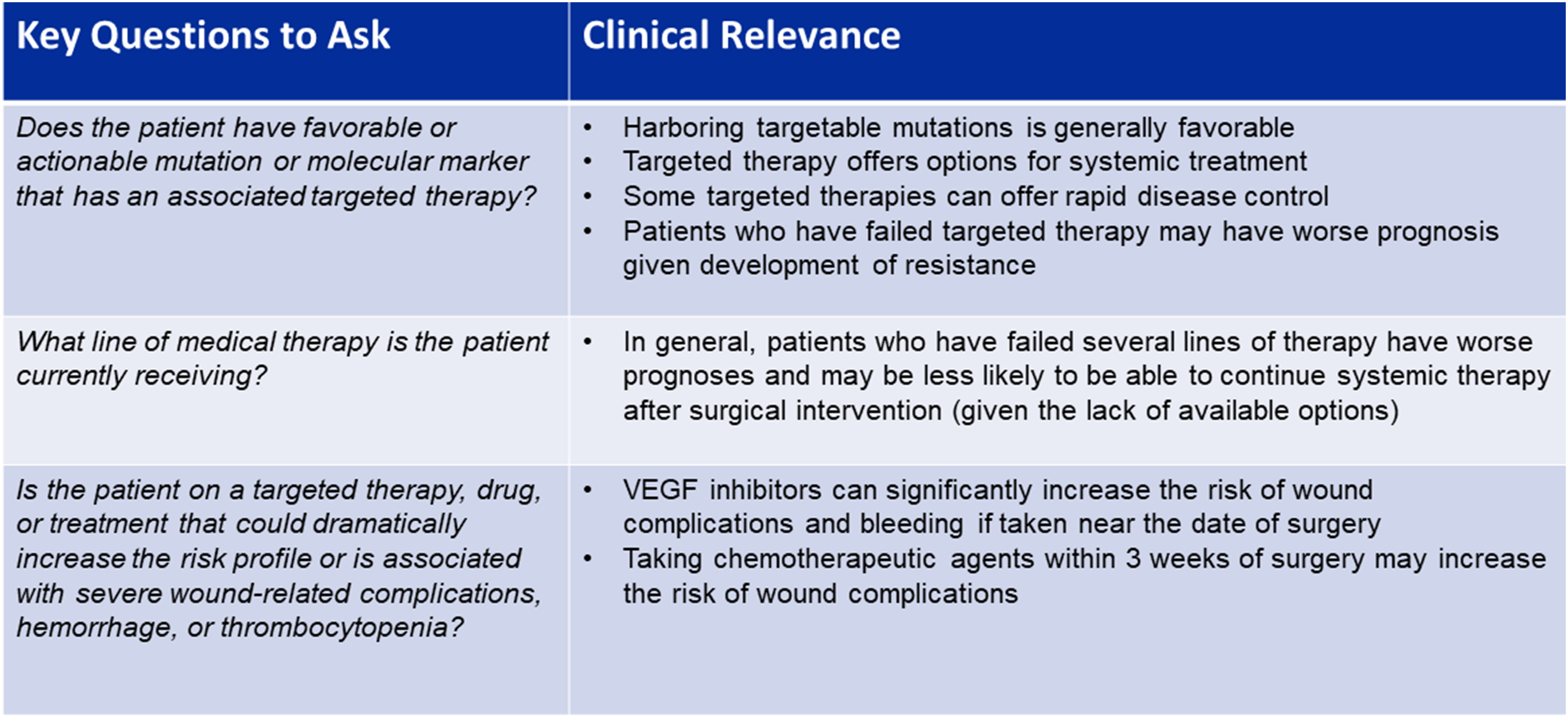
Case Examples
For patients not presenting with acute neurological deficits, the following examples highlight differences in tumor profiles and management using the same histology. The reader should note that the histology for each case example listed could be changed to a different histology with its corresponding molecular marker and/or line of therapy to illustrate their incorporation into surgical decision-making (i.e. melanoma and a BRAF V600 E mutation for the first case example).
Case 1: A 46-year-old man presents with 3 months of weight loss, back pain, and cough. He is a non-smoker. Chest imaging reveals a lung nodule consistent with NSCLC (adenocarcinoma) and molecular analysis reveals an EGFR mutation. There is a single metastatic lesion at L2 causing a pathologic fracture with greater than 50% loss of height and retropulsion. He is ambulatory and has pain-limited weakness 4/5 on the hip flexor. He has good performance status (ECOG 1) and his Spine Instability Neoplastic Score is 17. Given the recent diagnosis of NSCLC and the favorable EGFR mutation, patient is started on osimertinib and offered separation surgery plus stabilization. (Figure 2) Sagittal CT and MRI and axial MRI demonstrating at L2 causing a pathologic fracture with greater than 50% loss of height and retropulsion, bony destruction of posterior elements, and epidural compression. Spinal Instability neoplastic Score of 17.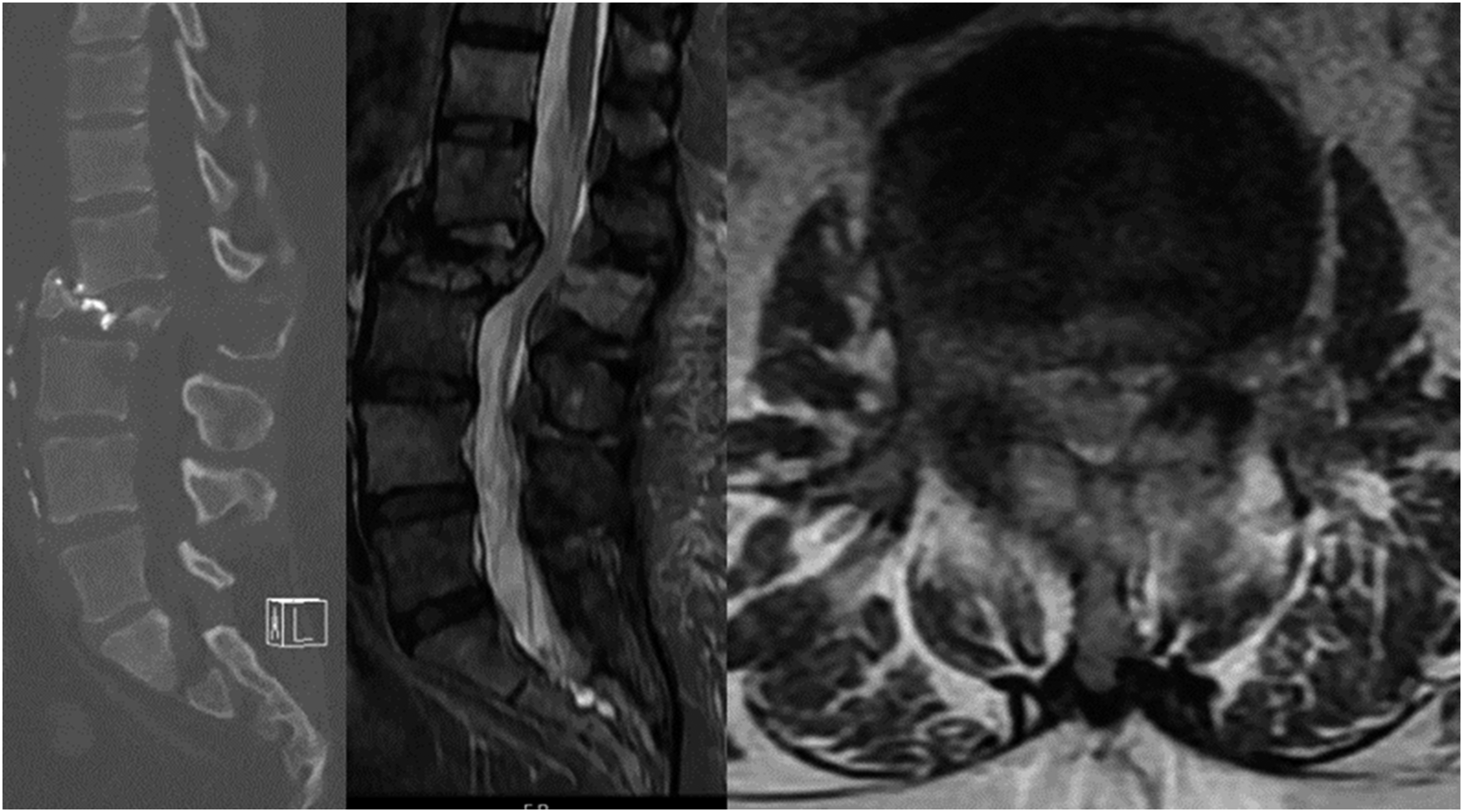
Case 2: A 71-year-old man presents with 1 week of back pain. He was diagnosed 5 months ago with NSLC adenocarcinoma also with an EGFR mutation and started on osimertinib. One month ago, he was found to have metastases to the liver and pelvis and was started on pembrolizumab/carboplatin/pemetrexed. He is now found to have an L2 pathologic fracture with retropulsion. He is ambulatory and full strength. His ECOG performance status is 2 and his SINS is 15. The patient seems to have progressed through targeted therapy but just started chemotherapy recently, which still leaves room for further systemic options. Patient is offered separation surgery plus stabilization. (Figure 3) Sagittal and axial CT and MRI demonstrating a lytic L2 lesion causing a pathologic fracture with greater than 50% loss of height, retropulsion, and epidural compression. Spinal Instability neoplastic Score of 15.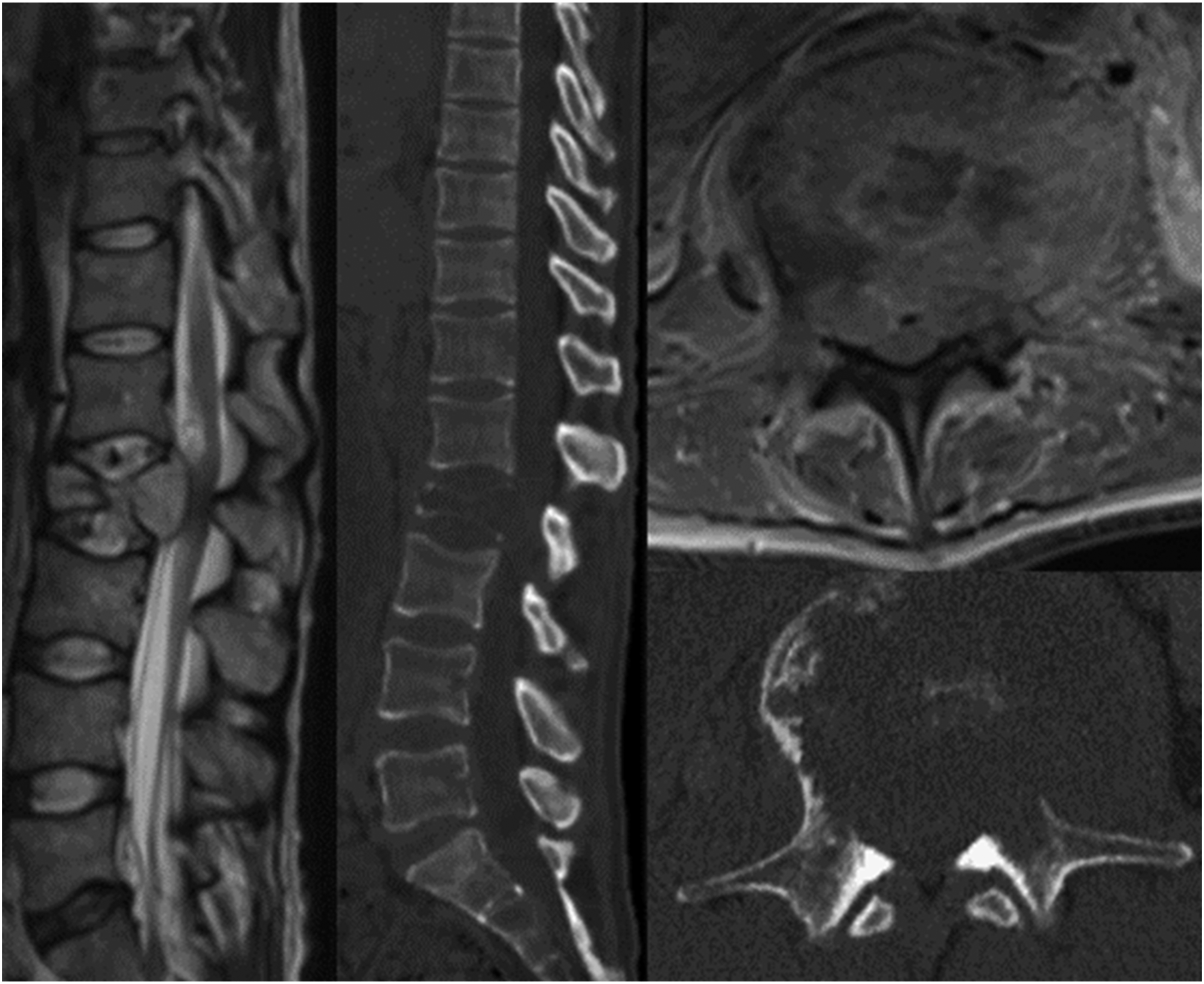
Case 3: A 60-year-old man presents with 3 weeks of severe neck pain and gait instability, which has resulted in him spending most time in bed. He has been previously treated with several lines of therapy including osimertinib, pembrolizumab/carboplatin/pemetrexed, docetaxel, and gemcitabine. He is found to have multiple lung nodules consistent with NSCLC (adenocarcinoma) and molecular analysis reveals no favorable mutation after testing for EGFR, ALK, BRAF, and KRAS. He has metastases to liver, lymph nodes, adrenal glands, pelvis, and spine. He has a T1 pathologic fracture with high-grade cord compression; on exam he is 4+/5 strength but severely myelopathic. His ECOG performance status is 4 and SINS 15. This patient does not harbor any favorable mutation for targeted therapy and is already presenting with advanced disease. Medical Oncology does not consider him a candidate for systemic treatment currently. Patient is not offered surgery and palliated with best supportive care. (Figure 4) Sagittal and axial CT and MRI demonstrating lytic T1 pathologic fracture with epidural extension. Spinal Instability neoplastic Score of 16.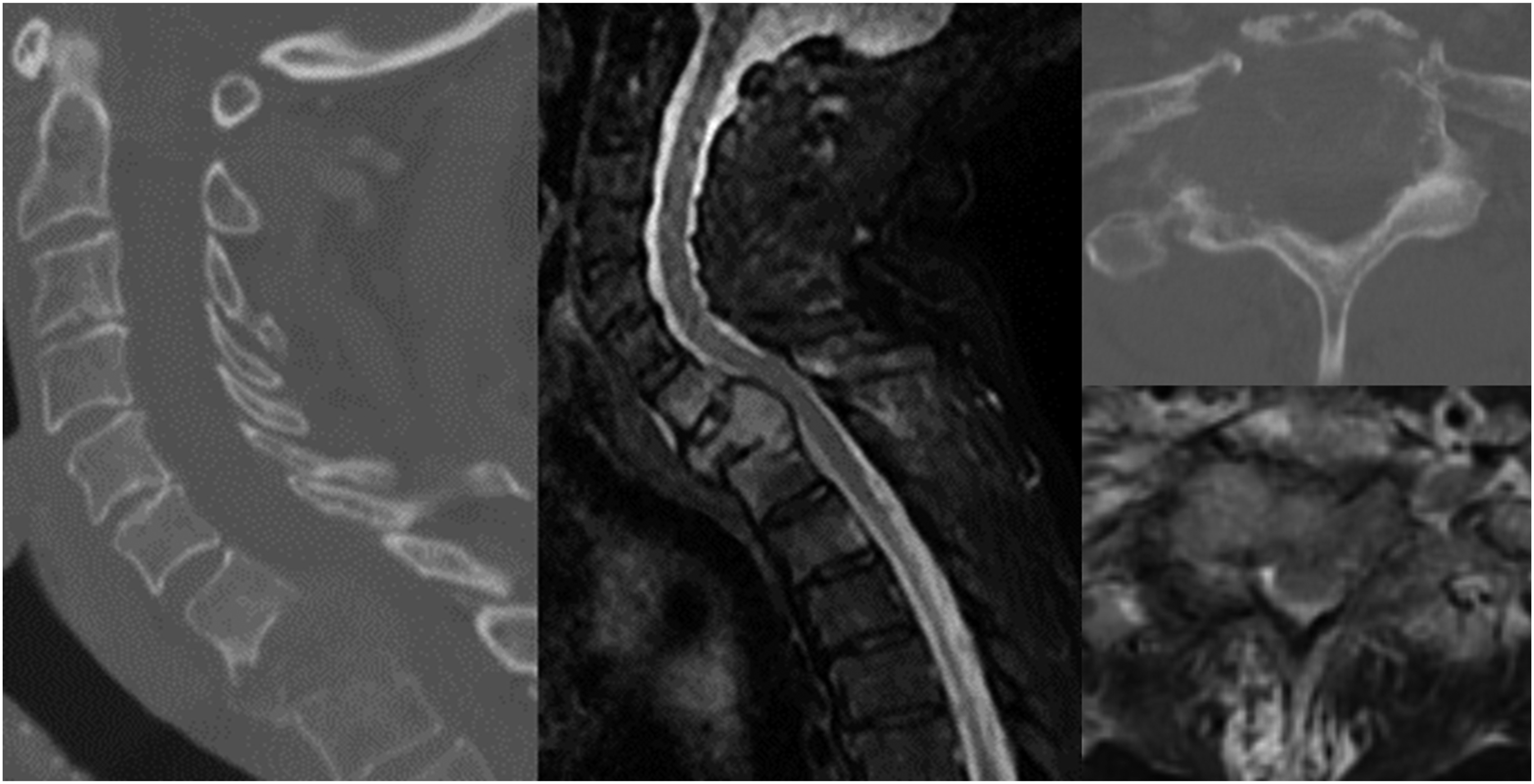
Strengths, Weaknesses, and Limitations
This manuscript aims to provide a general overview of important molecular markers and targeted therapies for the most common neoplasms (lung, breast, prostate and melanoma) that metastasize to the spine and offer guidance on how to best incorporate them in the clinical setting. A simplified discussion of relevant molecular markers is provided with the goal of providing a framework for incorporation of these molecular markers into a surgeon’s existing practice. Although a comprehensive review of the newest updates for each histology is not provided, this would be beyond the scope of the current manuscript, and furthermore, would most likely be quickly out of date, given the rapid discovery of genomic influencers of disease and the rapid development of novel therapeutics. With this in mind, we provide 3 relevant questions that can be used for any histology in order to simplify a surgeon’s decision-making algorithms in regards to the influence of molecular markers and systemic therapies. The case examples provided attempt to emphasize the influence of the molecular markers/systemic lines of therapy on surgical decision-making, independent of the neurologic deficits and overall physiologic condition of the patient. In terms of management differences globally, given the differences in resources, access, and practice patterns in developed and developing countries, our framework may have broader applicability as the questions can be tailored to an individual surgeon’s existing practice irrespective of the available resources. Taken together, we aim to provide a more functional algorithm, in which surgeons can incorporate molecular markers and therapeutics into their decision-making process.
Conclusion
Survival of patients with metastatic cancer has significantly improved in recent years. Molecular profiling of tumors has shown that patients with certain mutations have improved survival even if the primary histology is associated with high mortality, such as lung cancer. In this review, we highlighted important mutations and corresponding targeted therapies for the most common cancers that metastasize to the spine. Incorporation of molecular profiling into the decision-making framework is needed, as it may allow for better patient selection and outcome.
Footnotes
Acknowledgments
This study was organized by the AO Spine Knowledge Forum Tumor, a group of international spine oncology experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organisation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Deemed exempt from requirement given nature of study.