
Abstract
Study Design
Narrative Review
Objective
To provide an overview of etiology and risk factors of airway complications after anterior cervical spine surgery (ACSS).
Methods
A search was performed in PubMed and adapted for use in other databases, including Embase, Cochrane Library, Cochrane Register of Controlled Trials, Health Technology Assessment database, and NHS Economic Evaluation Database.
Results
81 full-text studies were reviewed. A total of 53 papers were included were included in the review and an additional four references were extracted from other references. 39 papers were categorized as etiology and 42 as risk factors.
Conclusions
Most of the literature on airway compromise after ACSS is level III or IV evidence. Currently, there are no systems in place to risk-stratify patients undergoing ACSS regarding airway compromise or guidelines on how to manage patients when these complications do occur. This review focused on theory, primarily etiology and risk factors.
Keywords
Introduction
Anterior cervical spine surgery (ACSS) is commonly performed to treat cervical spondylotic myelopathy and radiculopathy. 1 Anterior approaches to the cervical spine are generally safe but may be associated with complications such as dysphagia, hoarseness, dysphonia, and rarely airway-related complications. Airway complications are those causing obstruction requiring prolonged or unplanned respiratory support. These occur with a reported incidence of 0.57-6.1% after ACSS,1-4 of which approximately one-third result in postoperative reintubation. 5 The rate of postoperative prolonged ventilatory support has also been reported to be as high as 0.6% for single-level to 1.9% for multilevel cervical surgeries3,6 and is associated with a 2.5-to 4-fold increase in mortality. 7 Despite their infrequency, airway complications can be devastating if unrecognized or if treatment is delayed, and as such, comprehensive knowledge of their risk factors and treatment is necessary for any spine surgeon.6,8
We performed a systematic review of all available literature regarding airway complications after ACSS to compile information on the etiology and risk factors. Most studies found from this medical database search were level III or IV studies. The authors aim to provide a comprehensive narrative review that will focus on theory, primarily etiology and risk factors, of this important complication.
Methods
A search was performed by a medical librarian in PubMed. It was then adapted for use in other databases, including Embase, Cochrane Library, Cochrane Register of Controlled Trials, Health Technology Assessment database, and NHS Economic Evaluation Database. The search terms included a combination of keywords and controlled vocabularies: “airway complications,” respiratory difficulty”, “intubation,” “airway obstruction”, “anterior cervical spine surgery,” “anterior cervical discectomy,” “anterior cervical fusion, and” “anterior corpectomy.” The full search strategy can be found in the Appendix. The date range was limited to January 1, 1990, to December 21, 2021. The search was performed in all databases on April 18, 2019, with an update on December 21, 2021. Studies were imported into the Covidence platform (Veritas Health Innovation Ltd; Melbourne, Australia), where they were deduplicated, and the screening process was completed by three authors (LC, LB, and YK). Title and abstract screening was conducted first, followed by full-text screening (Figure 1). Any disagreements were resolved through an independent review by all authors. Disagreements after this secondary review were resolved through discussion between the authors after a full-text review. The selected papers included randomized controlled trials (RCT), meta-analyses, systematic reviews, prospective and retrospective cohort studies, case series, and case reports. PRISMA Diagram.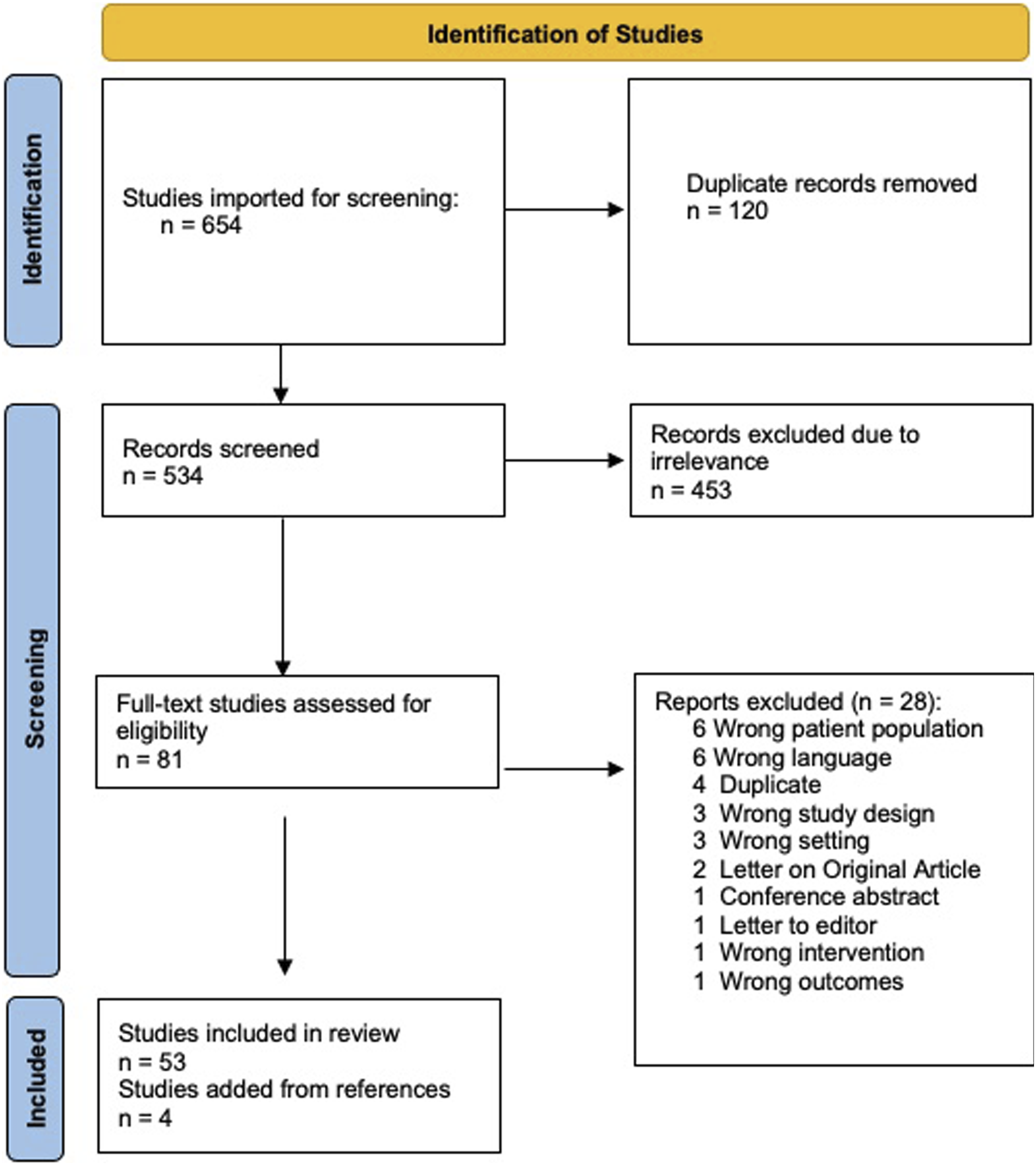
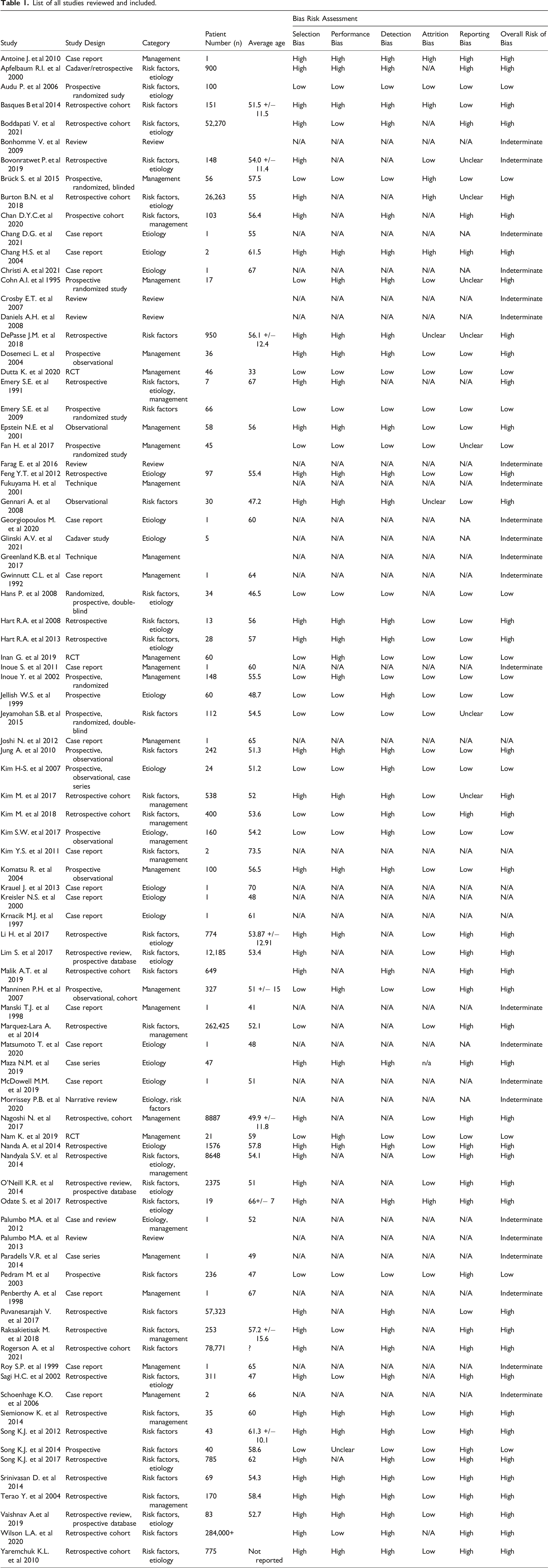
Each included paper was then grouped into two categories according to the content of the paper– etiology and risk factors. A paper was included under Etiology if the authors discussed the cause of the development of airway complications. The risk factor category included papers that assessed variables influencing the risk of developing airway complications. These categories were determined by three authors (LB, ES, and YK). Disagreements were resolved after discussion and majority voting. 39 papers were categorized as etiology, 42 as risk factors.
List of all studies reviewed and included.
Results
The screening and selection processes are presented in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram (Figure 1). A total of 654 studies were identified, of which 120 were duplicates. A total of 453 studies were excluded because of irrelevance during the first phase of the screening process. The reviewers assessed 81 full-text studies. Of these, 53 papers were found to be relevant and included in this review. The most common reasons for exclusion at this stage were incorrect patient population, 6 non-English language proficiency, 6 and duplicate papers. 4 Five additional papers were included in the references during full text review and writing of the manuscript; four were obtained from the references of the selected papers and one reference for the bias risk assessment used in this study.
As described above, the selected papers were grouped into three categories: etiology, risk factors, and management. This review is structured into two parts. The first part will focus on etiology and risk factors of airway compromise after ACSS. These will be grouped to allow for a discussion of the pre-complication evaluation and management. The second part discusses treatment after airway complications occur.
Etiology
Edema/Soft Tissue Swelling
Edema of the laryngopharynx and prevertebral soft tissues is the most common cause of airway obstruction in the early postoperative period.5,10 Risk factors for increased soft tissue swelling after ACSS are discussed later in this review. Although the current literature does not provide an evidence-based explanation for the cause of edema, the most supported hypothesis is that local trauma during surgical dissection or retractor splay may lead to soft tissue damage. In theory, trauma during surgical dissection may be minimized using low-power monopolar electrocautery, although this has not been proven. 11
Multilevel anterior cervical spine procedures are associated with increased soft tissue swelling. 12 Given the high risk in these cases, Emery et al. recommended that patients remain intubated overnight at a high acuity, closely monitored setting with a 20° head-of-bed elevation. They suggested evaluating functional edema with a postoperative cuff leak test, in which the endotracheal tube is only removed if the patient can demonstrate patent airflow around a deflated tube. 12 Furthermore, Emery et al. performed a separate double-blinded randomized controlled trial (RCT) and found that perioperative intravenous steroids decreased both prevertebral edema and the incidence of delayed extubation. 13 Despite both of these studies, such recommendations are not established practices or community standards.
Though peak swelling occurs on the second and third postoperative days, with swelling around or cranial to C5 being more clinically significant than caudal to C5,14,15 significant prevertebral soft tissue swelling may present immediately after surgery, leading to obstructed airways and cerebral hypoperfusion. 16 Edema can take up to one month to resolve postoperatively at C3 (pharyngeal airway) and three months at C6 (laryngeal airway). 11 Thus, surgeons should keep this in mind when evaluating patients postoperatively within three months after anterior cervical decompression and fusion (ACDF).
Compressive Hematoma
Postoperative hematoma can lead to airway compromise requiring acute reoperation after ACSS 17 in .4%-1.2% of cases.18-20 Although a compressive hematoma typically presents within the first 24 h of surgery, up to 37% of these are diagnosed after the patient has already been discharged from the hospital,17,21 up to six weeks postoperatively. 22 Potential causes of the development of compressive hematomas include vascular damage, intramuscular bleeding due to excessive intraoperative retraction, ineffective hemostasis, increased blood pressure, and delayed bleeding from arterial aneurysms or dissections.14,20 Additionally, a recent history of COVID infection may also worsen the prognosis of patients who develop a postoperative hematoma due to post-infection neurological hypercoagulability, the mechanism of which is not fully understood. 23
Patients who develop compressive hematoma have a higher risk of subsequent ventilator requirement, pneumonia, re-intubation, and reoperation.8,17,4 As such, identifying high-risk patients (as discussed below in the Risk Factors section) may assist surgeons in identifying those who may require prolonged observation after ACSS. Given the trend towards outpatient ACSS, the identification of such patients is crucial. 24
Cerebrospinal Fluid Leak
The incidence of dural tears in ACSS is 3.7%. 14 Patients undergoing revision ACSS and those with ossification of the posterior longitudinal ligament (OPLL) are at increased risk of dural tears, which can lead to airway compromise via the accumulation of compressive cerebrospinal fluid (CSF), similar to a hematoma.14,25 Treatment generally consists primary repair of the durotomy if feasible, observation, and possible placement of a closed lumbar drain in patients with a persistent dural CSF leak to prevent accumulation and compression. 25
Rare Etiologies
Bone graft extrusion can cause acute airway occlusion with a reported incidence of 0.88%. 18 Other rare etiologies of airway compromise after ACSS include laryngeal dislocation, improper fitting of a rigid cervical collar, bilateral vocal cord paralysis from recurrent laryngeal nerve (RLN) injury, and severe angioedema.18,26-29 Angioedema is often misdiagnosed due to its rarity but typically presents within 6-12 hours postoperatively. 29 Angioedema may occur as a rare side effect of medications (e.g., risedronate and parecoxib) or due to the presence of a lesion in the laryngopharynx, as is the case with a pre-existing epiglottic cyst; 29 but in most reported cases, it appears to be idiopathic. 28 Angioedema typically presents as a postoperative hematoma but is distinguished by associated tongue swelling and a lack of hematoma on imaging.
Risk Factors
Although the guidelines are not well established in the literature, several studies have evaluated the risk factors for postoperative airway compromise after ACSS. These are further subdivided into patient, operative, and anesthetic factors in the following section.
Patient Factors
Anatomy
Patients with OPLL are at an increased risk of complications following ACSS,14,19,30 including dural tears, compressive hematomas, and airway edema requiring additional postoperative respiratory support. 30 Both OPLL and diffuse idiopathic skeletal hyperostosis (DISH) have been found to be independent risk factors for the development of postoperative hematoma after ACSS. 19 DISH, a condition causing spinal ligamentous calcification, ossification, and paravertebral osteophyte formation, increases the risk of postoperative airway edema, requiring additional respiratory support after ACSS. 31 Additionally, anterior cervical vertebral osteophytes combined with subglottic stenosis in DISH may distort the airway, resulting in traumatic intubation, further increasing the risk of edema. Fiberoptic-assisted awake intubation is a safe option for such patients. 31
Sex
There are contradictory data supporting sex as a risk factor for airway complications after ACSS. Some studies have found that the female sex is a risk factor.5,13 Although unproven, it is postulated that the increased risk in women could be due to a smaller tracheal diameter or the mucous membranes being more susceptible to trauma. 13 In contrast, male sex has been found to be a risk factor for both pharyngeal and laryngeal airway soft tissue swelling 11 as well as unplanned intubation and ventilator requirement after ACSS in several other studies.2,4,32,33
Medical Comorbidities
Risk factors for Airway Complications after ACSS.
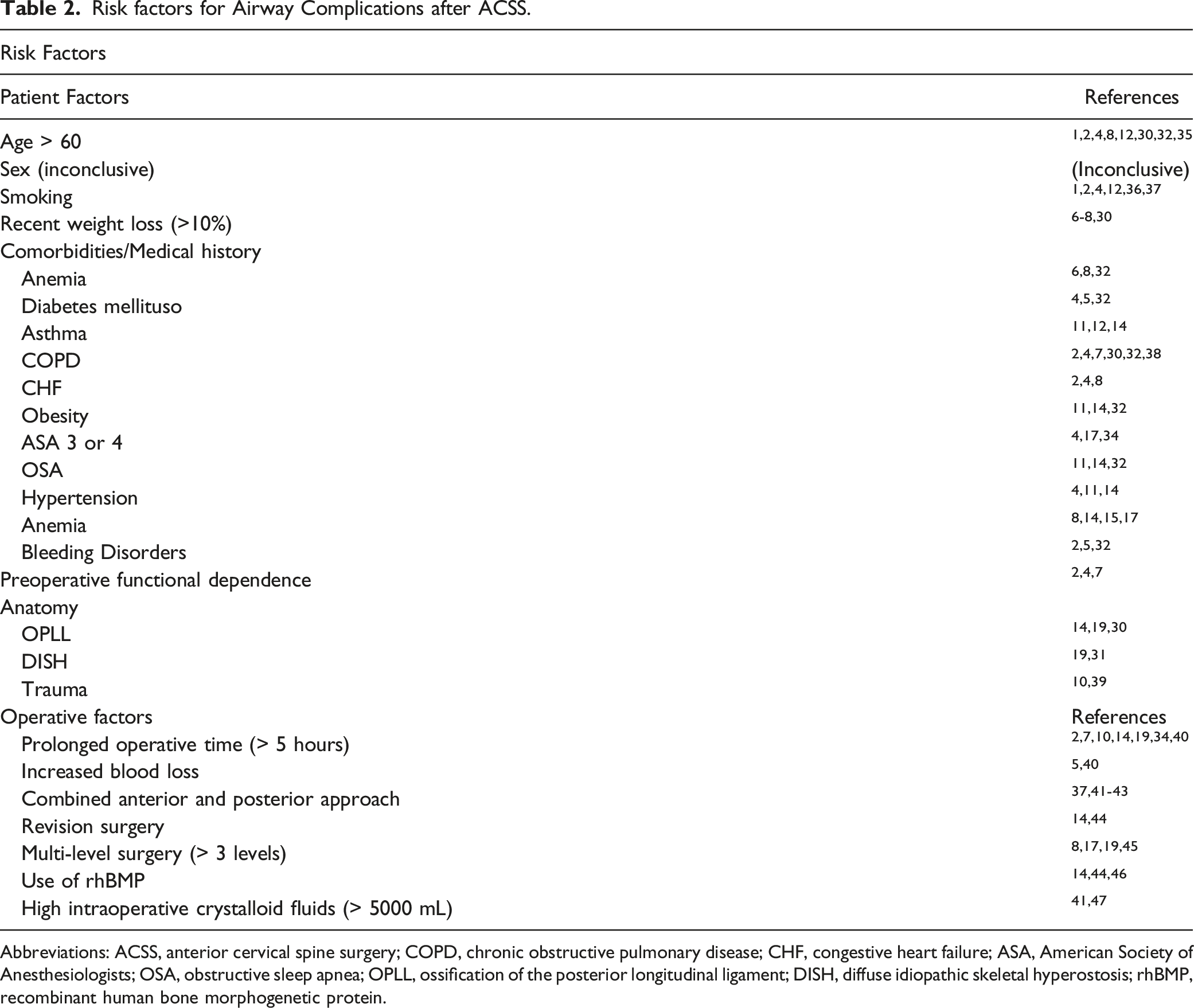
Abbreviations: ACSS, anterior cervical spine surgery; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; ASA, American Society of Anesthesiologists; OSA, obstructive sleep apnea; OPLL, ossification of the posterior longitudinal ligament; DISH, diffuse idiopathic skeletal hyperostosis; rhBMP, recombinant human bone morphogenetic protein.
Age
Age over 60 years is a risk factor for airway obstruction after ACSS.1,2,8,32 Furthermore, patients aged > 80 are more likely to experience reintubation (OR 2.34) and aspiration pneumonitis (OR 3.17) postoperatively when compared to patients aged 65-79 years. 35 Li et al. hypothesized that the capability of the airway mucosa to respond to stimulation, such as from compression from an obstructive lesion or edema, decreases in older patients, further increasing their risk of airway compromise. 1
Smoking
The literature on smoking as a risk factor for airway compromise after ACSS is mixed. Most studies have found that smoking is a risk factor for airway obstruction after ACSS (OR 1.5, P = .042).1,12 Li et al. found this risk to be further increased in smokers over the age of 60 years. Both smoking and increased age significantly reduce the quantity and length of epithelial cilia in the airway mucosa and inhibit fluid exchange from damaging peritubular capillaries; therefore, when obstruction or edema occurs, the subsequent decrease in oxygenation can result in vessel wall thickening, delayed resolution of edema, and postoperative ischemia. 1 Nevertheless, one study found that smoking was not a risk factor for airway complications after ACDF. 2
Importantly, the incidence and severity of coughing during both induction of anesthesia and extubation are significantly higher in smokers, regardless of the type of anesthesia used for maintenance. 36 Coughing during emergence from general anesthesia may place these patients at an increased risk of bleeding or displacement of the graft, given the high intrathoracic pressures generated during cough.
Functional Independence
Functional dependence is defined as requiring partial or total assistance to carry out activities of daily living 7 and has been found to be associated with respiratory complications after ACSS in several large registry studies.2,4,7 In their regression analysis, Lim et al. found that dependent status was a significant predictor of airway complications after ACSS (OR 2.4). 2 Boddapati et al. evaluated a larger cohort from the same registry over a longer period and found that dependent functional status was a significant risk factor for respiratory compromise after ACSS (OR 4.4). 4 Finally, Burton et al. found preoperative functional dependent status to be a good marker for unplanned postoperative intubation after elective ACSS 7
Trauma
Patients with cervical trauma present additional challenges in airway management. 39 These patients often have concomitant maxillofacial trauma and upper airway obstruction due to soft tissue swelling, which makes intubation difficult. Additionally, they often present without NPO or rigid immobilization from a cervical collar. Despite these circumstances, they often a require rapid airway. 39 In fact, in a study evaluating a postoperative protocol for delayed extubation in high-risk patients after ACSS, Kim et al. found trauma to be a significant risk factor for respiratory impairment requiring re-intubation or tracheostomy. 10
Operative Factors
Type of Surgery
Multi-level surgery is an independent risk factor for postoperative complications, such as dysphagia, postoperative hematoma, and unplanned re-intubation.3,8,19 In addition to the longer operative time,12,44 three- or four-level ACDF may result in increased complications, such as respiratory discomfort (6.9%), swallowing difficulty (9.3%), and hoarseness (2.3%). 45 Li et al. also found a direct correlation between the number of segments exposed during surgery and the risk of airway complications. In their series, the incidence of airway obstruction was 0.3% for single-level surgeries vs 5% for ≥3 levels; in addition, airway obstruction was 2.5x higher for surgeries above C5 than for below. 1
Li et al. found anterior cervical corpectomy to be a significant risk factor for postoperative airway obstruction compared with ACDF (OR 3.4, P < .01). 1 They reasoned that, in addition to the overall longer surgical time, corpectomy requires more dissection, disturbing more soft tissue with a higher incidence of peripheral nerve edema and injury. Additionally, subtotal vertebral resection generally results in increased bleeding and a higher rate of hematoma formation. Chan et al. developed and evaluated a protocol for all patients undergoing ACSS with corpectomy, involving admission to the ICU for observation after surgery. They did not find corpectomy to be associated with increased complications or an extended ICU stay. However, some patients were extubated in the operating room immediately after surgery, while others were kept inbutated upon admission to the ICU, and the authors did not mention their rationale or algorithm for choosing one. 48
Revision surgery is a risk factor for the development of postoperative dysphagia, prevertebral edema, and dural tears after ACSS.14,44 ACSS as a revision surgery for patients with OPLL who have previously undergone posterior cervical laminoplasty is associated with a 42% risk of CSF leak; thus, it is recommended that these patients undergo initial posterior fusion to prevent such challenging revision surgery. 30
Kim et al. also found that combined anterior and posterior (A-P) cervical procedures are associated with an increased risk of postoperative airway compromise (OR 10.9, P = .000). 10 Furthermore, A-P cervical procedures that cross the cervicothoracic junction pose an increased risk of airway complication.37,41-43 Hart et al. found a 38% incidence of postoperative re-intubation due to airway edema and a 7% incidence of pneumonia following AP cervical spine surgery. 42 As such, Hart et al. established a protocol for intraoperative crystalloid restriction and maintenance of hemodynamic status with vasopressors and colloids. This protocol resulted in a lower incidence of prolonged postoperative intubation or reintubation (45% vs 0%, P = .029). 41 In addition, they placed patients in an upright position overnight and used a standardized endotracheal tube.
Length of surgery
A prolonged surgical time, especially greater than five hours, is a risk factor for adverse airway events after ACSS.2,10,14,19,40 Daniels et al. reported that surgeries exceeding this length result in airway compromise caused by prevertebral swelling. 14 In addition, DePasse et al. found that patients with complications after cervical deformity surgery had an average longer surgical duration (mean, 5.6 hours). 34 Kwon et al. found that several intraoperative factors, including a longer operative time, were significantly associated with delayed extubation after single-stage A-P cervical decompression and fusion. Similarly, a higher volume of crystalloid replacement, blood transfusion, and increased blood loss are associated with delayed extubation. 47
The current literature suggests that patients undergoing shorter surgeries have minimal to no incidence of airway compromise and may qualify for ambulatory surgery after a short postoperative observation period. Gennari et al. had a 7% readmission rate when performing outpatient, single-level ACDF, or cervical disc replacement with the following strict patient selection criteria: absence of myelopathy, single-level disc disease, C5-C7 level, ASA 1 or 2, normal cervical morphology, no prior cervical spine surgery, and residing within 30 minutes of an emergency room. Of note, their reported average operative time was 38 min, and patients were monitored for an average of 7 h postoperatively. 49
Interbody Graft Extrusion
Interbody graft extrusion occurs with a reported incidence of 6.4% and may cause airway compromise in the intermediate postoperative period (1-6 weeks), requiring re-operation.14,50 Risk factors associated with graft extrusion include multilevel corpectomy, previous cervical laminectomy, graft over-tensioning, and osteoporosis. 14 Concomitant posterior segmental instrumentation should be considered when performing corpectomies exceeding two levels, especially when using a buttress plate anteriorly after graft placement. 51 In a case series, Riew et al. reported one patient who had graft dislodgement with failure of buttress plating, resulting in death from airway compromise after multilevel anterior cervical corpectomy. 51
Use of Bone Morphogenetic Protein
Recombinant human BMP-2 (rhBMP-2) has been used off-label in ACSS to augment the fusion. However, its use carries a significant risk of postoperative complications such as soft tissue swelling, dysphagia, respiratory failure, unplanned intubations, and increased 90-day mortality.14,44,46 Its use is also associated with increased LOS and ICU admission.14,46 The etiology is believed to be an extensive soft-tissue inflammatory reaction in the first week postoperatively caused by the use of BMP. 46 In their case series, Maza et al. used low-dose rhBMP-2 during single- and multi-level ACDF and demonstrated that adverse respiratory outcomes could be reduced through the administration of steroids without increased adverse effects. 52 If intended for use during ACSS, surgeons should be aware of its off-label use and the potential for airway complications. Further research is required to determine the benefit and appropriate dosing of rhBMP-2 in anterior cervical spine surgery.
Steroids
The benefits of using steroids must be weighed against the risks of wound complications and delayed fusion. In their RCT, Song et al. found that intravenous methylprednisolone for 24 hours after multilevel ACSS lowered the rate of dysphagia and soft tissue swelling in the acute postoperative period without increasing the risk of complications. 53 Similarly, other studies have suggested a benefit of the use of immediate postoperative intravenous methylprednisolone to reduce pharyngeal abnormalities after ACSS. 54 In a large registry database review, Wilson et al. found steroid use to be one of the few factors that decreased the risk of reintubation on postoperative day 1 after ACDF. 33 In addition to intravenous administration, local steroid application to the surgical wound after ACDF can significantly reduce soft tissue swelling and odynophagia without additional complications. 55 This practice is useful for patients at a high risk of developing dysphagia postoperatively, such as women and those undergoing multi-level or revision surgeries. A double-blinded RCT comparing intra- and post-operative dexamethasone-to-saline infusion had a 2.7% rate of airway compromise requiring intubation, all of which were in the saline-only group. Moreover, patients who received dexamethasone also had significantly lower rates of dysphagia, which translated into a shorter hospital LOS. However, patients who received steroids had lower fusion rates at 6 months, although these rates were equivalent at one year. 56
Drains
The use of drains is controversial, and their benefits have not been clearly defined in the literature. 57 Surgeons frequently place drains after ACDF to prevent postoperative hematoma. 58 Basques et al. found that age > 50 years, history of smoking, and multilevel surgery were associated with higher drain output. In their results, the odds ratio for high drain output (defined as more than 30 mL) increased from 2.7 for a 2-level surgery to 17.0 for 3- or 4- level surgeries. 58 These risk factors may help guide surgeons in selecting which patients may benefit from drain placement after an ACDF, but no current recommendation can be made for the effect of drains on airway safety.
Discussion
The present study provides a comprehensive review of the etiologies and risk factors of airway complications after ACSS. These are defined by an obstruction of the airway requiring unplanned advanced ventilatory support, either through prolonged postoperative intubation or unplanned re-intubation. To our knowledge, no other systematic review has specifically evaluated the etiology and risk factors of airway complications after ACSS. Sagi and Li et al. evaluated the incidence of reintubation after ACSS and the risk factors for airway complications after ACSS, respectively, in retrospective cohort studies.1,3 Nandyala et al. conducted a retrospective database study evaluating the incidence and risk factors of prolonged intubation or unplanned reintubation after cervical spine surgery, although it was not specific to the anterior approach. 6 Since then, two large database studies have reported the incidence and predictors of airway or respiratory complications specific to ACSS, but none have discussed the etiology or management of patients presenting with these complications.2,4
The two most common causes of airway compromise after ACSS are hematoma and soft tissue edema. Postoperative hematomas are hypothesized to occur secondary to iatrogenic vascular injury during surgery or excessive intramuscular bleeding, without adequate hemostasis. Laryngopharyngeal soft tissue swelling is hypothesized to occur because of local trauma from dissection and retraction during the anterior cervical spine approach. Other reported causes of airway compromise include cerebrospinal fluid (CSF) leakage, graft extrusion, and postoperative edema. Following the discussion of etiology, we reviewed the risk factors for airway complications after ACSS. The risk factors with the least controversy and high-level evidence are outlined in Table 1, each with their respective references. Briefly, the patient-related risk factors with the most support included age > 60 years, medical comorbidities (e.g., COPD), dependent functional status, and a history of smoking. Some surgery-related risk factors include combined A-P surgeries, operative time exceeding five hours, and revision surgery.
Currently, there are no classification or scoring systems to determine which patients undergoing ACSS are at an increased risk of airway complications. Following this review, future research should develop a scoring system to assist spine surgeons and anesthesiologists in selecting patients who are at increased risk and may require an extended postoperative monitoring period or delayed extubation. This is of particular importance as outpatient ACSS is becoming increasingly common. Additionally, this review does not discuss the available literature on management of patients with these complications or provide treatment recommendations, which is a topic of interest for a future systematic or narrative review. The authors initially conducted the medical library search for etiology, risk factors, and management of airway complications after ACSS, but focused on the former two due to the wealth of information on this topic and word count set by most journals. Thus, this review is limited in scope.
The authors hope this review provides the reader with a comprehensive summary of the available literature regarding airway compromise after ACSS – a rare but devastating complication. Spine surgeons should have a comprehensive knowledge of the etiology and risk factors in order to take any necessary steps to avoid this. The majority of literature on this topic is level III or IV evidence and efforts should be made to further investigate how to prevent this complication in the form of specific interventions that can be applied to a clinical practice guideline or algorithm.
Footnotes
Acknowledgments
The authors would like to acknowledge Bridget Jivanelli, medical librarian, for conducting a literature search and providing the manuscript with an appendix of all searched terms and medical subject headings.
Author’s Note
Dr. Albert receives royalties or licenses from DePuy Synthes Spine and Zimmer Biomet; he also has leadership or fiduciary role in other board, society, committee or advocacy groups, paid or unpaid; and has other financial or non-financial interests detailed in your journal’s desired Conflict of Interest forms. However, none of these conflicts are directly related to the work written in this manuscript. For the remaining authors, no conflicts of interest are declared.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.