
Abstract
Study design
Retrospective multicenter cohort study.
Objective
Recurrent lumbar disc herniation (ReLDH) is a common condition requiring surgical intervention in a large proportion of cases. Evidence regarding the appropriate choice between repeat microdiscectomy (RD) and instrumented surgery (IS) is lacking. To understand the indications for either of the procedures and compare the results, we aimed to provide an overview of spine surgeon practice in France.
Methods
This retrospective, multicenter analysis included adults who underwent surgery for ReLDHs between December 2020 and May 2021. Surgeons were asked which of the following factors determined their therapeutic choice: radio-clinical considerations, non-discal anatomical factors, patient preference, or surgeon background. Data on preoperative clinical status and radiologic findings were collected. Patient-reported outcome measures (PROMs) were assessed and compared using propensity scores preoperatively and at 3 and 12 months postoperatively.
Results
The study included 150 patients (72 IS and 78 RD). Radioclinical elements, anatomical data, patient preferences
Conclusions
The decision-making process included both objective and subjective factors, resulting in patient satisfaction in 80.3% to 81.5% of cases, with significant clinical improvement in radicular symptoms in 75.8% to 91.8% of cases, and quality of life in 75.8% to 84.9% of cases, depending on the procedure performed.
Keywords
Introduction
In France, 25 000 to 30 000 patients undergo surgery for lumbar disc herniation each year. 1 Although this procedure is successful in most patients, reherniation-related symptoms are reported in 3% to 18% of cases. 2 Patients with surgically treated lumbar disc herniations are up to 10 times more likely to undergo future spinal surgery than the general population; 62% of these reoperations can be attributed to the recurrence of lumbar disc herniation. 3 As a result, nearly 3000 patients undergo surgery for recurrent lumbar disc herniation (ReLDH) each year in France. 1 Although there are many theories as to what increases a patient’s risk of reherniation, no single factor has been consistently identified in the literature. Proposed risk factors include obesity, smoking, male gender, diabetes, weight lifting, size of the annular tear, and type of primary surgery4-6.4-6
The surgeon has a wide range of options for recurrent disc herniation, from repeated microdiscectomy (RD) to instrumented surgery (IS), anterior or posterior arthrodesis, combined procedures, or even arthroplasty. All of these surgical techniques have been shown in the literature to provide good clinical outcomes; however, despite guidelines and numerous meta-analyses, the indications for each technique to determine the best surgical option remain unclear.7-9
In the absence of a clear recommendation, the decision-making process includes objective elements (clinical and radiological evidence) and more subjective elements (surgeon experience and patient opinion).8,10-12
The first recurrence is mostly treated with microdiscectomy alone; however, overall, there is a 69% and 22% probability that 2 randomly selected spine surgeons would disagree on the surgical treatment of two- and one-time recurrent disc herniations, respectively. 13
Therefore, in this area where evidence is lacking, our goal was to provide an overview of the practice of French spine surgeons regarding the management of recurrent lumbar disc herniation, to understand the factors that lead surgeons to choose 1 procedure over another, and to compare the results of different management strategies.
Methods
Study Population
On behalf of the French Society of Spine Surgery (Société Française de Chirurgie du Rachis, SFCR), we performed an observational retrospective analysis of prospectively collected data from 11 French institutions representative of French spine surgical practice (orthopedics, neurosurgeons, and private and academic hospitals). The participating centers were selected by the SFCR Scientific Committee on the basis of their representativeness of national surgical schools and their routine use of a similar data acquisition process. At each center, a corresponding practitioner was responsible for data collection. Patients were adults over the age of 18 who underwent surgery for ReLDH between December 2020 and May 2021, with a 12-month postoperative follow-up. The study protocol was approved by the Saint Jean Hospital research ethics committee (IRB: IORG0010765/N° CER-2023-GL02).
Surgical Indication
The choice of treatment modality between RD and instrumented surgery (IS, i.e., anterior or posterior instrumented fusion or lumbar arthroplasty) was based on several clinical and radiographic variables and was at the discretion of the operating surgeon.
For each decision, the corresponding surgeon at each center was asked about the main factors that determined the final therapeutic choice. The decision factors were grouped into 4 metagroups: (i) Decision based on an objective radio-clinical factor (predominant radicular or lumbar pain, predominant disc herniation, or inflammatory disc disease). (ii) Based on a nondiscal anatomical factor but orienting the technique (foraminal stenosis, multilevel spinal disorder, patient obesity, etc). (iii) Based on the patient’s preference (refusal of a complex surgery such as arthrodesis, request for a definitive procedure, and refusal of an anterior approach). (iv) Subjective factors linked to the surgeon’s background (initial training, personal posture, surgical school, availability of equipment or team, critical analysis of the literature).
Data Collection
Data were collected at inclusion during the preoperative consultation, and on the day of surgery, and postoperative evaluation was performed at three months and 12 months after surgery. Written informed consent was obtained from all patients. We collected relevant demographic medical history data, including sex, age, marital status, professional category (unemployment/retired, sedentary, at-risk work, hard work), workers’ compensation claim status, comorbidities, and smoking status.
Data collected preoperatively included the number of recurrences, time in months between the initial discectomy and repeat surgery, symptom duration, work stoppage duration and considering previous surgery: surgical complications, satisfaction numerical rating scales (NRS), duration of improvement, and the need for continuous analgesic medication. Clinical assessment by the surgeon included neurological assessment (radicular pain, type and level, and motor and sensitive status), low back pain, assessment of predominant symptoms, and whether the present neurological impairment was acquired from previous surgery. Motor status was defined as normal if it was equal to 5 on MRC scale (Medical Research Council) and abnormal when it was equal or above 4. 14
Radiological assessment was performed on preoperative MRI; ReLHD was characterized (herniation volume as small, medium, and large, and herniation position as excluded, migrated, or subligamentous); disc abnormalities (Pfirmann grading system, Modic classification, disc height); scar tissue was evaluated on post-contrast MRI; and instability was defined on dynamic lumbar X-rays.
Patient-reported outcome measures (PROMs) were assessed using different surveys: back and leg pain was assessed using NRS scores, 15 quality of life was assessed using the Oswestry Disability Index (ODI) score, and EuroQol-5D (EQ-5D). 16 Neuropathic pain was assessed using the Neuropathic pain questionnaire 4 score (DN4), which defines the presence of neuropathic pain when DN4 ≥ 4. 17
Postoperative evaluation was performed at 3 and 12 months to assess complications, including pseudarthrosis, analgesic prescription, neurological status, working status with the ability to return to work, the need for modified work, and the total duration of work stoppage, and PROMs: satisfaction NRS, 18 leg and back pain NRS, ODI, EQ-5D, and DN4.
Outcome Comparison
We compared 6 outcome measures between patients who had undergone RD or IS: 1) Overall patient satisfaction at 1 year postoperatively: Patients were considered satisfied with their care if they gave an overall score of >7 out of 10.
18
2) Return to work at 1 year postoperatively, defined in 3 categories: (i) return to work under the same conditions, (ii) return to work under modified conditions, and (iii) no return to work. 3) ODI evolution was defined as the absolute difference between the ODI at 1 year postoperatively and the preoperative ODI score. A commonly used criterion for success is minimal disability (i.e., an ODI of 20 points) at 1 year.
18
Others have suggested that an improvement of at least 13 points in 1 year could serve as a success criterion.
19
A change in the ODI score of less than 33% or a raw ODI score of 48 or more after surgery has been suggested as the criterion with the highest accuracy for defining failure and worsening after surgery for lumbar disc herniation.
20
4) The evolution of radicular NRS was defined as the absolute difference between the radicular NRS 1 year postoperatively and the preoperative radicular NRS. 5) The evolution of the lumbar NRS was defined as the absolute difference between the lumbar NRS at 1 year postoperatively and the preoperative lumbar NRS. The minimal clinically important change for NRS scales is approximately 1.5-2.0 points,
20
we defined a good clinical improvement on NRS scales as an improvement of at least 2 points. 6) The evolution of the EQ5D index before recurrence surgery and at 1 year postoperatively was defined as the absolute difference between the EQ5D index at 1 year postoperatively and the preoperative EQ5D index.
Statistical Analysis
All statistical analyses were performed with R software (version 4.2.3)
Qualitative variables were described as frequencies and percentages, and quantitative variables were described as means and standard deviations. The number of missing data is presented for each variable.
Quantitative variables were compared using Student’s t-test (or Mann–Whitney U test, when appropriate) and qualitative variables were compared using a Chi-squared test (or Fisher’s exact test, if necessary).
To eliminate the bias caused by differences in the observable characteristics between the 2 groups of patients (implants vs rediscectomy), an estimate of the propensity score was calculated. The covariates used for propensity score estimation were the variables associated with the 20% threshold in the univariate analysis according to the type of procedure (rediscectomy vs implantation). Missing data were managed by imputation using quantitative variables or the modal value of qualitative variables.
Outcome measures were compared between the 2 groups (RD and IS) using univariate regression models adjusted for propensity scores (linear regression for quantitative variables and logistic regression for qualitative variables). Model results are presented as odds ratios with 95% confidence intervals for logistic regressions and β coefficients with 95% confidence intervals for linear regressions.
Results
Demographic Data
This study included 150 patients who underwent surgery for recurrent lumbar disc herniation at 11 French spine centers. The mean age of the total population was 48 years and 53.3% of the patients were male. 72 (48%) patients underwent IS and 78 (52%) patients underwent RD without implants. The mean age was 48 years for patients undergoing IS and 49 years for patients undergoing RD. Approximately 46% of the IS patients were male, while 60% of the RD patients were male (not significant).
Demographic Data for Patients With Repeat Lumbar Disc Herniation Who Underwent Repeat Discectomy or Instrumented Surgery.
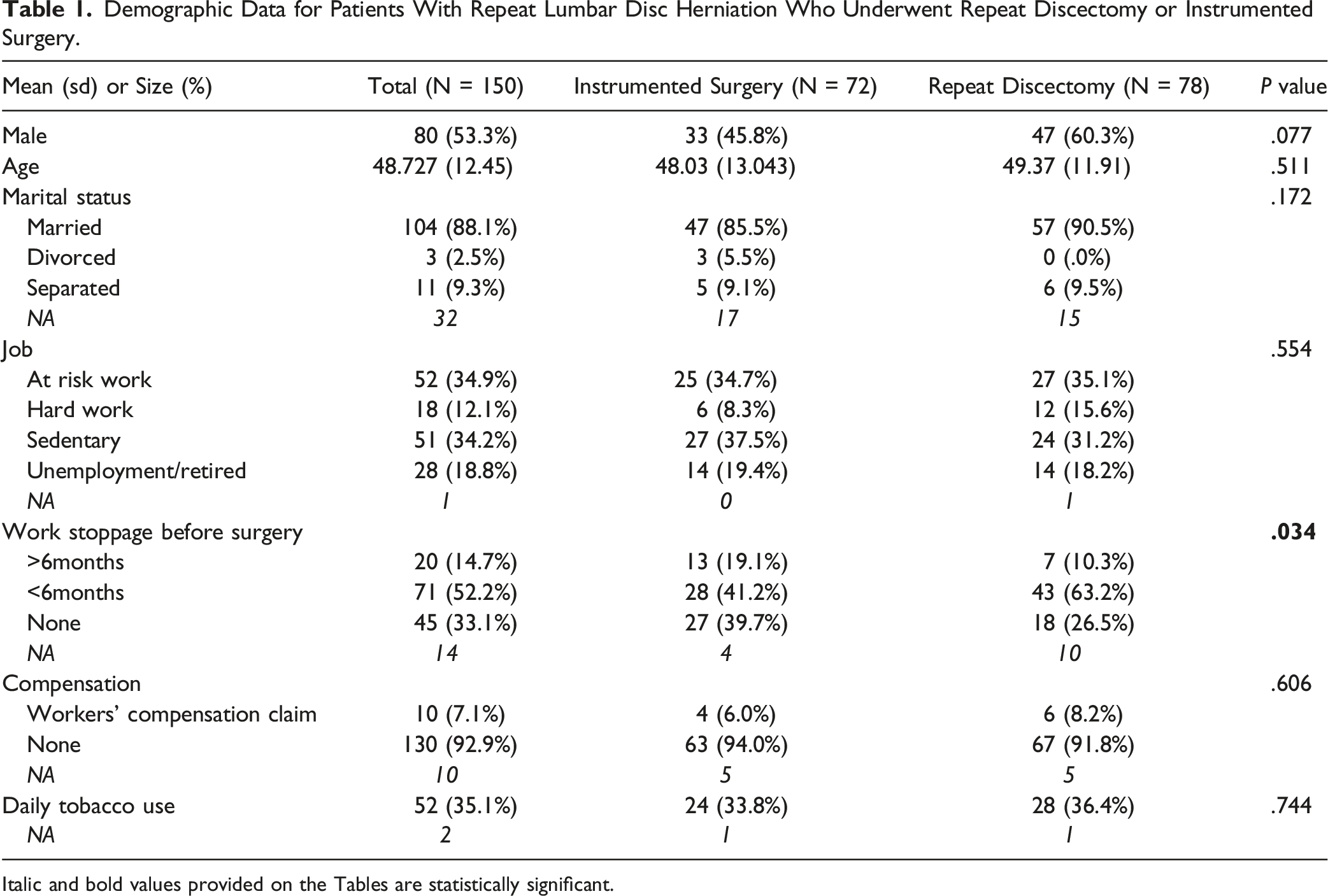
Italic and bold values provided on the Tables are statistically significant.
Clinico-Radiological Data
The distribution of elapsed time between previous surgery and ReLDH surgery was significantly different between the groups. In particular, 63% of patients who underwent RD for revision underwent surgery more than 2 years after the previous surgery, compared to 40% of patients who underwent IS.
The average number of recurrences was significantly higher in the IS group (1.25 vs 1.06 in the RD group).
Satisfaction after previous surgery, rated on a numerical scale, was significantly higher in the RD group (8.46 vs 6.85 out of 10 in the IS group).
The distribution of the duration of improvement after previous surgery was significantly different between the 2 groups. In particular, 54% of patients who underwent RD for revision had an improvement duration of more than 2 years compared to 29% of patients who underwent IS.
Patients who underwent revision with implants were significantly more likely to report lower back pain (LBP) for more than 6 months (77% vs 42% in the rediscectomy group).
The distribution of predominant symptoms was significantly different between the 2 groups. It was predominantly mixed (both lumbar and radicular) in the IS group (65%) and radicular only in the RD group (73%).
The distribution of Modic scores was significantly different between the 2 groups. It was mostly stage 1 in the IS group (49%) and stage 0 in the RD group (65%).
Preoperative Clinico-radiological Data for Patients With ReLDH Who Underwent Repeat Discectomy or Instrumented Surgery (n = 150).
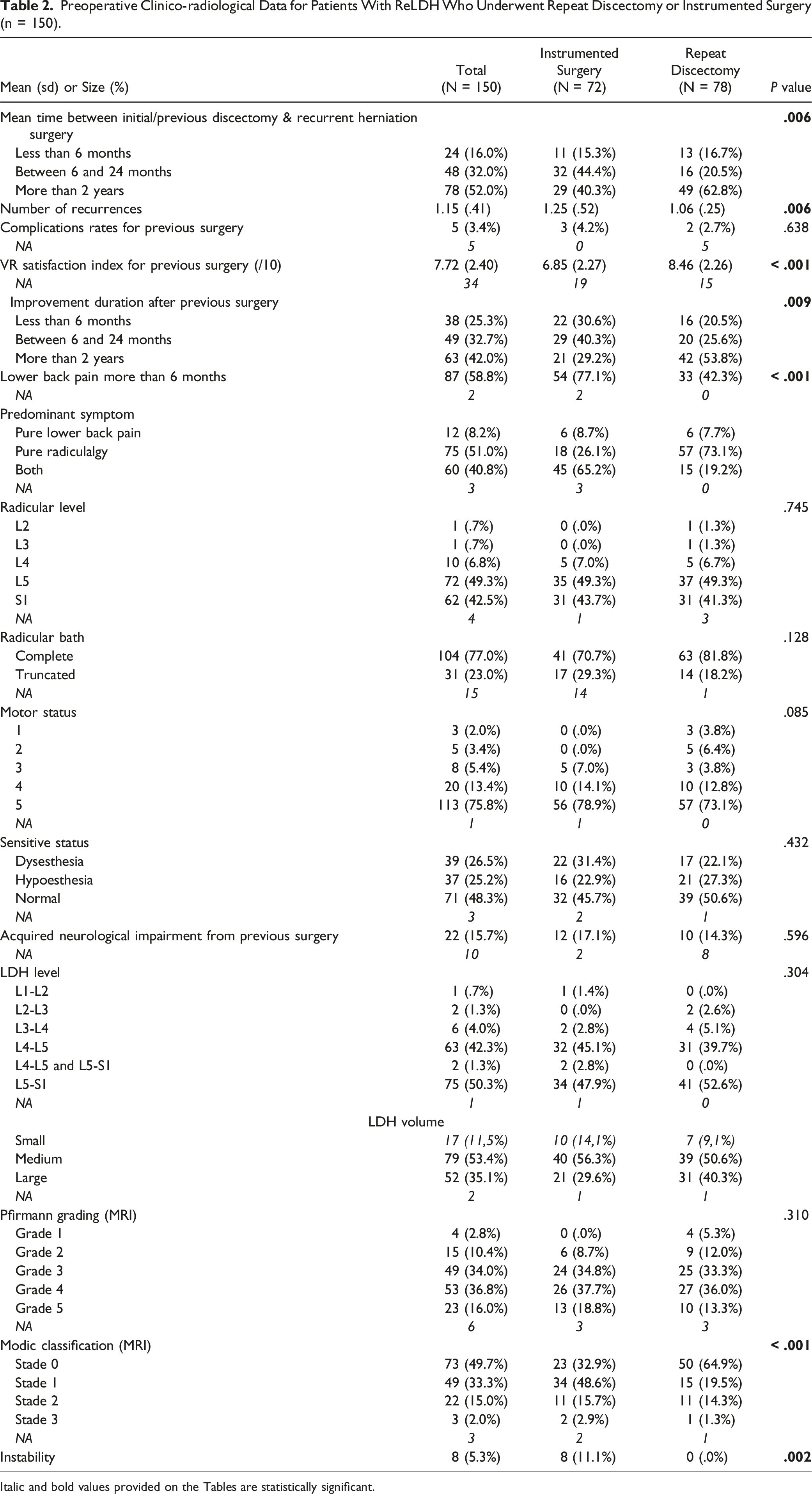
Italic and bold values provided on the Tables are statistically significant.
Surgeon decision
Description of the Surgeons' Indication Criteria According to the Chosen Technique (Instrumented Surgery or Repeat Discectomy).
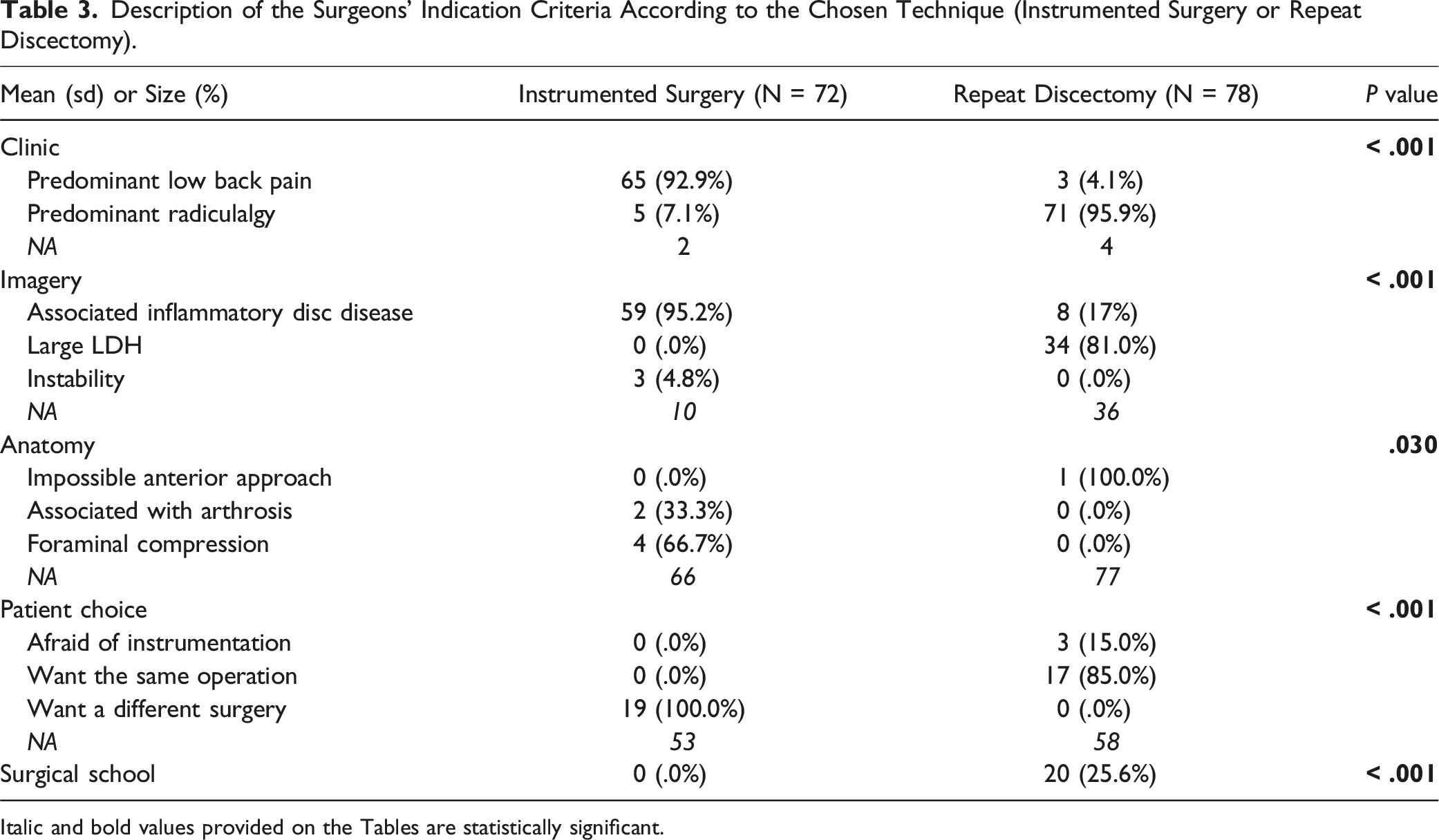
Italic and bold values provided on the Tables are statistically significant.
Factors related to surgeon background were significantly more common in the instrumented group (P = .0001) (Figure 1). Main factor for surgeon choice between repeat discectomy and instrumented surgery. Factors related to the surgeons' background are significantly more prevalent in the group of instrumented patients (P = .0001).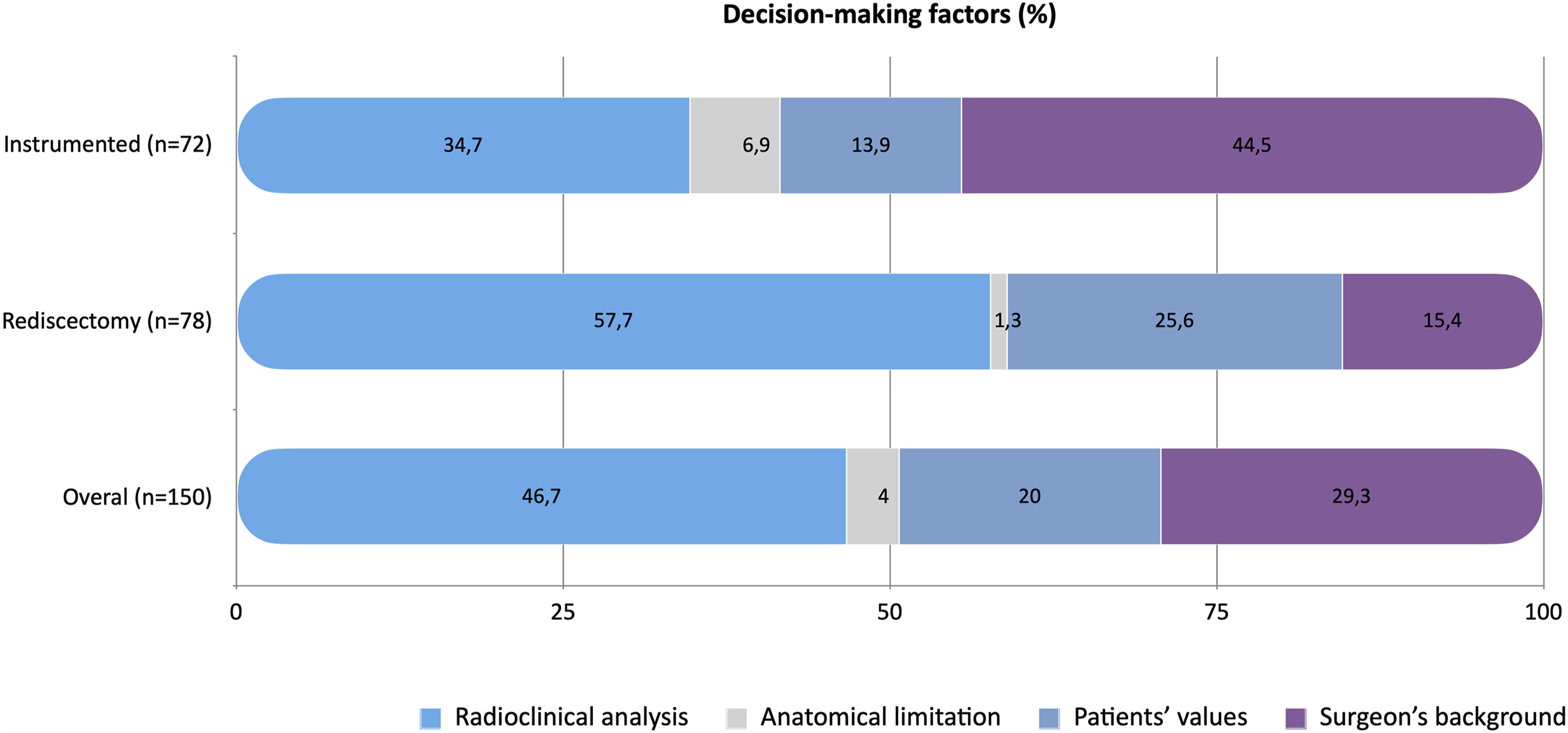
Surgical Outcome
One year after surgery, 9 complications (6.0%) were reported (4 infections, one of which resulted in pseudarthrodesis; 3 fractures; one postoperative hematoma; and 1 induced instability).
Of the 150 patients included in the study, 36 (24.2%) had abnormal motor status, including 15 (10.1%) in the IS group and 21 (14.1%) in the RD group. At 1 year, data were missing for 20 patients (13 in the IS group and 7 in the RD group). Of the remaining patients, 16 (12.3%) had abnormal motor status, including 5 (3.8%) in the IS group and 11 (8.5%) in the RD group.
PROMs
Regarding the ODI, among the 135 patients who were followed for 1 year, 47 (75.8%) patients in the IS group vs 62 (84.9%) patients in the RD group had a good clinical improvement in this score (defined by an improvement of at least 13 points in the score). At 1 year, 29 (46.8%) patients in the IS group vs 44 (60.3%) patients in the RD group had an ODI score ≤20 (a commonly used success criterion at 1 year). Five (8.1%) patients in the IS group had an ODI score improvement of less than 33%, while there were no such patients in the RD group. Finally, 9 (14.5%) patients in the IS group and four (5.5%) patients in the RD group had an ODI score ≥48 at 1 year. The last 2 criteria were suggested to be the most accurate in defining failure and postoperative worsening.
Among the 135 patients who were followed up for one year, 40 (64.5%) patients in the IS group vs 34 (46.6%) patients in the RD group showed good clinical improvement on lumbar NRS, while 47 (75.8%) patients in the IS group vs 67 (91.8%) patients in the RD group showed good clinical improvement on radicular NRS.
DN4 data were analyzed for 136 patients preoperatively and 130 patients 1 year postoperatively. Of these patients, 85 (62.5%) had neuropathic pain before revision surgery, including 39 (28.7%) in the IS group and 46 (33.8%) in the RD group; 42 (32.3%) patients had neuropathic pain at 1 year postoperatively, including 23 (17.7%) in the IS group and 19 (14.6%) in the RD group.
Propensity Scores for Outcome Measures
Surgical Outcomes at 1 Year Post-Operatively Compared by Type of Surgery on Patient Satisfaction, Return to Work, ODI, Lumbar and Radicular NRS, and EQ5D Index Adjusted on the Propensity Score (n = 115).
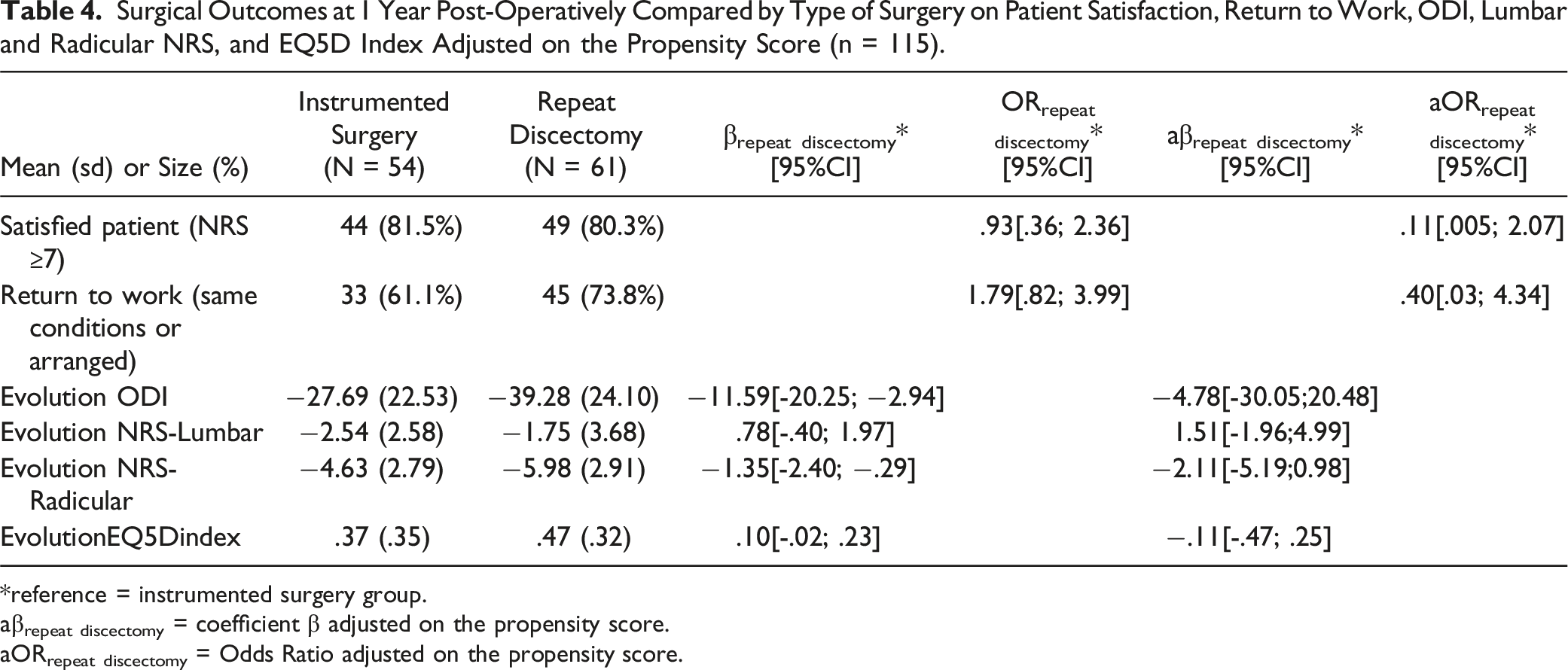
*reference = instrumented surgery group.
aβrepeat discectomy = coefficient β adjusted on the propensity score.
aORrepeat discectomy = Odds Ratio adjusted on the propensity score.
Discussion
Despite the availability of numerous studies on the subject, the optimal management of recurrent lumbar disc herniation remains unclear.7,10,21,22
Numerous variables must be taken into account, including the patient’s medical history, comorbidities and morphological factors, data from previous spinal surgery(s), clinical factors and in particular the balance between axial and radicular symptoms, radiological elements (inflammatory disc disease on MRI, signs of instability, deformity, etc.) and, more subjectively, the surgeon’s preferences, habits and educational elements added to the patient’s will. 2 The ideal algorithm is therefore difficult to define in the context of degenerative spine surgery, where the organization of a high-level RCT remains an insurmountable challenge. 23 As a consequence, the heterogeneity of surgical decisions was highlighted by Mroz et al, who identified inter-professional disagreement rates of up to 69% for common recurrence scenarios. 13
Decision Making: Does the Literature Help Us?
Collective data analysis seems to support repeat surgery as the current standard of care for ReLDH. However, the treatment options range from rediscectomy to procedures associated with anterior or posterior fusions, or even lumbar arthroplasty, all of which were used in our series. However, these different methods have very different clinical effects, morbidity and complication rates, and medico-economic consequences.2,3,8
Most clinical studies have evaluated a particular technique and concluded that it provides satisfactory results for recurrent lumbar disc herniation without comparison, with scarce details on preoperative symptoms and non-standardized postoperative evaluations.2,7,21 There was only 1 randomized trial and the results showed no difference between the 3 proposed techniques, although the need for reoperation was significantly higher in the discectomy alone group. 9
There have been many reviews and meta-analyses on this subject, most of which underline the low level of evidence in the available studies, with the conclusion that it is impossible to promulgate reliable recommendations between the options, which are often divided between rediscectomy and fusion (the arguments for the subgroups, such as types of fusion or minimally invasive techniques, are even less usable).21,22,24 Some selected elements (associated lumbar instability, radiographic degenerative changes and predominantly axial low back pain) can lead to the proposal of fusion, which is also the conclusion of the available guidelines, in particular those of the NASS.12,25 The range of acceptance of these radiologic and clinical decision criteria is sufficiently wide to leave considerable freedom of interpretation to the physician, explaining the variability found in our study. In order to limit the variability, Drazin et al. proposed 8 recommendations for future studies on the treatment of recurrent disc herniation in order to homogenize the reports; we tried to follow these suggestions in our protocol. 21
Variability and Inconclusive Evidence
The variability of attitudes is classically increased when the evidence is low and the gap in the risk-benefit balance is not large, which is typically the case in surgery for recurrent disc herniation, as highlighted in this series.2,4
The shared decision-making process includes the specific demands of the patient, which influence the option chosen, although some authors have shown that this influence is minor on variability. 26
A important factor is the surgeon’s beliefs, habits, and educational background, which expose the decision-making process to numerous biases. 13 This may explain why the guidelines are not necessarily followed, even though 60% of spine surgeons in the US reported following the NASS guidelines for their indications. 27 It is likely that, when faced with inconclusive evidence, surgeons rely on factors related to their perspective and reflect on their culture, training, and practice conditions more than on factors related to the patient’s perspective. 28 Therefore, it is interesting to note that, in our series, factors related to the surgeon’s background were significantly more prevalent when instrumented surgery was performed.
The different economic models and reimbursement systems for medical procedures may also influence the decision; although this phenomenon has been studied in some countries, we lack data in our country. 29 Access to innovative technologies may also alter technical decisions, requiring significant investments by physicians and institutions in appropriate hardware (minimally invasive ancillary instruments and spinal endoscopy equipment) or limiting organizational constraints (e.g., availability of an access surgeon for anterior surgery).30,31
Two Basic Radioclinic Patterns
Although the literature was not necessarily very helpful, most of the surgeons involved in our study made a pragmatic preselection that define the main radio-clinical patterns (Figure 2). Surgical decision-making process in recurrent lumbar disc herniation: the multiple factors influencing the decision from the medical history, the radio-clinical analysis and the elements that modulate the final therapeutic choice.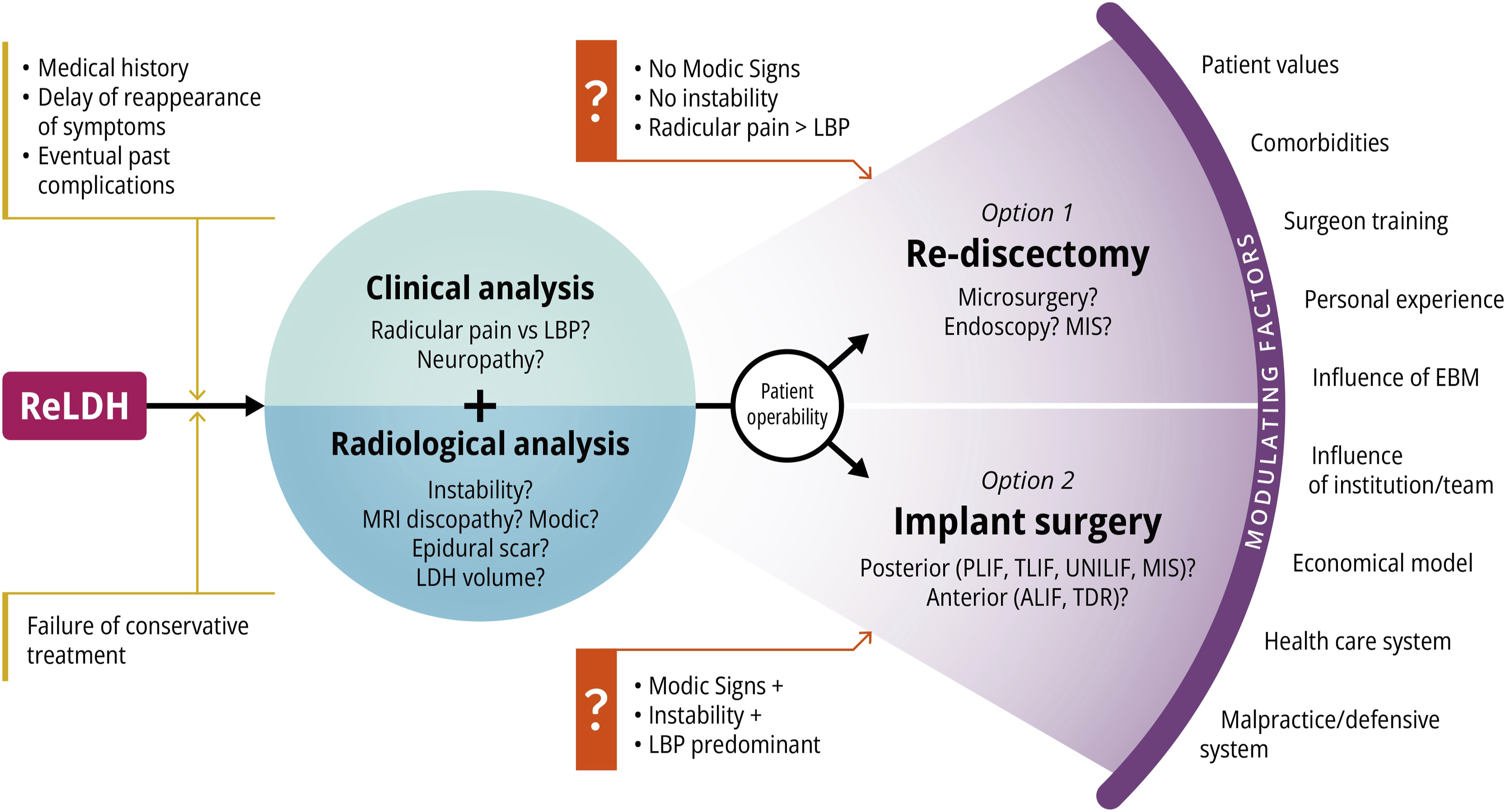
In our study, even if the final decision integrates elements related to the patient’s history or comorbidity and the surgeon’s point of view, 2 typical profiles emerge. On the 1 hand, in a patient with a recurrent herniation correctly defined on MRI, without instability or predominant inflammatory disc disease, and suffering from typical radiculalgia, a simple rediscectomy is most often proposed. 4 On the other hand, a patient with advanced disc disease with possible damage to the vertebral endplates, instability, or even deformity is clinically affected by severe LBP. In this case, the procedure most often involves implants, whether for anterior-posterior fusion or even arthroplasty.22,30 At the periphery of this basic algorithm are mentor/educational influences, surgeon preferences and beliefs, patient wishes, and the level of equipment in the institutions, which lead to the final decision.13,32 The fact that this dichotomy was respected for a large majority of the patients in our series probably explains why the results did not show any significant difference.
In conclusion, there is a clear need for high-level evidence studies that are not currently available in the literature.2,23 Attempts to achieve consistency in results are important, as are the various national registries or those developed by certain scientific societies, which reflect “real life” but require exhaustiveness. 33 The development of artificial intelligence and big data tools is also a solution to be explored, which we see emerging in studies on the spine, and future studies will confirm whether these aspects are fulfilled in this field.34,35
Currently, the decision-making process involves a combination of radiological, anamnestic, and clinical variables modulated by the subjective views of surgeons and patients, which must be adapted as closely as possible to individual cases, which are not necessarily reflected in even a perfectly designed RCT. 23
Bias and Limitations
This retrospective study had statistical weaknesses due to the lack of randomization. Moreover, there were limitations related to the brevity of the follow-up and the freedom given to the surgeons to choose the surgical procedure. However, this study allowed us to understand the current practices in 11 representative centers of French spine surgery, with a homogeneous distribution between academic and private centers and between orthopedic and neurosurgical specialists. It also allowed a better understanding of the surgeons' orientation towards a particular surgical procedure, with the identification of subjective ulterior motives that come into play in a way that is highly significant, given the invasive nature of the surgery.
Conclusion
This large multicenter retrospective study highlights the different factors that differentiate patients undergoing ReLDH from those undergoing IS. It shows that the objective decision-support factors that have already been highlighted in the literature, such as the presence of predominant low back pain and the presence of disc disease on imaging, are considered by the surgeon and are of considerable value when choosing the type of surgery. However, more subjective factors (e.g., surgical school, initial training, patient anxiety) also have a significant impact on the choice of the surgeon-patient decision making. The good clinical outcomes highlighted by the PROMs with no significant differences between the 2 groups of patients operated on with or without instrumentation show that this method of decision making, including objective evidence-based medicine criteria and subjective criteria linked to the experience of the surgeon-patient couple, promotes patient satisfaction.
Footnotes
Acknowledgments
The authors are grateful to Nicolas Lonjon, MD, PhD, Olivier Hamel, MD, Alexis Perez, MD, Nicolas Aurouer, MD, Stéphane Litrico, MD, Henry d’Astorg, MD, Alexandre Delmotte, MD, Solène Prost, MD for there collaboration with the inclusion of patients on behalf of the French Spine Surgery Society (SFCR).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.