
Abstract
Study Design
Narrative Review.
Objective
Pelvic fixation is a crucial technique in modern adult spinal deformity surgery, yet complications and failure rates remain high. Significant controversy exists regarding the type and number of points of pelvic fixation needed but remains poorly defined. The purpose of this article is to summarize current literature on pelvic fixation techniques, complications, and outcomes, discuss controversies, and suggest future directions.
Methods
A literature search was conducted in PubMed for publications written in English with full text available from January 2000 to January 2022 using the following search terms: “spinopelvic fixation”, “sacroiliac fixation”, “iliac screw”, “S2AI screw” and “complications” or “outcomes” together with “adult spinal deformity” and “scoliosis”.
Results
Twenty-two articles were identified as describing complications/outcomes comparing pelvic fixation techniques (S2AI vs iliac; n = 6) or as reporting on a single technique (n = 16). The main categories of pelvic fixation complications were mechanical, pseudarthrosis, wound infection, sacroiliac joint pain, and revision. Four studies found lower complication rates for S2AI screws vs iliac screws. Descriptive studies reported high rates of complications for both S2AI and iliac screws. The frequency of complications was as follows: screw fracture 1.9%-9%, screw loosening 2%-65%, L5-S1 pseudarthrosis 6%-23.9%, sacroiliac joint pain 3.2%-52.5%, revision rate 2.4%-50%.
Conclusions
Pelvic fixation with either S2AI or iliac screws provides significant stability to constructs that extend to the sacrum. Further study is needed to characterize the number of points of pelvic fixation needed and clarify the role of pelvic fixation in causation or treatment of sacroiliac joint pain.
Introduction
Pelvic fixation is a crucial tool in the spine surgeon’s armamentarium for adult and pediatric spinal deformity correction. However, risk of clinical and radiographic failure with pelvic fixation remains significant. Familiarization with multiple techniques of pelvic fixation, including revision strategies, is critical for practicing spine surgeons. Ongoing investigation into risk factors and prevention of pelvic fixation failure is necessary.
Methods
The authors performed a review of the literature to identify articles reporting complications and outcomes using pelvic fixation in adult spinal deformity. A search was conducted in PubMed database for publications from January 1, 2000 to January 1, 2022 with full text available in English language using the following search terms: “spinopelvic fixation”, “sacroiliac fixation”, “iliac screw”, “S2AI screw” and “complications” or “outcomes” together with “spinal deformity” and “scoliosis”. Inclusion criteria for the review were comparative or descriptive studies of complications, or clinical or radiographic outcomes of pelvic fixation in adult patients with thoracolumbar spinal deformity and/or scoliosis. Articles on pediatric patients, neuromuscular scoliosis, trauma, and oncology were excluded. Meta-analyses, systematic reviews, anatomical/technique descriptions, biomechanical in-vitro studies, and case-reports were excluded. All relevant full text articles were then reviewed in detail. For all reviewed articles, further assessment of reference lists including “similar article” and “cited by” functions in PubMed were performed to identify potential other qualifying studies. Because of literature heterogeneity and small number of available reports, the articles were used to create a narrative detail of the current state of knowledge of techniques, complications, and outcomes of pelvic fixation in adult spinal deformity, with special attention to limitations of current knowledge and areas of future study.
Results
Results of the Literature Review
Initial PubMed search resulted in 136 articles (Figure 1). Based on title and abstract review, 63 studies were excluded based on patient age and etiology of spinal deformity. The remaining 73 articles were then subjected to a full-text review and assessed using the described inclusion and exclusion criteria, resulting in exclusion of an additional 51 articles. The remaining 22 articles were then included for data summation and reporting on complications and outcomes of pelvic fixation in adult spinal deformity. Literature search for spinopelvic fixation complications.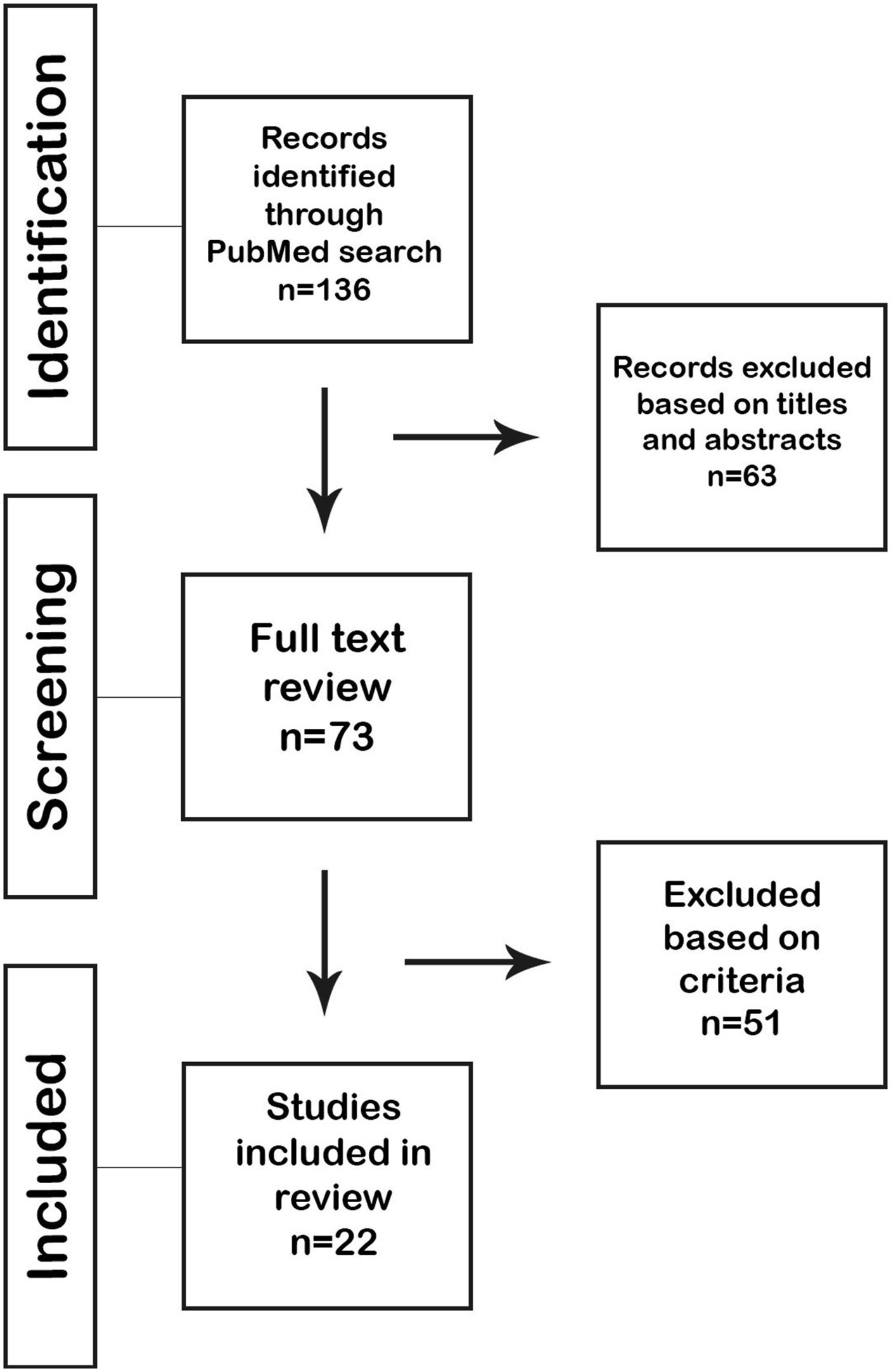
Discussion
Evolution of Spinopelvic Fixation
Pelvic fixation in spine surgery has evolved to counteract high biomechanical stress across the lumbosacral junction as well as increase deformity correction capability in cases of coronal plane malalignment. As the first surgeon to report using arthrodesis for spinal stabilization, Russell A. Hibbs recognized the lumbosacral junction as the point of greatest biomechanical strain in motion of the human spine due to the interaction of the mobile spinal segments with the immobile pelvis. 1
Hibbs’ pioneering work attempting arthrodesis across the lumbosacral junction was expanded upon by Ralph Ghormley. In 1933, Ghormley described using autogenous iliac bone graft to augment fusion across the lumbosacral junction for treatment of spondylotic pain. 2 Interfacet screws were developed in the 1940s to augment lumbosacral fusion attempts with bone grafting.3,4 Paul Harrington described the use of hook/rod constructs and a sacral bar in 1962 for treatment of spinal deformity. 5 As the evolution of spinal instrumentation continued with the development of segmental fixation by Eduardo Luque in the 1970s 6 and the popularization of pedicle screws by Yves Cotrel and Jean Dubousset in the 1980s, 7 rates of pseudoarthrosis decreased but still remained as high as 40% particularly across the lumbosacral junction. 8
Anatomy and Biomechanics of the Lumbosacral Junction
The inherent anatomy of the sacrum limits biomechanical strength of sacral fixation. 9 The transition from mobile spine to immobile pelvis concentrates significant flexion moment and cantilever force at the lumbosacral junction.9,10 A landmark biomechanical study identified a critical pivot point to be the junction site of the L5-S1 disc space and middle osteoligamentous column. 10 Extending spinal instrumentation anterior to this point significantly increased the biomechanical strength of the instrumentation construct, while extending instrumentation into the iliac wings was strongest.
The sacrum is largely cancellous bone with wide pedicles, and a thin cortical shell. Sacral cancellous bone density provides weaker anchor for sacral screw fixation that further worsens in cases with osteoporosis. 11 The S1 pedicle shape makes engaging the cortical pedicle walls difficult, while the anterior-posterior triangulated dimensions of the sacrum limit the length of screw fixation. Medial angulation of S1 pedicle screws increases screw strength, but can be technically challenging if the soft tissue envelope limits the extent of lateral to medial angulation. 12 Extending sacral screw purchase through the anterior sacral promontory, called tricortical screw purchase, significantly increases sacral screw pullout strength compared to bicortical screw purchase. 13 Addition of interbody graft at L5-S1 also increases biomechanical load to failure at sacral screws. 14 However, anchoring spinal deformity constructs at the sacrum is associated with a high rate of screw failure and pseudoarthrosis.15,16 Even using tricortical sacral pedicle screw purchase, the overall distance from the McCord pivot point to the sacral promontory is small compared to the flexion moment generated across the lumbosacral junction in long fusion constructs, meaning that even maximally sized sacral pedicle screws provide inadequate counterforce to prevent failure. Utilizing pelvic fixation extending into the iliac wings significantly increases the length of screw fixation possible to counteract the flexion moment, which in turn can decrease the rate of pseudoarthrosis and instrumentation failure seen in long-construct fusions that end at the sacrum.
Indications
Pelvic fixation was developed to counteract the anatomical constraints of sacral instrumentation and biomechanical stress of the lumbosacral junction. Multiple studies suggest that fusion across the lumbosacral junction including greater than 3 levels (i.e. above L3) is an indication for utilization of pelvic fixation to reduce the rate of pseudoarthrosis.17,18 Additional indications for pelvic fixation (Figure 2) include lumbar three-column osteotomies,
19
low thoracic or lumbar vertebral column resection,
20
high-grade spondylolisthesis, trauma with severe sacral fracture or spinopelvic dissociation, lumbosacral pseudoarthrosis, osteoporosis precluding adequate sacral fixation, and sacral tumors.21-25 Indications for pelvic fixation. A) lumbar fusion greater than 3 levels B) low thoracic/lumbar three-column osteotomy C) high-grade lumbar spondylolisthesis D) unstable sacral fracture.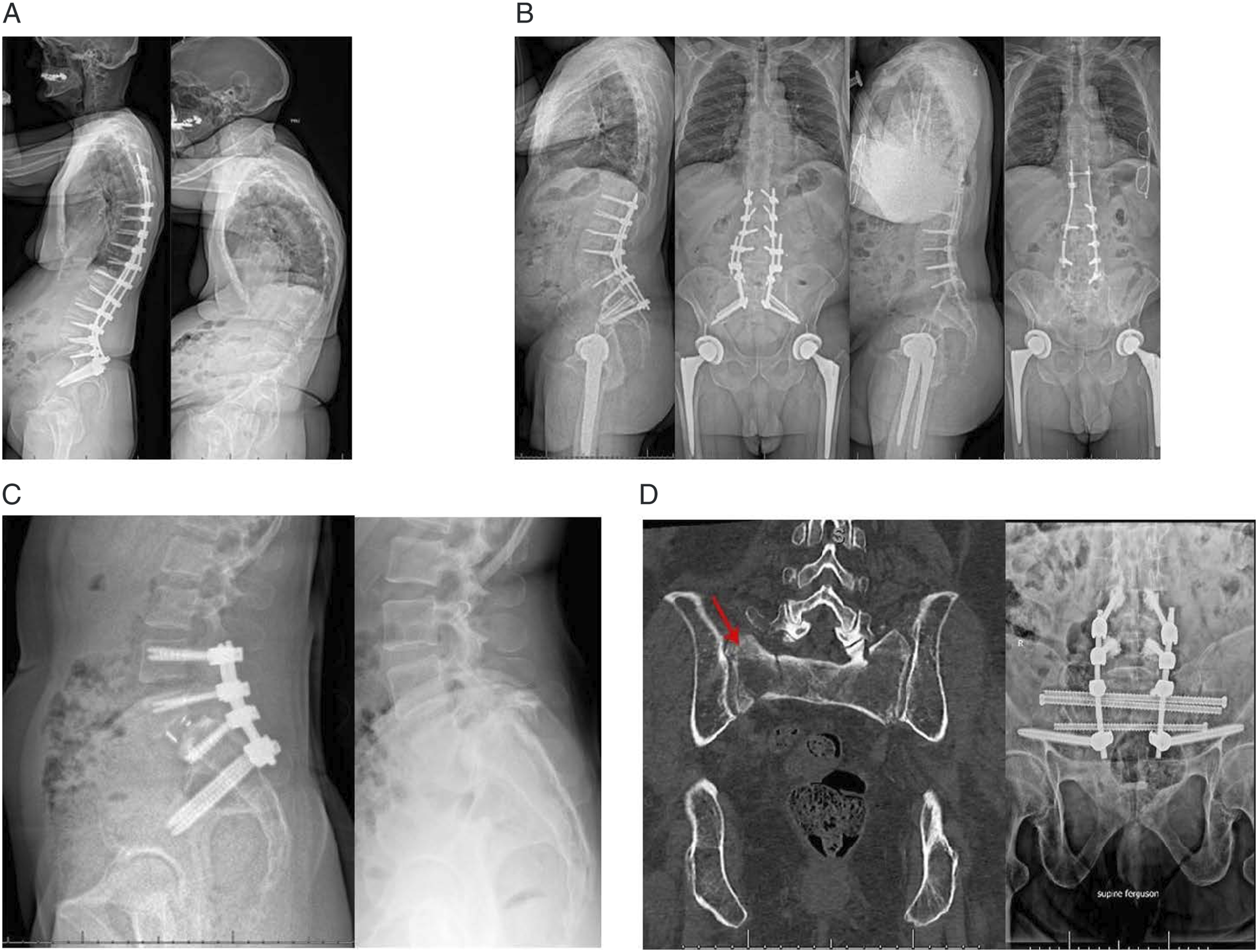
Techniques of Pelvic Fixation
Ben Allen Jr and Ron Ferguson began a new chapter in spinal instrumentation with description of the Galveston technique of pelvic fixation in the 1980s (Figure 3A).26,27 Utilization of the robust iliac cortical purchase added a strong anchor point across the lumbosacral junction and significantly decreased pseudoarthrosis rates. The Galveston technique involves contouring L-shaped rods that are connected to segmental spinal fixation points, tunneled beneath paraspinous muscles, and have the distal limb inserted at the posterior superior iliac spine (PSIS) and tunneled through the ilium between the inner and outer pelvic tables toward the anterior superior iliac spine (ASIS).
26
Allen and Ferguson investigated different lengths of pelvic segments of the Galveston rod, and reported that intraosseous iliac portions of the rod longer than 6 cm and within 1.5 cm of the sciatic notch had the highest rates of fusion.
26
Techniques of pelvic fixation. A) Galveston rods B) Iliac screws C) S2-alar-iliac (S2AI) screws D) “Stacked” S2AI screws, 4 points of pelvic fixation E) S2AI screws plus triangular titanium rods for SI joint fusion F) Kickstand rod technique with iliac screw for coronal deformity correction plus S2AI screws for pelvic fixation.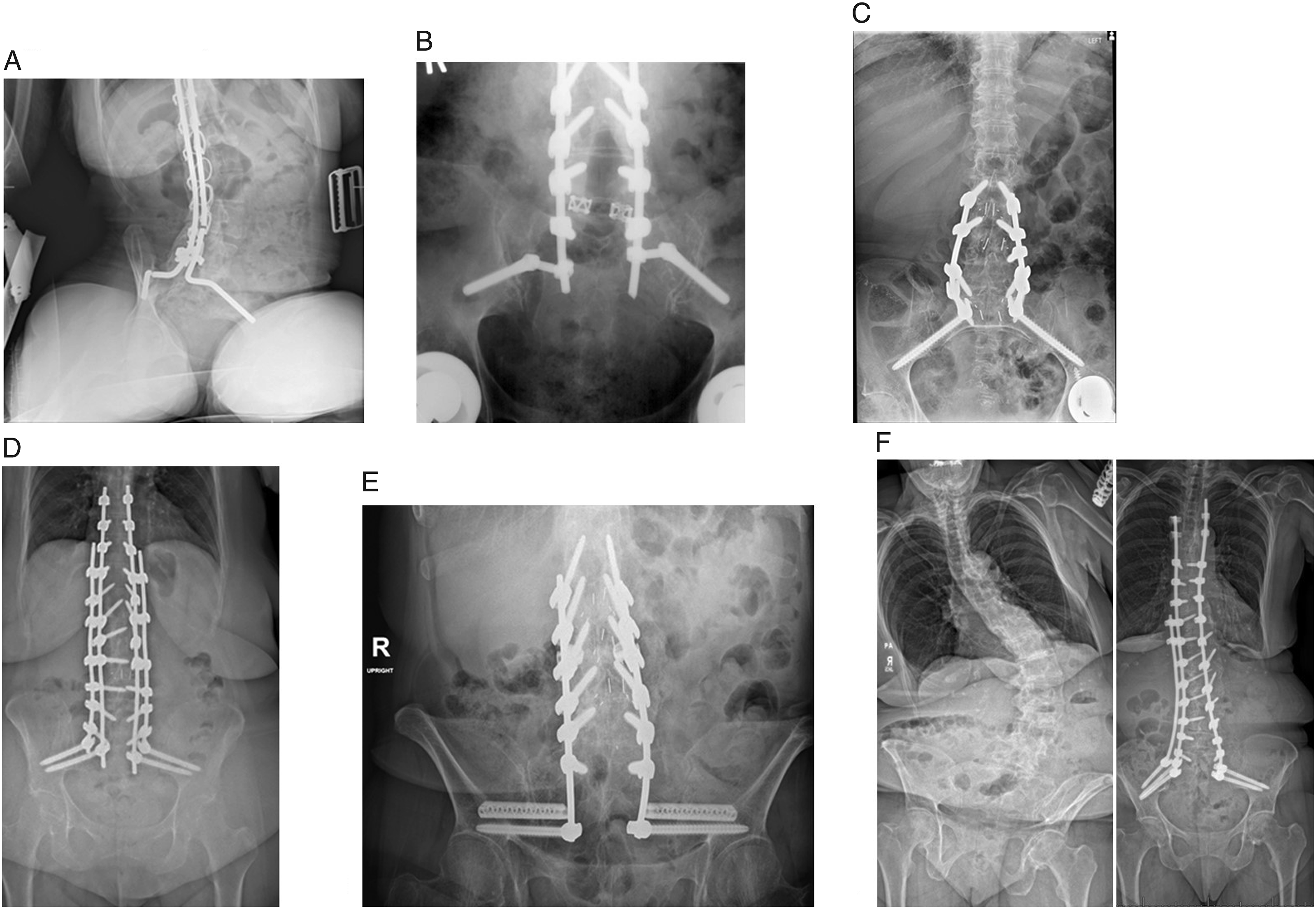
Posterior-only segmental spinal fusion attempts without pelvic fixation for adult scoliosis from above the thoracolumbar junction to the sacrum had a reported failure rate of over 50%. 28 With the advent of the Galveston technique for pelvic fixation, and popularization of anterior interbody arthrodesis, reported pseudoarthrosis rate in a similar adult spinal deformity population decreased to 12%. 29
Disadvantages of the Galveston technique include difficult rod contouring and implant prominence, leading to the development of alternate strategies of spinopelvic fixation. Iliac screws inserted as independent anchor points then connected to segmental spinal instrumentation simplified pelvic fixation technique (Figure 3B). Utilization of fully or partially threaded iliac screws with increased length reduced rates of pelvic fixation implant failure when compared to Galveston rods. 30 Traditional iliac screw starting point and trajectory is similar to the Galveston technique, inserted at the PSIS and directed through the ilium toward the ASIS. Therefore, implant prominence remains a concern for traditional iliac screw fixation, with varying reports of removal of pelvic fixation required due to symptomatic implant prominence. 31 A modified iliac screw trajectory has been described 32 to avoid implant prominence and obviate the need for offset connectors, with adequate efficacy. 33 Alternative strategies of pelvic fixation to reduce implant prominence include Jackson intra-sacral rods 34 and the Kostuik-Harrington transiliac bar. 35 When compared to sacral pedicle screws alone or sacral pedicle plus sacral alar screws or a sacral bar, the addition of iliac screws significantly increases load to failure. 14 Iliac fixation has therefore become the modern standard of care in spinopelvic instrumentation.
An alternative form of iliac fixation is the S2-alar-iliac (S2AI) screw trajectory first described in 2007. 36 S2AI screws utilize a more medial starting point than traditional iliac screw trajectory, approximately 25 mm off midline (Figure 3C). Compared to iliac screws, S2AI screws require less soft tissue dissection for placement, have decreased implant prominence, and do not require offset connector attachment for rod alignment with pedicle screw anchor points. 37 The starting point is defined by identifying a line connecting the lateral aspect of S1 and S2 dorsal foramina, then entering the sacrum at a point about 1/3rd the length of that line caudal to the S1 foramina. 37 The trajectory is about 40 degrees lateral and 40 degrees caudal, aiming just above the sciatic notch toward the anterior superior iliac spine. 31 Obturator oblique inlet radiographic images, aiming 30 degrees caudally and 30 degrees laterally, create a teardrop view to visualize the S2AI screw trajectory target from a medial-lateral perspective, while sagittal radiographs aiming at the greater trochanter allow for adjustment of the ideal superior-inferior trajectory. Unlike the traditional iliac screw, the S2AI screw trajectory crosses the sacroiliac (SI) joint. S2AI screws may be fully or partially-threaded.
Advanced Techniques in Pelvic Fixation
Multiple points of pelvic fixation can be used in varying configurations to increase the counterforce against flexion moment at the lumbosacral junction. S2AI screws can be “stacked” bilaterally with two implants on each side (Figure 3D), and multiple iliac screws can additionally be added. Triangular titanium rod implants can be inserted parallel to S2AI screws to perform concomitant open sacroiliac (SI) joint fusion along with pelvic fixation (Figure 3E). When performing more than two points of pelvic fixation in the S2AI trajectory, we prefer to place the distal S2AI screw first, locating the placement parallel to the iliopectineal line just above the sciatic notch (Video: Intraoperative technique of four points of pelvic fixation: S2AI screws plus triangular titanium rods for SI joint fusion). This strategy allows for maximal purchase strength in the iliac cortical bone as well as creates adequate room for another S2AI implant trajectory more proximally. We routinely place multiple points of pelvic fixation with 9.5 × 100 mm S2AI screws and 90 mm triangular titanium rod implants using this technique.
In cases of severe coronal deformity, an additional iliac screw placed on the side of trunk shift is useful for the kickstand rod technique to obtain additional coronal correction (Figure 3F). 38 In this technique, bilateral S2AI screws are placed along with a separate iliac screw on the side of the coronal plane deformity apex. The iliac screw serves as the base of the “kickstand” rod, which will be connected to another fixation point near the thoracolumbar junctional apex of the coronal deformity. Because sequential distraction is performed across the kickstand rod to help correct the coronal plane, this will result in flattening the lumbar lordosis. To prevent this, the sagittal contour is first optimized with conventional rods connecting pedicle screws to the S2AI screws on each side, with the set plugs on the rod contralateral to the planned kickstand rod then locked to preserve lower lumbar lordosis. The separate kickstand rod is inserted between the iliac screw and domino connectors at the thoracolumbar junction. Sequential rounds of distraction are then applied across the kickstand rod to obtain additional coronal plane correction. An alternative technique to closed-closed domino connectors is the use of dual-headed pedicle screws at the thoracolumbar junction to accommodate the kickstand rod. The ipsilateral pedicle-screw-based rod and the kickstand rod should be initially cut with enough length to accommodate the distraction.
Triangular osteosynthesis is a useful advanced pelvic fixation technique for spinopelvic dissociation with complex unstable sacral fractures or sacral tumors. 39 Trans-iliac trans-sacral screws are placed via a lateral incision, which can be done minimally-invasively. Spinopelvic fixation is then placed posteriorly (Figure 1(D)). Transiliac transsacral screw placement with fluoroscopy is technically demanding, particularly in cases of sacral dysmorphism, and carries significant risk of nerve root injury. 40 For this reason, we prefer utilization of CT-based navigation supplemented by fluoroscopy, which has been a safe and effective technique at our institution.
Biomechanics of Pelvic Fixation
Multiple biomechanical studies have demonstrated similarity between S2AI and iliac screw trajectory strengths. Lumbosacral fusion constructs anchored with iliac compared to S2AI screws have no significant difference in torsional stiffness or failure torque.41,42 Iliac screw insertional torque has been shown to peak near the lateral iliac cortex and superior iliac fossa, and is highest for screw lengths greater than 80 mm and diameter of 9.5 mm compared to 7.5 mm. 43 S2AI 65 mm and 80 mm screw lengths perform similarly to 90 mm iliac screws, and quad-cortical purchase does not significantly affect S2AI screw strength. 44 A finite element model (FEM) study found that peak von Mises stress (PVMS) values were all below physiologic fatigue strength levels for traditional iliac, modified iliac, and S2AI screw. 45 PVMS values were highest in the screw shaft for S2AI screws and highest at the iliac screw’s offset connector site. Interestingly, the FEM showed a distraction force between the screw head and screw shaft for S2AI screws but a compression force for the same area on iliac screws. Taken together, the FEM suggests potential for unique failure mechanisms in iliac vs S2AI screws. 45 Another FEM study comparing iliac to S2AI screws showed the lowest PVMS values occurred for S2AI screws greater than 90 mm in length and with 15 degrees of variable screw head adjustment angle. 46 The S2AI screws with 30 degree variable screw head adjustment angle experienced higher PVMS values, again potentially indicating a unique failure mechanism risk with hyper angulation of S2AI screw head angles.
Complications of Pelvic Fixation
Potential complications of spinopelvic fixation include mechanical failure, screw prominence/pain/wound healing difficulty, surgical site infection, neurovascular injury, sacral fracture, and sacroiliac joint pain (Figure 4). Despite technological advances in spinopelvic fixation, failure rate remains high. Mechanical failure mechanisms of pelvic fixation include fracture of the screw shaft or screw head/shaft interface, rod fractures, or dislodgement of offset connectors or set-plugs. Pelvic fixation screw loosening, manifested as radiographic lucency around the screw without frank instrumentation failure, often has unclear significance particularly in asymptomatic patients. Complications of sacropelvic fixation. A) Screw loosening B) Screw fracture C) Rod fracture D) Set-plug dislodgement with rod pull-out. E) Sacral fracture through Castellvi-Chan 3B lumbosacral transitional segment with resultant kyphotic angulation.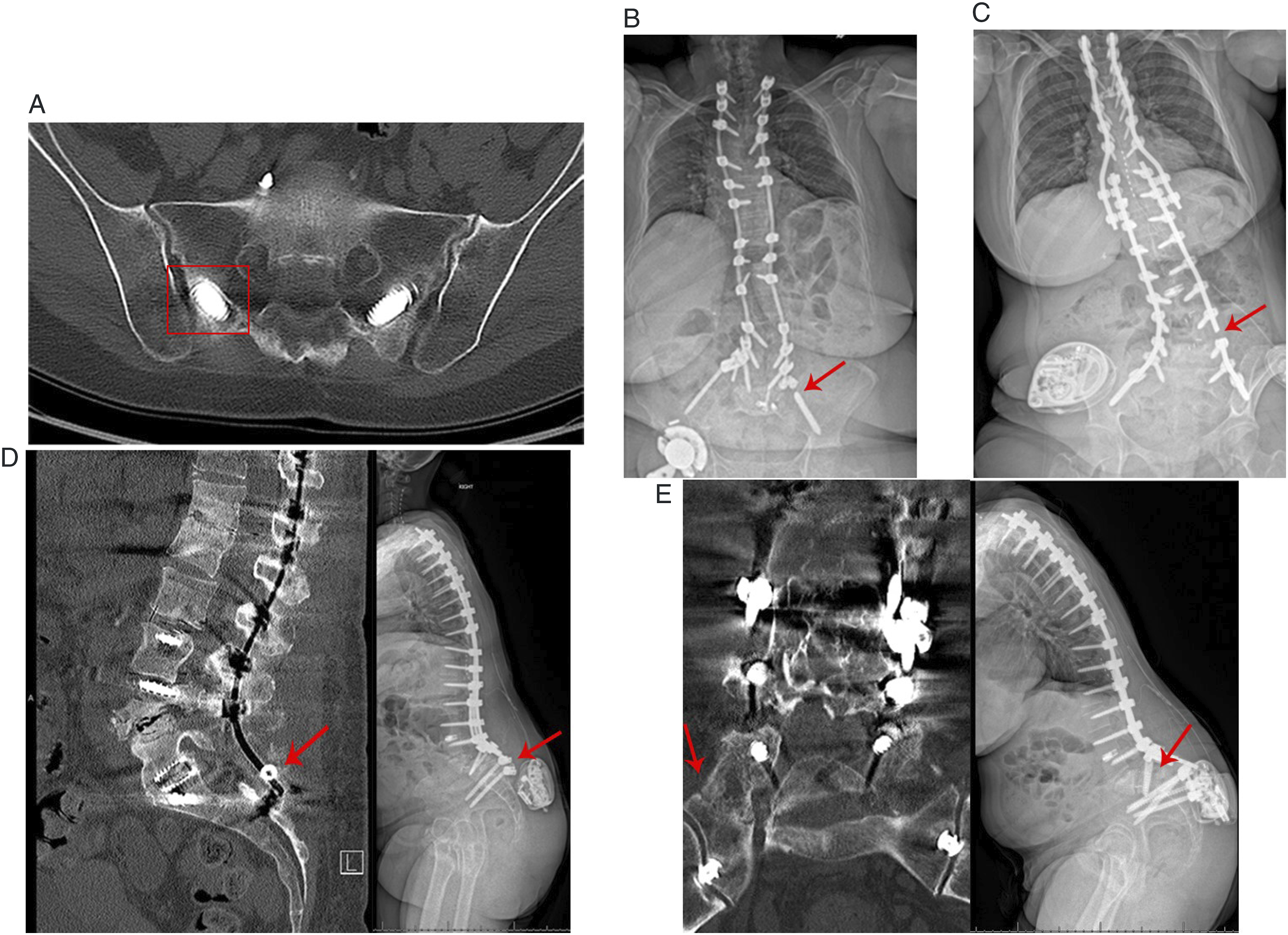
A large multicenter study of 410 adult spinal deformity patients with either S2AI or iliac screws reported an overall pelvic fixation failure rate (screw loosening/screw fracture/rod fracture) of 29.4% at two years postoperatively. 47 Revision surgery was required in 22.7% of patients overall, with no difference between S2AI and iliac groups. S2AI screws were more likely to show loosening but less commonly associated with rod fractures compared to iliac screws. Loosening of pelvic fixation without fracture occurred in 13.4% of patients and was four times as likely to occur in the S2AI group. 14% of patients had a rod fracture below L4, with a trend toward less occurrence in the S2AI group. Notably, patients who experienced any failure mechanism had less improvement in two postoperative HRQL.
At our institution, we observed acute mechanical failure of S2AI screws in 6 of 125 cases (5%) within 6 weeks postoperatively, 48 prompting a multicenter review of incidence, failure mechanisms, and risk factors. Our 18 month retrospective review across 13 institutions showed acute S2AI screw mechanical failure in 38 of 779 (5%) cases requiring surgical revision within 6 months of index surgery. 49 Of the failure cases, 6 of the 38 (16%) sustained a second acute failure requiring re-revision. Failure mechanisms were rod breakage at lumbosacral junction (7), S2AI screw shaft breakage (9), screw set cap dislodgement/loosening (17), sacral or iliac fracture (6), and screw loosening (9). 49 On univariate analysis, risk factors for failure were: screws less than 8.5 mm in diameter, three-column osteotomy at lumbosacral junction, high magnitude of preoperative pelvic incidence, magnitude of preoperative sagittal deformity (high preoperative T1PA, low preoperative lumbar lordosis), failure to correct deformity (postoperative high PI-LL mismatch, high T1PA). Multivariate analysis showed increased risk for failure with stainless steel rods, male gender, higher T1PA, and manufacturer type. Presence of an L5-S1 interbody cage was protective against failure.
A single-institution study of 50 adult deformity patients reported a 66% rate of S2AI screw loosening at 2 years postoperatively, although 85% of those patients had adequate L5-S1 fusion. 50 Independent risk factors for S2AI loosening were obesity and construct length extending above T5. Another study of 35 adult patients with S2AI screws reported screw loosening in 50% at 2 years postoperatively that was associated with pseudoarthrosis at L5-S1, lack of screw contact with iliac cortical table, and residual significant pelvic incidence-lumbar lordosis mismatch. 51
One series of 67 adult deformity patients with iliac screw fixation demonstrated overall failure rate of 34.3%. 52 11.9% of patients required revision surgery for rod breakage between L4-S1, failure of S1 screws, or prominent iliac screws. However, of note, iliac screw loosening or rod breakage between S1 and iliac screws occurred in 22.4% of patient and were considered minor failure, not treated with operative revision. Risk factors for failure included large pelvic incidence, failure to optimize pelvic incidence-lumbar lordosis mismatch, and revision surgery.
Another single-institution series of 260 adult patients with iliac screws with at least 2-year follow-up reported reoperation rate of 17.7%. 53 7.7% of patients had iliac screw fracture and/or loosening, 4.2% had rod or connector fracture below S1, 8.8% had L5-S1 pseudoarthrosis, 1.5% had S1 screw fracture, and 2.7% had wound infection at site unrelated to iliac screw. The authors’ technique included recessing the iliac screw head deep within the PSIS, and there were no complications related to iliac screw prominence. Iliac screw complications in this series were associated with revision fusions, greater postoperative pelvic tilt indicating potential residual sagittal malalignment, and greater number of levels fused. Multivariate analysis showed that reoperation was associated with longer clinical follow-up.
In additional to mechanical failure, spinopelvic fixation complications can include screw prominence/pain, wound healing complications, and surgical site infection. Multiple clinical studies have compared rates of these complications between S2AI screws and traditional iliac screws. A 2018 meta-analysis of five retrospective cohort studies in 323 adult patients found that compared to iliac screws, S2AI screws had significantly lower rates of revision surgery for mechanical failure, wound complications, surgical site infection, and screw prominence/pain. 54
A 2020 meta-analysis of six studies totaling 477 pediatric and adult patients showed lower risk of postoperative complications of screw prominence, screw loosening, implant breakage, and revision surgery with S2AI screws compared to iliac screws. 55 However, due to the heterogeneity of the patient population, individual examination of the data from each study within the meta-analysis is instructive. One study reported increased implant breakage in a neuromuscular scoliosis population with iliac screws. 56 However, the site of implant breakage localized to the offset connector for the iliac screws, indicating that obviating the need for an offset connector is a primary advantage of alternate iliac fixation trajectories rather than that the S2AI trajectory itself is superior. Another retrospective study in a pediatric neuromuscular population found that increased implant failure for iliac screws compared to S2AI screws was negated if a cross-link was added to the construct. 57 In another single institution’s pediatric population, S2AI screws were associated with increased correction of pelvic obliquity with significantly fewer instances of deep infections, implant prominence, skin breakdown, and anchor migration compared to iliac screws. 58 One single-institution retrospective review of adult deformity patients found significantly lower rates of surgical site infection, wound dehiscence, painful symptomatic screw prominence, and reoperation in S2AI screws vs iliac screws, but no difference in SI joint pain, lumbar pseudoarthrosis, or proximal junctional failure. 59 Another retrospective review of pooled adult and pediatric cohorts found that S2AI screws conferred small but statistically significant absolute risk reductions for acute infections, implant loosening, revision surgery, late pain, and delayed wound issues. 60 A single-institution retrospective cohort study of adult patients found that after controlling for additional risk factors, use of S2AI instead of iliac screws was the only independent predictor for preventing unplanned reoperation for instrumentation failure or wound complications. 61
Neurovascular injury during placement of spinopelvic fixation can occur from iliac cortical violation, either ventrally into the retroperitoneal space with iliac vessel injury or inferiorly into the sciatic notch with gluteal artery injury. Incidence of this is not well-reported but can have catastrophic consequences. Placement of pelvic fixation freehand without radiographic imaging has a been reported with a 5% incidence of cortical breach without complications. 62 However, without supervision by an experienced surgeon, S2AI screws can ventrally breach where crossing the SI joint with potentially significant neurovascular injury. Therefore, utilization of fluoroscopy or navigation for placement of S2AI screws in commonly practiced. 63
Sacroiliac Joint Pain in Pelvic Fixation
The development of sacroiliac (SI) joint pain following lumbosacral fusion is well-described but likely under-reported due to the diagnostic challenges of SI joint-mediated pain. 64 The SI joint is innervated by nociceptive fibers allowing pain sensation. 65 Motion between the sacrum and the ilium occurs across the SI joint in the sagittal plane predominantly as rotation, known as nutation and counternutation, with a lesser amount of movement in the axial and lateral bending planes. 66 The SI joint typically has a small range of motion of less than 5 degrees.
Lumbar fusion significantly increases stress across the SI joint and also significantly increases movement of the SI joint above normal physiological levels, which can be a pain generator.
67
This effect multiplies with increasing levels of fusion. An L5-S1 fusion increases SI joint movement by 52%, while an L4-S1 fusion increases SI joint movement by 168% (Figure 5).
67
The majority of the movement is rotational occurring with flexion/extension loading.
68
Because of the clinical crossover between low back/buttock/leg pain symptoms generated by the sacroiliac joint, lumbar spine, and hip joint, clinical diagnosis relies on a combination of physical exam maneuvers as well as relief response to diagnostic local anesthetic injection of the sacroiliac joint.
69
Radiographic attempts to diagnose sacroiliac joint pathology are unreliable, although the sacroiliac joint has been shown to have chronically increased uptake on SPECT
70
following lumbar fusion as well as progressive degenerative changes on CT scan.
71
Strain and movement across sacroiliac (SI) joint increases with increasing levels of lumbar fusion. Fusion of the SI joint provides minor stress on the hip and lumbosacral facet joints.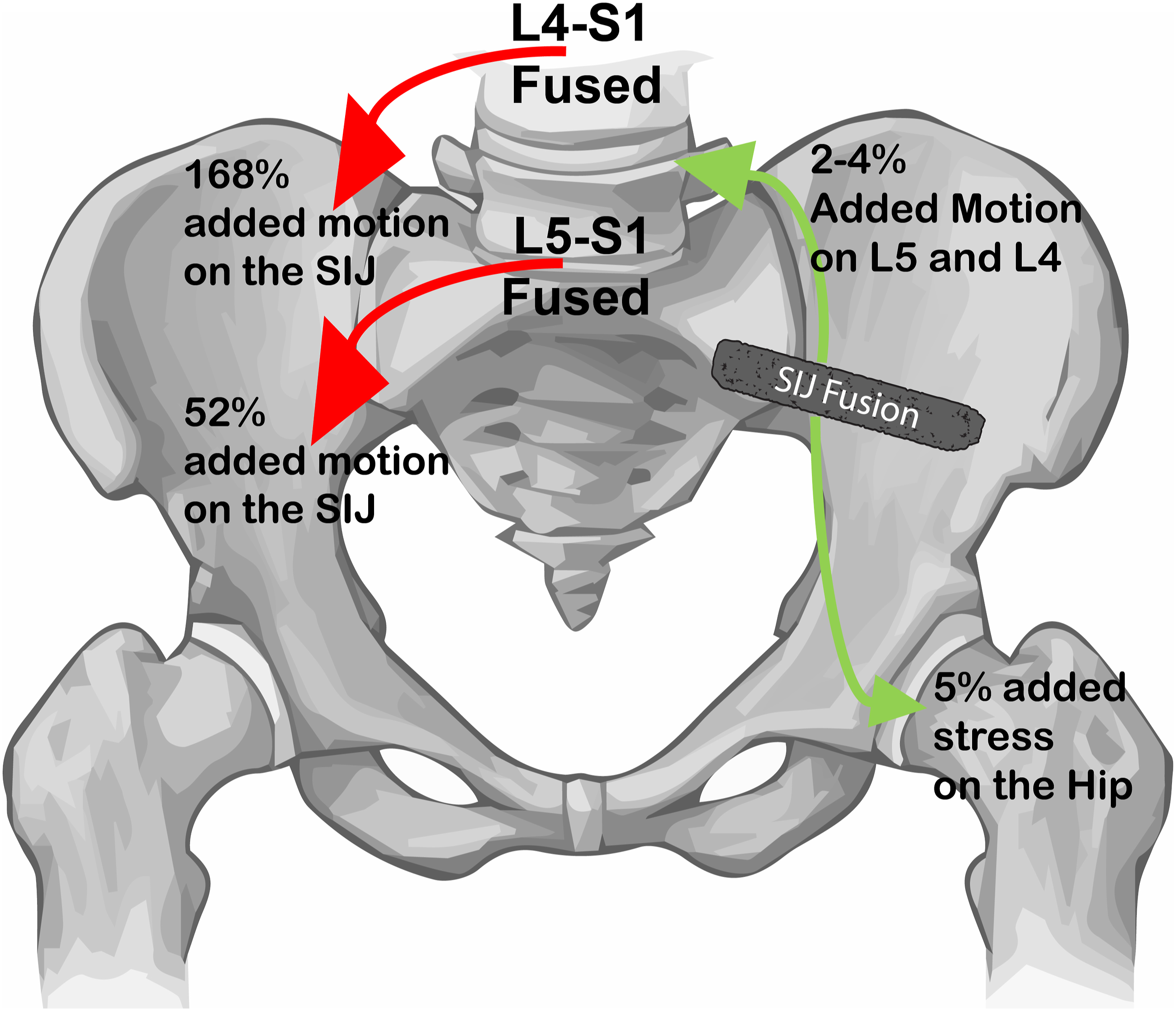
Development of new SI joint pain in lumbar fusions greater than 3 levels has been reported to occur in 14%–22% of patients by two years postoperatively.72-74 Residual sagittal malalignment, manifested as high pelvic tilt or significant PI-LL mismatch, is associated with the development of postoperative SI joint pain after lumbar fusion. 75 One prospective multicenter study of SI joint pain after lumbar fusion surgery found that baseline large pelvic incidence was associated with increased risk of developing SI joint pain even without any significant postoperative PI-LL mismatch. 76 Another study of patients with SI joint pain without any prior spine surgery found an association between higher pelvic incidence and higher sacral slope and SI joint pain, indicating a potential predisposition to SI joint pain. 77
The risk of developing SI joint pain after pelvic fixation with S2AI vs iliac screws is unclear. 78 One small series suggested a decrease in the incidence of SI joint pain in patients with fusion >3 levels receiving S2AI screws, but no patients in this study received alternative forms of iliac fixation for comparison. 79 Another study reported a new incidence of SI joint pain in 3% of patients after S2AI screw placement. 80 One study of 65 adult deformity patients with S2AI screws found a higher rate of postoperative SI joint pain, a shorter time to onset of pain, and poorer response to conservative therapy in patients with partially-threaded S2AI screws as compared to fully-threaded screws. 81 S2AI screws reduce movement of the SI joint by 50% 82 but do not result in fusion of the SI joint. 81
Current Limitations and Future Directions in Pelvic Fixation
SI joint pain occurs frequently and adds significant disability burden after long-construct spinal fusion with pelvic fixation. It is unknown whether fusion of the SI joint with pelvic fixation at the time of spinal deformity surgery can reduce disability. Also unknown is the optimal implant density for pelvic fixation to prevent failure.
The newest frontier in spinopelvic fixation explores the potential utility of concomitant SI joint fusion at the time of long-construct spinal fusion to reduce incidence of symptomatic SI joint arthropathy. SI joint fusion for appropriately-selected candidates is associated with a high fusion rate and significant improvement in patient-reported outcomes.83,84 For patients with symptomatic SI joint arthropathy treated with SI joint fusion, one year outcomes show high fusion rate of 88% and significant decrease in back and leg pain, with about 50% of patients meeting the MCID at one year postoperatively. When placed along with S2AI screws, triangular titanium rods placed across the SI joint further reduce SI joint motion and offload stress from S2AI screws. 82 Further study is required to evaluate the effect of this approach on instrumentation failure or symptomatic SI joint arthropathy after spinal deformity surgery.
While patients with symptomatic SI joint arthropathy prior to spinopelvic fixation are clear candidates to receive concomitant SI joint fusion, it is unclear whether there is a benefit to performing SI joint fusion in patients without symptomatic SI joint arthropathy as a preventative measure. A multicenter randomized controlled has completed data collection regarding this question: Sacroiliac Joint Stabilization in Long Fusion to the Pelvis (SILVIA; clinicaltrials.gov NCT 04062630). Patients undergoing lumbar fusion surgery >3 levels with S2AI pelvic fixation were randomized to receive no SI joint fusion vs receiving open SI joint fusion with a triangular titanium implant placed in a trajectory parallel to S2AI screws via already-existing midline posterior exposure. Primary outcomes at two years were incidence of SI joint pain, change in self-reported SI joint pain, and presence of S2AI screw loosening/breakage/failure/rod fracture on CT scan. Analysis of results is pending.
Another controversial topic is the number of necessary pelvic fixation points. A single-institution retrospective review of 46 adult spinal deformity patients undergoing unilateral iliac screw placement compared to 26 patients undergoing bilateral iliac screw placement found a reoperation rate of about 50% without significant difference between unilateral vs bilateral iliac screws. 85 Utilization of more than two points of pelvic fixation, such as four S2AI screws and one iliac screw, 86 is clinically advantageous in revision strategy to confer additional stability by utilizing more than two rods connecting the spine to the pelvis. In a multicenter review of revision cases for acute spinopelvic fixation failure, none of the patients with revision using at least 4 rods connecting lumbar pedicle screws to pelvic fixation points had another failure, while 16% of the patients initially revised had another failure requiring re-revision if at least 4 rods connecting to pelvic fixation were not used. 49 Additional study is necessary to identify standard criteria for multiple (>2) points of pelvic fixation.
Limitations of the current review include low level of available literature evidence, lack of defined criteria of pelvic fixation failure, and a paucity of understanding regarding effects of pelvic fixation on the sacroiliac joint as potential pain generator.
Conclusion
Incidence of pelvic fixation failure remains high despite modern techniques. Evaluation of pelvic fixation failure incidence with an international, multi-center prospective study of pelvic fixation failure is warranted to better identify patient demographics, radiographic alignment, surgical techniques, and implant characteristics associated with pelvic fixation failure. Future study should also focus on optimizing utilization of pelvic fixation to minimize complications such as sacroiliac joint pain after spinal deformity surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.