
Abstract
Study Design
International survey.
Objectives
To assess variability in the treatment practices for spinal metastases as a function of practice setting, surgical specialty, and fellowship training among an international group of spine surgeons.
Methods
An anonymous internet-based survey was disseminated to the AO Spine membership. The questionnaire contained items on practice settings, fellowship training, indications used for spinal metastasis surgery, surgical strategies, multidisciplinary team use, and postoperative follow-up priorities and practice.
Results
341 gave complete responses to the survey with 76.3% identifying spinal oncology as a practice focus and 95.6% treating spinal metastases. 80% use the Spinal Instability Neoplastic Score (SINS) to guide instrumentation decision-making and 60.7% recruit multidisciplinary teams for some or all cases. Priorities for postoperative follow-up are adjuvant radiotherapy (80.9%) and systemic therapy (74.8%). Most schedule first follow-up within 6 weeks of surgery (62.2%). Significant response heterogeneity was seen when stratifying by practice in an academic or university-affiliated center, practice in a cancer center, completion of a spine oncology fellowship, and self-identification as a tumor specialist. Respondents belonging to any of these categories were more likely to utilize SINS (P < .01-.02), recruit assistance from plastic surgeons (all P < .01), and incorporate radiation oncologists in postoperative care (P < .01-.03).
Conclusions
The largest variability in practice strategies is based upon practice setting, spine tumor specialization, and completion of a spine oncology fellowship. These respondents were more likely to use evidenced-based practices. However, the response variability indicates the need for consensus building, particularly for postoperative spine metastasis care pathways and multidisciplinary team use.
Introduction
Vertebral body metastases are by far the most common tumor of the spinal cord and spinal column, occurring at a rate of 11-26 per 100 000 persons per year.1,2 Given the increased survival of patient with spine metastasis, 3 there is a growing number of patients with spine metastases. Many of these patients have indications for surgical intervention and management frequently depends on the effective collaboration of stakeholders from multiple specialties. Despite this, there are no broadly accepted guidelines for the management of spinal metastases. Pursuant to this, there is likely variability in the treatment strategies applied to this patient. 4 However, little is known about the extent of this variability or whether the variability is influenced by practice setting, specialization, or age. In the present study, we surveyed the AO Spine membership to identify variability in indications for surgery, utilization of multidisciplinary care teams, and structure of postoperative treatment pathways to identify potential areas for consensus building.
Methods
Population Studied
Emails were sent to all enrollees in the AO Spine email listserv in February 2021. AO Spine (www.aospine.org) is an internationally recognized professional spine community dedicated to education and research for the purposes of improving spine patient care and outcomes. The listserv included 28 915 recipients, of whom 4700 are dues-paying AO Spine members. The email included a cover letter outlining the goals of the survey and the importance of the study along with a link to the SurveyMonkey Inc. questionnaire (San Mateo, CA). Respondents were given 3 weeks to complete the form with a reminder sent at the 2-week time point. Survey participation was anonymous.
Survey Items
Supplementary material 1 shows the survey items that were sent to respondents. Items were blocked into four sections: (1) general respondent demographics, (2) hospital characteristics, (3) surgical practices for spine metastases, and (4) postoperative treatment practices. The first two sections included items on hospital setting, respondent specialty, practice make-up, practice volume, and case-mix. Surgical practices examined included indications for surgical intervention and strategies employed for patients with instability or neural element compression. Additionally, the use of multidisciplinary teams, tumor boards, and the recruitment of plastic and reconstructive surgery (PRS) specialists were examined. Last, items on postoperative treatment include postoperative treatment priorities, timing of resumption of systemic therapy and radiotherapy, and timing of follow-up. Those completing fellowships had their fellowship categorized as a spinal oncology fellowship if >10% of the time was dedicated to the treatment of spine tumors.
Statistical Analysis
Results were collated using Microsoft Excel (Redmond, WA) and analyzed using Tibco v.13.3 (Statistica, Palo Alto, CA). Data are reported as counts and percentages. Only complete response data were analyzed. Comparisons of practice behaviors by surgical specialty, practice setting and make-up, and surgical training were made using Fisher exact tests and χ2-analyses. Statistical significance was defined as P < .05.
Results
Respondent Demographics, Training and Practice Settings
Demographics of Survey Respondents and Affiliated Institution Characteristics. Results Are Presented for Entire Cohort and for Respondents Who Completed the Survey.
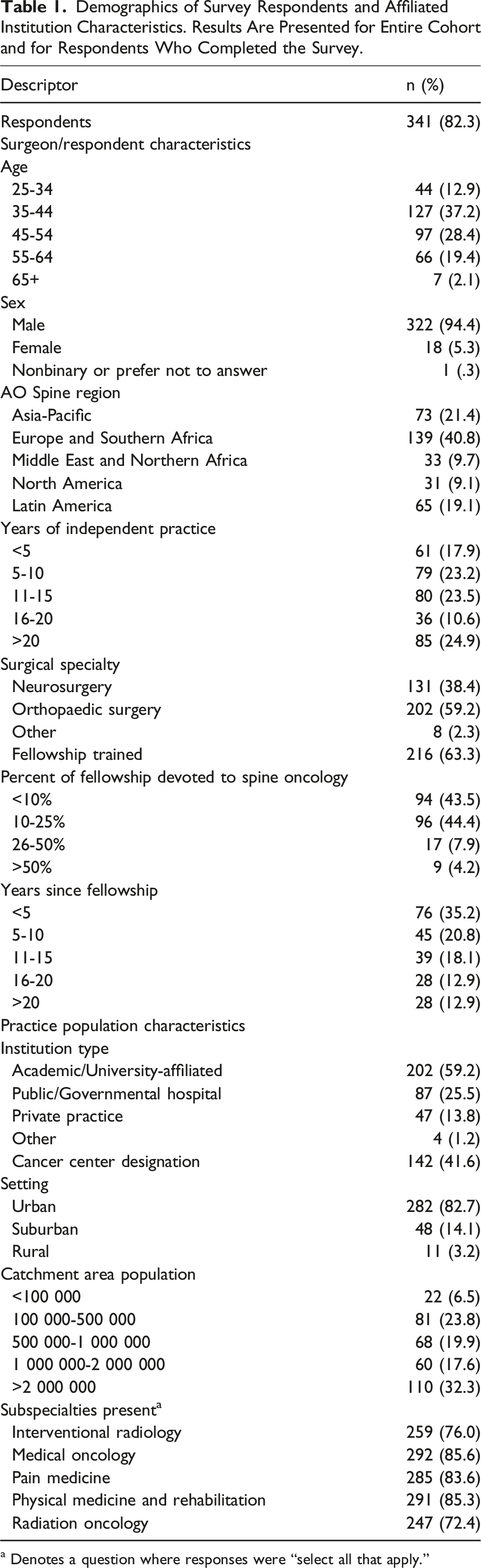
a Denotes a question where responses were “select all that apply.”
Practice Characteristics of Survey Respondents. Results Are Presented for Entire Cohort and for Respondents Who Completed the Survey.
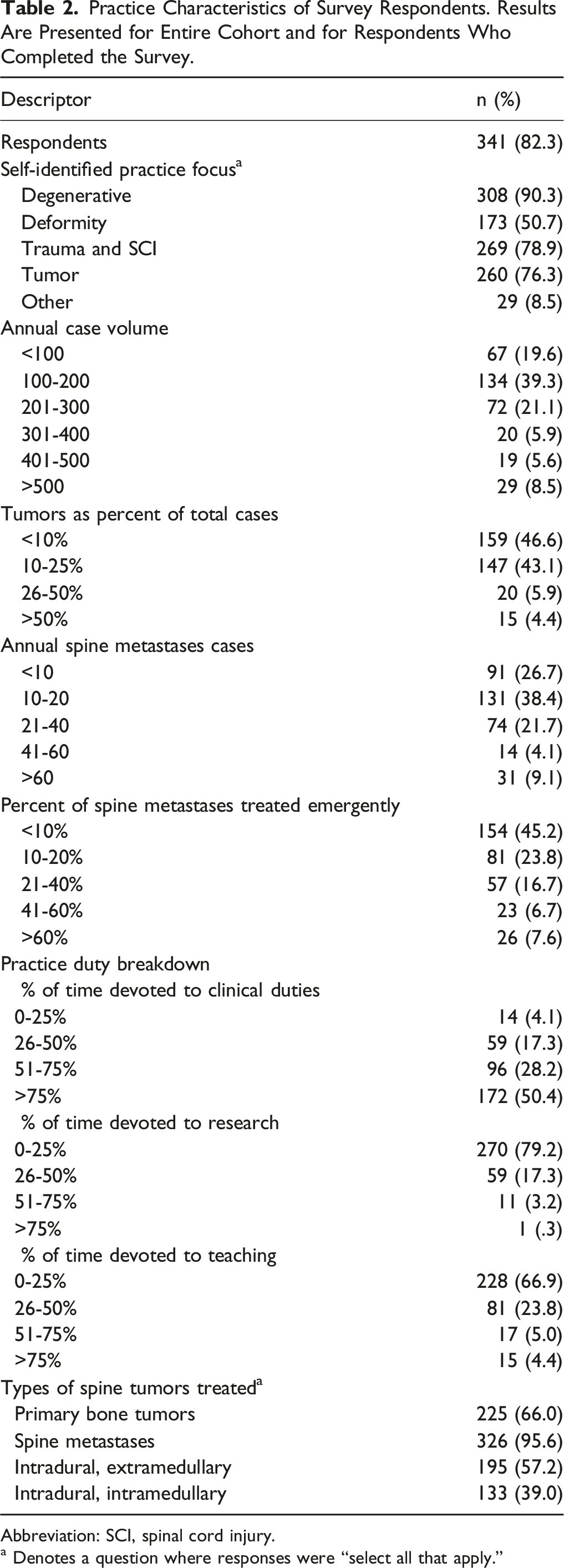
Abbreviation: SCI, spinal cord injury.
a Denotes a question where responses were “select all that apply.”
Surgical Indications and Strategies
Indications for Surgical Management, Surgical Strategies Employed.
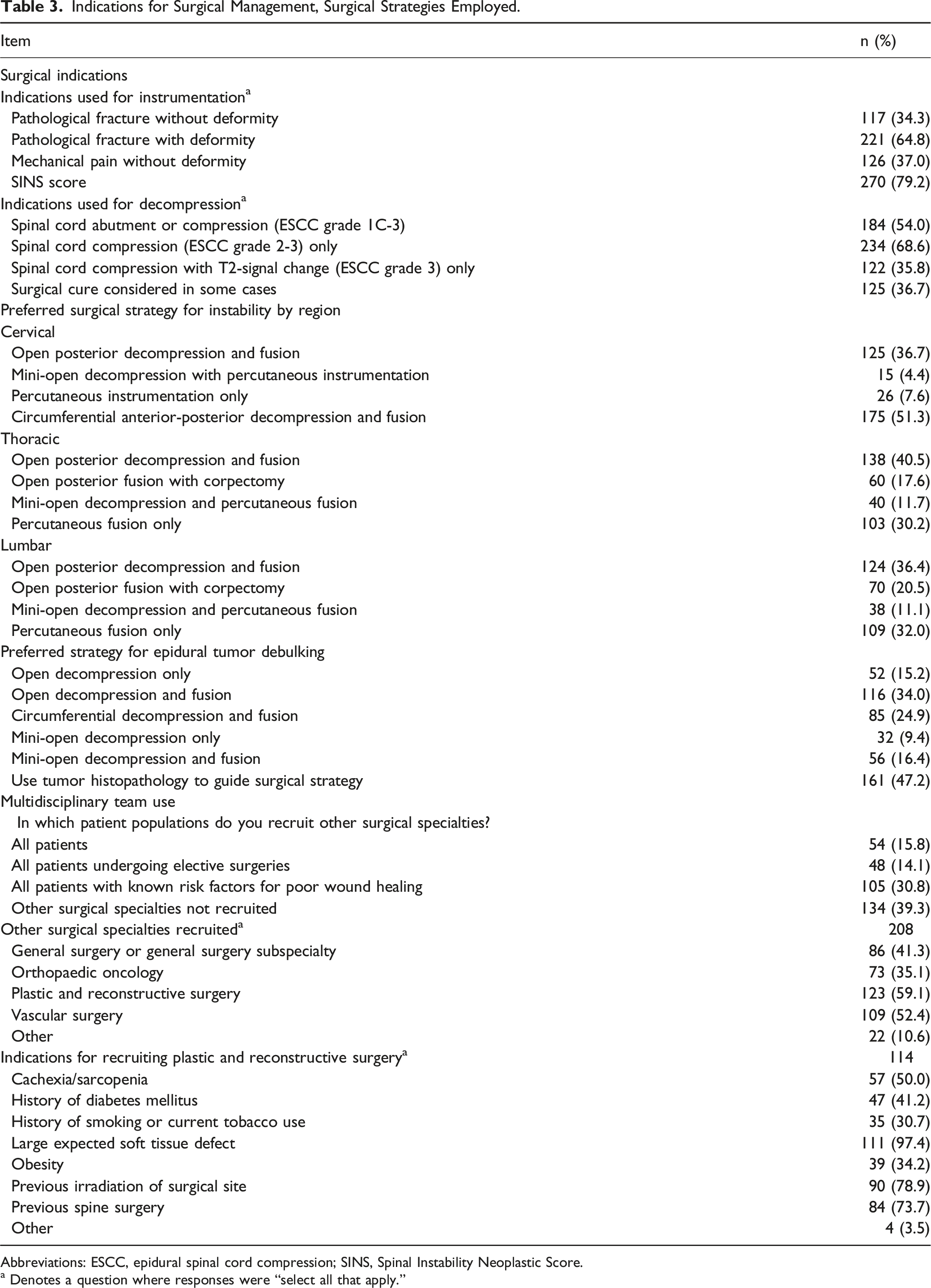
Abbreviations: ESCC, epidural spinal cord compression; SINS, Spinal Instability Neoplastic Score.
a Denotes a question where responses were “select all that apply.”
Surgical strategies for instrumented stabilization were most variable for lumbar metastases and least variable for cervical metastases. For cervical lesions, most surgeons favored open posterior decompression and fusion (36.7%) or circumferential anterior-posterior decompression and fusion (51.3%). For thoracic and lumbar lesions, open posterior decompression and fusion (40.5% and 36.4%, respectively) and percutaneous fusion only (30.2% and 32.0%, respectively) were the most popular strategies. For patients with epidural disease requiring decompression but without underlying instability, open decompression and fusion (34.0%) followed by circumferential decompression and fusion (24.9%) were the most popular strategies; minimally invasive (MIS) approaches were the preferred strategy for only 25.8% of respondents.
Nearly sixty-one percent recruited other specialties as part of the surgical team, most commonly for patients with risk factors for poor wound healing (50.7%). Plastic and reconstructive surgery (59.1%) and vascular surgery (52.4%) were the most commonly recruited specialties. Of those enlisting the services of plastic surgery, the most common reasons reported were a large expected soft tissue defect following decompression (97.4%), previous irradiation of the surgical site (78.9%), and prior surgery at the operative site (73.7%).
Multidisciplinary Teams, Postoperative Follow-up Priorities and Practices
Timing and Composition of Multidisciplinary Teams, Postoperative Care Priorities, and Follow-Up Strategies.
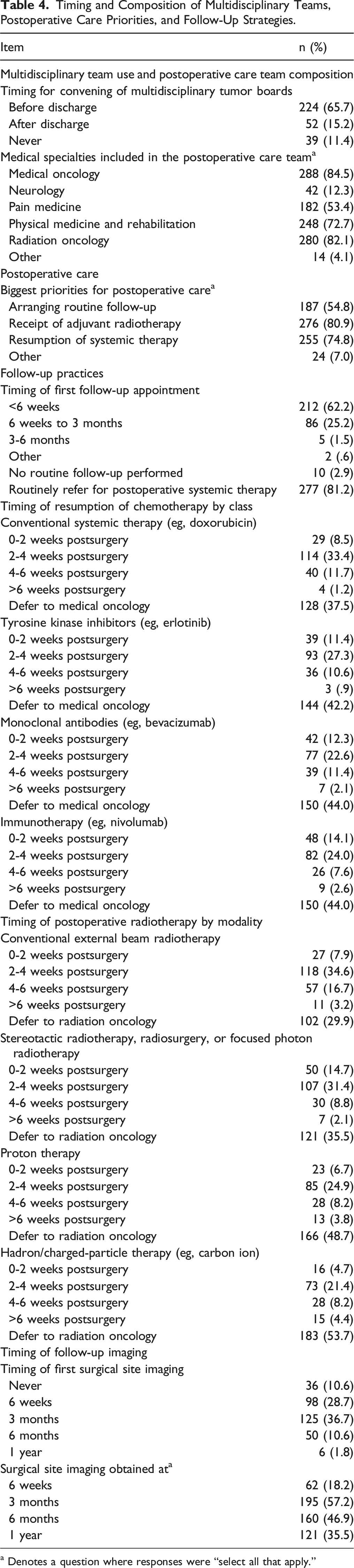
a Denotes a question where responses were “select all that apply.”
The biggest priorities for postoperative care were resumption of systemic therapy (74.8%) and administration of adjuvant radiotherapy (80.9%). Most surgeons scheduled first follow-up within 6 weeks of surgery (62.2%) and obtained the first images at the 6-week (28.7%) or 3-month follow-up (36.7%). A plurality of surgeons deferred to medical oncologists regarding the initiation of postoperative chemotherapy (37.5-44.0%), though the most popular timing for those demonstrating a preference was 2-4 weeks post-surgery. This was seen for all agent classes: conventional therapy (33.4%), tyrosine kinase inhibitors (27.3%), monoclonal antibodies (22.6%), and immunotherapy (24.0%). A large proportion similarly deferred to radiation oncologists for the timing of postoperative radiotherapy. However, this preference was strongest for proton therapy (48.7%) and hadron therapy (53.7%), perhaps due to the lower availability of and familiarity with these modalities. For conventional external beam radiotherapy (34.6%) and stereotactic radiotherapy (31.4%), the most commonly preferred timeframe was 2-4 weeks post-surgery.
Behavior as a Function of Training and Practice Setting
Comparison of Surgical Strategies and Indications for Stabilization and Decompression by Training Specialty, Practice Type, Practice Setting, Cancer Center Designation, and Completion of a Spine Oncology Fellowship.
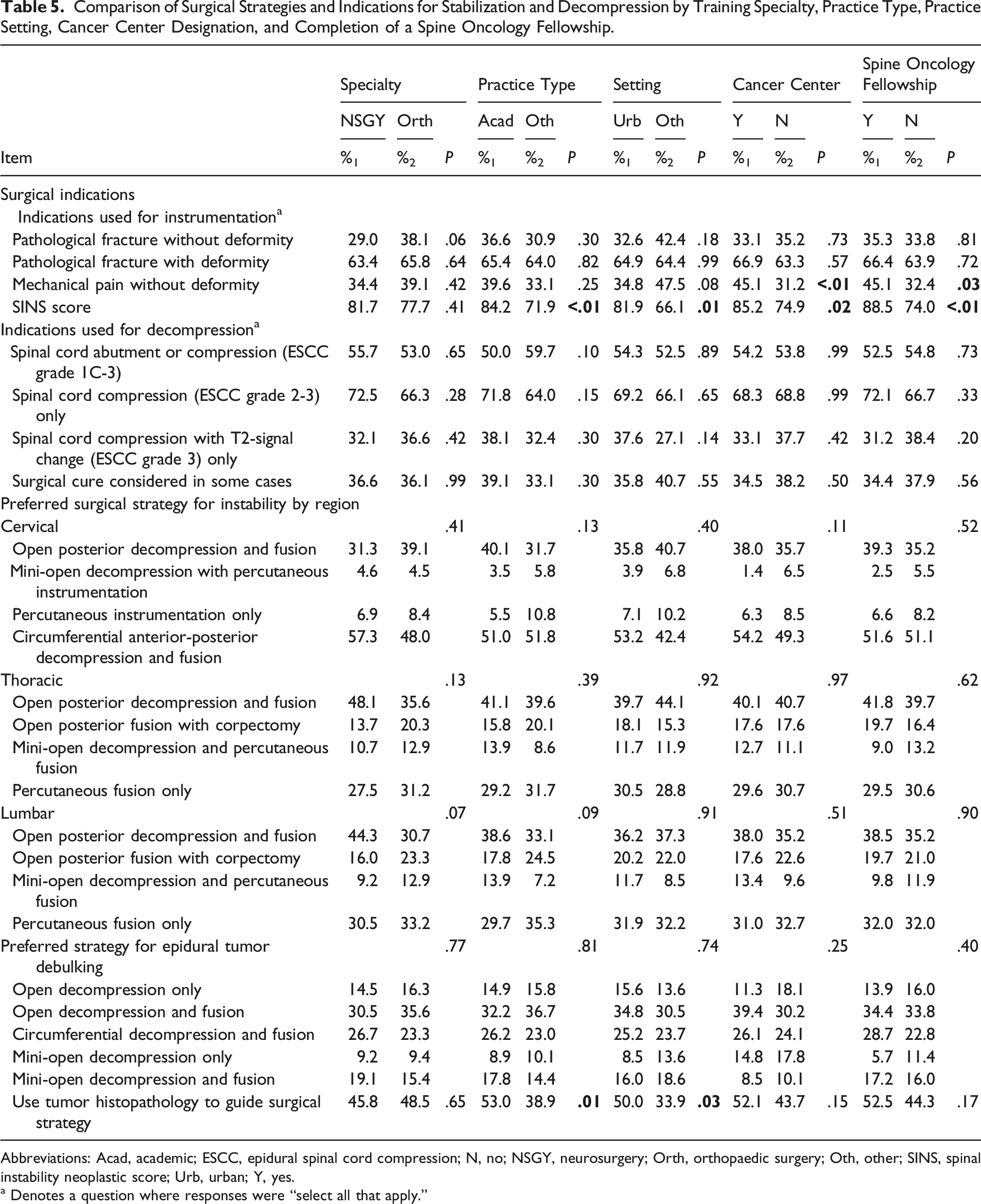
Abbreviations: Acad, academic; ESCC, epidural spinal cord compression; N, no; NSGY, neurosurgery; Orth, orthopaedic surgery; Oth, other; SINS, spinal instability neoplastic score; Urb, urban; Y, yes.
a Denotes a question where responses were “select all that apply.”
Comparison of Multidisciplinary Team Recruitment and Composition by Training Specialty, Practice Type, Practice Setting, Cancer Center Designation, and Completion of a Spine Oncology Fellowship.
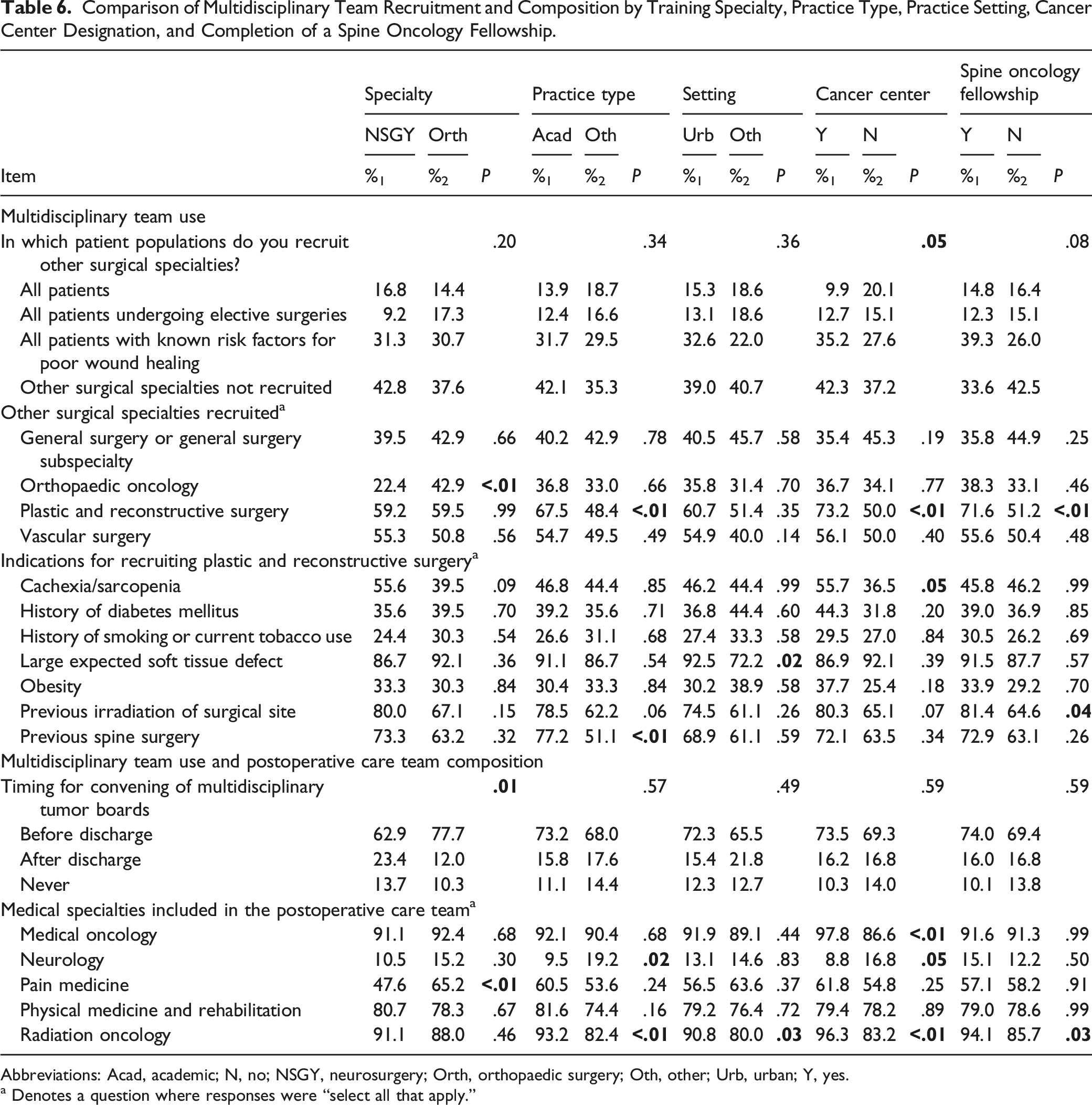
Abbreviations: Acad, academic; N, no; NSGY, neurosurgery; Orth, orthopaedic surgery; Oth, other; Urb, urban; Y, yes.
a Denotes a question where responses were “select all that apply.”
Comparison of Postoperative Treatment Strategies and Follow-Up by Training Specialty, Practice Type, Practice Setting, Cancer Center Designation, and Completion of a Spine Oncology Fellowship.
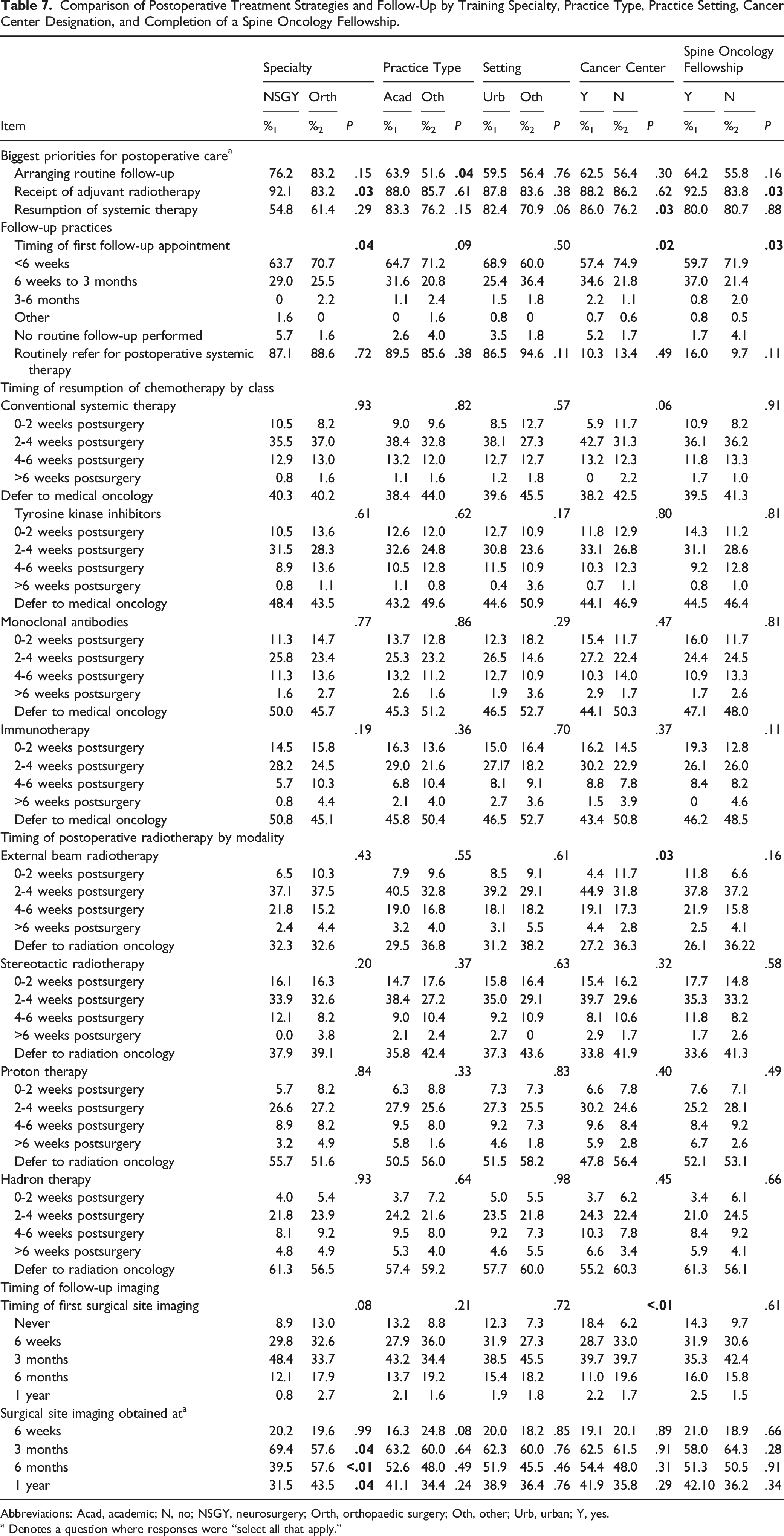
Abbreviations: Acad, academic; N, no; NSGY, neurosurgery; Orth, orthopaedic surgery; Oth, other; Urb, urban; Y, yes.
a Denotes a question where responses were “select all that apply.”
Of note, there were differences in the practices of respondents who self-identified as having a tumor focus as part of their practice (Supplementary material 2). `These respondents were less likely to operate for pathological fracture without deformity (30.8 vs. 45.7%; P = .02) and more likely to use SINS to guide this decision (85.0 vs. 60.5%; P < .01). They were also more likely to use spinal cord compression (72.7 vs. 55.6%; P < .01) as their threshold for surgical decompression and less likely to include other specialties in the surgical team (P = .01). However, those recruiting other teams were more likely to include plastic surgeons (64.9 vs. 43.9%; P < .01). Spine tumor specialists also more commonly recruited medical oncologists, physiatrists, and radiation oncologists in the postoperative care team (P < .01-.02) and more commonly prioritized resumption of systemic therapy (83.9% vs. 68.1%; P < .01). Similarly, those who completed spine oncology fellowships (Tables 5-7) were more likely to use the presence of mechanical pain without deformity (45.1 vs. 32.4%; P = .03) and SINS (88.5 vs. 74.0%; P < .01) as indications for instrumentation, to include plastic surgeons in their surgical teams (71.6 vs. 51.2%; P < .01), to recruit the assistance of plastic surgeons for patients with prior radiotherapy (81.4 vs. 64.6%; P = .04), to incorporate radiation oncologists in their multidisciplinary teams (94.1 vs. 85.7%; P = .03), and to see receipt of adjuvant radiotherapy as a priority for postoperative care (92.5 vs. 83.8%; P = .03).
Differences were also noted in those practicing at academic/university-affiliated versus non-academic centers and between those practicing in nationally recognized cancer hospitals versus other facilities (Tables 5-7). Those practicing in academic hospitals were more likely to use the SINS (84.2 vs. 71.9%; P < .01), to use histology to guide surgical strategy (53.0 vs. 38.9%; P = .01), to recruit plastic surgeons for their surgical teams (67.5 vs. 48.4%; P < .01), to use plastic surgeons in patients with prior spine surgery (77.2 vs. 51.1%; P < .01), to recruit radiation oncologists for their postoperative care teams (93.2 vs. 82.4; P < .01), and to see routine follow-up as a priority of postoperative care (63.9 vs. 51.6%; P = .04). Those practicing at cancer centers more commonly used mechanical pain without deformity (45.1 vs. 31.2%; P < .01) and SINS (85.2 vs. 74.9%; P = .02) to guide the use of instrumentation, to recruit plastic surgeons for their surgical teams (73.2 vs. 50.0%; P < .01), to use cachexia or sarcopenia as an indication for plastic surgery closure (55.7 vs. 36.5%; P = .05), to include radiation oncologists in their postoperative care teams (96.3 vs. 83.2%; P < .01), and to see resumption of systemic therapy as a priority for postoperative care.
Discussion
Vertebral column metastases are the most common type of spine tumor1,2 and autopsy studies suggest they affect up to 80% of patients with advanced cancer. 5 Despite the ubiquity of these lesions, there remain no uniformly accepted guidelines, and previous studies have shown heterogeneity in outcomes based upon where and from whom a patient receives care. 6 The present results suggest that this heterogeneity in outcomes may in part stem from differences in the type and level of training of spine providers. Those with formalized spine oncology fellowship training, those with practices having a tumor focus, and those practicing at a university or academic center appear more likely to base instrumentation decision-making on the systematic, formalized SINS framework, to recruit the assistance of plastic and reconstructive surgeons for wound closure, and to involve radiation oncologists in the postoperative care of those with spinal metastases. Each of these draws support from the literature. The SINS framework has been extensively validated 7 and shown to successfully predict patient-reported outcomes following instrumented stabilization for spinal metastasis. 8 Recruitment of plastic surgery has been suggested to reduce wound complications in patients operated for spine metastases9,10 and is consequently utilized by many centers, as illustrated here. Likewise, postoperative adjuvant radiotherapy improves local tumor control. 11 However, this body of evidence is considered low quality, as echoed by a recent publication of the Spinal Oncology Study Group, the precursor to the current AO Spine Knowledge Forum Tumor. 12
Also, the present survey results identified several differences in surgical indications and practice patterns across the AO regions (Supplemental material 2). Notably, there was great similarity in the responses given by those from the Europe and South Africa and the North America regions with regard to surgical indications. Respondents from these regions were also the most likely to recruit assistance from other surgical specialties for only patients with poor wound healing or to altogether forego assistance from other specialties. Postoperatively, respondents for these regions were least likely to recruit assistance from pain medicine specialists and most likely to recruit assistance from radiation oncologists; they also most commonly cited resumption of systemic therapy as a postoperative care priority. Though the basis for these differences is unclear, it may be due to the geographical differences in treatment philosophies. Providers from these regions may see surgery as a temporizing measure designed to improve the patients’ quality-of-life enough to expedite resumption of the broader treatment regimen. However, the current data lack the granularity to support or refute this supposition. Nevertheless, they do highlight the need for consensus building in multiple spinal oncology issues.
Areas for Investigation and Consensus Building
In their 2016 issue focusing on the state of the spine metastases literature, the AO Spine Knowledge Forum Tumor made several recommendations about the management of patients with spine metastases. The majority of these recommendations were graded as “weak” though, and all were based upon low or very low quality of evidence. Additionally, the recommendations predominately focused on perioperative issues with the most detailed recommendations focusing on the administration of adjuvant stereotactic beam radiotherapy (SBRT). With the exception of the weak recommendation that ESCC grade 2 or 3 lesions be debulked before SBRT, none of the recommendations attempted to identify strategies for decompression or instrumentation based upon the validated ESCC 13 or SINS 8 scoring systems. As both systems have gained increased utilization and allow for objective comparison of outcomes and indications across providers, guidelines based upon them might see increased adoption across the spine community.
Additionally, the 2016 AO Spine Knowledge Forum Tumor's recommendations largely avoided the issues of priorities of postoperative care, follow-up practices, and the timing of resumption of postoperative radiotherapy or systemic therapy. The present results find that the majority of respondents view the resumption of systemic therapy (74.8%) and administration of adjuvant radiotherapy (80.9%) as priorities of postoperative therapy. Despite this, there is still great uncertainty amongst providers about the optimal timing for adjuvant radiotherapy and the resumption of systemic therapy. Similarly, there is significant heterogeneity in practices depending upon practice setting (academic/university-affiliated vs. non-academic and designated cancer center vs. other), provider training (spinal oncology fellowship vs. not), practice focus (tumor vs. not), and geographic region. This suggests that the quality of care received by patients may vary widely simply based upon the location of their residence. Such a notion has been supported by prior examinations of data from the United States. 6 These data have shown that patients receiving care from surgeons performing large numbers of spine metastases operations (e.g., those with a tumor-focus) and those receiving care at hospitals performing large number of spine metastases operations (e.g., designated cancer centers) have lower rates of complication and unintended readmission. Similarly, data from the lumbar degenerative disease literature have identified significant geographic variation in rates of arthrodesis and postoperative complications.14,15 Consequently, the geographic variations seen in the present data may reflect non-evidenced-based biases that would benefit from the development of broader guidelines.
Additionally, the AO Spine Knowledge Forum Tumor guidelines did not attempt to address the utilization of multidisciplinary surgical teams or tumor boards in patient care. Over 60% of respondents reported using collaborating with other surgical teams for some or all patients, and nearly 90% endorsed using multidisciplinary tumor boards to formulate care plans for patients with spine metastases. Prior studies have found heterogeneity even amongst the care provided at centers with established tumor boards, 16 and despite the publication of experiences from multiple centers,16-18 it is unclear to what degree tumor boards facilitate better outcomes. It is similarly unclear when they should meet to discuss patient cases, what structure they should adopt for case discussion, and which medical specialties should be recruited for these teams. 18 Consequently, there appears to be a need for consensus building on these topics to help ensure a uniformly high-level of care for spine metastasis patients.
As the present study was intended as cross-sectional, specific guidelines cannot be generated based upon the present data. Nevertheless, the significant disparities in practices identified within the survey help to highlight the need for such guidelines to help ensure a uniformly high level of care for all patients. Additionally, the priority that most providers place on the resumption of systemic therapy and administration of adjuvant radiotherapy postoperatively indicates the need for guidelines on these topics. Said guidelines should not only identify those patients most likely to benefit from these interventions, but also the proper timing for these surgical adjuvants as a wide range of timeframes were recommended by survey respondents with a large plurality completely deferring to medical and radiation oncologists, especially for novel chemotherapeutic agents and charged particle therapies.
Limitations
There are several limitations to the present data. Foremost, while over 300 surgeons completed the survey, this represents at most 5% of the AO Spine membership, potentially limiting the generalizability of the results. Notably, the survey was sent to a large cohort—the entire AO Spine listserv, which includes some 28 000 persons, meaning that the actual response rate may have been as low as 1%. This low response rate, while consistent with contemporaneously conducted surveys of the AO Spine community, 19 means that the results may not be reflective of the practices of a majority of spine surgeons worldwide. Additionally, the classification of respondents as tumor specialists was based upon respondent self-identified specialization, which could create response bias. Another potential limitation of the present results is that some of the analyses may have insufficient power to yield meaningful results due to the small group sizes. Also, in an attempt to keep the survey to a manageable length while still address core elements of spinal oncology care, some of the question in the survey were necessarily broad. The lack of granularity limits the ability of the survey results to determine how surgeons would act in specific situations. Nevertheless, in order to try and minimize the ambiguity of survey wording and to ensure the survey touched on the major topics of interest, the survey was reviewed by a small set of members of the AO Spine community prior to dissemination. Along these same lines, as the survey was designed to elicit general practices from respondents and did not ask query surgeon preferences as applied to specific patient cases, it is possible that the results may reflect guiding principles employed by surgeons, which may not be applicable in all cases. Nevertheless, we feel the present survey highlights the existing variability in treatment patterns that may indicate a need for consensus building amongst the spine oncology community.
Conclusion
Here, we illustrate the presence of significant variability in spine metastasis practice patterns worldwide, including surgical indications employed, multidisciplinary team utilization, and postoperative follow-up practices. There appear to be significant differences in provider practices based upon spine oncology specialization, practicing at an academic/university-affiliated center or designated cancer center, and having completed a spine oncology fellowship. These results suggest that the care received at designated cancer centers by dedicated, formally trained spine oncologists may differ from that provided elsewhere and highlights a potential need for further consensus building in spinal oncology to ensure a uniformly high-level of care for all patients.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211046904 – Supplemental Material for International Variability in Spinal Metastasis Treatment: A Survey of the AO Spine Community
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211046904 for International Variability in Spinal Metastasis Treatment: A Survey of the AO Spine Community by Zach Pennington, Jose L. Porras, Sheng-Fu Larry Lo and Daniel M. Sciubba in Global Spine Journal
Supplemental Material
sj-pdf-2-gsj-10.1177_21925682211046904 – Supplemental Material for International Variability in Spinal Metastasis Treatment: A Survey of the AO Spine Community
Supplemental Material, sj-pdf-2-gsj-10.1177_21925682211046904 for International Variability in Spinal Metastasis Treatment: A Survey of the AO Spine Community by Zach Pennington, Jose L. Porras, Sheng-Fu Larry Lo and Daniel M. Sciubba in Global Spine Journal
Footnotes
Acknowledgments
We would like to give a special thank you to Niccole Germscheid MSc and Dino Samartzis DSc for their assistance in constructing, disseminating, and compiling the results of the survey used to provide the data for the present study. We would also like thank the AO Spine members who took the time to complete the survey that provided results for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was organized and funded by AO Spine. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization.
Ethical Approval
RB approval was not required for the present study as it did not meet the definition of human subjects research.
ORCID iDs
Zach Pennington https://orcid.org/0000-0001-8012-860X
Jose L. Porras https://orcid.org/0000-0001-8664-7646
Sheng-Fu L. Lo https://orcid.org/0000-0001-7262-2544
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.