
Abstract
Study Design:
Narrative review.
Objectives:
To identify the risk factors and surgical management for recurrent lumbar disc herniation using a systematic review of available evidence.
Methods:
We conducted a review of PubMed, MEDLINE, OVID, and Cochrane Library databases using search terms identifying recurrent lumbar disc herniation and risk factors or surgical management. Abstracts of all identified articles were reviewed. Detailed information from articles with levels I to IV evidence was extracted and synthesized.
Results:
There is intermediate levels III to IV evidence detailing perioperative risk factors and the optimal surgical technique for recurrent lumbar disc herniations.
Conclusions:
Multiple risk factors including smoking, diabetes mellitus, obesity, intraoperative technique, and biomechanical factors may contribute to the development of recurrent disc disease. There is widespread variation regarding optimal surgical management for recurrent herniation, which often include revision discectomies with or without fusion via open and minimally invasive techniques.
Introduction
Recent efforts in orthopedic research have generated insights into the efficacy, safety, and preferred methodology in dealing with recurrent postdiscectomy lumbar disc herniation (LDH). Recurrent herniation of the nucleus pulposus (HNP) and subsequent disc degeneration after a discectomy is a common problem, with reported rates ranging from 2% to 25%. 1 –6 When it occurs, recurrent herniation is a major contributor to debilitating pain, disability, and reoperation following primary surgery, and it is therefore an important factor in determining postoperative success. 7 This type of complication also places a significant burden on the health care system. Estimates regarding the additional costs associated with the diagnosis and management of recurrent LDH have demonstrated significant discrepancies between patients requiring revision surgery, who have a mean cost of $39 386 per patient, and those responding to conservative management, who cost on average $2315 per patient. 8 As such, it is important to identify patients who may be at an increased risk of recurrent herniation, as well as the best practices regarding its management to decrease the cost and morbidity associated with this condition.
Risk Factors
Numerous factors have been associated with an increased rate of herniation following primary discectomy. While biomechanical and anatomic changes during surgery inherently increase risk, there may be modifiable factors that can be addressed preoperatively to decrease the risk of complication. Still appropriate patient selection for primary discectomy remains controversial with conflicting reports in the literature. 9 –11
Smoking
In a recent retrospective analysis of patients undergoing discectomies for LDH, Miwa et al found that current smokers had a postsurgical herniation recurrence rate of 18.5%, which correlated with an odds ratio of 3.472 versus nonsmokers. 10 Their findings are consistent with other studies that have suggested that smoking is a predictive factor for recurrent herniation. 12 –14 The possible mechanism underlying this association could be due to smoking’s detrimental effects on annulus oxygenation and nutrition, nucleus pulposus replication and recovery, or ligamentous healing following the index procedure. 12,15,16 Despite strong evidence about the effects of smoking on disc health, some investigators do not support smoking as a main contributor to recurrent LDH, indicating that additional factors are likely necessary. 17,18
Obesity
Meredith et al examined 75 patients undergoing a 1- or 2-level lumbar microdiscectomy and found that obesity had a strong correlation with recurrent HNP. 17 Individuals in the study with a body mass index (BMI) ≥ 30 were 12 times more likely to sustain recurrent HNP and 30 times more likely to require reoperation compared with nonobese individuals, with odds ratios of 12.46 and 32.81, respectively. However, the study was limited by a relatively small sample size and low number of cases requiring reoperation. Kim et al also demonstrated a similar association between increasing BMI and recurrence following percutaneous endoscopic lumbar discectomy. 19 The authors found that patients with recurrent LDH exhibited higher mean BMIs compared to those without recurrence (24.9 vs 22.9), but neither value fell within parameters of clinical obesity.
Additional studies have failed to show such a correlation between obesity and recurrence. In a recent analysis of patients enrolled in the Spine Patient Outcomes Research Trial, Rihn et al found that following lumbar discectomies, obese and nonobese patients had similar rates of recurrence (7 and 6%, respectively). 20 Quah et al reported lower rates of recurrence in obese (8.6%) versus nonobese (10.0%) patients undergoing single-level microdiscectomy. 21 While their findings failed to demonstrate statistical significance, Moliterno et al conducted a larger retrospective review of patients undergoing single-level tubular lumbar microdiscectomies and found a significantly higher risk of recurrence in nonobese patients with relatively lower BMIs. 22 The clinical significance of these findings is controversial as the difference in average BMI between those with and without recurrence was small (24.9 and 28.3, respectively).
Though the effect of BMI is debated as a cause of recurrent postdiscectomy LDH, the aforementioned evidence suggests that obesity may not be an insignificant variable.
Diabetes Mellitus
In a review of patients undergoing discectomy for LDH, Mobbs et al reported higher rates of LDH recurrence and reoperation in diabetics (28%) compared with controls (3.5%). 23 Analysis of proteoglycans in the discs of patients with diabetes demonstrated decreased sulfate incorporation into the glycosaminoglycan molecules and lower glycosylation rates, which was consistent with a Robinson et al study showing fewer proteoglycans in the intervertebral discs of diabetics compared to nondiabetics. 14 These differences could contribute to increased susceptibility for recurrent herniation among diabetics because sulfation and proteoglycans are known to strengthen the disc collagen matrix. However, clinical studies have failed to support the histologic findings, and a definitive relationship between diabetes and rates of recurrent LDH has not been described. 11,24
Biomechanical Factors
Changes in vertebral load properties and biomechanics that result from degenerative disease and subsequent surgical intervention may contribute to accelerated spondylotic changes and reherniation. This was demonstrated by Kim et al who used preoperative imaging in the evaluation of potential biomechanical factors that contribute to recurrent herniation. 24 The authors found that patients with sagittal motion >10° had a recurrence rate of 26.5% compared with those with <10° who had a rate of 4.1%. Using magnetic resonance imaging (MRI), they also quantified preoperative disc height index (DHI = disc/vertebral body height) to assess for disc degeneration, and they found that those with recurrent LDH had significantly lower preoperative DHI indicative of worse disc degeneration versus those without recurrence (0.37 vs 0.29, respectively). The authors attributed this to the effects of disc degeneration on annular collagen degradation. Though the most severe instances of disc degeneration were not associated with increased rates of recurrent LDH, it has been suggested that severe disc height loss increases intervertebral stability by decreasing index-level motion. This relationship between preoperative disc height and risk of reherniation has motivated some surgeons to defer surgery in patients with herniations and normal disc height until all conservative options have been exhausted.
Factors Related to the Primary Discectomy
Intraoperative debulking may also contribute to recurrent LDH. 25 –27 McGirt et al found that larger annular defects and smaller percentage of disc removed during primary surgery, rather than absolute volume as reported in previous studies, were associated with an increased risk of reherniation while more aggressive removal contributed to accelerated disc height loss. 27 In a systematic review, McGirt et al found that while limited discectomies result in shorter operative times, a quicker return of function, and similar functional status at 6 months postoperatively, limited discectomies and were again associated with higher rates of recurrent herniation versus aggressive discectomy (8.7% vs 3.3%). 28 The question remains how to balance the desire for maintaining disc height with minimizing the risk for reherniation.
Management of Recurrent Herniation
The management of postoperative recurrent LDH remains controversial. A consensus is difficult to achieve because of the multitude of variables discussed above with reported rates of disagreement among surgeons ranging from 22% to 69%. 29 The current literature regarding surgical management of recurrent herniation consists primarily of case series or reviews with a low level of evidence. However, collective data analysis appears to support repeat surgery as the current standard for the treatment of recurrent LDH. Surgical options include repeat discectomy either via a conventional or minimally invasive technique, with or without instrumented spinal fusion. When determining the optimal approach, factors including surgeon preference, presenting symptoms, presence of axial low back pain, radiographic evidence of instability or deformity, and number of prior herniations must be considered.
Revision Discectomy
Studies focusing on revision surgery for recurrent disc herniation have demonstrated variable outcomes. While many recent reports have shown clinical results comparable to primary discectomies, early studies demonstrated no statistical difference and even worse outcomes following revision discectomy (Table 1). 4,6,30 –32 Cinotti et al conducted an early prospective analysis that compared 26 revision microdiscectomies for ipsilateral recurrent disc herniations with a control group consisting of primary discectomies. 30 Using a nonvalidated 100-point clinical outcome assessment, the authors found that patient-reported outcomes following revision discectomies were similar to those following primary discectomies (85% vs 88%, respectively). However, the study population included associated pathologies such as epidural fibrosis and foraminal stenosis that may have confounded the results. Suk et al controlled for these mixed populations by defining recurrent LDH as MRI confirmed same-level disc herniations after a pain-free interval greater than 6 months. 31 Using these criteria they identified 28 patients treated with revision open discectomy following an index open discectomy. There were no significant differences in pain-free interval, length of stay, or clinical improvement assessed by visual analogue scale (VAS) scores between the 2 procedures, although the authors did note an increase in length of surgery for revisions.
Revision Versus Primary Discectomies.
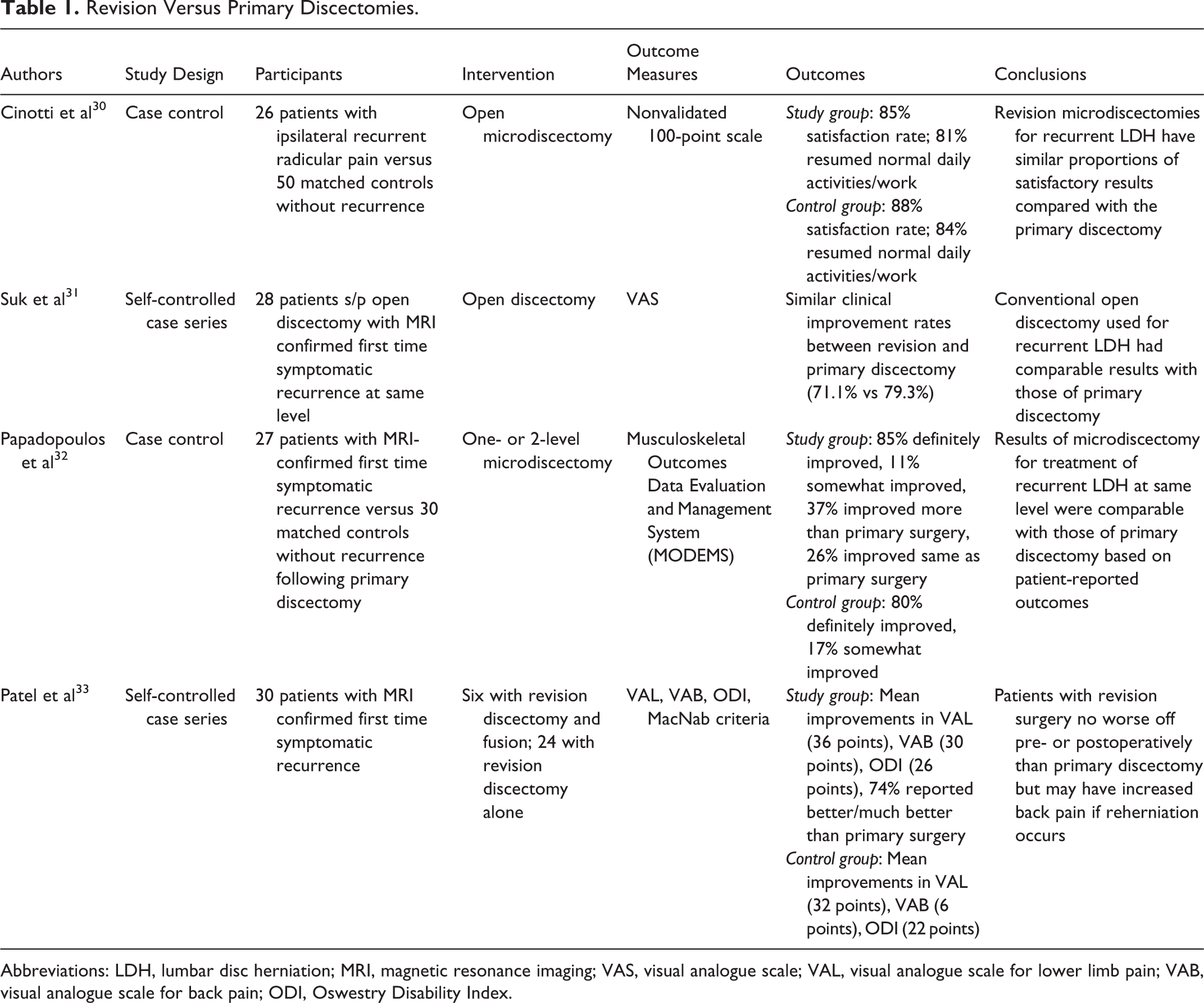
Abbreviations: LDH, lumbar disc herniation; MRI, magnetic resonance imaging; VAS, visual analogue scale; VAL, visual analogue scale for lower limb pain; VAB, visual analogue scale for back pain; ODI, Oswestry Disability Index.
More recently, Papadopoulos et al retrospectively reviewed the clinical outcomes of revision microdiscectomy for MRI-confirmed same-level recurrent disc herniation. 32 Compared with a matched control group, the authors found that those undergoing revision surgery had similar postoperative satisfaction (80% vs 85% reporting definite improvement, respectively) despite significant differences in residual leg numbness and frequency of back pain. Patel et al also reported comparable improvements following primary discectomy and revision surgery in their analysis of 30 patients who had undergone both procedures for single-level LDH. 33 The authors found that all patients reported significant improvements in outcome scores for both primary and revision surgeries and that there was no significant difference between the 2 procedures. As such, many authors advocate that repeat discectomies can be used as an effective treatment for recurrent disc herniation with radicular symptoms unless patients have indication for instrumented fusion, which will be discussed below.
Instrumented Fusion
While many surgeons advocate for repeat discectomy alone, others support the use of varying methods of fusion with or without minimally invasive techniques (Table 2). Current recommendations suggest the use of repeat discectomy for patients with recurrent LDH with consideration for fusion in patients with significant deformity, instability, or associated axial low back pain. 34 The addition of instrumented fusion may help provide added stability that counteracts segmental motion at the affected level. 35 A recent review by Dower et al found similar rates of satisfactory outcomes in patients undergoing discectomy alone versus discectomy with fusion (79.5% vs 77.8%, respectively). However, significant improvements were noted in back pain scores in patients undergoing fusion compared with isolated discectomy (60.1% vs 47.2%, respectively), highlighting the potential benefit of fusion in patients with preoperative back pain. 36
Segmental Fusion Techniques.
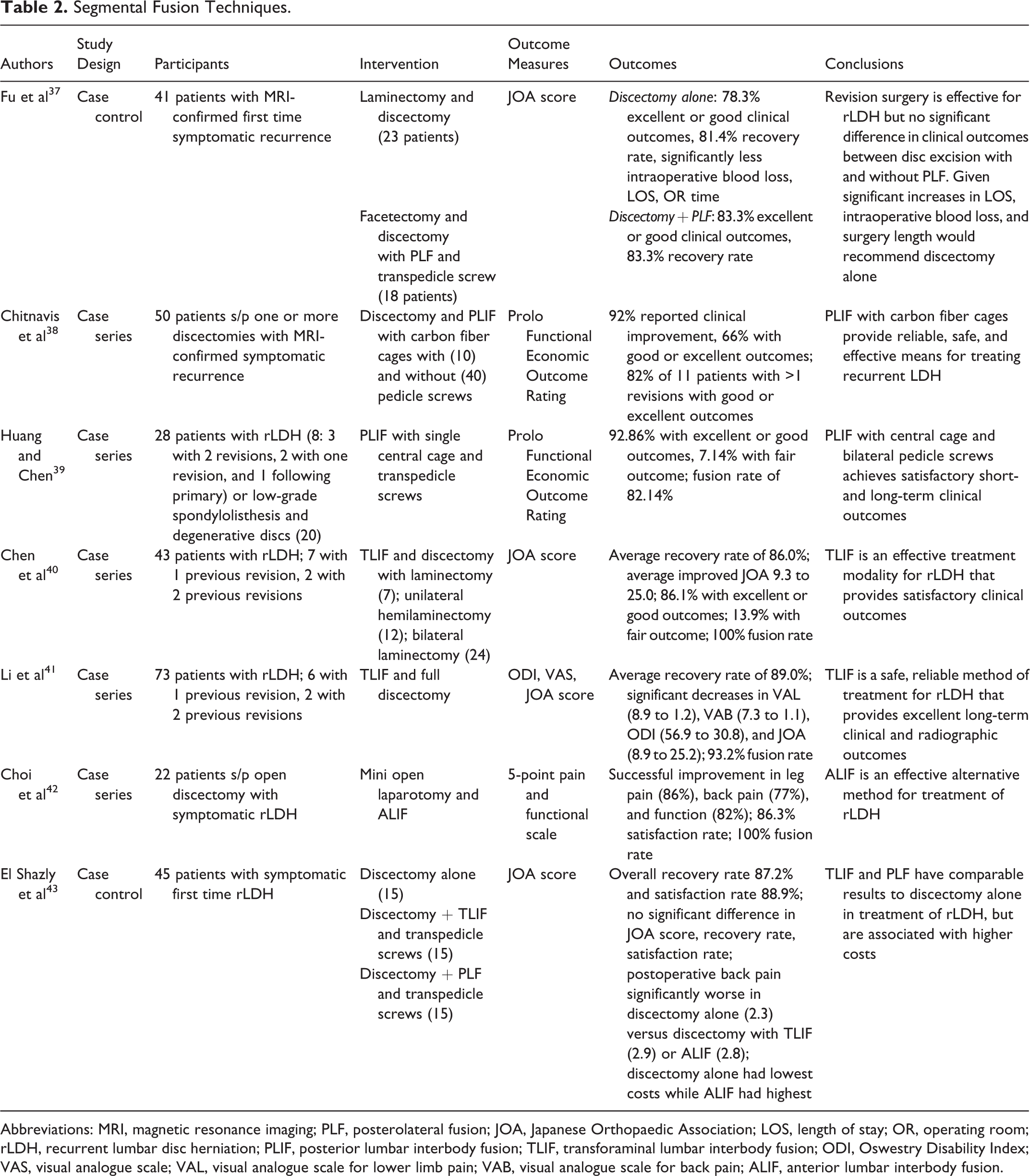
Abbreviations: MRI, magnetic resonance imaging; PLF, posterolateral fusion; JOA, Japanese Orthopaedic Association; LOS, length of stay; OR, operating room; rLDH, recurrent lumbar disc herniation; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; ODI, Oswestry Disability Index; VAS, visual analogue scale; VAL, visual analogue scale for lower limb pain; VAB, visual analogue scale for back pain; ALIF, anterior lumbar interbody fusion.
The primary means of achieving fusion in cases of recurrent LDH consists of posterolateral fusion (PLF). In their retrospective review, Fu et al compared the results of PLF with disc excision to those undergoing disc excision alone for patients with isolated recurrent LDH. 37 Of the 18 patients treated with concurrent disc excision and PLF, 83.3% had an excellent or good clinical outcome versus 78.3% of the 23 patients undergoing revision discectomy alone. The authors found no significant difference between the 2 groups in intraoperative blood loss, surgery length, and length of stay, suggesting comparable results between discectomy with and without fusion in patients without associated pathology or instability.
Multiple studies have focused on the use of alternative methods of interbody fusion for recurrent LDH with varying results. Chitnavis et al studied the use of posterior lumbar interbody fusion (PLIF) with carbon cages in their prospective analysis of 50 patients treated for recurrent LDH with symptomatic back pain or signs of instability. 38 The authors noted high satisfaction rates with 92% reporting significant symptom relief after a follow-up ranging from 6 months to 5 years. These findings were similar to those reported earlier by Huang and Chen, who reviewed 28 patients undergoing PLIF with cages and pedicle screws, 8 of whom were indicated for recurrent LDH and 20 for low-grade spondylolisthesis. 39
Chen and colleagues reported on the outcomes of transforaminal lumbar interbody fusion (TLIF) for the treatment of recurrent LDH. 40 Added benefits of this approach include dissection through virginal tissue, minimal retraction of the dural sac, and low risk of postoperative radiculitis. The authors found significant improvements in leg pain with improvements in Japanese Orthopaedic Association (JOA) score from 9.3 preoperatively to 25.0 at final follow-up (mean of 45 months) and satisfaction rates of 86%. The clinical outcomes were also comparable to other methods of interbody fusion with 23 (53.5%) reporting excellent, 14 (32.6%) good, and 6 (13.9%) fair. More recently, Li et al reviewed 63 patients undergoing revision surgery with TLIF following conventional discectomy with symptomatic recurrent LDH. 41 Compared to preoperative evaluation, postoperative clinical outcomes including JOA (8.9 to 25.2), Oswestry Disability Index (56.9 to 20.4), and VAS for leg and back pain significantly improved at a mean follow-up of 4.1 years while the overall fusion rate was 93.2%, suggesting TLIF as an effective treatment in the management of recurrent LDH.
Choi et al reviewed the use of anterior lumbar interbody fusion (ALIF) for recurrent disc herniation in 22 patients and found a satisfaction rate of 86.3% with significant improvements in leg pain, back pain, and functional status following revision surgery. 42 However, because ALIF is performed from the opposite direction of the disc herniation when compared with posterior approaches, some surgeons argue that thorough removal of the herniated portion of the disc may not be possible in certain cases.
While these studies have demonstrated that multiple methods may be effective in treating recurrent LDH, there is limited evidence comparing different surgical techniques. In one large prospective study, El Shazly et al evaluated 45 patients with recurrent LDH randomly treated with 1 of 3 methods of fixation: discectomy alone, discectomy with TLIF, or discectomy with PLF. 43 While the overall satisfaction rate was 88.9%, the authors found no significant difference between the 3 groups in postoperative JOA score (26.1, 27.9, and 27.9, respectively), recovery rate (82.8 vs 90.1 vs 88.8), and satisfaction rate (86.7 vs 93.3 vs 86.7). They found significantly higher postoperative low back pain scores and need for revision surgery with the discectomy alone group, but also noted a decrease in surgery length, intraoperative blood loss, and total cost of procedure compared with those treated with discectomy and fusion. Therefore, the type of fusion methods selected to treat recurrent LDH seems to rely on a case by case basis as well as surgeon’s preferences.
Currently, there is no clear consensus regarding the number of repeat herniations required prior to consideration for instrumented fusion at the affected level. In the absence of low back pain or radiographic instability, the most common surgical intervention for first time recurrence is repeat discectomy. However, with each subsequent surgery the chance of introducing or worsening segmental lumbar instability increases as repeat exposure often requires more aggressive facetectomies and dissection for visualization of the neural foraemn. 35 As such, the threshold to incorporate instrumented fusion decreases with the number of recurrent herniations. This was demonstrated by Mroz et al using an electronic survey sent to 2560 orthopedic and neurologic surgeons throughout the United States. 29 For first time recurrence, the majority of surgeons replied that they would treat with revision microdiscectomy alone regardless of region, specialty, fellowship training, or practice type. For second time recurrence previously treated with microdiscectomy, there was significant discordance in preferred management with a 69% chance of disagreement between surgeons. Specifically, those who performed 201 to 500 cases per year had 3.47 greater odds of choosing to treat via revision microdiscectomy with PLIF/TLIF rather than revision microdiscectomy alone compared with those surgeons performing only 0 to 100 cases per year. 29
Minimally Invasive Techniques
While the use of microdiscectomies for recurrent LDH has become a well-accepted and widely used modality, the emergence of minimally invasive techniques for primary disc herniations has sparked interest in their applicability for revision discectomies. The use of microendoscopic techniques for recurrent LDH remains controversial with varying reports regarding clinical success and complication rates, as well as steep learning curves and the possibility of poor visualization of nonvirginal tissue (Table 3). 44 Isaacs et al reported on their early experience with microendoscopic discectomy (MED) in 10 patients treated for recurrent herniation. 45 The authors found that 100% of patients reported improvement in sciatica with 90% having good or excellent outcomes at a mean of 13.1-month follow-up. Compared with a series of 25 patients treated with single-level MED for primary discectomies, there were no significant differences in operating time, blood loss, length of stay, or operative complications with one durotomy and one recurrent herniation following MED for recurrent LDH. In another retrospective series, Ahn et al studied 43 patients treated with MED for recurrent disc herniation following open discectomy and found that 81.4% had excellent or good outcomes with significant decreases in VAS score. 46 Smith et al reported similar outcomes in their review of 16 patients treated with MED for recurrent herniation. 47 The authors found significant improvements in all outcome measures including VAS (8.2 to 2.2), ODI (28.3 to 42.4), and SF-36 (38.2 to 48.3), with 80% of patients showing good or excellent outcomes with the rest exhibiting a fair outcome at mean follow-up of 14.7 months. While these studies demonstrate favorable clinical outcomes, the small sample sizes and retrospective analysis make direct comparisons between MED and conventional open techniques difficult.
Microendoscopic Techniques.
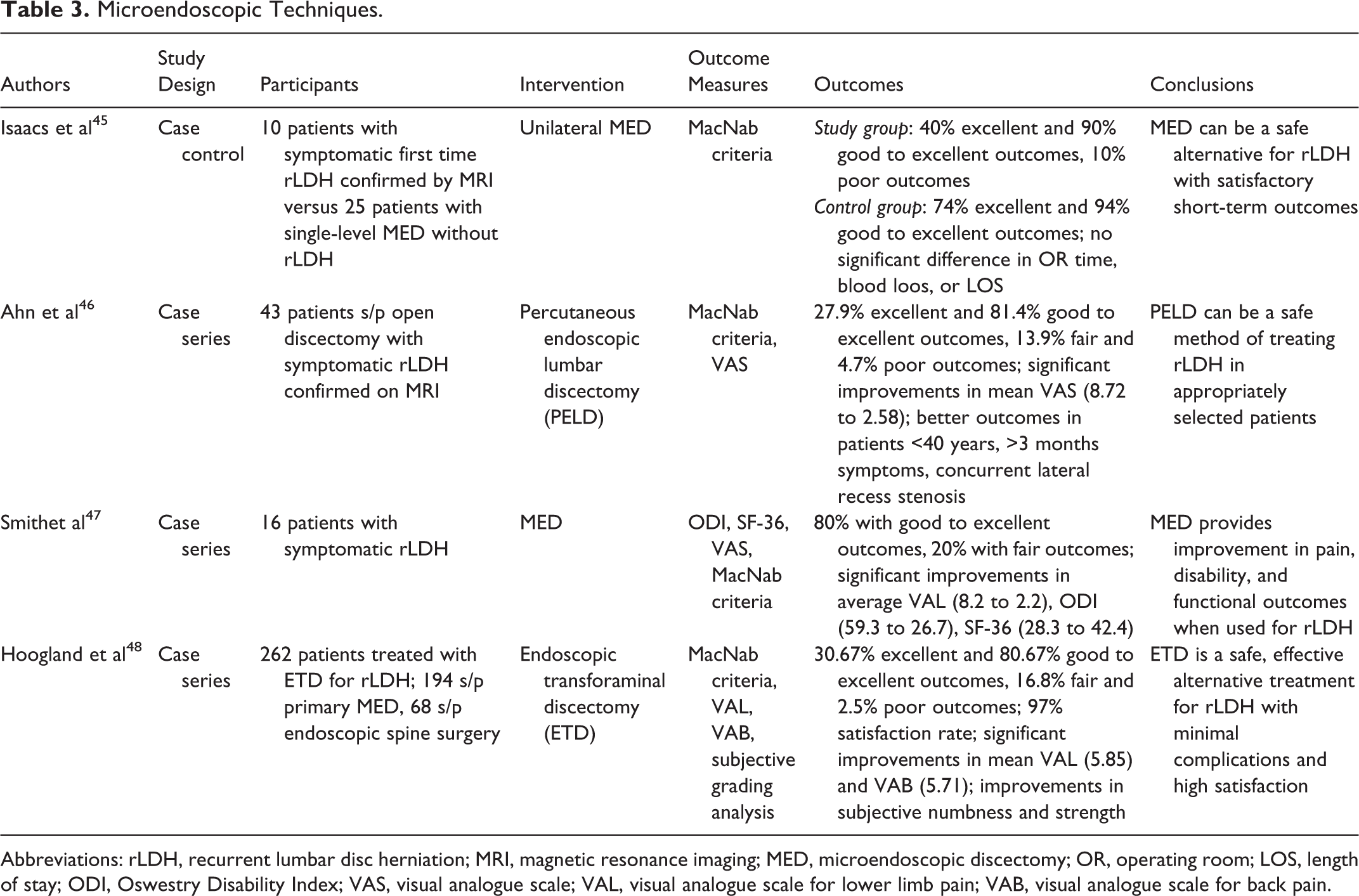
Abbreviations: rLDH, recurrent lumbar disc herniation; MRI, magnetic resonance imaging; MED, microendoscopic discectomy; OR, operating room; LOS, length of stay; ODI, Oswestry Disability Index; VAS, visual analogue scale; VAL, visual analogue scale for lower limb pain; VAB, visual analogue scale for back pain.
Hoogland et al carried out a larger review of 262 cases of endoscopic discectomies for recurrent herniation. 48 Similar to previous reports, the authors found an 85.1% good or excellent success rate at 2-year follow-up, with 9.66% and 4.62% showing fair and unsatisfactory results, respectively. While the overall complication rate was 3.8% (10/262), postoperative nerve root irritation did not result in permanent damage and the 4.62% (11/262) recurrence rate after 3 months was similar to that of previous reports. Taken together, these studies demonstrate that a minimally invasive endoscopic technique is feasible for revision discectomy and can provide an effective alternative to conventional approaches. However, there is limited high-quality evidence supporting the use of MED over microdiscectomies with surgeon preference and comfort often dictating the operative technique used for recurrent LDH.
Summary
Recurrent LDH is a common complication following primary discectomy. Numerous risk factors have been reported including modifiable patient-related variables and biomechanical or surgical factors. While there has been an emphasis on identifying the optimal surgical candidate and technique, there is conflicting data regarding which factors truly increase the risk of recurrent herniation. For those with recurrent LDH who have failed nonoperative management, repeat discectomy appears to be a safe and effective surgical option. However, the next challenge is determining the appropriate surgical intervention (eg, conventional or endoscopic and with or without instrumented fusion). Important considerations include presenting symptoms (radicular pain vs axial low back pain), radiographic instability, sagittal or coronal deformity, history of previous reherniations or surgery, and surgeon comfort. Additional comparative clinical studies are necessary to better understand the optimal surgical treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.