
Abstract
Study Design
A prospective study.
Objectives
This study aims to explore the correlation between interleukin (IL)- 6 levels in intervertebral disc (IVD) tissue and clinical outcomes in patients undergoing lumbar surgery for lumbar degenerative disease (LDD).
Methods
This prospective study analyzed 32 patients (22 men and 10 women, average age 69.6 years) who underwent lateral lumbar interbody fusion (LLIF). IL-6 gene expression in IVD tissues collected during surgery was measured and correlated with pre- and postoperative clinical outcomes, including pain intensity assessed via Numeric Rating Scales (NRS) and quality of life (QOL) evaluated through the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ).
Results
IL-6 levels showed statistical correlations with postoperative intensity of low back pain (LBP) and several JOABPEQ domains. Patients with higher expression of IL-6 levels experienced more severe postoperative LBP and lower scores in lumbar function, walking ability, social life function, and mental health. The effectiveness rate of JOABPEQ scores was exceptionally high for low back pain (.548), walking ability (.677), and social functioning (.563), demonstrating the effectiveness of LLIF. The average operation time was 105.6 minutes, and the estimated blood loss was 85.6 mL.
Conclusions
The study underscores IL-6 as a potential biomarker for predicting surgical outcomes in LDD. High IL-6 levels correlate with worse postoperative LBP and lower QOL scores. Integrating molecular markers like IL-6 with patient-reported outcomes could provide a more comprehensive approach to postoperative care in spinal disorders, aiming to improve the overall QOL for LDD patients undergoing LLIF surgery.
Keywords
Introduction
Low back pain (LBP) is a global health concern, significantly impacting individual well-being, work performance, social roles, and healthcare costs.1-3 The primary etiology of LBP is intervertebral disc (IVD) degeneration, which compromises spinal stability and contributes to various spinal disorders. Although spinal fusion surgery, particularly in cases of spinal degenerative diseases with instability, is a common treatment, it often results in low patient satisfaction and sometimes necessitates multiple surgeries. Recent research has increasingly acknowledged the molecular link between the degradation of the extracellular matrix in IVD cells, influenced by inflammatory cytokines, and the development of LBP.4,5 It has been demonstrated that, compared to pain-free IVD tissue, there is an increased expression of cytokines, particularly interleukin (IL)- 6 and tumor necrosis factor (TNF)-α, in painful IVD tissue, emphasizing the potential role of cytokines in the pathophysiology of LBP.6,7
Our prior research explored this relationship further, uncovering a significant correlation between elevated IL-6 levels in IVD tissues and increased pain severity. 8 This discovery is pivotal for understanding the impact of preoperative cytokine levels on postoperative LBP, especially in spinal fusion surgeries. Additionally, the utility of minimally invasive spine surgeries, such as lateral lumbar interbody fusion (LLIF) for indirect decompression,9-14 is recognized, along with the need for patient-reported outcome measures (PROMs) postoperative evaluation methods.
To assess the disability of patients with lumbar degenerative diseases (LDD), accessible and cost-effective tools that address both physical and psychometric aspects, such as questionnaires, are necessary. 15 While tools like the Roland-Morris Disability Questionnaire (RMDQ) 16 and the Oswestry Disability Index (ODI) 17 have their applications, their limitations have paved the way for promising alternatives like the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ).18,19 JOABPEQ’s comprehensive domains cover back pain, lumbar function, walking ability, social life function, and mental health, offering a holistic understanding of patient health with high reliability.
In light of this background, our study aims to bridge the existing knowledge gap by correlating the molecular mechanisms of LBP with clinical outcomes following spine surgery. Understanding the interaction between cytokine levels in IVD tissue and patient-reported outcomes, post-surgery could revolutionize postoperative treatment approaches and optimize care for patients with LDD. Therefore, our study aims to evaluate the gene expression of IL-6 in IVD tissue collected during LLIF and its correlation with postoperative clinical outcomes using tools like JOABPEQ and pain scores.
Methods
IRB Statement
This study was conducted following the guidelines of the Helsinki Declaration 20 and received approval from the Ethics Committee and the Profit Reciprocity Committee of the Tokai University School of Medicine (Approval Number: 20R-263). All participants submitted written informed consent. The consent form detailed that during surgery, degenerated or herniated IVD tissue would be removed, and a part of this tissue might be requested for donation. This research investigated the correlation between IL-6 gene expression in the IVD during surgery and pain intensity, as well as JOABPEQ scores, pre- and post-LLIF surgery.
Included Patients
The research participants were all over 20 years old and had received conservative therapy-resistant treatment for at least 3 months before undergoing lumbar surgery to treat LDD. All patients were diagnosed based on a detailed medical history, neurological and radiological examinations, myelography results, and post-myelography computed tomography (CT) scans and/or magnetic resonance imaging (MRI). Before the surgery, the authors explained to the patients the use of the IVD samples collected during the surgery, and participants read and consented to the sample donation. The exclusion criteria were severe mental illness, severe disability or paralysis causing difficulty in standing or moving, a previous (within 5 years) or current cancer diagnosis, current suspected infection, or the presence of symptoms that the principal investigator suspected might be an infection. These were contraindications for inclusion in this study.
Demographic and clinical data were collected after the commencement of the study. From August 2019 to May 2021, IVD tissue was collected from patients diagnosed with lumbar degenerative disc disease with accompanying LBP, leg pain (LP), and/or leg numbness (LN) who consented to specimen collection. IVD tissue from multi-level discs was collected into a single tube for genetic testing. The study investigated the correlation between the expression of the IL-6 gene in the IVD tissues and the severity of pain and JOABPEQ scores before and 1 year after surgery.
Ultimately, we analyzed 32 patients (22 men and 10 women, average age 69.6 ± 6.8 years) who underwent indirect surgery through LLIF with percutaneous pedicle screw and were available for evaluation of pain and JOABPEQ scores 1-year post-operation. We also evaluated lumbar spine bone mineral density (BMD) and T-score using a dual-energy X-ray absorptiometry (DXA) scan (Horizon W ® DXA system, Hologic, Inc). Our criteria for fusion surgery were a sagittal plane translation exceeding 3 mm, a segmental angle formation angle exceeding 10° in dynamic X-ray evaluation, or a posterior expansion of the intervertebral disc space exceeding 5° in flexion X-ray images.
Surgical Technique
We executed the basic procedure for indirect decompression through LLIF and posterior fixation based on the surgical technique described by Ozgur et al., 14 as outlined in our previous papers.21-26 The approach for LLIF surgery was performed using either extreme lateral interbody fusion (XLIF) (NuVasive, San Diego, California) or oblique lateral interbody fusion (OLIF) (Medtronic, Minneapolis, Minnesota). There was no specific criterion for choosing between XLIF and OLIF, and the choice of approach was left to the surgeon’s discretion. For all patients, we implemented LLIF using a single-incision mini-open direct visualization approach. Briefly, this involved placing the patient in a lateral position and making a skin incision towards the target intervertebral disc. We then approached the disc, conducted a discectomy, and performed a cage trial and insertion. In all LLIF segments, we added percutaneous pedicle screw fixation, utilizing either intraoperative fluoroscopy or an intraoperative CT navigation system.
Lumbar MRI
All patients received a standard lumbar MRI scan prior to surgery. The MRI, covering the lumbar region from L1–L2 to L5–S1, was conducted using T2-weighted sequences, employing either a 1.5- or 3.0-Tesla imaging system (Ingenia or Achieva models, Philips Medical Systems, located in Best, The Netherlands). The severity of IVD degeneration was assessed using the midsagittal T2-weighted images, adhering to the criteria of the Pfirrmann classification system and its modified version. 27 Moreover, the modified Pfirrmann grading, a method based on MRI characteristics, is widely recognized for its noninvasive approach to determining the extent of IVD degeneration. 28
We also performed MRI to determine the midsagittal canal diameter (CD) and axial central canal area (CCA) of the thecal sac before and within 2 weeks after surgery.
RNA Isolation and Quantitative Reverse Transcription-Polymerase Chain Reaction
Total cellular RNA from the IVD tissues was extracted using the Trizol technique. The tissues were initially preserved in RNALater (Ambion, Foster City, CA) and kept at −80°C until needed. The RNALater was discarded for RNA extraction, and the tissues were immediately frozen in liquid nitrogen before being immersed in Trizol (Invitrogen, Carlsbad, CA). Solid tissues were then homogenized using an Omni Tissue Homogenizer (Omni International, Kennesaw, GA). The RNA was precipitated using 70% ethanol and further purified with the RNeasy Mini Kit (Qiagen, Valencia, CA), following the provided instructions. The reverse transcription of RNA into cDNA was conducted using the High-Capacity cDNA Reverse Transcription Kit (Thermo Fisher Scientific, Waltham, MA), with a reaction mixture containing 100 ng of total RNA and a volume of 20 μL. The resultant cDNA was diluted 10 times using nuclease-free water. Quantitative PCR (qPCR) was then performed to measure the expression levels of specific genes, utilizing a SYBR Green Real-Time PCR kit (Thermo Fisher Scientific) on the LightCycler® 480 System (Roche Applied Science, Mannheim). The qPCR reactions were done in triplicates in a 96-well plate, with each well containing 10 μL using ABI 2x SYBR Green Master Mix. The PCR conditions were an initial 20 s denaturation at 95°C, followed by 40 cycles of 3 s at 95°C and 30 s at 60°C. GAPDH was used as the normalization control. The cycle threshold (Ct) values were calculated by subtracting the Ct value of GAPDH from that of the target gene. Primers for IL-6 and GAPDH were obtained from Sangon Biotech (Shanghai, China). Primer sequences that were employed for IL-6 were 5′- GATGAGTACAAAAGTCCTGATCCA -3′ for forward sequence and 5′- CTGCAGCCACTGGTTCTGT -3′ for reverse sequence. The sequences for GAPDH were 5′- TGGGTGTGAACCATGAGAAGTA -3′ for forward primer sequence and 5′- GAGTCCTTCCACGATACCAAAG -3′ for reverse primer sequence.
Pain Intensity
Three Numeric Rating Scales (NRS) scores were used to assess pain severity: LBP, LP, and LN, respectively. For assessing LBP, LP, and LN, 22 NRS evaluations were conducted, ranging from 0, indicating no pain, to 10, representing the most severe pain conceivable. These assessments were carried out both prior to and 1 year following surgery. The symbol Δ was used to denote the difference in pain levels, comparing postoperative measurements with those taken preoperatively.
JOABPEQ
The JOABPEQ is a patient-centered tool for assessing the quality of life (QOL) in individuals with lower back disorders. It generates 5 functional scores (about low back pain, lumbar function, walking ability, social life, and mental health) based on responses to 25 questions. These scores can be calculated either through the formulas provided or by inputting the data into an Excel file available on the Japanese Orthopaedic Association’s website (https://www.jssr.gr.jp/jssr_web/html/index.html). We conducted assessments using the JOABPEQ both before surgery and 1 year after. The evaluation of its effectiveness was based on 2 parameters: the effectiveness rate and the gained score. The effectiveness rate was determined either by an increase of 20 or more points in a patient’s score from pre-surgery to post-surgery or by achieving a post-treatment score of 90 or above. In addition, cases with a score of 100 points preoperatively and a score of 100 points postoperatively were deleted. The effectiveness rate was computed as the proportion of patients who met these criteria out of the total number examined. The gained score was determined by comparing pre-and post-surgical scores among the patients.
Statistical Analysis
We performed all statistical analyses using IBM SPSS Statistics (version 23.0, IBM Corp., Armonk, NY), and reported all values as mean ± standard deviation. To verify the normal distribution of our data, we adopted the Shapiro-Wilk test. Specifically, we used Student's t-test to analyze normally distributed data, while applying the Mann-Whitney U test to non-normally distributed data. Additionally, to identify significant correlations, we utilized either Pearson’s or Spearman’s product-moment correlation analysis. We set a threshold of 5% for type 1 error in all statistical tests, considering P values less than .05 as indicative of statistical significance.
Results
Characteristics of the Subjects in the Present Study.
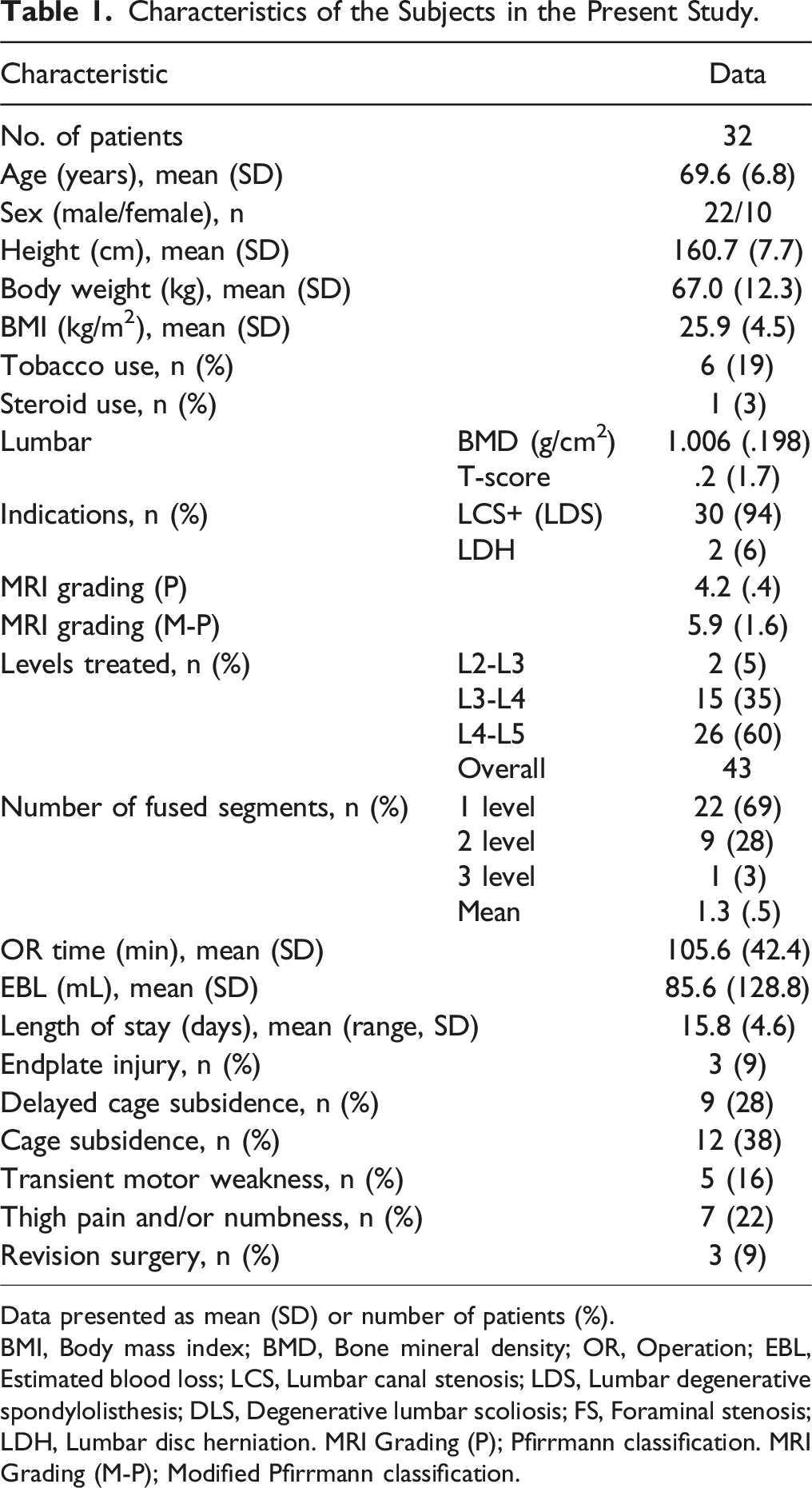
Data presented as mean (SD) or number of patients (%).
BMI, Body mass index; BMD, Bone mineral density; OR, Operation; EBL, Estimated blood loss; LCS, Lumbar canal stenosis; LDS, Lumbar degenerative spondylolisthesis; DLS, Degenerative lumbar scoliosis; FS, Foraminal stenosis; LDH, Lumbar disc herniation. MRI Grading (P); Pfirrmann classification. MRI Grading (M-P); Modified Pfirrmann classification.
Gene Expression of Chemokine and Inflammatory Cytokine in IVD Tissues by RT-PCR.
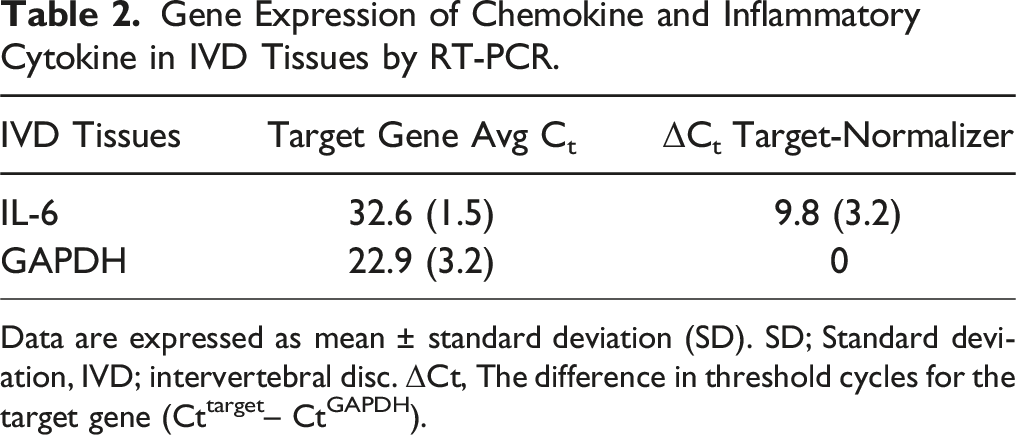
Data are expressed as mean ± standard deviation (SD). SD; Standard deviation, IVD; intervertebral disc. ΔCt, The difference in threshold cycles for the target gene (Cttarget– CtGAPDH).
Pain Intensity for Each Group.
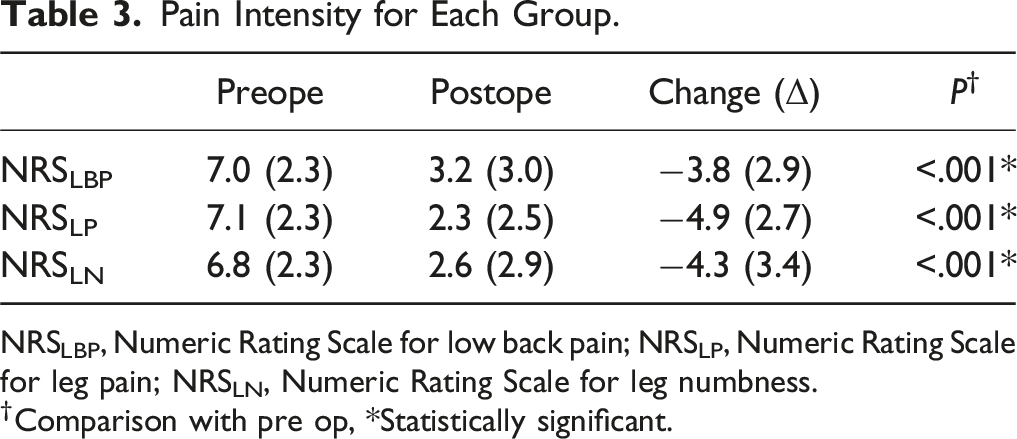
NRSLBP, Numeric Rating Scale for low back pain; NRSLP, Numeric Rating Scale for leg pain; NRSLN, Numeric Rating Scale for leg numbness.
†Comparison with pre op, *Statistically significant.
Two-Group Comparison Pre and Postoperative JOABPEQ.
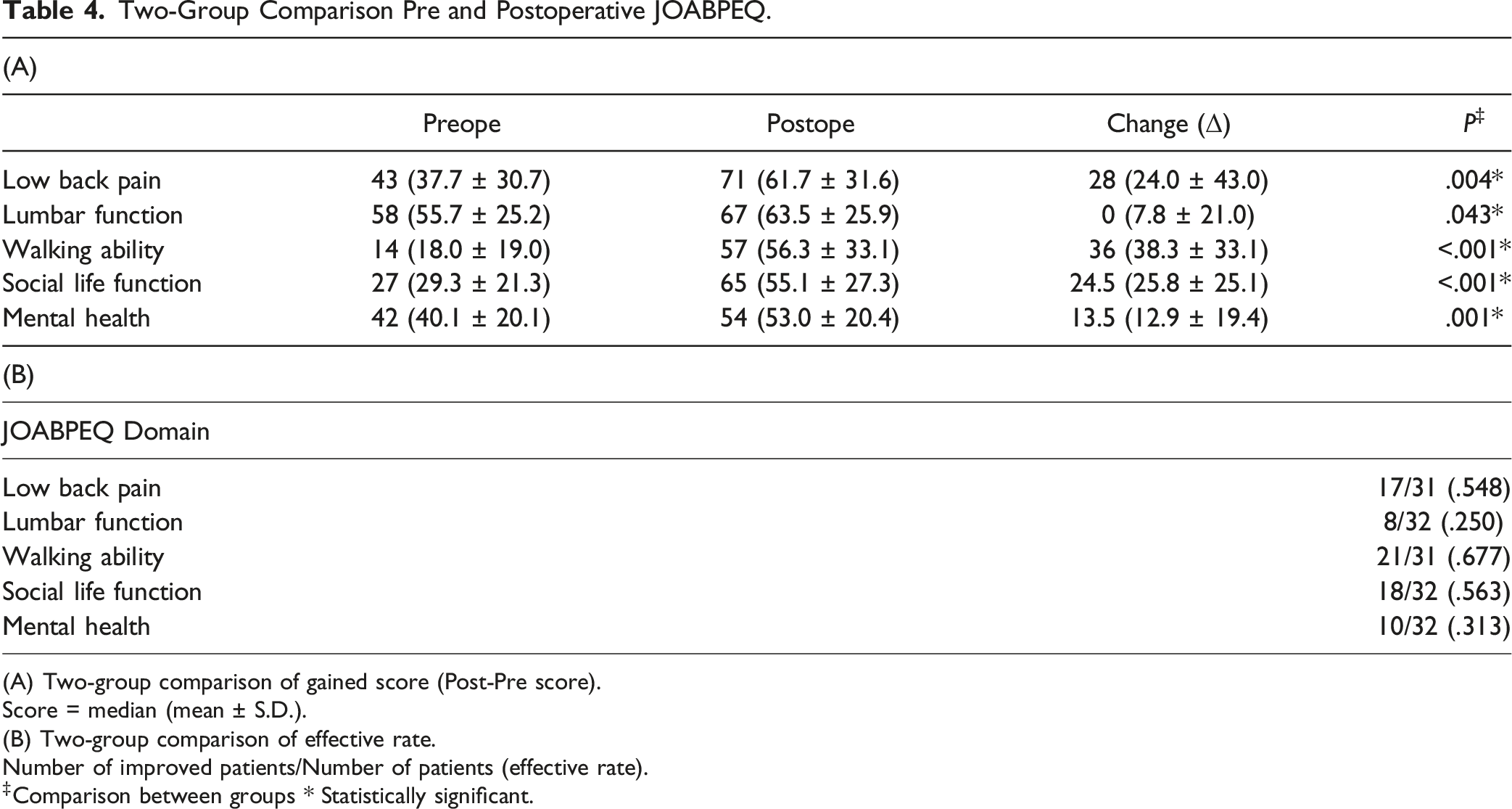
(A) Two-group comparison of gained score (Post-Pre score).
Score = median (mean ± S.D.).
(B) Two-group comparison of effective rate.
Number of improved patients/Number of patients (effective rate).
‡Comparison between groups * Statistically significant.
Correlation Analysis Between IL6 and Patient Background.

*Statistically significant.
MRI Grading (P); Pfirrmann classification. MRI Grading (M-P); Modified Pfirrmann classification.
Correlation Analysis Between Each Domain of NRS Score (A) or JOABPEQ (B) and Patient Satisfaction. * Statistically Significant.

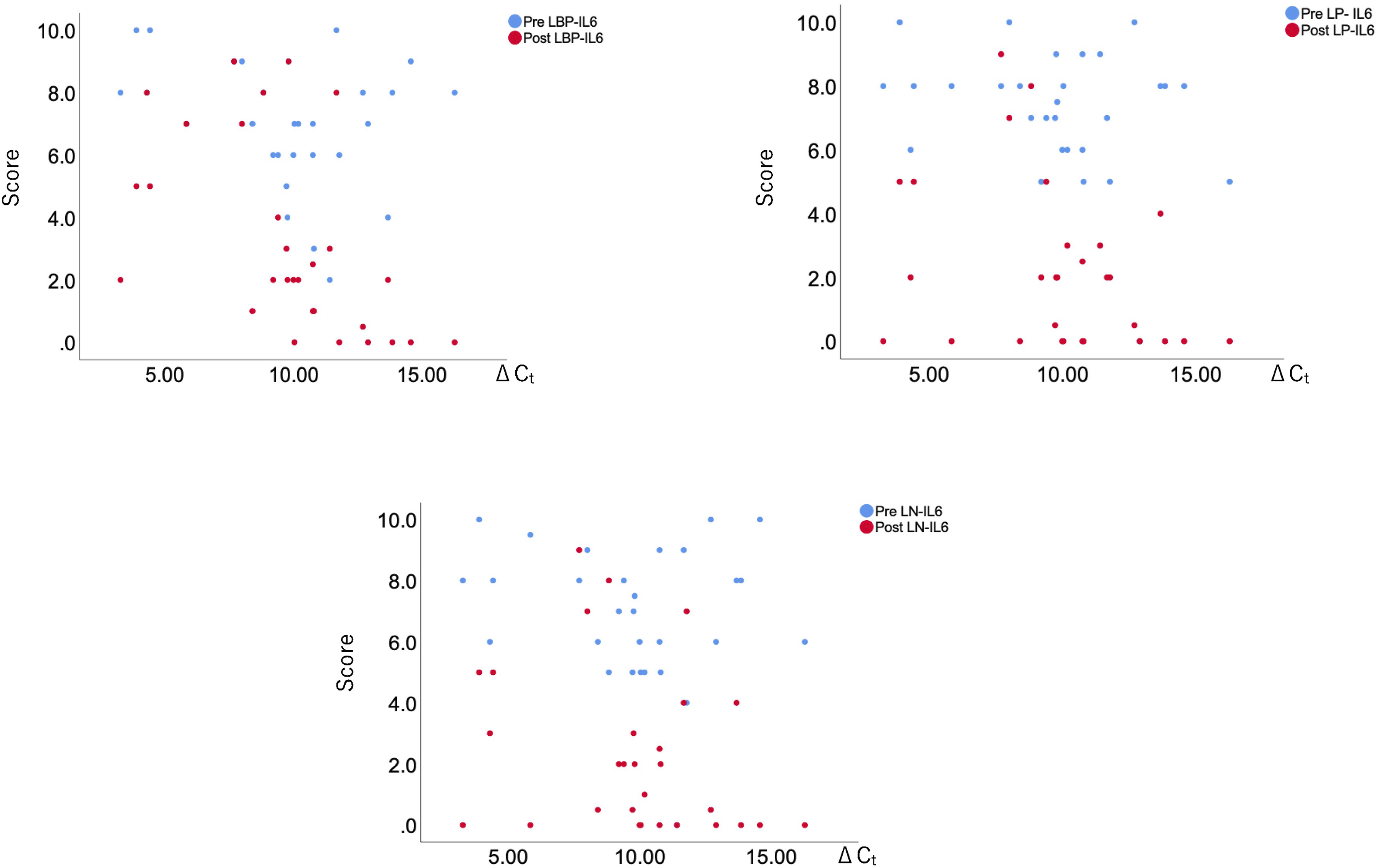
Scatter plots illustrating the correlation between each domain of pain and IL-6 levels before and after surgery. LBP (Low Back Pain), LP (Leg Pain), LN (Leg Numbness).
Correlation Analysis Between IL6 and JOABPEQ Domains.
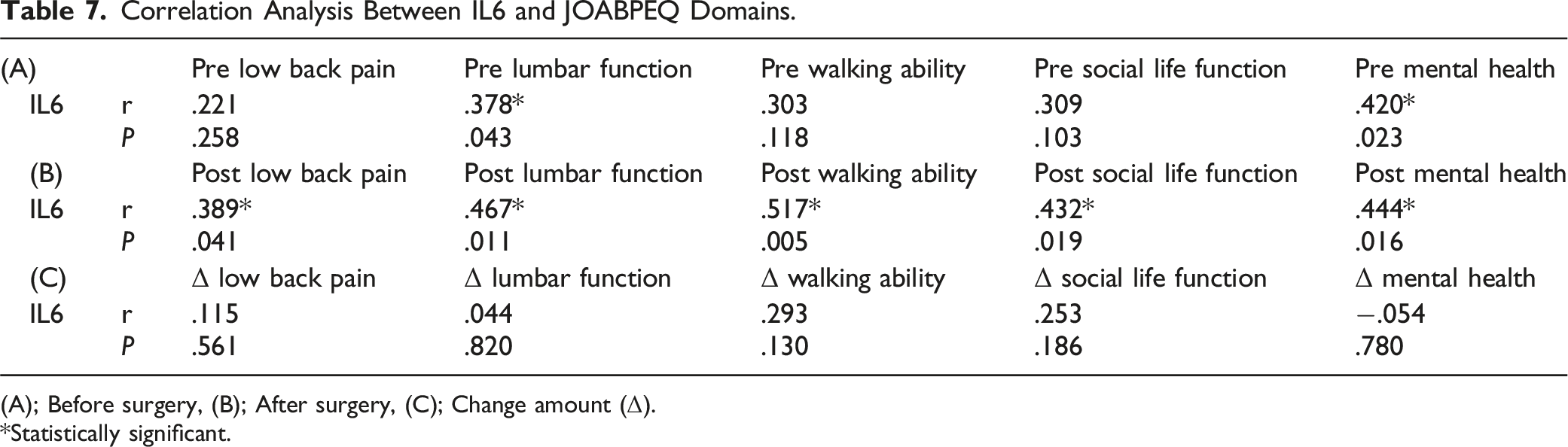
(A); Before surgery, (B); After surgery, (C); Change amount (Δ).
*Statistically significant.
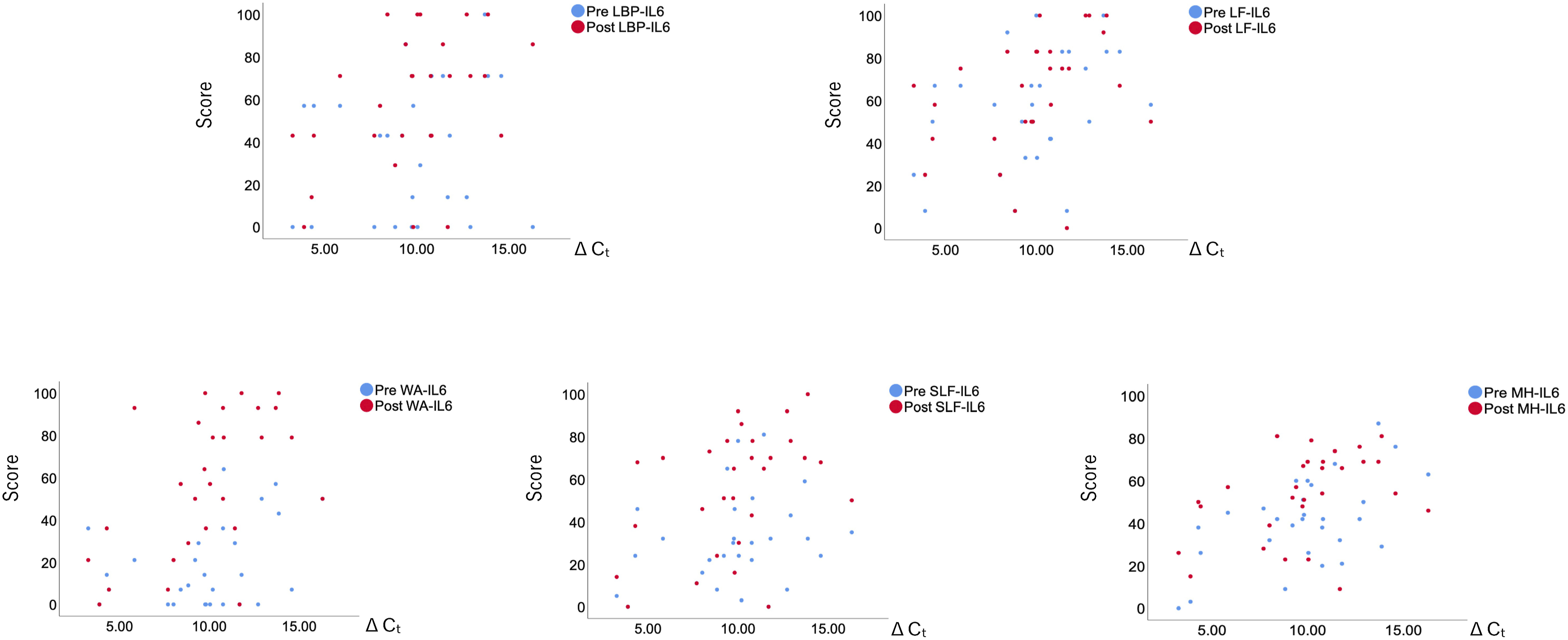
Scatter plots depicting the relationship between each domain of the Japanese Orthopedic Association Back Pain Evaluation Questionnaire (JOABPEQ) and IL-6 levels pre- and post-surgery. Domains include: LBP (Low Back Pain), LF (Lumbar Function), WA (Walking Ability), SLF (Social Life Function), MH (Mental Health).
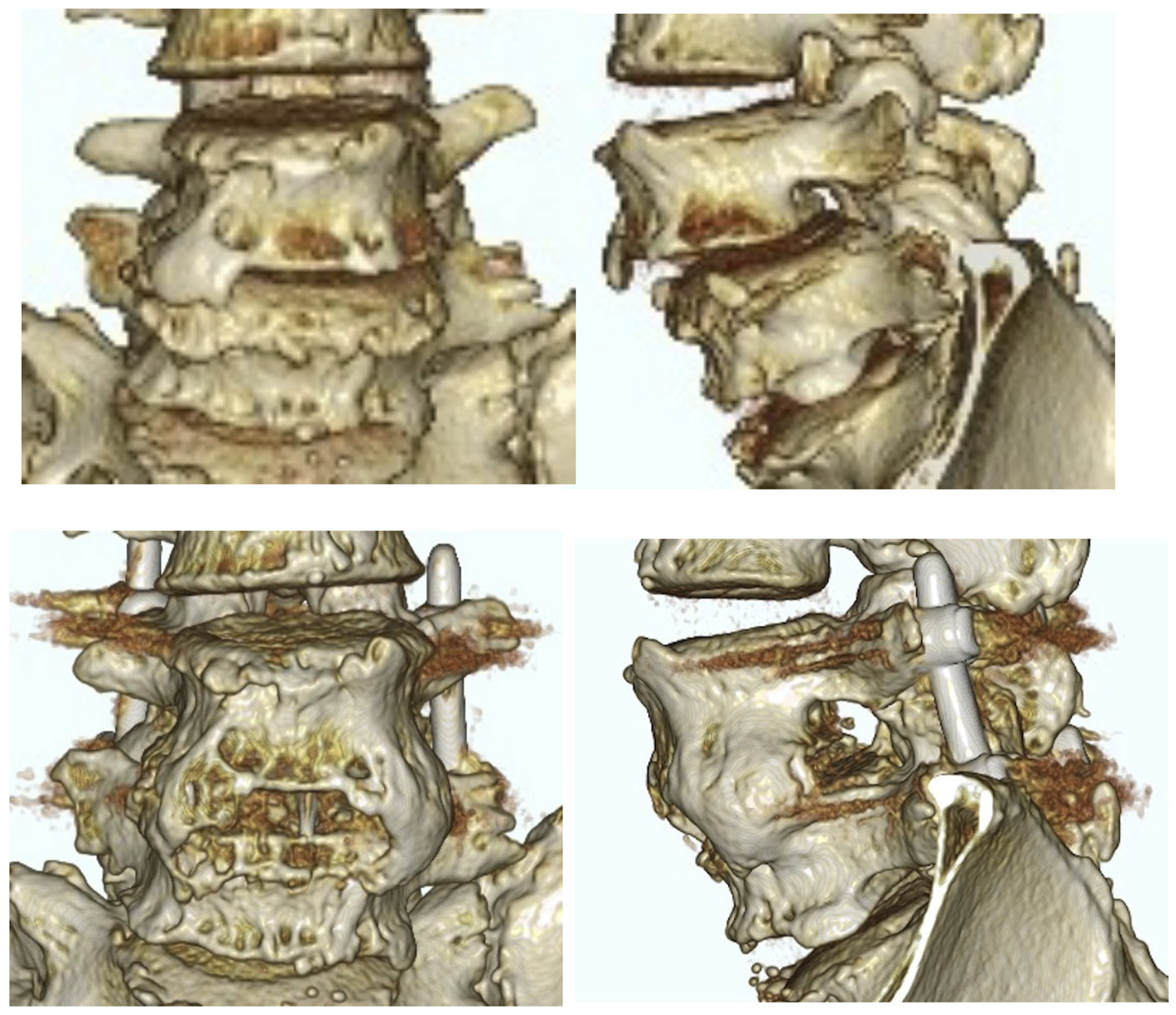
Case Example
A 70-year-old man presented with L4 LDS accompanied by LBP and radicular pain, with scores of 8.5 on the NRSLBP, 8.5 on the NRSLP, and 9 on the NRSLN. He underwent an L4/5 surgical procedure (as shown in Figure 3). The patient experienced a smooth post-surgical recovery without any complications. MRI scans post-surgery revealed successful correction of the slippage and achievement of indirect decompression. There was an improvement in all preoperative pain symptoms. The JOABPEQ scores showed significant improvements across various domains: low back pain improved from 14 to 100, lumbar function from 58 to 83, walking ability from 21 to 64, social life function from 24 to 51, and mental health from 34 to 48. The ΔCt value of IL-6 was 15.67. CT scans conducted 1 year post-surgery confirmed successful bone fusion (as depicted in Figure 4). Pre- and postoperative lateral radiograph and sagittal and axial MRIs revealing indirect decompression of the central canal at L4/5. Preoperative and postoperative coronal and sagittal 3D CT scans were performed. A postoperative bony bridge was successfully achieved. 3D CT (Three-dimensional Computed Tomography).
Discussion
This study delved into the correlation between IL-6 levels in IVD tissue and the clinical outcomes of patients undergoing surgery for LDD. Our research suggests that molecular markers, particularly the pro-inflammatory cytokine IL-6, indicate surgical outcomes, impacting patient-reported pain levels and functional outcomes.
IL-6 plays a vital role in LDD pathophysiology. We found a correlation between preoperative IL-6 levels and postoperative outcomes, notably in LBP and lumbar function. This indicates IL-6’s potential as a biomarker for predicting surgical outcomes and guiding postoperative management. Notably, elevated IL-6 levels in IVD tissue during surgery could foresee more intense LBP a year post-surgery.
The utility of the JOABPEQ in the evaluation of PROMs is well-recognized.29,30 Our findings show significant correlations between IL-6 levels and various JOABPEQ domains postoperatively, linking molecular changes in the spine to patients’ QOL. This dual approach, combining molecular markers with patient-reported measurements, advances our understanding of surgical outcomes.
Furthermore, consistent with previous reports, the indirect decompression achieved through LLIF enhances patients’ QOL. The improvement in JOABPEQ scores following LLIF underscores the potential of this surgical technique in managing patients with LDD.10,31 However, further research is necessary to fully understand the relationship between IL-6 levels and this surgical outcome.
Moreover, an interesting aspect of our study is the lack of significant correlation between IL-6 levels and changes in JOABPEQ scores (ΔJOABPEQ). Despite the significant correlations with several postoperative JOABPEQ domains, the relationship between IL-6 levels and the changes in these scores post-surgery was not statistically significant. This could be due to the smaller sample size when calculating ΔJOABPEQ, which requires pre- and post-surgery scores for each patient. Additionally, the 1-year timeframe for evaluating JOABPEQ scores may allow for numerous physiological and psychosocial changes, potentially diminishing or complicating IL-6’s influence.
Although IL-6 is a key biomarker in understanding inflammation in lumbar surgeries and subsequent LBP development, it is 1 of many biomarkers available.32,33 We recognize the importance of longitudinal evaluations post-surgery to gain a deeper understanding of the dynamics of inflammatory responses and their correlation with patient recovery and pain management. Longitudinal studies involving blood and potentially IVD tissue samples would allow us to track changes in IL-6 levels and other inflammatory markers over time. This could provide valuable insights into the effectiveness of surgical interventions and the progression of postoperative recovery.
Finally, recognizing the limitations of this study is crucial. Firstly, our cohort’s small size may limit our results’ reliability. Furthermore, expanding our analysis to include a broader range of inflammatory markers, not just IL-6, could provide more comprehensive insights into ongoing inflammatory processes. Additionally, while our study investigated the correlation between IL-6 expression in IVD tissue during surgery and changes in LBP intensity and postoperative JOABPEQ scores 1 year after surgery, it did not explore correlations with longer-term postoperative outcomes. Understanding these relationships could enhance our knowledge of how preoperative molecular profiles impact long-term patient outcomes. Moreover, the issue of adjacent segment disease following fusion surgery and the potential investigation of the impact of inflammatory cytokines within the disc in such scenarios could also be valuable. Another limitation is the absence of an assessment of systemic inflammation through blood markers, which are vitally important in understanding the extensive inflammatory response associated with spinal disorders and their treatment. Future research should aim to measure systemic inflammatory markers like IL-6 in the blood both preoperatively and postoperatively, to compare systemic and local inflammation levels and their correlation with clinical pain outcomes.
To address these limitations, future studies should include a larger patient population and investigate the roles of various cytokines and molecular markers. This approach could enable a closer understanding of the complex interplay between molecular changes, surgical techniques, and patient-reported outcomes, ultimately contributing to more personalized and effective treatments for patients with LDD.
Conclusions
In conclusion, this study demonstrated the significance of preoperative IL-6 levels within the IVD in predicting and understanding the clinical outcomes of surgical interventions in patients with lumbar LDD. IL-6 within the IVD is a key component in the network of inflammatory mediators involved in the pathology of LDD and the postoperative recovery process, representing a critical factor influencing patient outcomes. Therefore, IL-6 levels within the IVD may serve as a valuable biomarker for enhancing patient care in the management of LDD patients following surgery.
Footnotes
Authors’ Note
This study, including any part of it, does not have any prior or duplicate submissions or publications elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.