
Abstract
Study Design
National population-based cohort study.
Objective
The overall complication rate for patients with athetoid cerebral palsy (CP) undergoing cervical surgery is significantly higher than that of patients without CP. The study was conducted to compare the reoperation and complication rates of anterior fusion, posterior fusion, combined fusion, and laminoplasty for degenerative cervical myelopathy/radiculopathy in patients with athetoid cerebral palsy.
Methods
The Korean Health Insurance Review and Assessment Service national database was used for analysis. Data from patients diagnosed with athetoid CP who underwent cervical spine operations for degenerative causes between 2002 and 2020 were reviewed. Patients were categorized into four groups for comparison: anterior fusion, posterior fusion, combined fusion, and laminoplasty.
Results
A total of 672 patients were included in the study. The overall revision rate was 21.0% (141/672). The revision rate was highest in the anterior fusion group (42.7%). The revision rates of combined fusion (11.1%; hazard ratio [HR], .335; P = .002), posterior fusion (13.8%; HR, .533; P = .030) were significantly lower than that of anterior fusion. Revision rate of laminoplasty (13.1%; HR, .541; P = .240) was also lower than anterior fusion although the result did not demonstrate statistical significance.
Conclusion
Anterior fusion presented the highest reoperation risk after cervical spine surgery reaching 42.7% in patients with athetoid CP. Therefore, anterior-only fusion in patients with athetoid CP should be avoided or reserved for strictly selected patients. Combined fusion, with the lowest revision risk at 11.1%, could be safely applied to patients with athetoid CP.
Keywords
Introduction
Athetoid cerebral palsy (CP) causes continuous involuntary neck movements of the cervical spine, leading to early degeneration, cervical myelopathy, radiculopathy, and deformity.1-3 Excessive spondylotic changes and severe dynamic instability of the spine are frequently observed in patients with athetoid CP, often due to the strain of cervical muscle imbalance and sustained involuntary movements.4-7 While initial conservative management can be provided, surgical treatment often becomes necessary for the decompression of neural elements, stabilization, and correction of deformity.8,9
However, the postoperative course in patients with athetoid CP is often complicated.2,10 Continuous neck muscle movement causes loosening of instruments, non-union, instability, and progressive kyphosis, resulting in clinical aggravation.6,11 The overall complication rate for patients with athetoid CP undergoing cervical surgery is known to be significantly higher than that of patients without CP. 2 Previous studies have suggested that strong fixation using pedicle screws or combined anterior-posterior fusion is warranted to decrease long-term complications and reduce complication rates.12,13 However, these surgical options are technically demanding and are associated with greater surgical morbidity. Laminoplasty, without fusion, has also been suggested as a viable, relatively non-invasive surgical option for selected patients with athetoid CP without significant deformity and instability.6,14 Nevertheless, the long-term prognosis of laminoplasty in patients with athetoid CP may be complicated by progressive deformity and the occurrence of instability. 13
Studies demonstrating the prognosis of patients with athetoid CP undergoing cervical spine surgery are limited in sample size due to the low incidence of athetoid CP. It remains unclear which surgical strategy is superior in minimizing complications and the possibility of revision operations.1,2,6,11,15 Utilizing a national cohort database, the postoperative prognosis of patients with athetoid CP could be examined with a much larger sample size. 16 If a certain surgical approach is associated with a decreased rate of reoperation or surgical complications, it would be considered a primary treatment choice when selecting a surgical strategy for patients with athetoid CP. Therefore, this study was conducted to (1) compare the reoperation and complication rates of anterior fusion, posterior fusion, combined fusion, and laminoplasty performed for degenerative cervical myelopathy/radiculopathy in patients with athetoid CP and (2) identify risk factors for reoperation rates in this patient group.
Materials and Methods
Study Design and Population
This study was approved by the institutional review board of the relevant institution (DUIH 2022-06-005) and conducted as a national, prospectively collected population database analysis. Informed consent was not required since the study was conducted using national database. The Korean Health Insurance Review and Assessment Service, a mandatory, universal, single health insurance service managed by the government, provided the database. This dataset contains medical information for all patients nationwide, categorized by diagnosis and procedural codes and standardized according to the International Classification of Disease, 10th edition.
Inclusion Criteria
Patients were included if they (1) were diagnosed with athetoid CP (G803) and (2) underwent cervical spine operations for degenerative cervical myelopathy (G951 - 959, G992, M500, M510, M4710-4819, M4800-M4803, M4809, M9951, M9971) or cervical radiculopathy (M501, M5412, M4722, M4720, M4723, M4729, M502, M503, M508, M519, M5410, M5411, M5413, M5419) between January 2006 and December 2020. Since the study was conducted in December 2023, minimum of 3 years of follow-up data would be obtained for all patients. Patients who (1) underwent operations for cervical spine infection (M465), fracture (S129, S1290, S127, S122, S120, S121, T08), tumor (C412, M495, C795, C900), tuberculosis (A1800); (2) were diagnosed with Arnold-Chiari malformation (Q070), ankylosing spondylitis (M45, M081), and Klippel–Feil syndrome (Q761); were <18 years at the time of operation; and (3) had cervical spine operations between 2002 and 2005 (wash-out period) were excluded from the study (Figure 1). Patient selection process.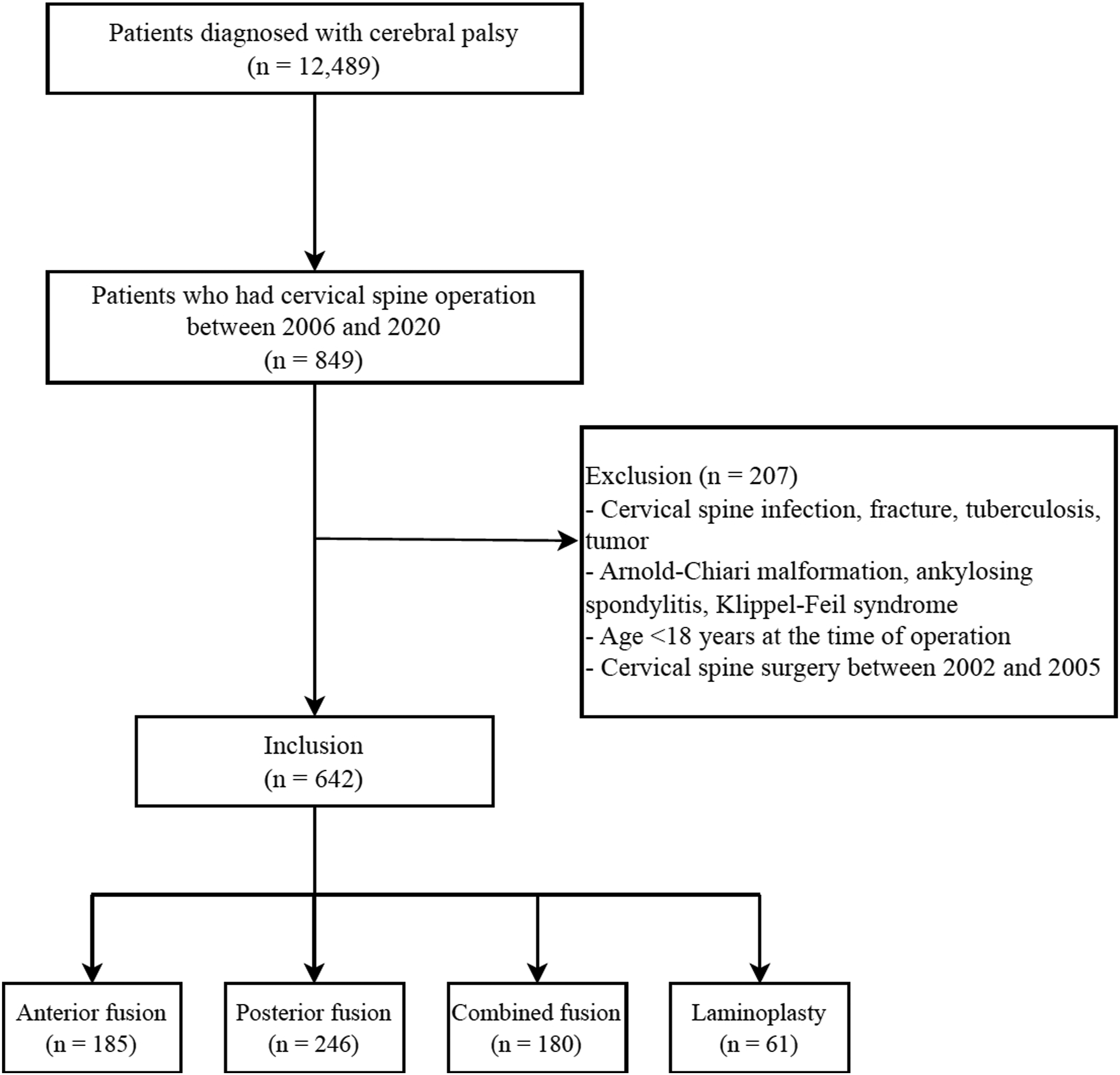
Classification of Surgical Procedures
Patients were classified according to the type of initial operation, including anterior discectomy (N1491), anterior fusion (N2463), and corpectomy (N0451) in the anterior fusion group; laminectomy (N1497) and posterior fusion (N2469) in the posterior fusion group; laminoplasty (N2401, N2492) in the laminoplasty group; and both anterior fusion (N2463, N0451) and posterior fusion (N2469) within 2 weeks in the combined fusion group.
Surgical Indications
As this was a national database analysis involving multiple centers, surgical indications were not uniformly controlled. However, all hospitals in Korea followed the Korean National Health Insurance Corporation requirements for reimbursement. Operations for cervical myelopathy required objectively demonstrable neurologic deficit or signs of cervical myelopathy. Surgical treatment of cervical radiculopathy required intractable pain despite nonsurgical treatment for at least 6 weeks or associated progressive neurologic deficit. Such indications were considered for patients in this cohort, and therefore, surgical indications were not considerably different for most patients. 16
Variables
Patient demographic factors including age, body mass index (BMI), sex, and underlying diseases based on the diagnosis codes were recorded. Additionally, clinical diagnoses of cervical degenerative diseases, including cervical myelopathy (G951 - 959, G992, M500, M510, M4710-4819, M4800-M4803, M4809, M9951, M9971), and cervical radiculopathy (M501, M5412, M4722, M4720, M4723, M4729, M502, M503, M508, M519, M5410, M5411, M5413, M5419) were identified. Types of reoperations after the initial operation, along with the interval between the initial and second operations were also documented. Only the second operation was considered as the event of interest; third and subsequent reoperations were not included in the analysis. Immediate postoperative complications, including infection (T814), hematoma (T810, T140, I610, I620), and mechanical failure (T856, T843, T842, T844, T856), along with mortality within 2 years of the operation, were recorded.
Statistical Analyses
Comparisons were made between the anterior fusion, posterior fusion, combined fusion, and laminoplasty groups. Categorical variables, including underlying disease, diagnosis, and surgical complications, were analyzed using the chi-square test. Continuous variables were analyzed using analysis of variance. Time-to-event (reoperation) survival analysis was performed, defining reoperations as the presence of any cervical spine operation code 2 weeks after the index procedure code, considering a 2-week interval as indicative of a staged operation. Cox regression analysis was performed to identify risk factors associated with reoperation after the initial operation. Multivariate Cox regression analysis was performed with factors that were significant in the univariate analysis to adjust for confounding factors. Data management and analysis were performed using SAS software (SAS Institute, Inc., Cary, NC, USA). A P-value of <.05 was considered significant.
Results
Study Population and Baseline Characteristics
Patient Baseline Characteristics.
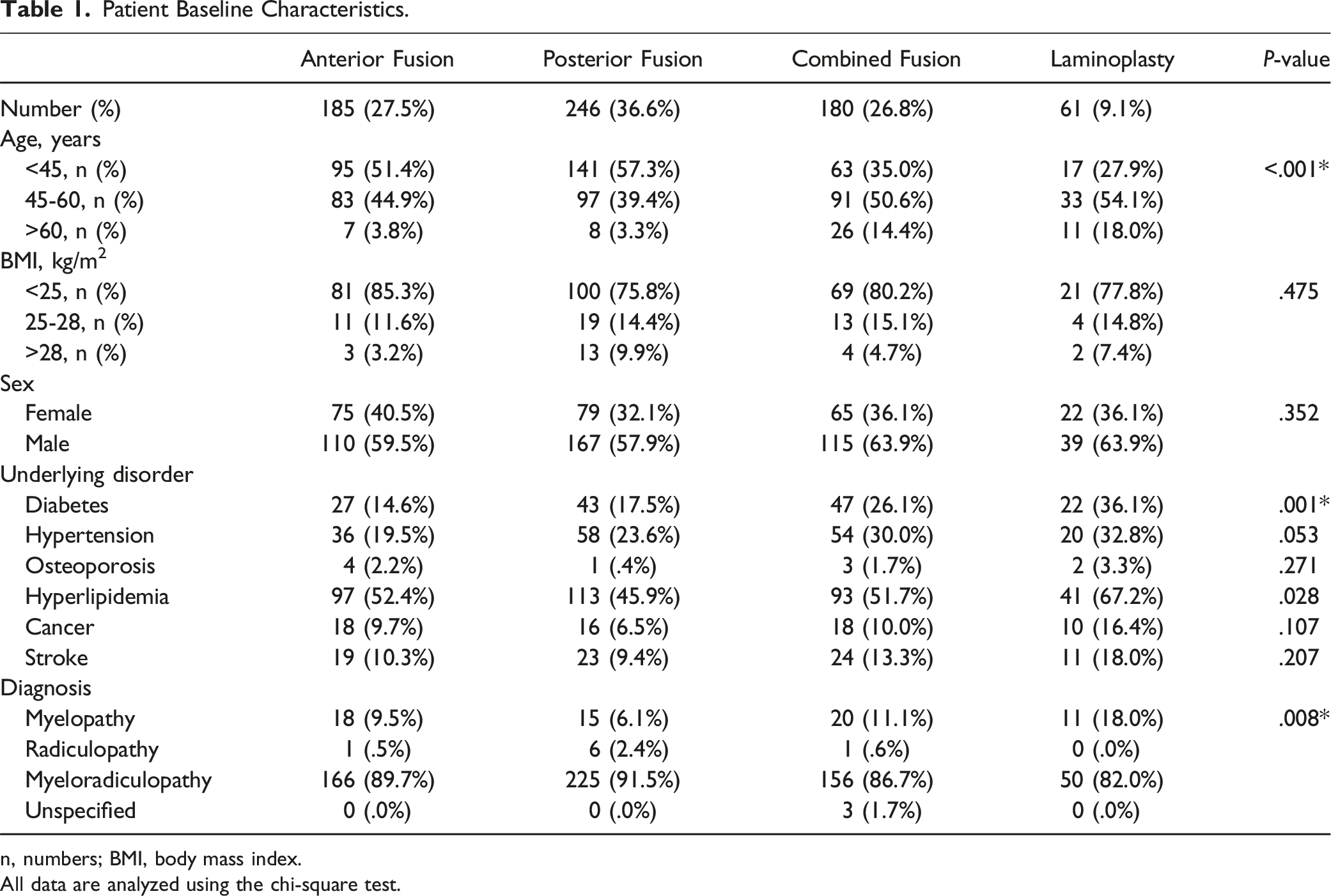
n, numbers; BMI, body mass index.
All data are analyzed using the chi-square test.
Reoperation After the Initial Operation
Incidence by Postoperative Period and Cumulative Incidence of Revision Operation.
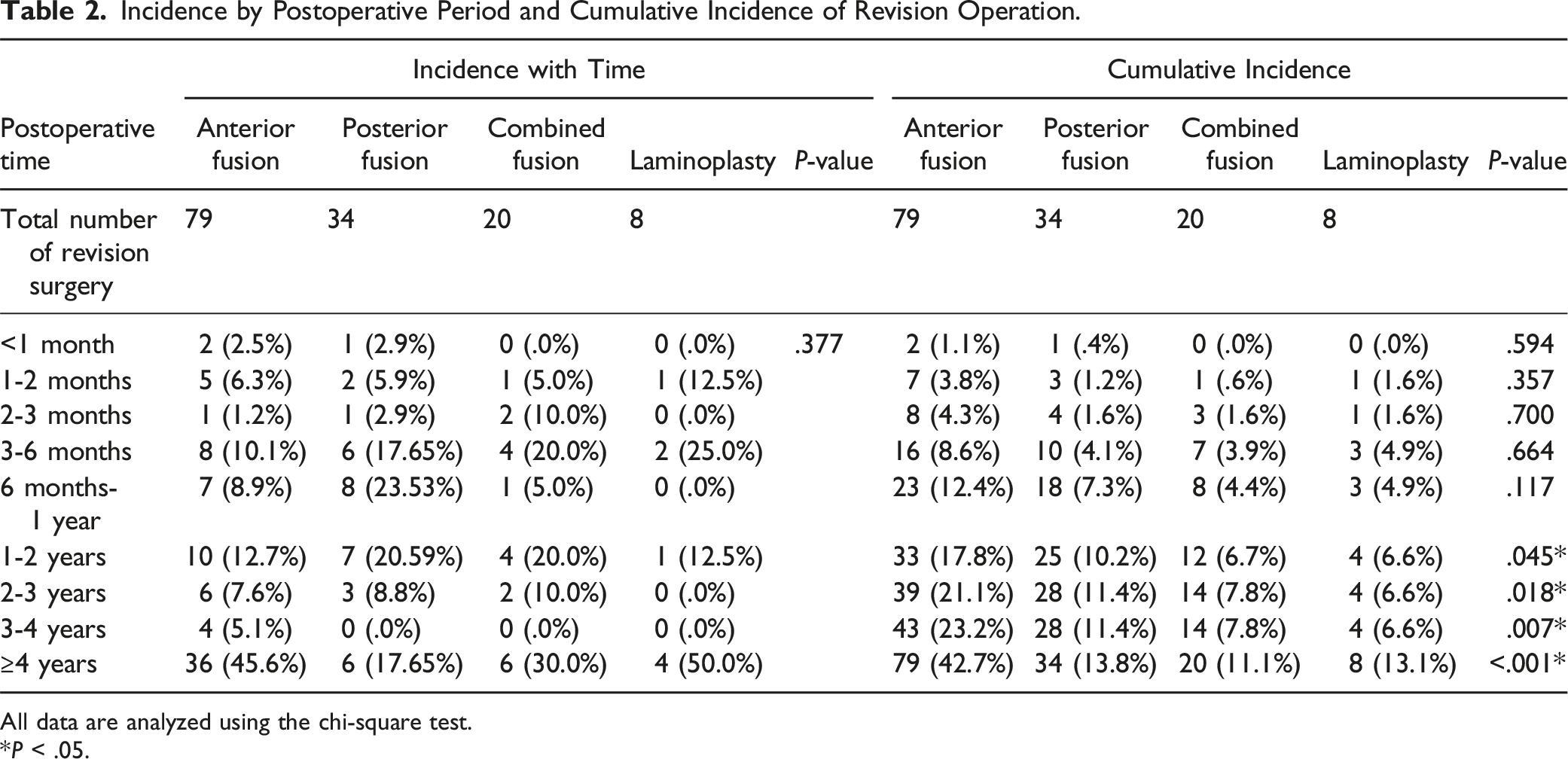
All data are analyzed using the chi-square test.
*P < .05.
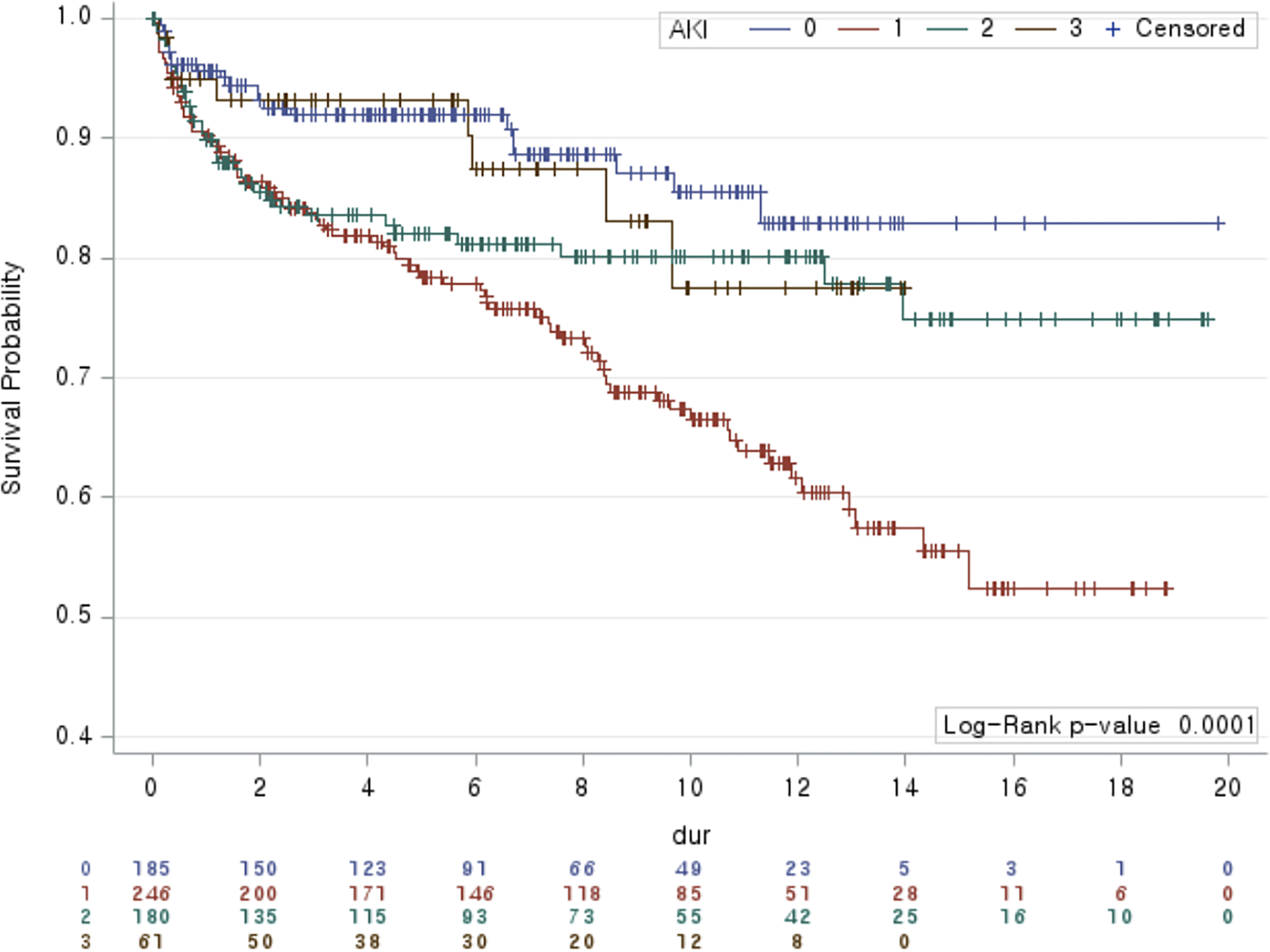
Kaplan–Meier survival curve demonstrating reoperation free survival in each group 0 (blue line): combined fusion, 1 (red line): anterior fusion, 2 (green line): posterior fusion; 3 (brown line): laminoplasty.
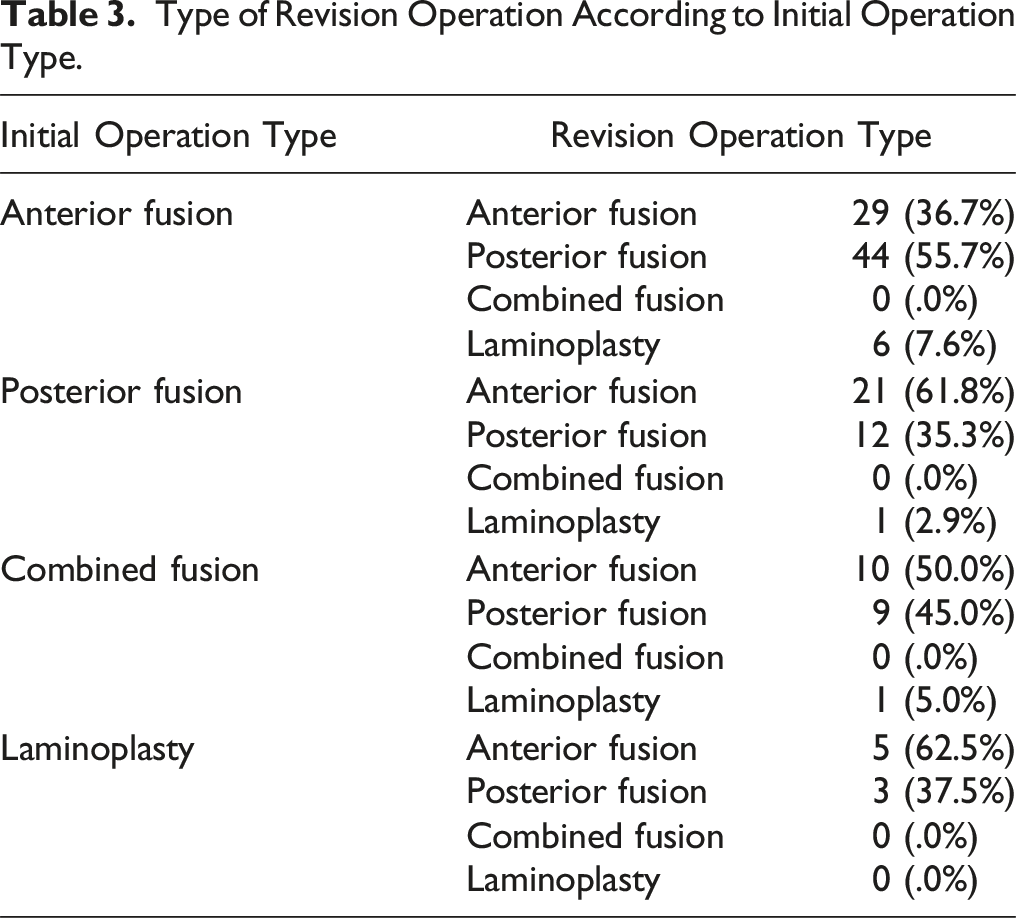
Type of Revision Operation According to Initial Operation Type.
Surgical Complications
Surgical Complications After Initial Operation According to Initial Surgery Type.
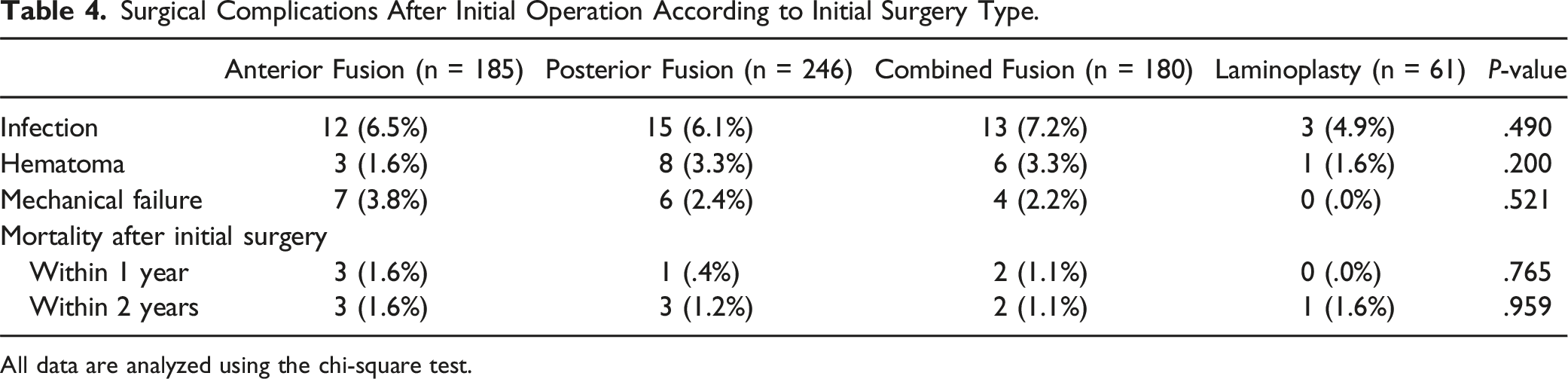
All data are analyzed using the chi-square test.
Risk Factors Associated with Revision Operation
Results of Cox Regression Analysis Demonstrating Factors Associated With Revision Surgery.
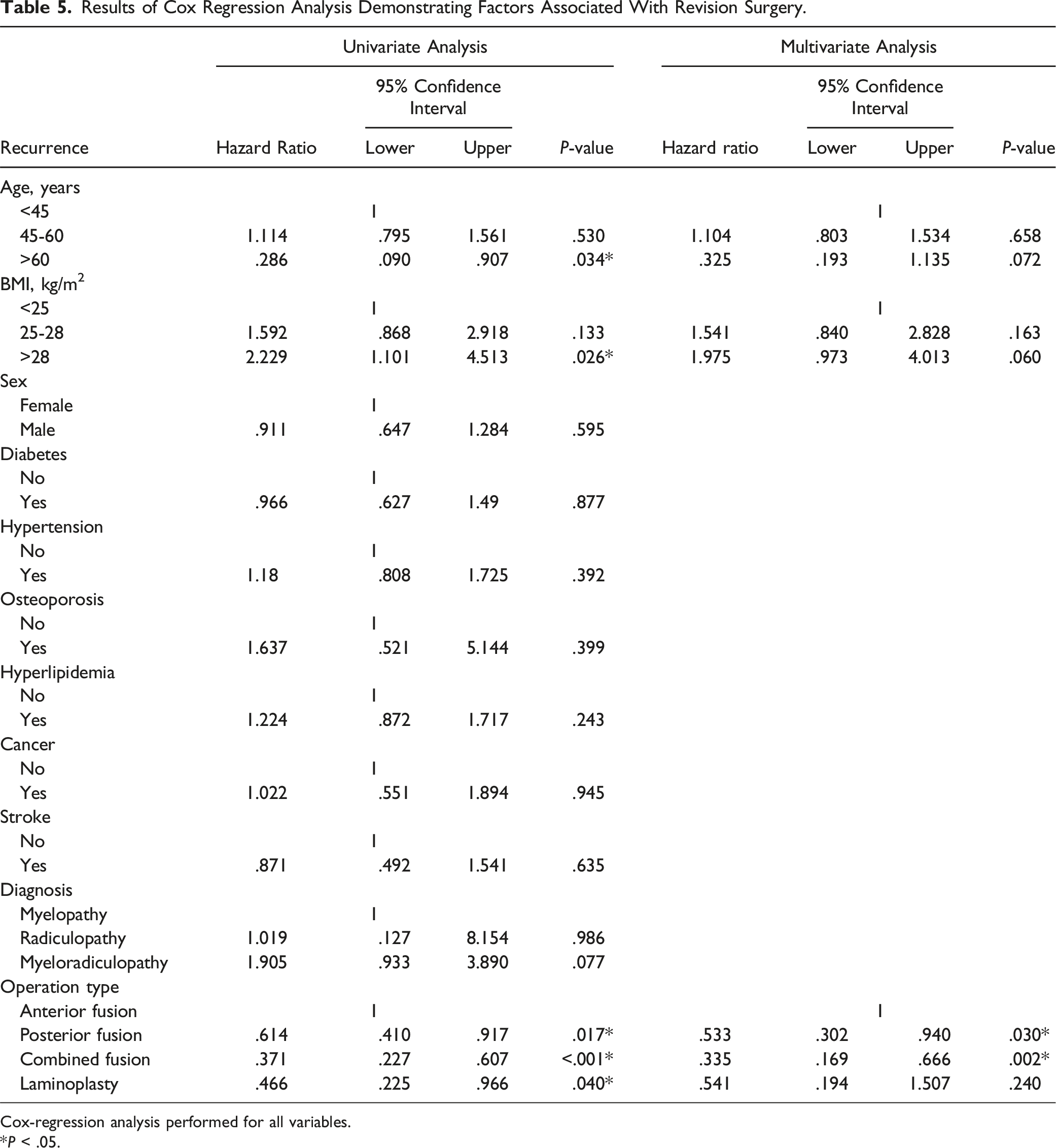
Cox-regression analysis performed for all variables.
*P < .05.
Furthermore, anterior fusion presented the highest risk of revision, whereas combined fusion exhibited the lowest risk in univariate analysis. Compared to anterior surgery, posterior fusion (HR, .614; 95% CI, .410-.917; P = .017), laminoplasty (HR, .466; 95% CI, .225-.966; P = .040), and combined fusion (HR, .371; 95% CI, .227-.607; P < .001) exhibited sequentially lower HRs of revision operation, which were statistically significant. In multivariate analysis, posterior fusion (HR, .533; 95% CI, .302-.940; P = .030), and combined fusion (HR, .335; 95% CI, .169-.666; P = .002) demonstrated significantly lower risk compared to anterior fusion, while laminoplasty (HR, .541; 95% CI, .194-1.507; P = .240) did not show significant results (Table 5).
Discussion
The present study demonstrated that reoperation rate after cervical spine operations in patients with athetoid CP was 21.0%. Anterior fusion exhibited the greatest risk of revision at 42.7%, whereas combined fusion exhibited the least risk at 11.1%. For patients who underwent anterior fusion as the initial operation, posterior fusion was the most common type of revision operation, and vice versa. However, complication rates, including infection, hematoma, mechanical failure, and mortality, did not significantly differ according to the type of initial surgery.
Postoperative courses in patients with athetoid CP undergoing cervical spine surgery have been reported to be more complicated than those in patients without CP.2,17 Continuous involuntary neck muscle movement accelerates degenerative changes, which can lead to adjacent segment problems, progression of kyphosis, instability, and instrumentation loosening.8,15,18 More rigid fixation, including anterior-posterior combined fusion, has been advocated in previous studies.12,13 Kim et al compared clinical and radiographic outcomes between posterior-only fusion and anterior-posterior combined fusion 12 and found that the fusion rate was significantly higher in the combined fusion group (93%) than in the posterior-only fusion group (63%) (P = .02). 12 Additionally, the combined fusion group demonstrated significantly lower neck pain at the final follow-up, whereas instrumentation loosening was significantly higher in the posterior-only fusion group (60% vs 21%, P = .01). 12 Our study also demonstrated that the revision rate of combined fusion (11.1%) was the lowest compared to other surgical methods (HR, .371; P < .001). Combined fusion provides the greatest fixation power, aiding in solid fusion and maintaining kyphosis correction, potentially lowering the need for revision surgery.12,13 Therefore, combined fusion should be considered a primary option when planning surgical treatment for cervical myelopathy/radiculopathy in patients with athetoid CP, especially for those requiring multi-level surgery, correction of deformity, or instability.12,13
Anterior fusion was associated with the highest cumulative revision rate (42.7%). It provides stability through the anterior cervical plate and friction between the interbody device and vertebral body.19,20 However, the lack of posterior fixation cannot limit facet joint movement and degeneration due to continuous involuntary neck muscle movements, which can lead to pseudarthrosis or progression of deformity.12,21 Few studies have focused on anterior cervical fusion in patients with athetoid CP, and the mode of failure requiring revision surgery is not well understood. In a case series reported by Azuma et al, outcomes of anterior cervical fusion for patients with athetoid CP were poor, resulting in both neurological and radiographic deterioration. 6 Therefore, anterior-only fusion in patients with athetoid CP should be avoided due to the significantly high complication rate compared to other methods. 6
In this study, the revision rate for posterior fusion in patients with athetoid CP was higher at 13.8% compared with that of combined fusion; however, the difference (2.7%) was not substantial. Demura et al reported favorable outcomes for posterior-only fusion in patients with athetoid CP. 5 The study reported that solid fusion was achieved in all patients, and 2 of 17 (11.7%) patients required revision operation due to adjacent segmental instability. 5 Posterior fixation can limit cervical spine movement due to continuous posterior neck musculature movement, which may decrease the complication rate compared to anterior surgery.1,21 A cadaveric biomechanical study by Dahdaleh et al suggested that the mechanical loading on the cervical spine of a posterior instrumentation-only construct is not significantly different from that of combined fusion. 22 However, since this study and previous reports have demonstrated higher complication and revision rates for the posterior-only construct than those of the anterior-posterior combined construct, 12 posterior-only fusion should be performed after careful patient selection, considering the degree of involuntary movement, deformity, medical condition, and instability. Although the number of levels fused could not be identified in the national database, considering that posterior fusion usually involves more levels than anterior fusion, the lower revision rate for posterior fusion further supports the advantages of posterior over anterior surgery. 17
The revision rate for cervical laminoplasty in patients with athetoid CP was 13.1%, which was the second lowest value, although the results of multivariate cox-regression analysis did not reach statistical significance. Previous studies have suggested that laminoplasty is a feasible surgical option for patients with athetoid CP without resulting in significant instability or deformity, despite fusion being recommended for most cases.13-15,23 It appears that laminoplasty is also a good option when only decompression is needed without the need for alignment correction or fusion. 14 However, as this study is based on a national cohort analysis, details of each patient were not available. Factors such as sagittal alignment, instability, and preoperative symptoms are not included in the database, so we could not clarify which factors led to the selection of laminoplasty rather than fusion for treating cervical degenerative pathology in patients with athetoid CP. Further clarification on this matter is warranted.
Obesity and older age of >60 years demonstrated significant result in the univariate cox-regression analysis. Puvanesarajah et al suggested that obesity is a risk factor for readmission after cervical spine operation in patients aged >65 years. 24 Kalanithi et al reported that obesity increases cost and complication rates in spinal arthrodesis procedures. 25 Furthermore, in their healthcare database analysis, Derman et al reported that younger age is associated with an increased risk of revision operation after cervical spine arthrodesis. 26 Nevertheless, multivariate analysis in the current study did not demonstrate significant results with age and BMI, and these factors would not be considered as a risk factor for revision surgery after cervical spine operation for athetoid CP patients.
This study has both strengths and limitations as a national database analysis. The study included a larger number of patients with athetoid CP who underwent cervical spine surgery than could be acquired from a single-center study. Since the incidence of athetoid CP is low, this study design could more clearly identify the risk of revision operation after initial cervical spine operation. However, several limitations also exist. First, details of patients undergoing revision could not be identified. Data including the number of levels fused, patient symptoms, severity of athetoid CP, and detailed reasons for revision could not be identified from the national cohort database, as the database includes only demographic factors, diagnosis codes, and procedural codes. Patients could have different reasons for reoperation, including adjacent segment problems, progressive deformity, or postoperative pseudarthrosis.2,23,27 Although this study clarifies the overall risk of reoperation, it could not demonstrate individual risks for each postoperative complication. Second, the rate of perioperative complications may not be clearly identified since physicians are not obligated to register complication diagnoses within the national cohort. Third, the materials and devices used for fusion could not be identified. Since the revision rate for anterior fusion was high, identifying interbody device and cervical plate used for anterior fusion surgery is particularly important. Different interbody spacers could lead to different fusion rates, and applying anterior cervical plates could enhance construct stability.28,29 However, the codes for interbody device and anterior cervical plate were not stored in the national database, and such information could not be identified. Fourth, we could not identify whether the revision rate differed between different techniques used for posterior fusion since information regarding screw insertion techniques was not recorded in the national database. Pedicle screw fixation for the cervical spine provides strong three-column fixation which might decrease the need for revision, while lateral mass screw fixation may increase risk of construct failure. 30 Finally, the study was conducted in a single race-dominant nation and may not be equally applicable to different ethnic groups. However, these limitations are inherent to being a national cohort-based study and cannot be completely avoided. Future research should aim to clarify different risks of reoperation with various surgical approaches in patients with athetoid CP using a large sample size and national data. 16
In conclusion, anterior fusion exhibited the greatest reoperation risk (42.7%) after cervical spine surgery in patients with athetoid CP. Therefore, anterior-only fusion in patients with athetoid CP should be avoided or provided to strictly selected patients. Combined fusion exhibited the lowest revision risk (11.1%) and can be safely applied to these patients. The revision rates for posterior fusion (13.8%) and laminoplasty (13.1%) were also lower than that of anterior fusion and can be performed in selected patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was financially supported by IL-YANG Pharmaceutical Co., Ltd.