
Abstract
Study Design:
Historical cohort study.
Objective:
To evaluate progression in the coronal and sagittal planes in nonsurgical patients with adult spinal deformity (ASD).
Methods:
A retrospective analysis of nonsurgical ASD patients between 2005 and 2017 was performed. Magnitude of the coronal and sagittal planes were compared on the day of presentation and at most recent follow-up. Previous reported prognostic factors for progression in the coronal plane, including the direction of scoliosis, curve magnitude, and the position of the intercrest line (passing through L4 or L5 vertebra), were studied.
Results:
Fifty-eight patients were included with a mean follow-up of 59.8 ± 34.5 months. Progression in the coronal plane was seen in 72% of patients. Mean Cobb angle on the day of presentation and most recent follow-up was 37.2 ± 14.6° and 40.8° ± 16.5°, respectively. No significant differences were found in curve progression in left- versus right-sided scoliosis (3.3 ± 7.1 vs 3.7 ± 5.4, P = .81), Cobb angle <30° versus ≥30° (2.6 ± 5.0 vs 4.3 ± 6.5, P = .30), or when the intercrest line passed through L4 rather than L5 vertebra (3.4 ± 5.0° vs 3.8 ± 7.1°, P = .79). No significant differences were found in the sagittal plane between presentation and most recent follow-up.
Conclusions:
This is the first study that describes progression in the coronal and sagittal planes in nonsurgical patients with ASD. Previous reported prognostic factors were not confirmed as truly relevant. Although progression appears to occur, large variation exists and these results may not be directly applicable to the individual patient.
Introduction
Adult spinal deformity (ASD) comprises a wide range of conditions that result in an abnormality in the alignment, formation, or curvature of the spine. This diverse group of spine deformities seen in adults can result in strong medical, psychological, and social impairments due to severe back pain and neurological symptoms including leg weakness and numbness. 1 Nonsurgical management of ASD has been reported to be insufficient in providing relief of symptoms. Still, a large subset of patients ultimately may reach the point of undergoing reconstructive spinal surgery, a decision that depends on patient-surgeon preferences, functional limitations, neurological symptoms, or curve progression. The prevalence of ASD in the low back pain population has been reported to be 15%, and 68% in asymptomatic adults over the age of 60 years. 2 In light of the ageing population, the prevalence of ASD will continue to increase and will undoubtedly lead to increased surgical interventions for ASD. For this reason, the matter of evaluating the natural history of ASD, is becoming even more urgent.
In ASD, curve progression differs markedly between patients. 3 This unpredictable rate of curve progression subsequently makes it challenging for health care providers to accurately inform patients about their prognosis, the need for follow-up examinations, and the subsequent timing of possible interventions. 4 In the current literature, there are a limited number of studies that evaluated curve progression in ASD. These studies found several prognostic factors that may influence the degree of curve progression in the coronal plane, including the direction of scoliosis, curve magnitude, and the position of the intercrest line (passing through L4 or L5 vertebra). 5 -10 However, best to our knowledge, no studies have evaluated curve progression in the sagittal plane, albeit that restoration of sagittal spinopelvic malalignment has become a focal target in ASD when planning surgical correction in providing relief of symptoms and improving health-related quality of life. 11
The primary aim of this study was to evaluate the natural history of ASD, hence curve progression in the coronal and sagittal planes in a cohort of nonsurgical patients. This may provide more insight in the natural history of progression in ASD, including its complex pathophysiology, and may aid health care providers to inform patients about their prognosis and need for clinical follow-up examination.
Materials and Methods
Study Design and Patient Population
This is a single-center historical cohort of ASD patients who consulted the outpatient clinic between 2005 and 2017. Patients had complete series of standing anteroposterior (AP) and lateral (L) full-length spine radiographs. All full-spine radiographs were retrieved in order to adequately evaluate curve progression in the coronal and sagittal planes. Inclusion criteria were the following: (1) age ≥40 years; (2) diagnosed with ASD (de novo degenerative lumbar scoliosis [DNDLS] and adult idiopathic scoliosis [AIS]) 12 ; (3) patients that had undergone conservative treatments, which included (but was not limited to) exercise therapy if possible, steroid injections, and/or pharmacological treatments; (4) no history of spine surgery; and (5) a follow-up ≥2 years between initial and final radiographs. Patients with a follow-up of less than 2 years and a history of juvenile or neuromuscular spinal abnormalities, metabolic spinal pathology, or surgical treatment were excluded. The hospital’s Institutional Review Board approved the study protocol (SMK713).
Data Collection
Demographic data including age, follow-up time, and gender were retrieved from electronical medical records. Radiographic measures were obtained using a dedicated spine measurement software (Surgimap, Nemaris Inc) and included the following: Cobb angle (CA), position of the intercrest line through L4 or L5, direction of scoliosis, thoracic kyphosis (TK), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), sacral slope (SS), and pelvic incidence minus lumbar lordosis (PI − LL). Finally, recently proposed T1-pelvic angle (TPA; T1 sagittal tilt + pelvic tilt) 13 was measured, which accounts for pelvis motion and is least affected by the patient’s position during radiographic examination. All radiographic measures were independently measured by 2 authors (interrater reliability: intra-class correlation [ICC] = 0.96).
Curve Progression in the Coronal Plane
In ASD patients with complete standing AP full-length spine radiographs at initial presentation and final follow-up, curve progression was evaluated in the coronal plane. Previous reported prognostic factors for curve progression were evaluated (direction of scoliosis, curve magnitude [Cobb angle <30° or ≥30°], and position of the intercrest line). 3 Finally, patients were stratified into 3 groups according to the amount of curve progression in Cobb angle: no progression (group 1), 0° to 1° progression per year (group 2), and ≥1° progression per year (group 3).
Curve Progression in the Sagittal Plane
In ASD patients with complete L full-length spine radiographs, curve progression in sagittal spinopelvic parameters were evaluated between initial presentation and final follow-up.
Statistical Analysis
Data collection was tested for normal distribution (Shapiro-Wilk test). Descriptive analysis was used to calculate demographic and radiology data. Baseline demographic and radiographic values were compared between both groups using independent Student’s t test. Frequency analysis of categorical variables (direction of scoliosis, curve magnitude, and position of the intercrest line) was performed using a Fisher exact test. Finally, patients were stratified according to the amount of curve progression in Cobb angle in 3 groups: no progression (group 1), >0° to 1° progression per year (group 2), and ≥1° progression per year (group 3). Mean values of demographic and radiographic parameters were compared between groups using a one-way ANOVA test for continuous variables and a χ2 test for categorical variables. All statistical tests were performed with SPSS 25.0 IBM. Statistical significance was set at P < .05.
Results
Study Population
A total of 5407 complete standing full-length spine radiographs of 3573 patients were retrieved between 2005 and 2017. Based on the study criteria, a total of 58 patients were included: 31 (53%) patients underwent AP full-length spine radiograph, whereas 27 (47%) patients underwent AP and L full-length spine radiographs at baseline and final follow-up (Figure 1).
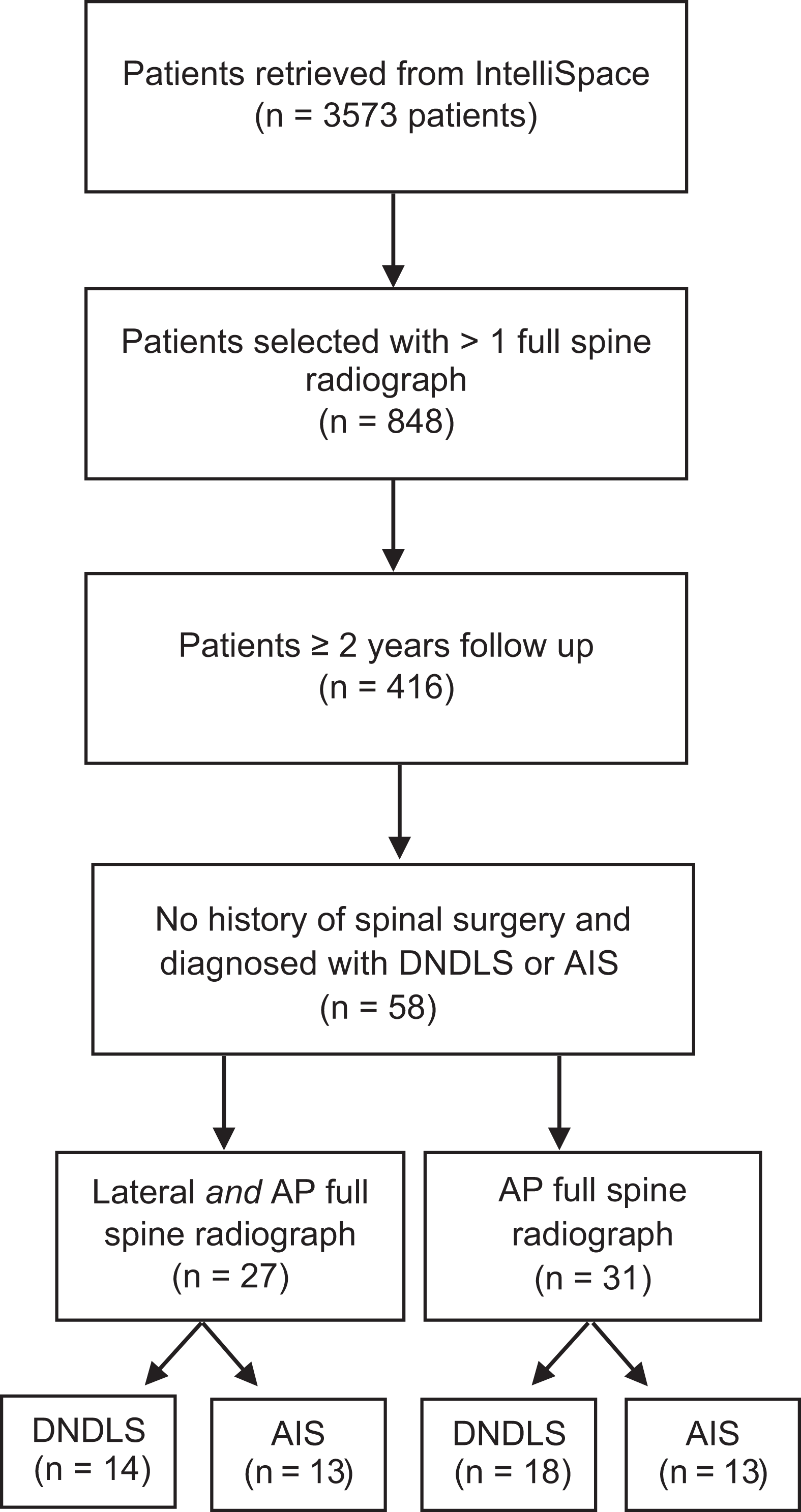
Patient selection.
In this group of 58 patients, comprising 31 (53%) DNDLS and 27 (47%) AIS patients, the mean patient age was 56.0 ± 10.1 years with a mean follow-up of 59.8 ± 34.5 months (Table 1). A significant difference in age was shown between patients diagnosed with DNDLS and AIS (P = .03; 58.9 ± 10.6 vs 53.3 ± 8.7, respectively).
Demographics
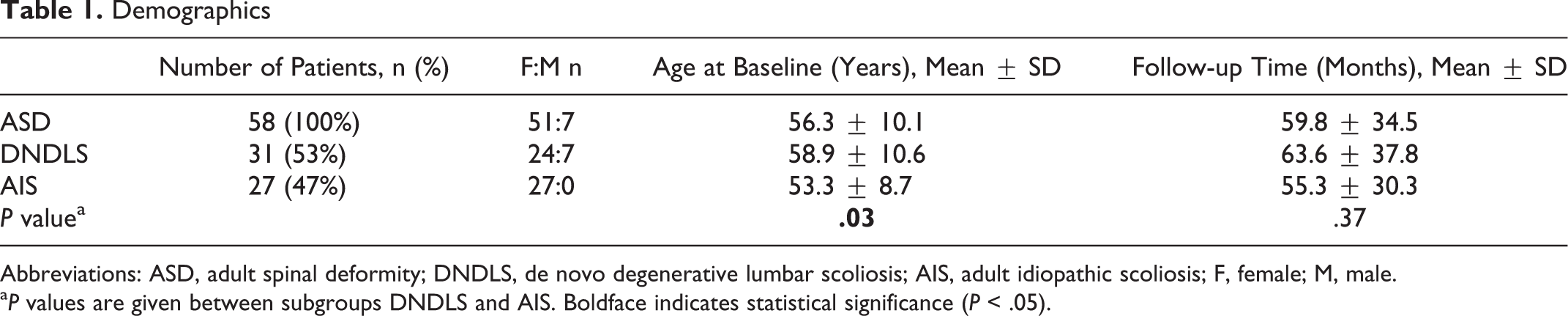
Abbreviations: ASD, adult spinal deformity; DNDLS, de novo degenerative lumbar scoliosis; AIS, adult idiopathic scoliosis; F, female; M, male.
a P values are given between subgroups DNDLS and AIS. Boldface indicates statistical significance (P < .05).
Curve Progression in the Coronal Plane
ASD patients demonstrated a mean coronal curve progression of 0.83 ± 1.1° per year, concomitant to an increase of 3.6° in Cobb angle between initial presentation and final follow-up (Table 2). No significant difference was shown in mean coronal curve progression per year between patients subdiagnosed with DNDLS and AIS (P = .07; 0.98 ± 1.1 vs 0.37 ± 1.4, respectively). Figure 2 present the gradual curve progression in the coronal plane of both subgroups.
Progression in the Coronal Plane After a Mean Follow-up of 5 Years.
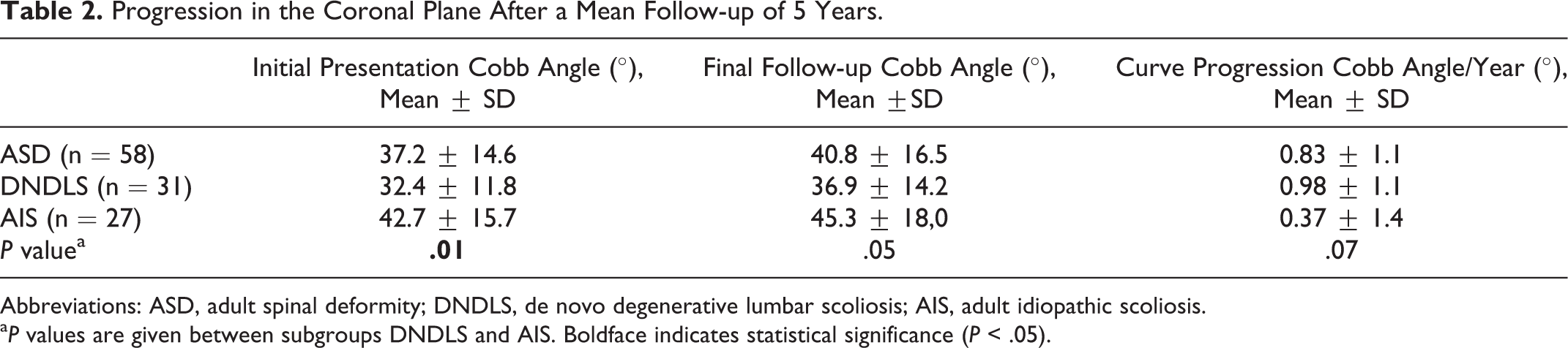
Abbreviations: ASD, adult spinal deformity; DNDLS, de novo degenerative lumbar scoliosis; AIS, adult idiopathic scoliosis.
a P values are given between subgroups DNDLS and AIS. Boldface indicates statistical significance (P < .05).
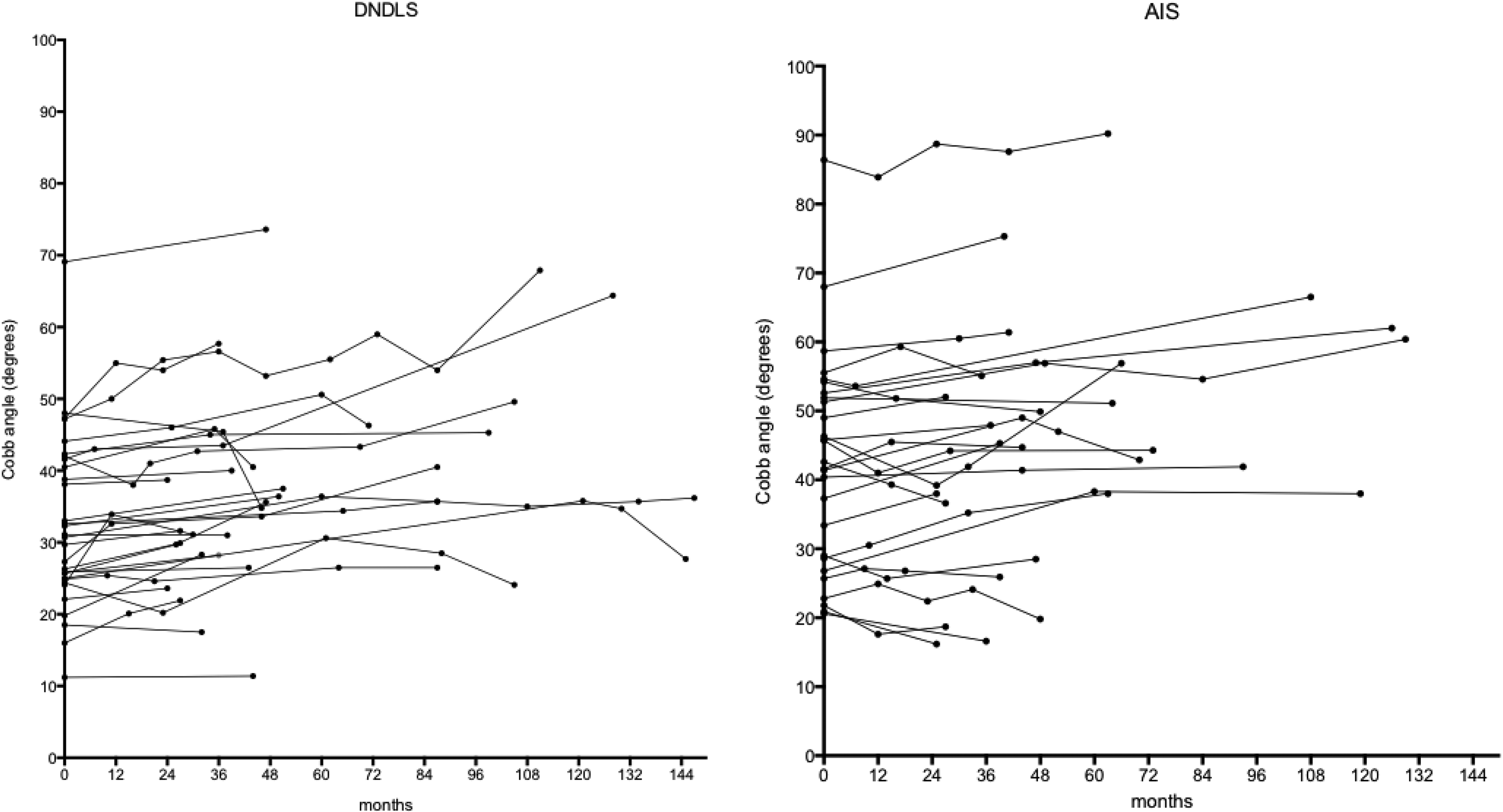
Curve progression in Cobb angle in de novo degenerative lumbar scoliosis (DNDLS; n = 31) and adult idiopathic scoliosis (AIS; n = 27) patients over a mean follow-up of 5 years.
Previous Reported Prognostic Factors for Curve Progression in the Coronal Plane
No significant differences were found in mean curve progression per year with regard to direction of scoliosis, curve magnitude, and position of the intercrest line (Table 3).
Previous Reported Prognostic Factors for Curve Progression in the Coronal Plane in ASD (n = 58)a.
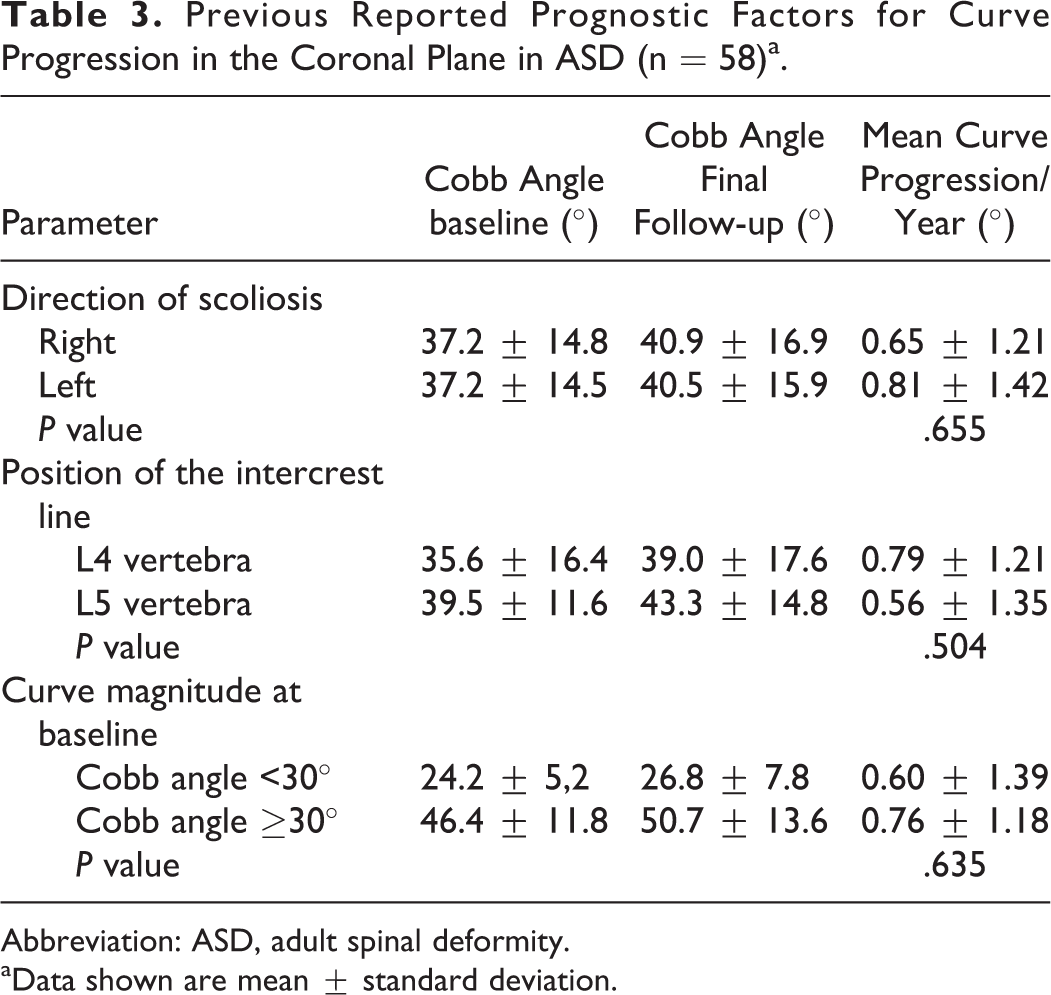
Abbreviation: ASD, adult spinal deformity.
aData shown are mean ± standard deviation.
Group Stratification According to Severity of Curve Progression
Progression in the coronal plane was seen in 42/58 (72%) of patients with ASD (Table 4). Stratification into 3 groups according to the amount of curve progression demonstrated no significant difference in age, follow-up time, direction of scoliosis, position of the intercrest line, and curve magnitude at baseline (P < .05).
Group Stratification According to Severity of Curve Progression in ASD (n = 58).
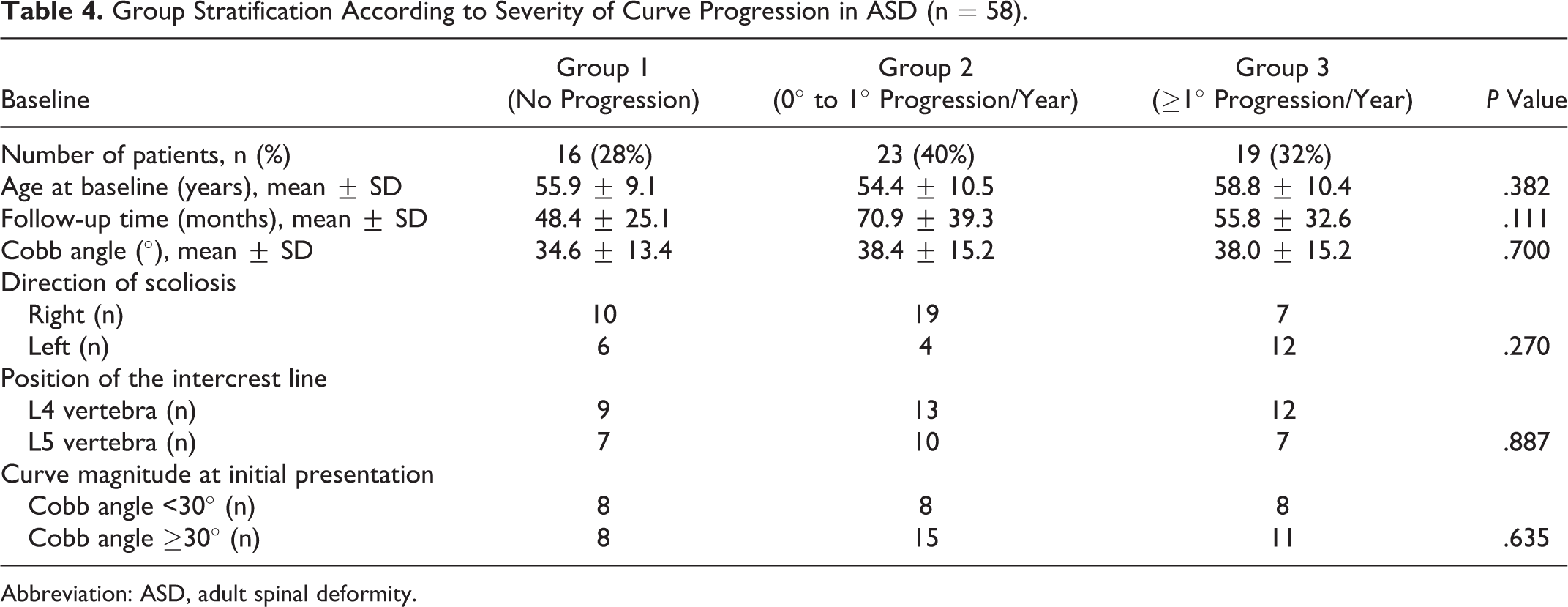
Abbreviation: ASD, adult spinal deformity.
Curve progression in the Sagittal Plane
In the cohort of 58 ASD patients, a total of 27 were identified with complete standing AP and L full-length spine radiographs, comprising 14 (52%) DNDLS and 13 (48%) AIS patients. The mean patient age was 56.7 ± 10.6 years with a mean follow-up of 58.2 ± 33.7 months. No significant differences were found with regard to sagittal radiographic parameters at baseline between DNDLS and AIS (Table 5). No significant differences were found with regard to progression in the sagittal spinopelvic parameters between initial presentation and final follow-up (Table 6).
Demographic Parameters of ASD Patients Who Underwent Complete AP and L Full-Length Spine Radiographs (n = 27).
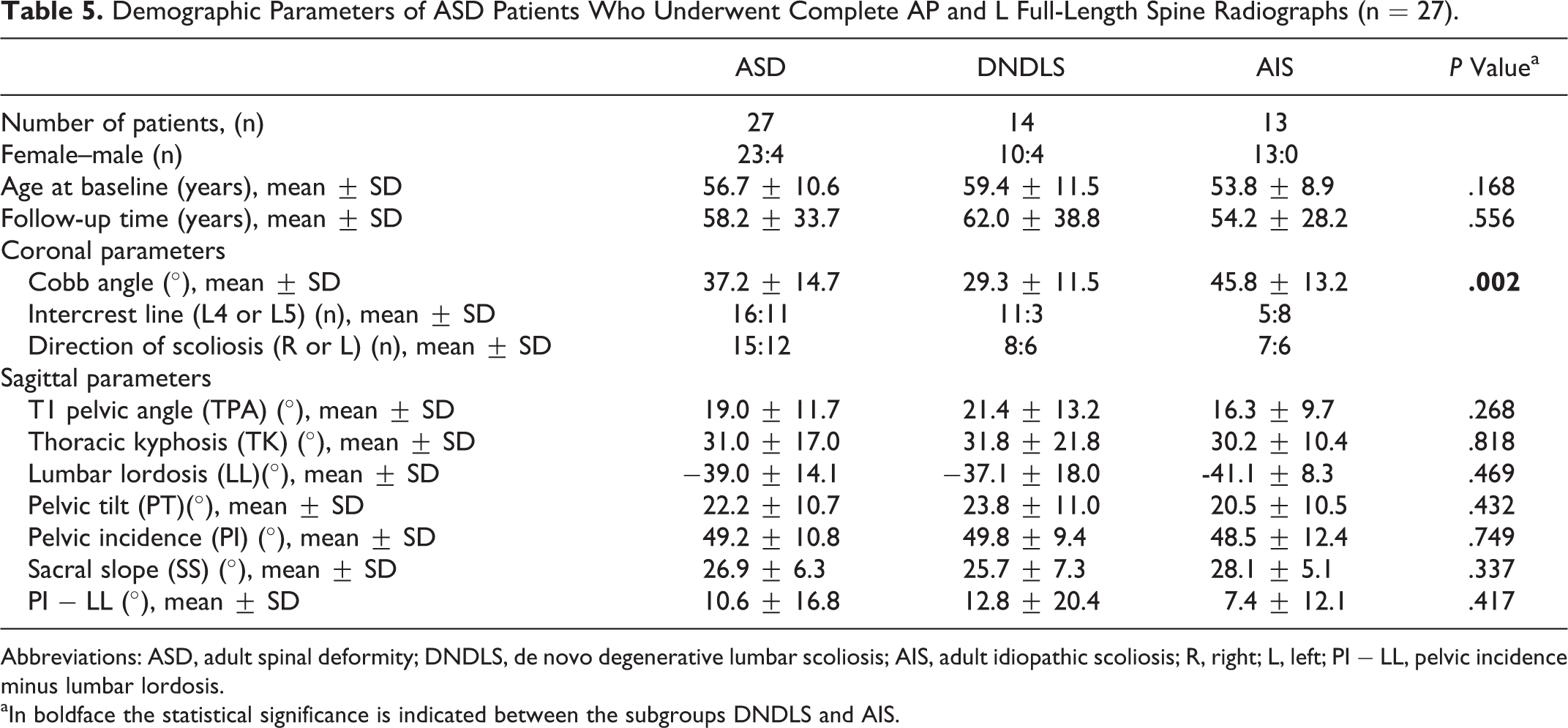
Abbreviations: ASD, adult spinal deformity; DNDLS, de novo degenerative lumbar scoliosis; AIS, adult idiopathic scoliosis; R, right; L, left; PI − LL, pelvic incidence minus lumbar lordosis.
aIn boldface the statistical significance is indicated between the subgroups DNDLS and AIS.
Curve Progression in the Sagittal Plane in ASD Patients Between Initial Presentation and Final Follow-up (n = 27).

Abbreviation: PI − LL, pelvic incidence minus lumbar lordosis.
Discussion
This study provides the first long-term evaluation of progression in the coronal and sagittal planes in a cohort of nonsurgical ASD patients. Although nonsignificant, the results of the present study demonstrate that progression in the coronal and sagittal planes occurs over a mean follow-up of 5 years. Progression in the coronal plane was seen in 72% of patients with ASD, and previous reported radiographic risk factors for curve progression were not confirmed as truly relevant (direction of scoliosis, curve magnitude, and position of the intercrest line).
The findings of the present study seem contradictory compared with previous studies that have suggested that there is a strong relationship between the direction of scoliosis and the likelihood of curve progression. In a retrospective analyzed case series, Chin et al 7 described the natural course of curve progression in 24 ASD patients with a mean follow-up of 4.85 years. Chin and colleagues found a significant difference in curve progression between the direction of scoliosis: patients with left-sided scoliosis progressed 3° per year, whereas patients with a right-sided scoliosis 1° per year. 7 These results differ from the present study in which we found that the direction of scoliosis should not be considered as a relevant risk factor for curve progression (Tables 3 and 4). These contradicting findings may be explained by the difference between the 2 groups. The study by Chin and colleagues 7 included patients with curves of no more than 30°, while the present study included all ASD patients with curves of more than 10°. It is possible that the direction of scoliosis may be a risk factor for rapid curve progression in the early phase of ASD and not in the later phase. Additionally, in the current study, we were not unable to demonstrate that curve magnitude at initial presentation should be considered a risk factor for curve progression (Table 3 and 4). This is contrary to previous studies. 6,10 In a retrospective study, Sapkas et al 6 evaluated the risk of curve progression in 162 ASD patients (all women) with a mean follow-up of 8 years. Sapkas and colleagues reported that patients with a Cobb angle ≥30° were more likely to progress, while in the present study we found no significant difference in mean curve progression per year between patients with a Cobb angle <30° and ≥30° (Table 3). The relatively short follow-up time of the present study, including the nonlinear tendency of curve progression in particularly women, 7 might account for this discrepancy.
We found that adult patients with AIS appear to demonstrate less progression than DNDLS (Table 2). We postulate that a possible explanation for this variation is caused by the difference in etiology. Adult idiopathic (nondegenerative) scoliosis is a pediatric deformity. Over time, the pediatric curve may progress, leading to a compensatory curve, or in some instances it may be affected by secondary degeneration as patients get older. 14 This is very different from DNDLS, which is caused by primary mono- and multilevel disc degeneration located in the lumbar region, and typically develops after the sixth decade of life. 12 As such, adult patients with DNDLS are unlikely to suffer from the same distribution, localization, and intensity of degenerated areas as patients with AIS, as argued before. 12,15 Moreover, in a landmark study by Weinstein et al 16 (including the Iowa series 17 -19 ), it was demonstrated that these entities have their own natural histories based on curve type and magnitude, including associated problems that may significantly affect daily functioning. It is, therefore, most likely that a distinction between subtypes of ASD should be made in determining the clinical course.
Previous multicenter studies demonstrated that in ASD, sagittal spinopelvic malalignment is associated with pain and poor health-related quality of life scores. 11 As a result, Schwab et al 20 developed a classification system for ASD based on the most clinically relevant sagittal spinopelvic modifiers that are associated with pain and health-related quality of life scores: sagittal vertical axis (SVA), PT, and PI − LL mismatch. Consequently, it is of paramount importance to evaluate progression in these sagittal spinopelvic parameters. Notable, the present study did not include the SVA as measurement to evaluate progression in the sagittal plane. Previous studies have demonstrated that the SVA is dependent of positional changes during radiographic examination, 21,22 and was therefore deemed not appropriate to evaluate progression in the sagittal plane. Consequently, we included the recently proposed T1-pelvic angle to evaluate progression in the sagittal plane, which accounts for pelvis motion and is least affected by the patient’s position during radiographic examination. 13 Although we did not find any significant changes over a mean follow-up of 5 years, our results seem to indicate that PI remains relatively stable (+1.8°) and that there is a nonsignificant tendency toward loss of LL (−7.4°; Table 6). As a result, we observed a concomitant nonsignificant increase in PI − LL mismatch (+4.9°). Notable, PI − LL mismatch has become a focal target when planning surgical correction in ASD in order to achieve global sagittal balance and improve health-related quality of life scores. Lafage et al 23 demonstrated that ideal sagittal spinopelvic values varies with age, and that elderly ASD patients may tolerate PI − LL mismatch (ie, sagittal malalignment) better than relatively young patients, which could be related to the natural human aging process. As humans age, a loss of lumbar lordosis occurs that induces an anterior displacement of the trunk, a so-called “stooped posture.” 24 Although our findings seem to indicate that patients with ASD show a tendency toward an increase in sagittal malalignment over time, it is not clear whether this is part of a normal aging process or not.
Limitations
First, although the Cobb angle is considered the gold standard in evaluating the coronal plane, a measurement error of 3° to 5° is known. 25 This subsequently increases the chance of obtaining a nonsignificant result. 26 Second, selection bias might have been introduced. Nonsurgically treated ASD patients were included with a minimal follow-up of 2 years. As such, we may have excluded patients with more rapid curve progression who underwent surgical management. Subsequently, this may not accurately reflect the rate of curve progression in clinical practice and these results may not be directly applicable to the individual patient. Third, there is an absence of data related to nonsurgical management (eg, physiotherapy, bracing) between initial presentation and final follow-up that patients may have tried. Fourth, there is a small sample size. A larger number of patients could render the trend of an association between prognostic factors with progression more statistically significant. Finally, clinical factors such as osteoporosis, cigarette smoking, and body mass index were not reported. It is possible that these clinical factors may influence the degree of progression in ASD and future studies are warranted. To date, patient data (including clinical and radiographic data) on the surgical management of ASD are collected in multiple multicenter, regional, and national spine registries worldwide. 27 Unfortunately, there is a lack of comprehensive data on the nonoperative course of ASD. For this reason, we recommend that nonsurgically treated ASD patients should be included in current spine registries and as part of future long-term follow-up studies. This will provide more insight in the manifestation and natural history of ASD and provide the opportunity to evaluate prognostic (clinical and radiographic) factors associated with the variance found in curve progression.
Conclusion
This is the first study that evaluates curve progression in both the coronal and sagittal planes in a nonsurgical cohort of patients with ASD. Our results appear to indicate that curve progression occurs over a mean follow-up of 5 years in both the coronal and sagittal planes. In contrast to previous studies, the direction of scoliosis, curve magnitude, and position of the intercrest line were found not to be risk factors for coronal curve progression. On average adult patients with AIS appear to demonstrates less progression than DNDLS. Large variations exist, and individual guidance is very difficult to give, even with the current data. Until then perhaps the best advice is to perform a new radiograph after 3 to 5 years to be able to identify those patients whose curve progresses, in order to provide patients with personalized advice. Moreover, sagittal malalignment in ASD appears to increase with age; however, we do not know whether this is part of a normal aging process or not.
Footnotes
Author Contributions
The study was designed by SSAF, MvH and MS. Statistical analysis was done by SSAF and NtH. All authors were involved in writing the manuscript; SSAF and NtH wrote the initial draft and all authors critically revised and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.