
Abstract
Study design
Retrospective comparative study.
Objectives
(i)to compare spinal cord drift between laminectomy and fusion(LF) and cervical laminoplasty(LP) for degenerative cervical myelopathy(DCM) treatment,(ii)to study relationship between preoperative cervical alignment, postoperative spinal cord drift, functional outcome, and C5 palsy.
Methods
A cohort of 114 patients who underwent LP or LF for DCM were identified. After propensity-score matching, both groups included 30 patients each.Cobb angle(C2-C7) was used to assess pre-and postoperative cervical spine alignment(at 2-year follow-up).Based on alignment, there were lordotic(L) and straight(S) subgroups.Spinal cord position was measured on sagittal-and axial-T2W MRI of cervical spine pre-and postoperatively at 2-year follow-up and cord drift was measured by subtracting preoperative values from postoperative values.Functional recovery(mJOA score, mJOA recovery rate),and C5 palsy in patients were recorded and compared.
Results
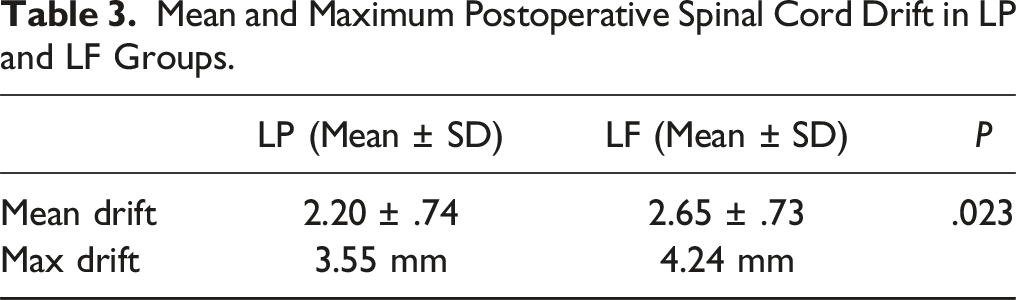
LF had higher mean spinal cord drift than LP(2.66 ± .77 vs 2.16 ± .80 mm, P = .049).Lordotic subgroups exhibited greater cord drift than straight subgroups within LP and LF groups.Both groups significantly improved mJOA scores at 2-year follow-up, with no LP-LF difference in mJOA recovery rate(mJOA-RR).Lordotic subgroups had significantly higher mJOA-RR(LP-L vs LP-S,P = .048; LF-L vs LF-S,P = .045).Preoperative cervical alignment, cord drift, and mJOA-RR correlated well(Spearman’s ρ .7143 and .6053 respectively).Patients with >2.5 mm cord drift(n = 24) had significantly higher mJOA-RR as compared to <2.5 mm cord drift(n = 18). Substantial clinical difference was seen in C5 palsy risk between LP-S and LF-L, with the LF-L group having 3-fold higher risk.
Conclusion
LF had a biomechanical advantage in maximizing spinal cord drift in severe DCM cases, while both LP and LF showed significant improvements in neurological function. However, variability in C5 palsy rates highlights the need for individualized patient assessment.
Introduction
Amongst the elderly population, degenerative cervical myelopathy (DCM) is the major cause of functional impairment. It happens due to the spinal cord’s gradual compression when the cervical spinal canal gradually narrows due to component deterioration.1,2 For progressive DCM, surgery has traditionally been the basis of care. The most often used posterior-based surgical methods for treating DCM are laminectomy (without fusion), laminoplasty (LP), and laminectomy and fusion (LF).3,4 Because there is a lesser chance of complications associated with the technique, posterior options are particularly appealing in the context of multilevel disease. 5
Spinal cord back drift has been considered the desired endpoint of posterior decompression procedures for degenerative cervical myelopathy (DCM). As a desired radiological endpoint for effective posterior decompression in the context of DCM, the idea of posterior spinal cord drift has been advocated recently. However, agreement on the connection between posterior spinal cord drift and neurologic results following posterior decompression is still difficult to come by. Furthermore, it is unclear how radiographic and clinical factors can predict spinal cord displacement. The difference in spinal cord drift between the LP and LF has not been well documented.
When the posterior cord drift is insufficient, residual anterior spinal cord compression may exacerbate the neurological deficit.6-8 In the published research, there has been a lot of interest in the possibility of predicting posterior spinal cord drift based on preoperative cervical alignment. The majority of studies examining spinal cord drift following posterior decompression have been on cervical laminoplasty,9-11 with only a small number compared with laminectomy. 12 We, therefore, carried out this study with the following objectives: (i)to compare spinal cord drift between Cervical Laminoplasty (LP) and Laminectomy with lateral mass screw fixation (LF) in patients with degenerative cervical myelopathy (DCM), (ii)to examine the relationship between preoperative cervical alignment, postoperative cord drift, functional outcome and occurrence of C5 palsy.
Methods
The institutional ethics committee (IEC Kothari Medical Center) granted permission for this retrospective study (IRB approval number KMC/2019/007) and all study participants provided informed consent for the study.
Data Collection
We retrospectively reviewed patients with DCM who had undergone LP or LF surgery from January 2018 to December 2020. These patients were prospectively followed up for a minimum of 2 years to assess clinical and radiological outcomes. Demographic data of patients including age, gender, and Charlson Comorbidity Index (CCI), 13 an index that predicts a 10-year survival rate in patients with comorbidities, were recorded. Both pre- and 2-year postoperative Cervical spine radiographs and magnetic resonance imaging(MRI) scans of DCM patients undergoing LP and LF were examined by 2 independent authors. The mean value of the 2 authors' recordings was taken as the final value. The intraclass correlation coefficient (ICC) was used to evaluate intra- and inter-rater reliability.
Study Cohorts and Propensity-Score Matching
A total of 114 patients (54 in the LP group and 60 in the LF group) were identified. After propensity-score matching, both groups included 30 patients each. The laminoplasty (LP) group consisted of 30 patients (18 men and 12 women). The Laminectomy and fusion (LF) group consisted of 30 patients (20 men and 10 women). Figure 1 demonstrates the flowchart of the number of patients in each group before and after propensity-score matching. One senior spine surgeon performed the surgeries on all of the patients. The surgical technique remained the same for all patients. LP group underwent a single-hinge door laminoplasty from C3 to C7, and the laminae were kept open by fixation with titanium mini plates and screws. LF group underwent lateral mass screw fixation from C3 to C7 followed by a C3 to C7 decompressive laminectomy. A case-by-case analysis was done while deciding which surgical method to employ. Flowchart demonstrating the patients in LP and LF groups before and after propensity score matching.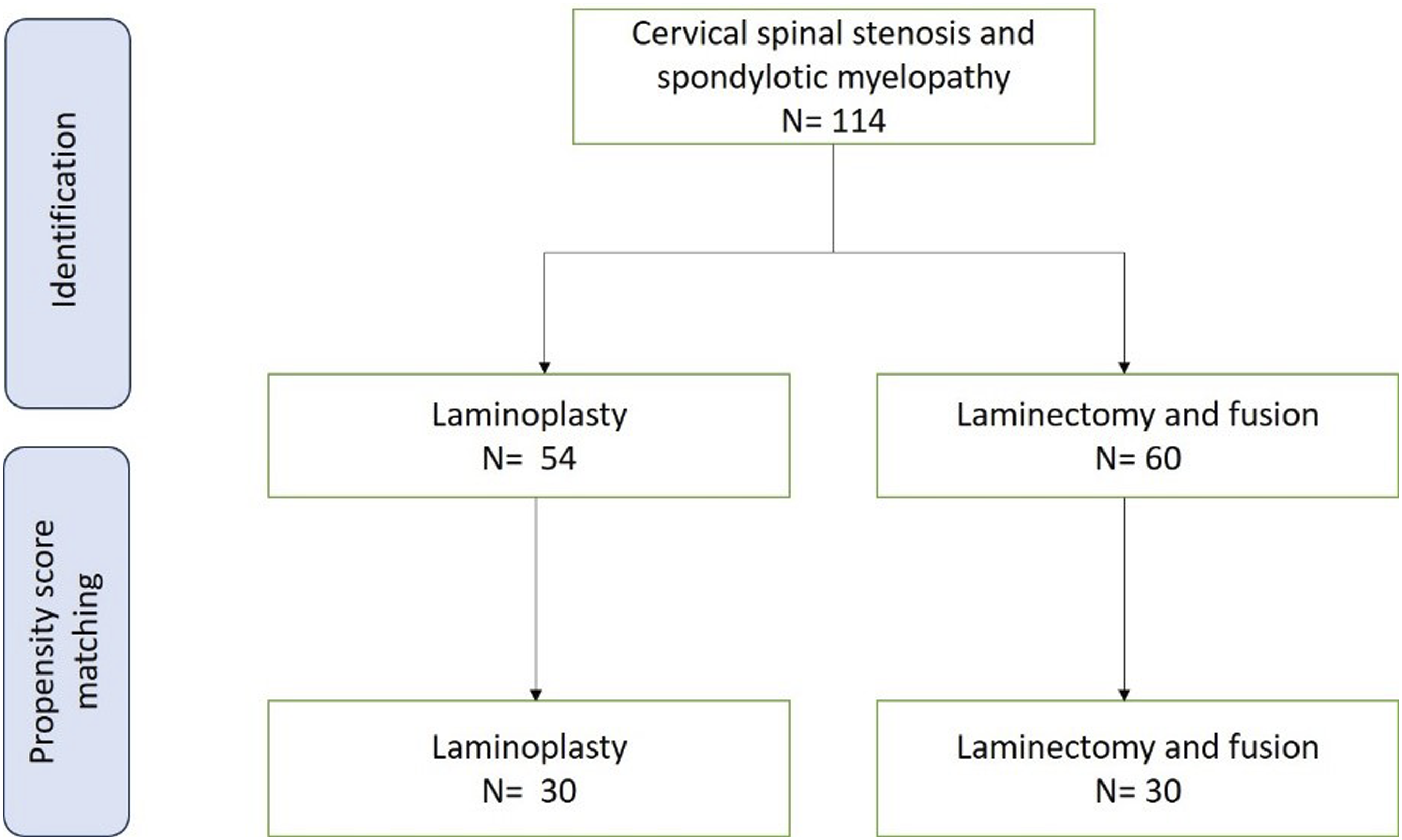
Patients were included if they (1) were 18 years or older; (2) had at least 1 myelopathy sign with symptomatic DCM; (3) had evidence of spinal cord compression on imaging. Patients with significant kyphosis and instability were contraindications for LP, whereas fixed severe kyphosis constituted a contraindication for LF. The following patients were excluded: a past history of undergoing cervical spine surgery; combined anterior cervical spine surgery along with posterior surgery; diagnosis of infection, tumor, acute trauma, or central cord syndrome; the concurrent existing other recognized neurological conditions disorder (such as multiple sclerosis, Parkinson’s disease, polio, or normal pressure hydrocephalus); or MRIs took after surgery within 24 months from surgery and those whose MRIs showed metallic artifact.
Radiological Parameters
Analysis of preoperative and postoperative MRI scans was performed with a Medsynapse picture archiving and communication system (PennsylvaniaCS) viewer and imaging software (2012 Medsynaptic Private Limited, Pune, Maharashtra, India). The measurements were performed using virtual calipers at a unified magnification of 200%. The Cobb angle(C2–C7) was used to compare cervical alignment before and after surgery on standing lateral radiographs. Subgroup analyses were conducted after further subclassifying both groups as Lordotic (L; Cobb angle >10o), straight (S; 0-10o), and kyphotic (K; <0o).14-16 At each cervical vertebral level, the position of the spinal cord was evaluated on sagittal and axial T2-MRI scans of the cervical spine before and after surgery. Sagittal and axial T2-MRI images of the cervical spine were used to assess the position of the spinal cord at each cervical vertebral level both pre-and post-surgery. The mean value of the 2 sagittal and axial measurements was selected as the final measurement for that particular level either on pre- or post-operative MRI scans. The spinal cord midpoint was calculated by adding the space anterior to the spinal cord (X) to the halfway value of the spinal cord’s AP diameter (Y/2). A value [X +(Y/2)] was calculated at each level of decompression and averaged to provide a representation of the spinal cord position globally (Figure 2). The spinal cord drift was calculated by deducting the preoperative measurements from the postoperative readings at each vertebral level from C2 to C7 in all the cases. (A) – The anterior space to the spinal cord (X) and half of the spinal cord AP diameter (Y/2) were added to find the spinal cord’s midpoint. At each decompressed level, this value [X + (Y/2)] was calculated, averaged, and used to represent the spinal cord position globally; (B) – Actual measurements done using Medsynapse PACS software, showing the calculation of midpoint of the spinal cord on T2W axial MRI image; Representative preoperative (C) and postoperative (D) T2W MRI images showing actual measurements and postoperative spinal cord drift in a patient who underwent laminectomy and fusion.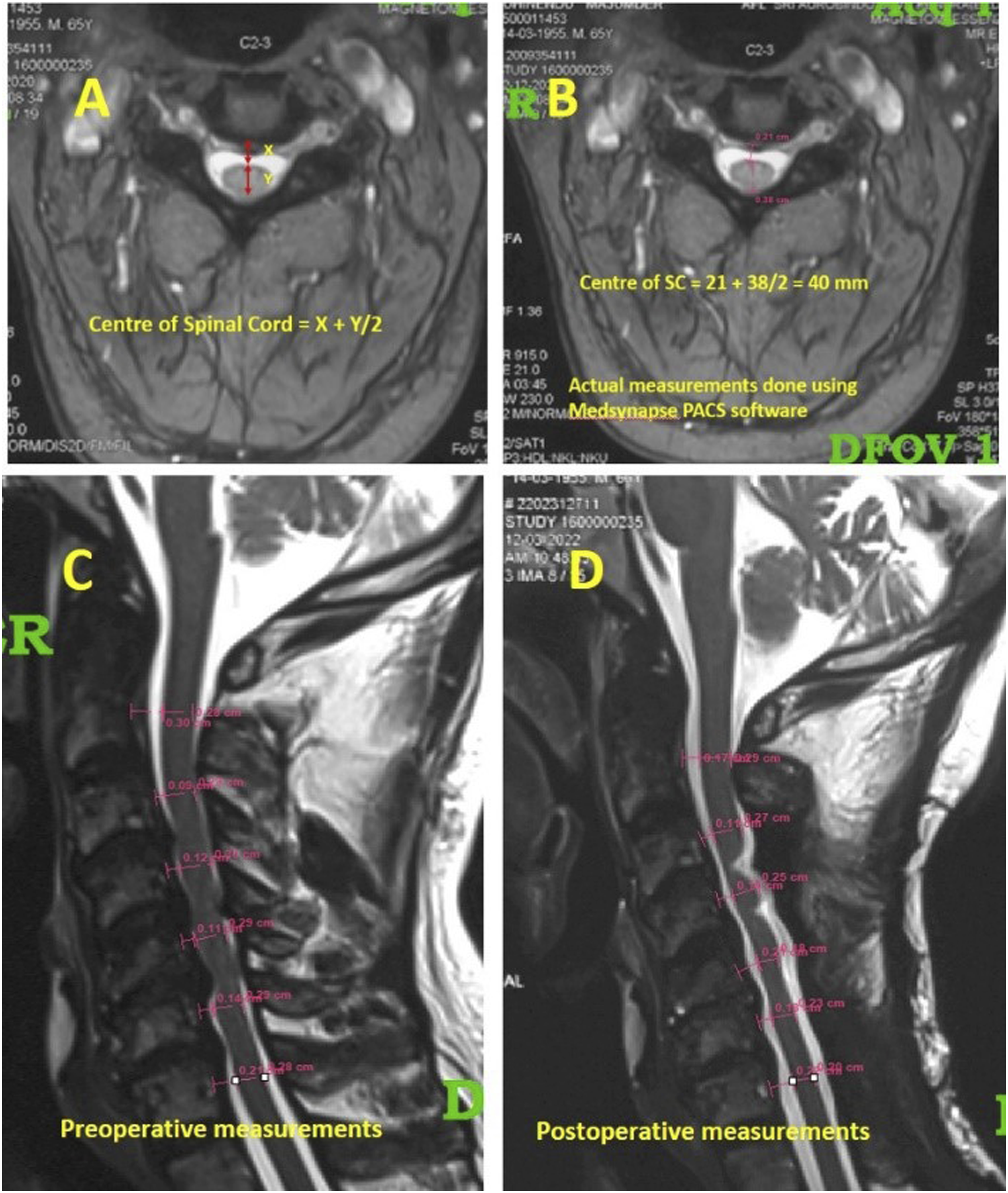
Functional Parameters
The neurological disability of each patient was determined using preoperative and postoperative calculations from the modified Japanese Orthopedic Association (mJOA) score and mJOA Recovery rate (mJOA RR). New postoperative occurrences of deltoid and/or biceps brachii paralysis were the diagnostic criteria for C5 palsy. In the C5 innervated area, some individuals may have sensory abnormalities and unbearable pain. The mJOA score was recorded preoperatively, at 3-, 6- months, and at 2-year follow-up and compared.
Statistical Analysis
This study used a propensity score matching method to take into consideration the potential selection bias caused by the possibility that some patients are more likely to have Laminoplasty compared to laminectomy and fusion. Based on a certain set of variables (such as age, gender, and CCI comorbidities), propensity score matching determines the conditional likelihood that each patient case will undergo a particular operation. Each laminoplasty case, for instance, is paired with the LF case that has the most similar propensity score. Thus, the preoperative distribution of confounding variables becomes comparable between the 2 cohorts. Propensity score-matched analysis was performed with multiple Chi-squared tests with Bonferroni correction of significance level (P < .05) to compare the complications between both groups.
Data extraction was performed to calculate mean scores when data were published. A chi-square test (categorical data) and a t test (continuous data) were used to analyze categorical and continuous parameters respectively. We utilized Spearman correlation coefficients to analyze relationships between independent factors and the dependent variable. A P-value of less than .05 was considered to be statistically significant. SPSS (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp) was used for statistical analysis.
Results
Demographic and Clinical Data
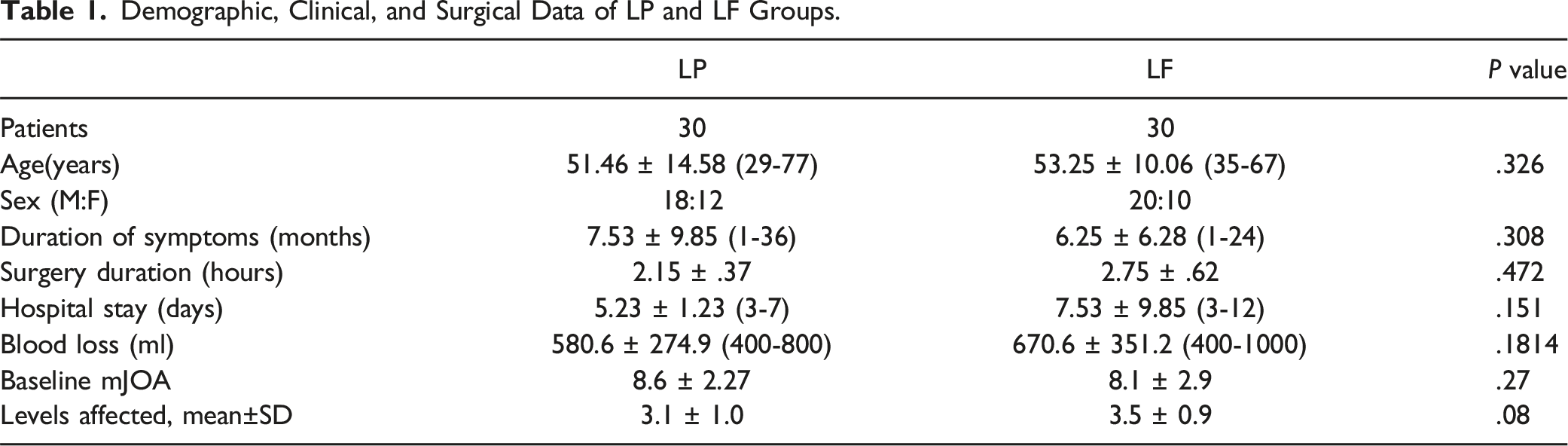
Demographic, Clinical, and Surgical Data of LP and LF Groups.
Functional Outcome
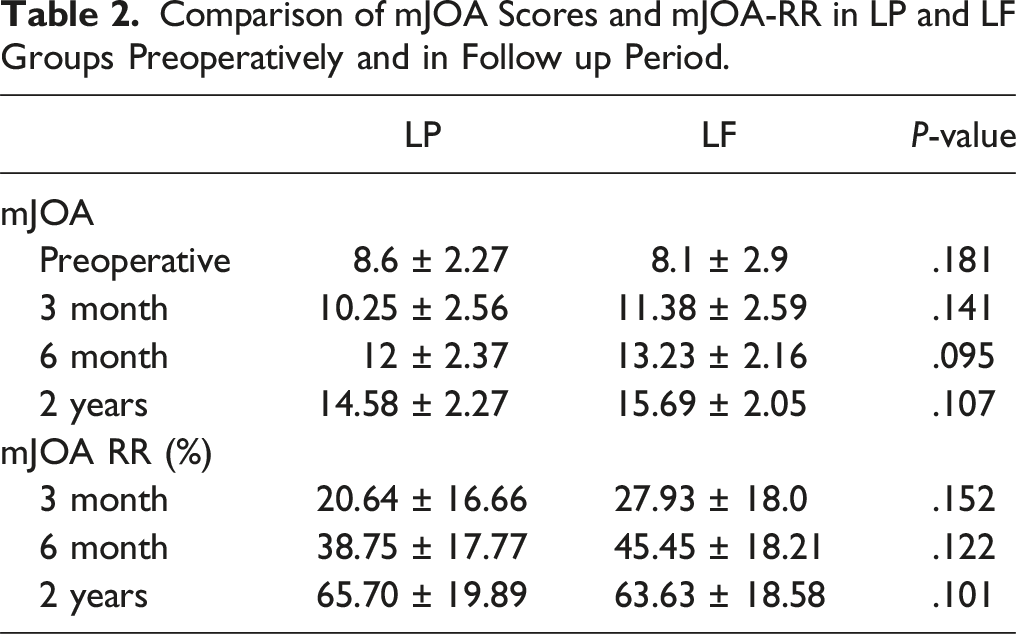
Comparison of mJOA Scores and mJOA-RR in LP and LF Groups Preoperatively and in Follow up Period.
Radiological Parameters
Influence of Preoperative Cervical Alignment on Postoperative Spinal Cord Drift
The preoperative cervical curvature was designated lordotic if the Cobb (C2-7) was greater than 10°; straight for Cobb (C2-7) between 0° and 10°; and kyphotic for Cobb (C2-7) less than 0°. Stratifying our cohorts based on these parameters yielded 17 lordotic (LP-L) (mean Cobb, 17.97; SD 6.06; range, 10.2-34.6) and 13 straight (LP-S) (mean Cobb, 5.43; SD 3.14; range, 0-9.7) in the laminoplasty group, and 14 lordotic(LF-L) (mean Cobb, 18.35; SD 6.24; range, 10.4-29.6) and 16 straight (LF-S) (mean Cobb, 4.21; SD 3.0; range, 0-9.4) in the laminectomy group. Preoperatively, the mean Cobb angle was comparable in both groups (LP = 12.54o vs LF = 10.81o, P = .42). The preoperative cervical curvature among the subgroups was also comparable. (LP-L vs LF-L, P = .86; LP-S vs LF-S, P = .30).
Mean and Maximum Postoperative Spinal Cord Drift in LP and LF Groups.
Mean Preoperative Cobb Angle and Mean Postoperative Spinal Cord Drift in LP and LF Subgroups.

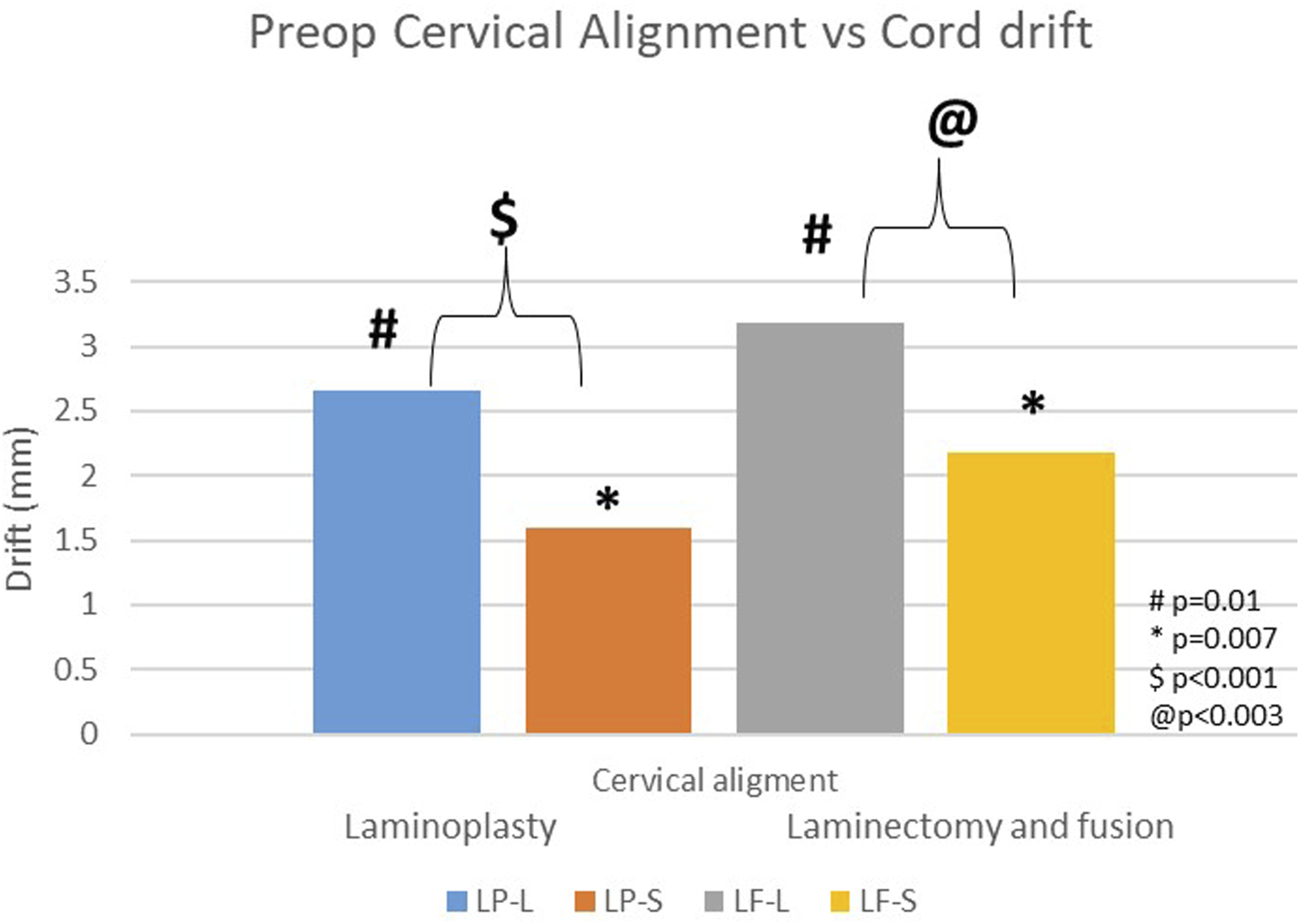
Comparison of mean postoperative spinal cord drift between LP and LF subgroups based on preoperative cervical alignment.
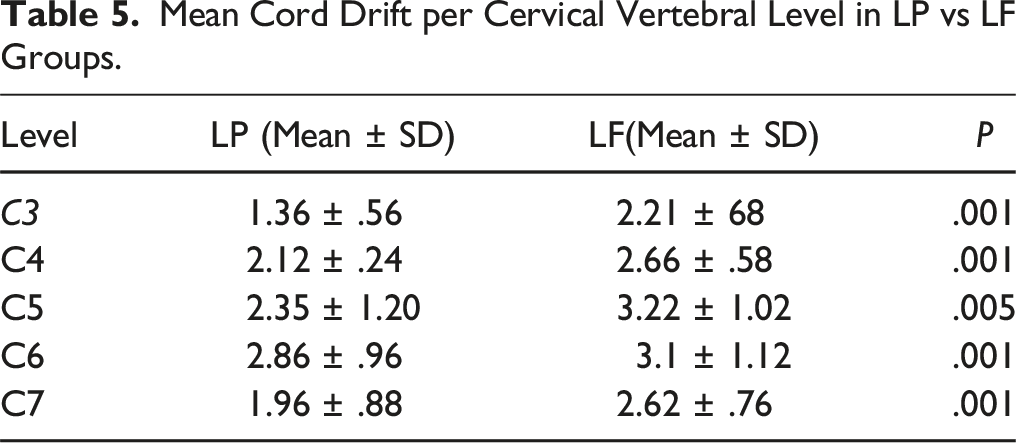
Mean Cord Drift per Cervical Vertebral Level in LP vs LF Groups.
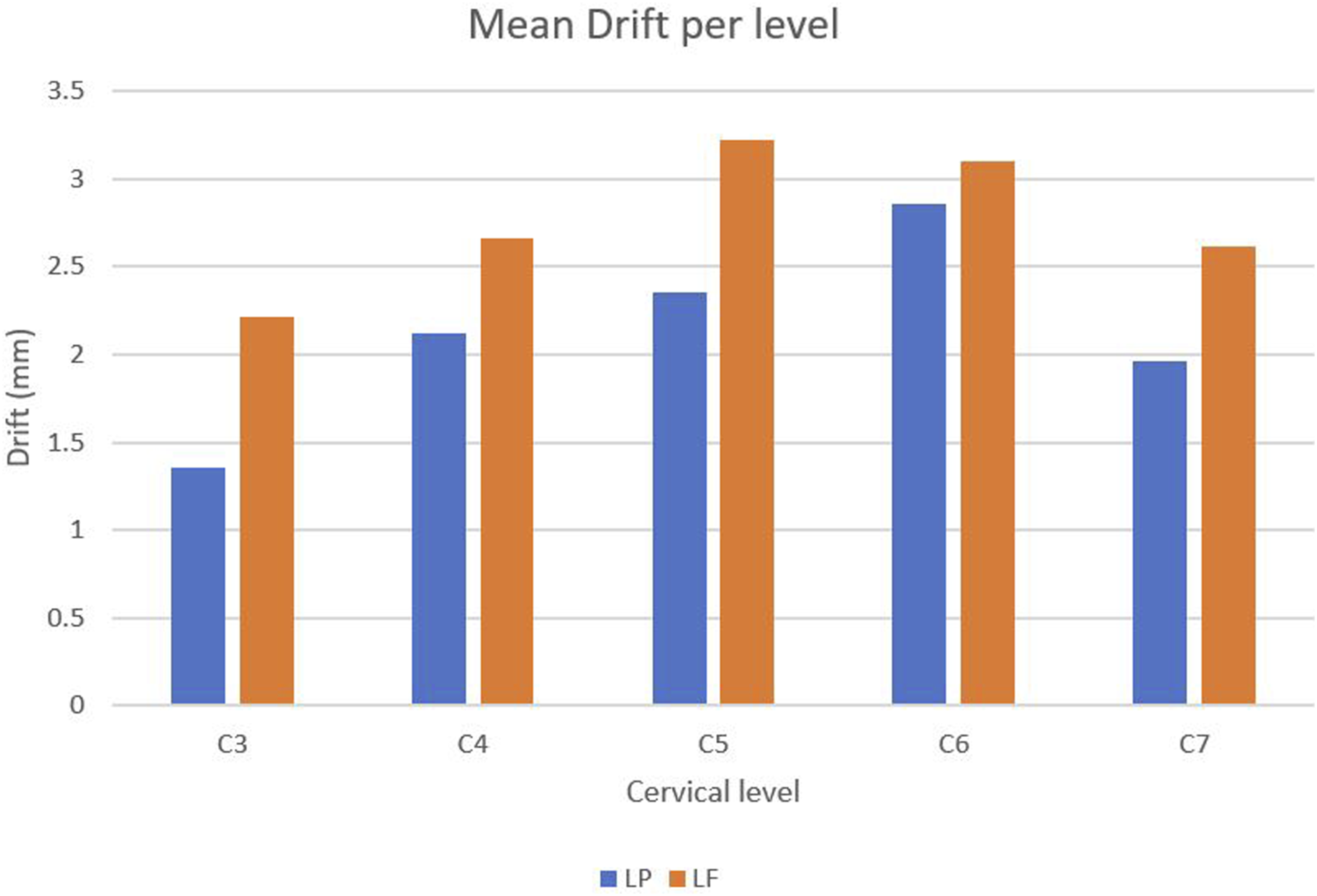
Mean cord drift per cervical vertebral level in LP vs LF groups.
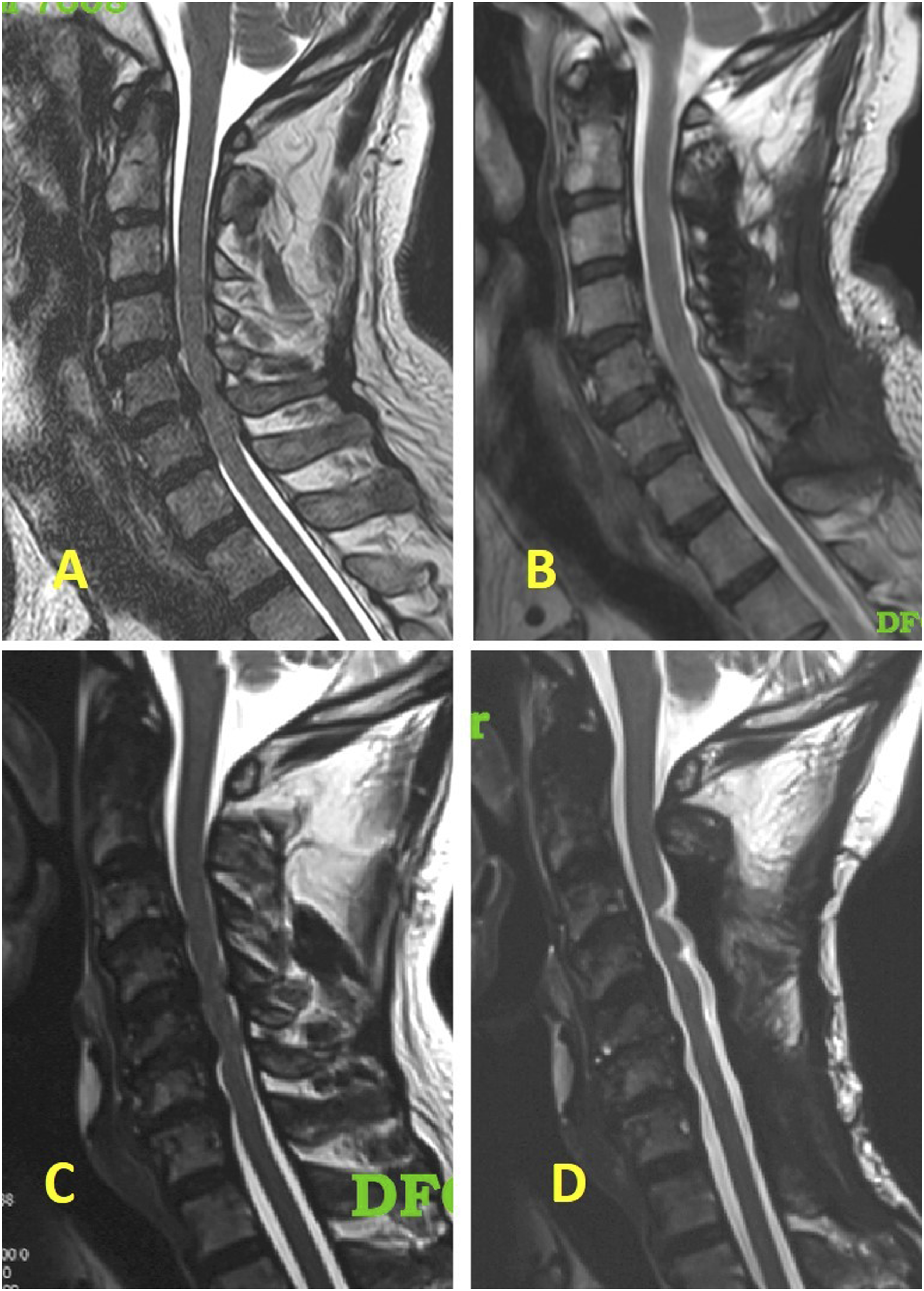
(A and B) – Preoperative and postoperative T2W sagittal MRI scan images respectively of a 57-year-old male who underwent C3-7 laminoplasty; C and D - Preoperative and postoperative T2W sagittal MRI scan images respectively of a 65-year-old male who underwent C3-7 laminectomy and fusion.
At 2-year follow-up, the mean Cobb angle decreased significantly for both groups (LP = 9.324 vs LF = 7.242, P < .01). However, the decrease was significantly greater following LF (P < .01). Subgroup analyses yielded no significant difference in drift observed with each group based on postoperative alignment (LP, P = .112; LF, P = .524). There was a strong positive correlation between preoperative cervical alignment and cord drift (Spearman’s ρ .713) (Figure 6) A - Scatter plot of preoperative cervical Cobb angle and mean postoperative spinal cord drift, B- Scatter plot of mean postoperative spinal cord drift and modified Japanese Orthopaedic Association recovery rate (mJOA RR).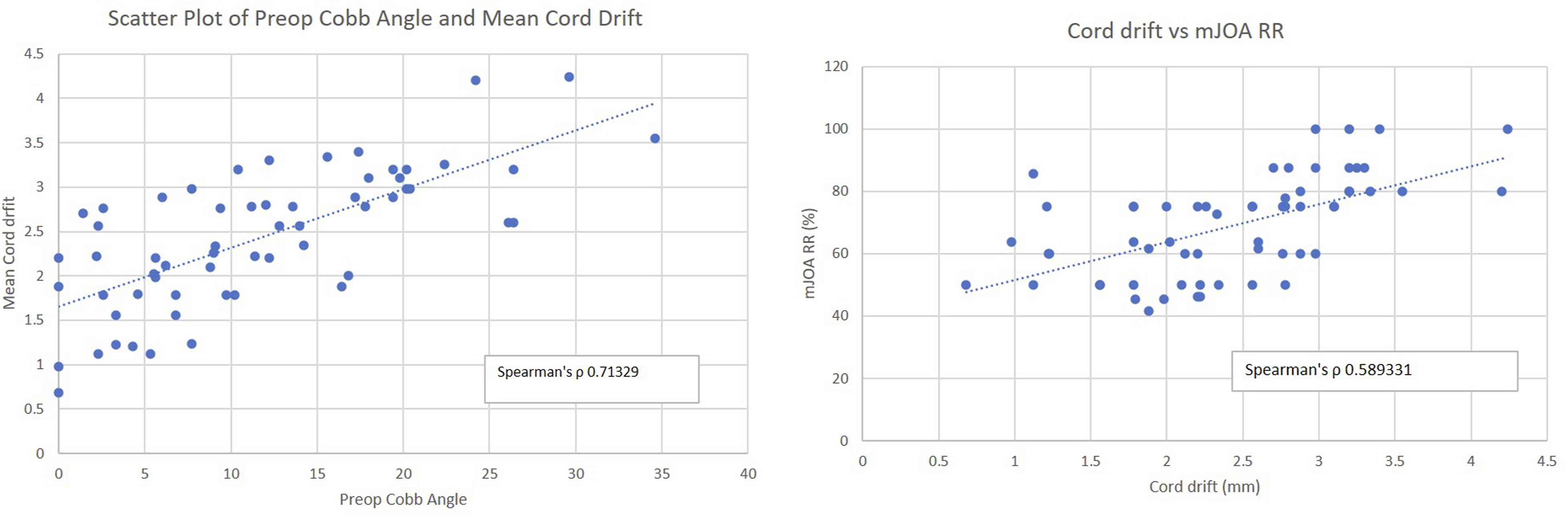
Relationship of Preoperative Cervical Alignment and Postoperative Spinal Cord Drift with Recovery Rate
The mean preoperative mJOA scores in LP and LF groups were 8.6 and 8.1 compared to mean postoperative mJOA scores of 14.9 and 15.9 respectively. Both groups showed significant improvement in mJOA scores postoperatively as compared to their preoperative value(LP, +6.3, P < .001; LF, +7.8, P < .001). However, there was no difference in mJOA score improvement postoperatively between 2 groups (P = .115).
There was no significant difference in the mJOA Recovery Rate (mJOA RR) between LP and LF groups (P = .9766). Subgroup analyses revealed significant improvement in mJOA RR in the lordotic subgroup as compared to the straight subgroup (LP-L vs LP-S, P = .013; LF-L vs LF-S, P = .043; LF-L vs LP-S, P = .017; LP-L vs LF-S, P = .041). However, no significant difference was found in comparing subgroups of LP and LF (LP-L vs LF-L, P = .751; LP-S vs LF-S, P = .844). The analysis of spinal cord drift and mJOA RR revealed a strong positive correlation (Spearman’s ρ .5893) (Figure 6B).
Comparison of Postoperative Spinal Cord Drift (less than 2.5 mm and More Than 2.5 mm) and mJOA Recovery Rate in these 2 Groups.

Influence of Preoperative Cervical Alignment on the Occurrence of C5 Palsy
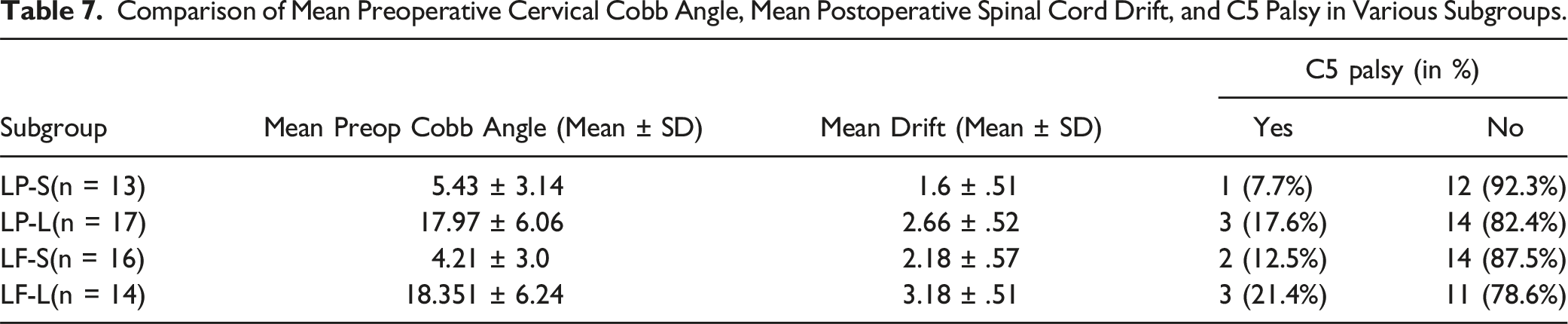
Comparison of Mean Preoperative Cervical Cobb Angle, Mean Postoperative Spinal Cord Drift, and C5 Palsy in Various Subgroups.
Discussion
Posterior spinal cord drift signifies the indirect decompression of the anterior aspect of the spinal cord, which is why it is the intended outcome of both laminoplasty and laminectomy and fusion. The goal of this study was to directly compare the degree of spinal cord drift experienced in a cohort of DCM patients who underwent LP or LF surgery. The mJOA score and mJOA RR were used as supplemental measures to correlate the spinal cord drift acquired with either group with the functional result. Laminoplasty offers various benefits over both laminectomy and laminectomy with fusion. 17 Laminoplasty, as opposed to laminectomy alone, retains cervical alignment better. Laminoplasty, as opposed to laminectomy and fusion, is a relatively motion-preserving treatment. 17 Du et al 18 found that patients with laminoplasty and laminectomy with fusion experienced excellent neurological improvement, with recovery rates of ≥75%. These results are comparable to our study, where both LP and LF groups had comparable functional outcomes concerning mJOA and mJOA-RR. However, Du et al reported high axial symptoms in the LP and laminectomy alone groups. 18 In the LF group, lateral mass screw fixation effectively prevented the loss of cervical curvature, reducing axial symptoms. 18 Lee et al 19 found that cervical lordosis, C2–C7 Cobb angle, and cervical curvature index decreased gradually in all patients, except for the Sagittal vertical axis, which was maintained in the laminectomy with fusion group. Clinical outcomes improved in all patients undergoing laminectomy alone, LP, and LF, and the progression of OPLL was observed more frequently with the laminectomy alone group than LF group.
The Influence of Cervical Alignment on Spinal Cord Posterior Drift
On plain radiographs, preoperative cervical alignment was assessed in both groups, and the patient population was categorized depending on the Cobb angle (C2–C7). The stratification yielded 4 subgroups of patients (LP-L, LP-S, LF-L, and LF-S). We did not have any patients with preoperative cervical kyphosis. Comparing the LF group to the LP group, the mean postoperative cord drift was much higher in the LF group. When comparing the individual cervical vertebral levels, considerably higher drift was once more reported after LF at all cervical levels, with the highest amounts of drift being seen in both groups at C5 and C6. This result is in line with earlier research that showed a pattern of higher spinal cord drift in lower cervical vertebral levels as opposed to the upper levels.20,21
A better outcome in the setting of postoperative cord drift has encouraged various researchers to look into which particular preoperative radiographic measures may be connected with postoperative cord drift. The first improved outcome in cases with preoperative cervical lordosis was reported by Batzdorf and Batzdorff. 6 Conceptually, spinal cord drift (bowstring principle) should be highest in the situation of cervical lordosis (bow) because, after the posterior vertebral canal has been surgically extended, the cervical lordotic arc places the anterior spinal cord farthest away from more anterior compressive structures. The tensile stress caused by the cervical curvature arc is imaged as the spinal cord drift distance. 22 Baba et al 22 discovered a correlation between preoperative cervical alignment and posterior spinal cord drift, but multiple later studies by different authors23-28 have been unable to confirm this association. However, we found that the lordotic subgroups (LP-L and LF-L) had significantly more spinal cord drift as compared to the neutral subgroups (LP-S and LF-S). Preoperative cervical alignment and spinal cord drift showed a significant positive correlation (Spearman’s ρ .713).
Regardless of the surgical approach, all patients who had posterior neck surgery(laminectomy alone, LP, and LF) tended to lose cervical lordosis to some degree. 19 In our study as well, both groups experienced lordosis loss postoperatively. When LF was performed as opposed to LP, this was more obvious. This could be due to adjacent segment degeneration and biomechanical changes induced by fusion surgery, potentially contributing to changes in the cervical alignment. Furthermore, in the surgical technique, there might have been a conscious effort to under-contour the rods to prevent postop C5 palsy. Despite this, after LF, greater cord drift was seen. We postulate that the extensive posterior space made accessible by LF and the removal of potential cord tethers result in a wider range of dynamic cord movement unrelated to the effects of alignment. On the other hand, restricted posterior space and remaining posterior parts after laminoplasty theoretically limit the maximum range of dynamic cord mobility in that situation. In these circumstances, attaining sufficient drift might depend on optimizing all helpful factors, including alignment.
Relationship of Preoperative Cervical Alignment and Postoperative Spinal Cord Drift with Recovery Rate
Both groups (LP and LP) showed significant improvement in mJOA and mJOA RR at 1-year follow up and there was no difference between the 2 groups. However, the subgroup analyses revealed significant improvement in mJOA-RR in the lordotic subgroup as compared to the straight subgroup (LP-L vs LP-S, P = .048; LF-L vs LF-S, P = .045). Spinal cord drift and mJOA-RR showed a strong positive correlation(Spearman’s ρ .5893). The choice of 2.5 mm was motivated by our interest in identifying a cutoff that holds clinical relevance, where the magnitude of drift is likely to have a meaningful impact on patient recovery. This threshold was not arbitrarily chosen; rather, it emerged from our data analysis as a point of significance. On further analysis and comparing spinal cord drift of greater than 2.5 mm vs lesser than 2.5 mm, a statistically significant improvement in mJOA RR was seen with a drift of more than 2.5 mm.
The existing literature is discordant regarding the correlation between spinal cord drift and mJOA RR. Baba et al 16 found that the postoperative posterior cord shift was substantially linked with neurological improvement and a greater posterior shift was observed in patients whose neurological recovery exceeded 50%. According to Sodeyama et al, 23 a mean displacement of 3 mm was necessary to significantly improve the neurologic condition, and the average recovery rate following laminoplasty was 53.8 ± 25.4%. However, other studies emphasizing the therapeutic significance of the postoperative spinal cord shift were unable to show a relationship between the recovery rate and the cord shift.24,28 A review of published studies has suggested that the degree of posterior spinal cord shift is not the only factor affecting satisfactory decompression in patients with DCM. An overview of potential factors affecting the mJOA, rather than the only measure of the back shift, would be of greater value in clinical practice. 29
Occurrence of C5 Palsy
A very typical side effect of LP or LF is C5 nerve paralysis. The increased cervical lordosis promotes posterior spinal cord drift and raises the stress of the C5 nerves, resulting in the development of C5 palsy. 30 According to Radcliff et al, 31 patients with C5 palsy had a considerably higher spinal cord drift distance at the C5 level (5.1 mm) than those without nerve paralysis. In the present study, the mean spinal cord drift for groups LP-S, LP-L, LF-S, and LF-L were 1.6 ± .51 mm, 2.66 ± .52 mm, 2.18 ± .57 mm, and 3.18 ± .51 mm respectively and the occurrence of C5 palsy was 7.7%, 17.6%, 12.5%, and 21.4% respectively, without any statistically significant difference in the incidence of the C5 palsy. Although the incidence of C5 palsy was higher in LF group than in LP group, it was not statistically significant. Although statistically insignificant, the clinical implications of these findings are considerable. The significant difference in C5 palsy risk between LP-S and LF-L, with the LF-L group having a 3-fold greater risk, emphasizes the need to take these details into account in therapeutic conversations with patients. This underlines the need to take a nuanced approach when communicating the risks associated with various surgical methods, where clinically important distinctions may persist despite statistical non-significance.
There was no significant difference in the occurrence of C5 palsy in lordotic and straight subgroups. We reasoned that because the LF-L group had the largest cervical curvature and the mean cord drift was only 3.18 mm, much less than the 5.1 mm in Radcliff et al.’s study, 31 the degree of cord drift was insufficient to alter the frequency of C5 palsy significantly.
Limitations
While this study contributes valuable insights into the comparative outcomes of cervical laminoplasty (LP) and laminectomy with fusion (LF) for degenerative cervical myelopathy, several limitations warrant acknowledgment. The study primarily focused on the comparison of LP and LF, omitting the inclusion of laminectomy without instrumentation, which is a common technique, particularly in resource-constrained settings. Future research could benefit from a more comprehensive comparison encompassing laminectomy without instrumentation to offer a more holistic view of surgical interventions for cervical myelopathy. Additionally, the study faced constraints related to the timing of postoperative measurements, particularly in assessing the temporal aspects of lordosis changes. The absence of early postoperative measurements hinders a precise determination of when the postoperative loss of lordosis occurred, especially in the context of laminoplasty where motion segment preservation is a key consideration. While efforts were made to address subgroup comparisons and statistical significance, the study’s sample size may have limitations in detecting smaller yet clinically relevant differences between groups. Despite these limitations, this research adds valuable data to the existing literature on surgical interventions for degenerative cervical myelopathy.
The propensity score matching reduced the selection bias, created more homogeneous treatment groups, and eliminated the confounding variables of both the study groups making it more accurate in characterizing outcomes following LP and LF for DCM. The strengths of this study include multidimensional assessment involving preoperative cervical alignment, postoperative spinal cord drift, functional recovery (mJOA score, mJOA recovery rate), and C5 palsy incidents, supported by correlation analyses and robust statistical methods. The clinical value of this study resides in guiding treatment choices and improving comprehension of the surgical outcomes for DCM patients, with implications for the broader clinical application.
Conclusion
Our findings underscore the biomechanical advantage of LF in achieving greater spinal cord drift, suggesting its potential role in maximizing decompression in severe DCM cases. Despite this, both LP and LF demonstrated significant improvements in functional outcomes, emphasizing their efficacy in enhancing neurological function. The absence of a significant difference in the occurrence of C5 palsy between LP and LF provides an easier choice of posterior surgery for clinicians and patients. However, subgroup analyses revealed variability in C5 palsy rates among different subgroups, underscoring the need for individualized patient assessment, clinical discussions with patients, and risk mitigation strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.