
Abstract
Study Design
Retrospective Administrative Database Analysis.
Objective
The purpose of this study was to compare the rate of subsequent cervical fusion surgery between patients that received cervical laminectomy and cervical laminoplasty for degenerative cervical disease.
Methods
The PearlDiver database for years 2010 to 2021 was queried for patients who received either a posterior cervical laminectomy or a cervical laminoplasty for a diagnosis of degenerative cervical disease. A matched analysis was performed using the significant variables. Rates of subsequent fusion surgery were determined for each cohort for 2-year, 5-year, and 10-year after surgery. Survival analysis was performed.
Results
A total of 4406 patients (Laminectomy: 2258; Laminoplasty: 2148) were included in this study. In the matched analysis, the rate of subsequent fusion surgery for laminectomy at 2-year, 5-year, and 10-year were 3.2%, 5.0%, and 5.7%, respectively. The rate of subsequent fusion surgery for laminoplasty at 2-year, 5-year, and 10-year were 2.2%, 3.2%, and 3.5%, respectively. There was no significant difference between the 2 groups at 2-year after surgery (P = 0.07). Patients who received cervical laminectomy had a higher rate of subsequent fusion surgery than cervical laminoplasty at 5-year (P < 0.01), and 10-year (P < 0.01) after surgery. Conclusions: In patients with degenerative cervical disease, cervical laminectomy had a significantly higher rate of subsequent fusion surgery than cervical laminoplasty at 5-year and 10-year post-surgery. This is the largest study comparing laminectomy to laminoplasty to date.
Introduction
Degeneration of the disc and facets result in neck pain and neurologic compression causing signs and symptoms of myelopathy and radiculopathy. 1 Degeneration of the cervical discs and facet joints lead to cervical degenerative disease (CDD), which includes cervical spondylosis and degenerative cervical disc disease. CDD can be found in over 60% of patients over the age of 40.1 The goal of surgery is to decompress neurological elements to improve symptoms and to prevent neurological decline. Various surgical options exist including cervical laminectomy, cervical laminoplasty, and cervical decompression and fusion.
Nonoperative conservative measures are typically the first line treatment for symptomatic CDD. However, for patients in which nonoperative treatment is insufficient or for those who have significant neurological symptoms, surgical decompression is suggested. Over the years, there has been substantial debate over the most appropriate surgical treatment of cervical myelopathy. Up until the 1980s, cervical laminectomy was considered the gold standard approach because it preserved cervical range of motion compared to fusion, while providing effective decompression.2,3 However, following concerns of post-laminectomy cervical kyphosis, laminoplasty was introduced as an alternative surgical approach that widened the spinal canal without permanent removal of the dorsal elements.4,5 The theoretical benefit of performing a laminoplasty is to preserve motion while minimizing spinal structural instability, which could necessitate subsequent revision and fusion. 5
Despite the widely purported benefits of cervical laminoplasty over laminectomy alone, there is limited and conflicting literature comparing patient outcomes between these 2 procedures.6-8 Given the considerable discrepancy and limited sample sizes in prior literature, the purpose of this study was to analyze a nationwide patient population to compare rates of subsequent fusion surgery following cervical laminectomy vs cervical laminoplasty in the treatment of compressive CDD.
Materials and Methods
Study Design and Data Source
This was a retrospective cohort study using Pearldiver. Pearldiver is a national insurance database consisting of over 150 million patients covered by Medicare, Medicaid Advantage, cash claims, and private insurance. Pearldiver was queried for years 2010 to 2021 using International Classification of Disease codes (ICD-9, ICD-10) and Current Procedural Terminology (CPT) codes. Two cohorts were identified using CPT codes: laminoplasty (CPT-63051, CPT-63959) and laminectomy (CPT-63001, CPT-63015). Inclusion criteria required a diagnosis of CDD and a minimum follow-up period of 2 years. Patients were excluded if they had: (1) a diagnosis of cervical kyphosis (ICD: ICD-10-D-M40209, ICD-10-D-M40202, ICD-9-D-73710, ICD-9-D73720), (2) previous cervical laminectomy, (3) previous cervical laminoplasty, (4) previous cervical fusion, (5) a history of spinal trauma, neoplasm, or infection within 90 days of their index procedure, or (6) cervical spine surgery (intentionally staged fusions or immediate revisions) within 90 days of their index procedure. Patient demographics including age at time of procedure, gender, geographic region (Midwest, Northeast, South, or West), and year of procedure were extracted.
Outcomes and Statistical Analysis
The primary outcome of interest was subsequent cervical fusion surgery at 2-year following initial laminectomy or laminoplasty. Secondary outcomes of interest included subsequent cervical fusion surgery at 1-, 3-, 4-, 5-, and 10- years following initial procedure. Subsequent cervical fusion was defined as any instrumented fusion procedure following the index cervical laminectomy or cervical laminoplasty. The instrumented fusion procedures were defined using CPT codes (CPT-22548, CPT-22551, CPT-22552, CPT-22585, CPT-22590, CPT-22595, CPT-22600, CPT-22614). All indications for subsequent cervical fusion were included, such as adjacent segment disease, kyphosis, instability, and inadequate decompression. Patients that had fusions performed 90 days before their index surgery, the same day as their index, or within 7 days of the index procedure were not included to exclude intentionally staged procedures and instrumented fusions.
A multivariable logistic regression analysis was performed to identify possible risk factors (diabetes, tobacco use, obesity, gender, age, Elixhauser Comorbidity Index, and osteoporosis) associated with subsequent cervical fusion surgery. These factors were chosen a priori based on previous literature and clinical relevance. Factors that significantly impacted risk for subsequent cervical fusion surgery were used to perform a 1:1 matched analysis between the laminectomy and laminoplasty cohorts. Rates of subsequent cervical fusion surgery at 1-, 2-, 3-, 4-, 5-, and 10-year post index procedure were compared between the 2 cohorts using Chi-square test. Survival analysis was performed and Kaplan-Meier curves were generated for subsequent cervical fusion surgery at 2- and 10-year post procedure. An alpha value of 0.05 was used as the threshold for statistical significance. All statistical analysis was performed using Pearldiver software.
Results
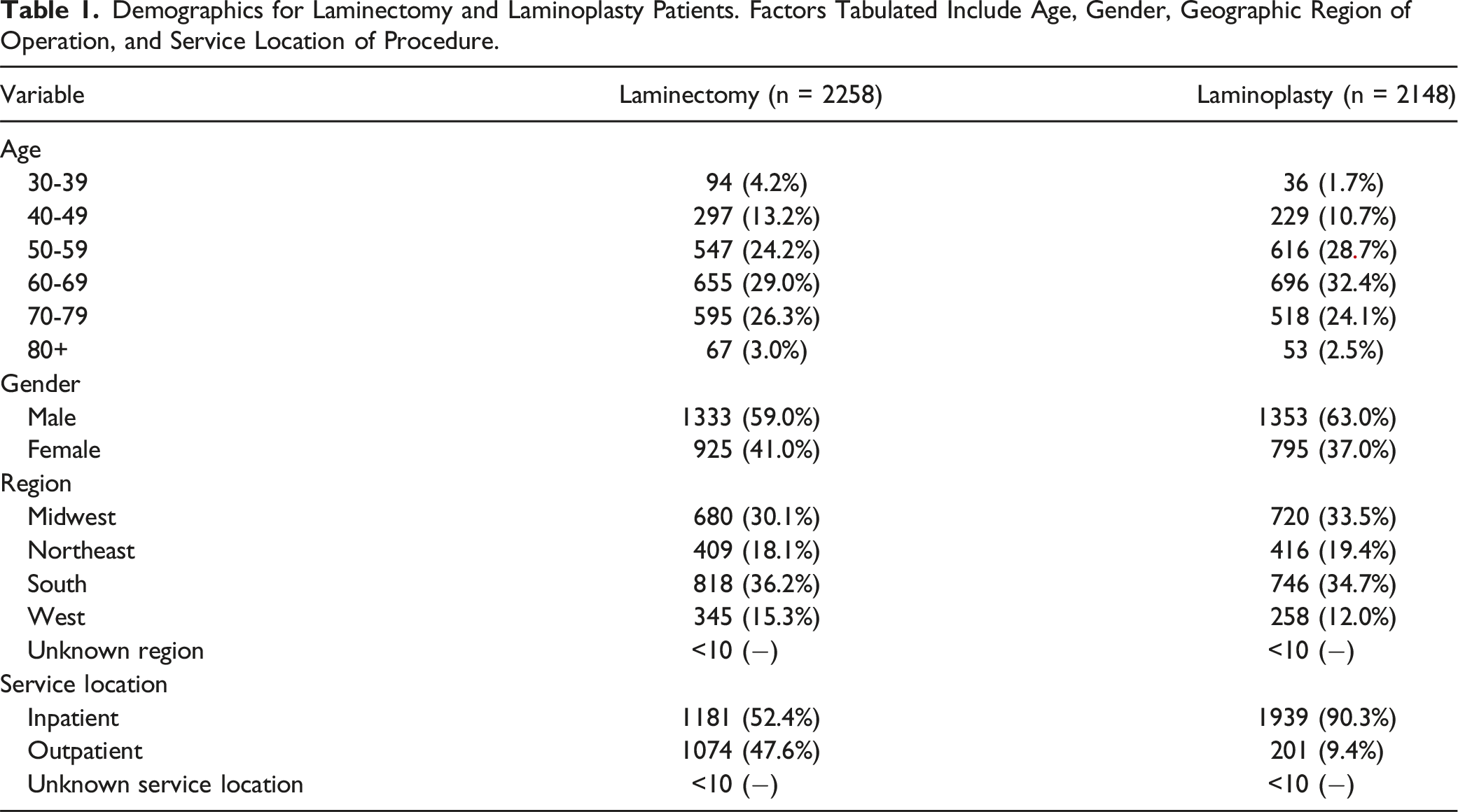
Patient Demographics
Demographics for Laminectomy and Laminoplasty Patients. Factors Tabulated Include Age, Gender, Geographic Region of Operation, and Service Location of Procedure.
Multivariable Logistic Regression Analysis on Subsequent Cervical Fusion Surgery
Multivariable Logistic Regression Analysis on Risk Factors for Fusion Following Laminectomy.
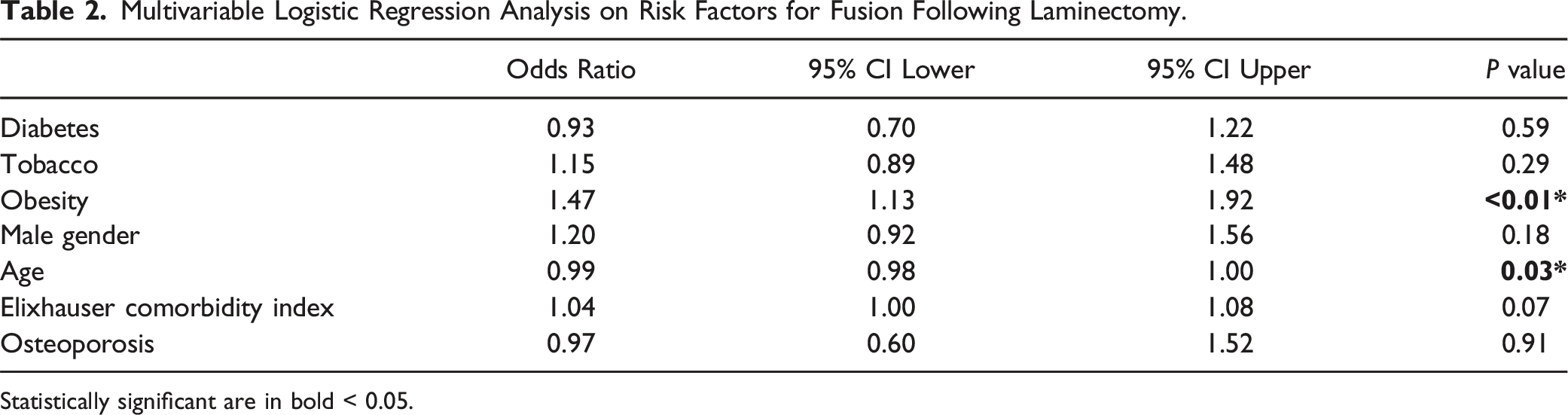
Statistically significant are in bold < 0.05.
Rate of Subsequent Cervical Fusion Surgery in Matched Analysis
Multivariable Logistic Regression Analysis on Risk Factors for Fusion Following Laminoplasty.
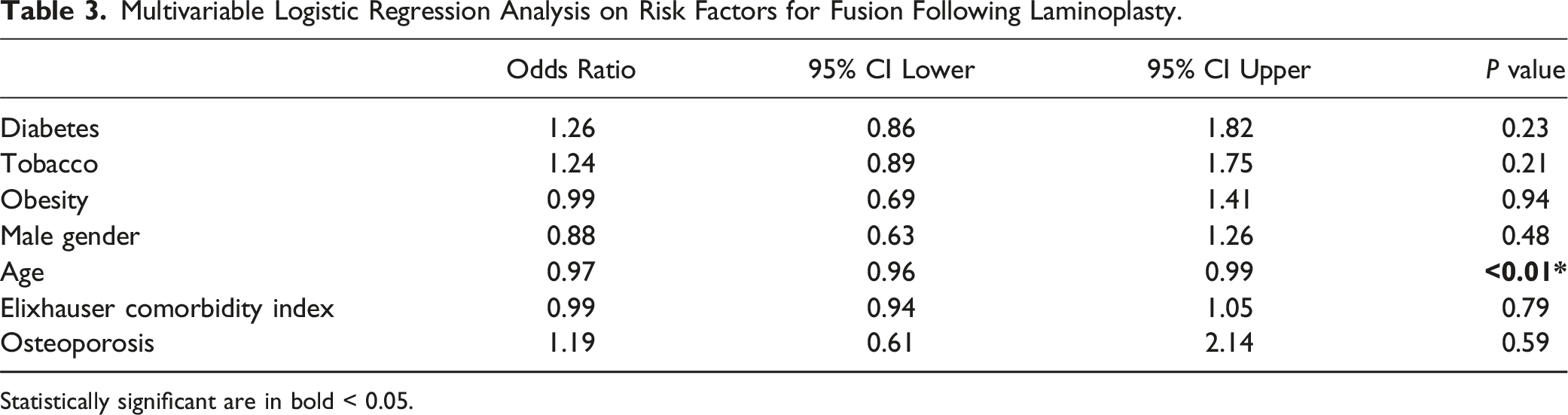
Statistically significant are in bold < 0.05.
Rates of Postoperative Fusion Following Laminectomy and Laminoplasty at 1-, 2-, 3-, 4-, 5-, and 10 Years. Cohorts Matched for Age and Obesity.
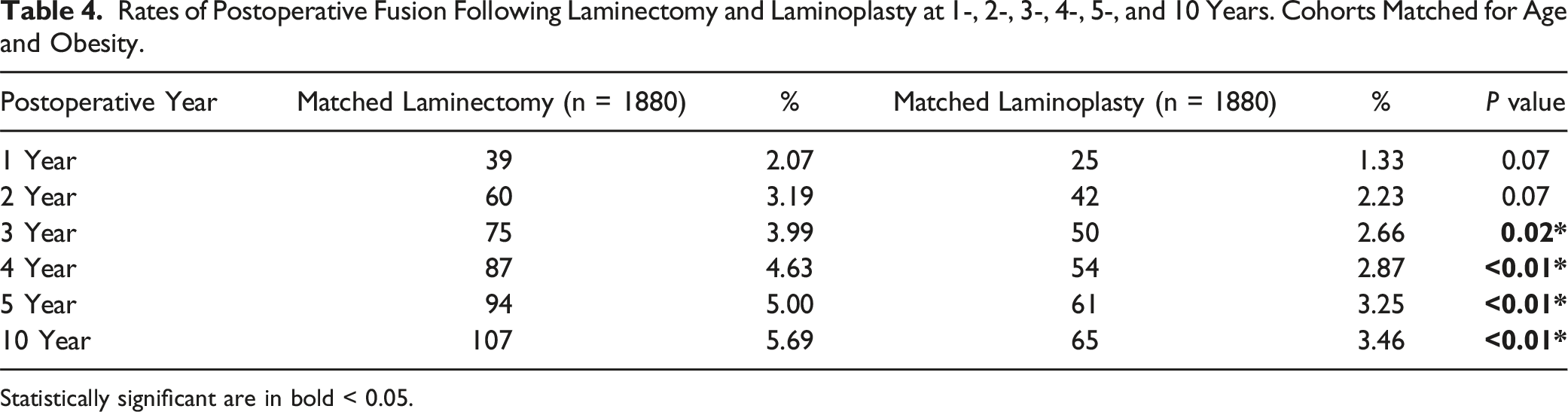
Statistically significant are in bold < 0.05.
Survival Analysis of Time to Subsequent Cervical Fusion Surgery
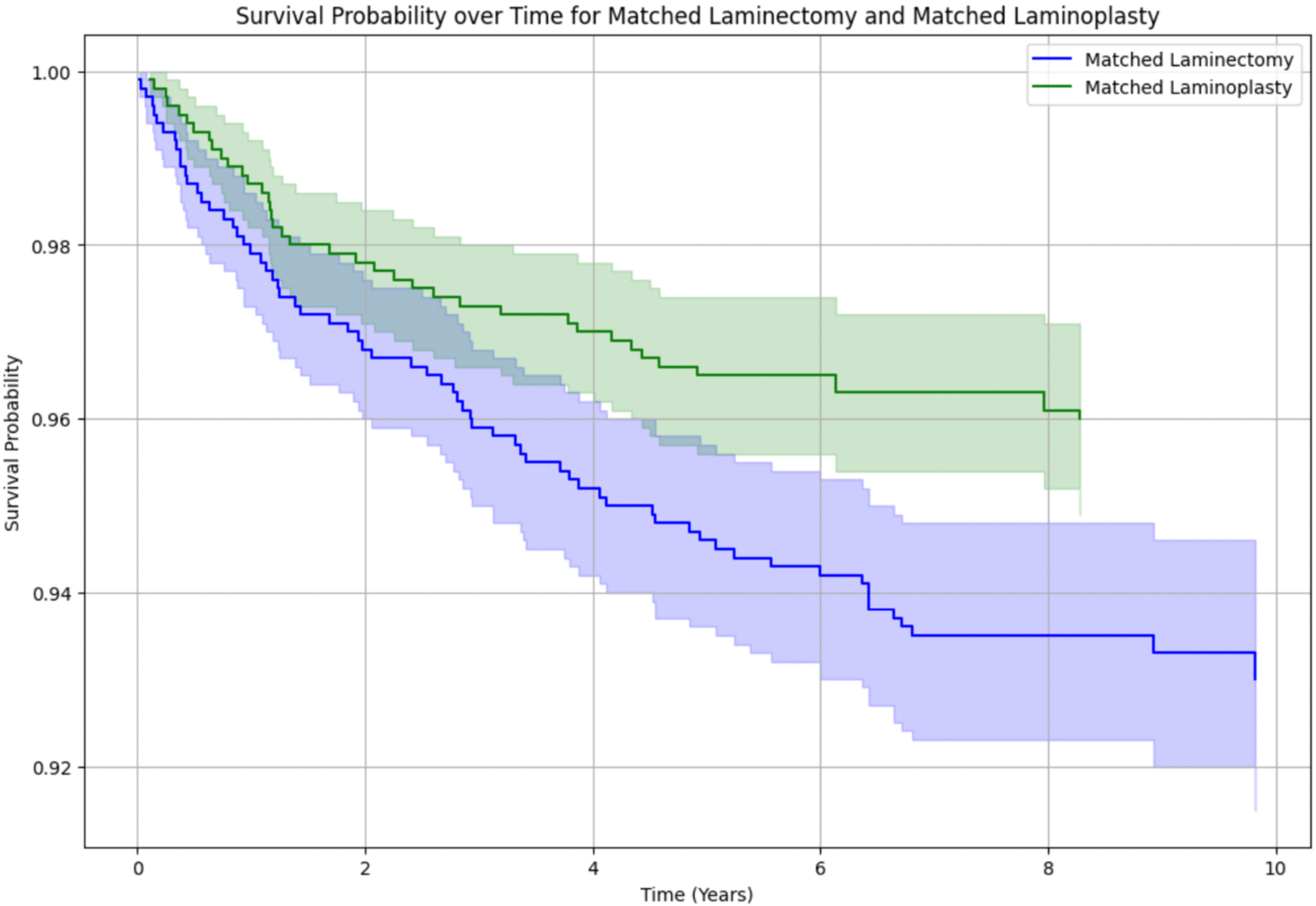
The Kaplan-Meier survival curve for matched patients following laminectomy or laminoplasty assessed time to subsequent cervical fusion surgery. The 2-year Kaplan-Meier survival curve demonstrated no significant difference in rate of subsequent cervical fusion surgery and no difference in time to reoperation between the laminectomy and laminoplasty cohorts, with a log-rank test P value of 0.92 (Figure 1). The 10-year Kaplan-Meier surgical curves demonstrated a steeper slope for the laminectomy cohort, and no significant difference in subsequent cervical fusion surgery between the 2 cohorts at 3.5 years, with a log-rank test P value of 0.23 (Figure 2). The survival probability, for both the laminectomy and laminoplasty cohorts, had the largest decline in the first 2 years following index procedure, reflecting most fusions occurring in the first 2 year post operative period. Kaplan Meier curve of survival probability for matched laminectomy and laminoplasty cohorts over 2 years. Log-Rank test demonstrated a P-value of 0.92 demonstrating no significant survival difference over 2 years between the 2 cohorts. Kaplan Meier curve of survival probability for matched laminectomy and laminoplasty cohorts over 10 years. Log-Rank test demonstrated a P-value of 0.23 demonstrating no significant survival difference over 10 years between the 2 cohorts.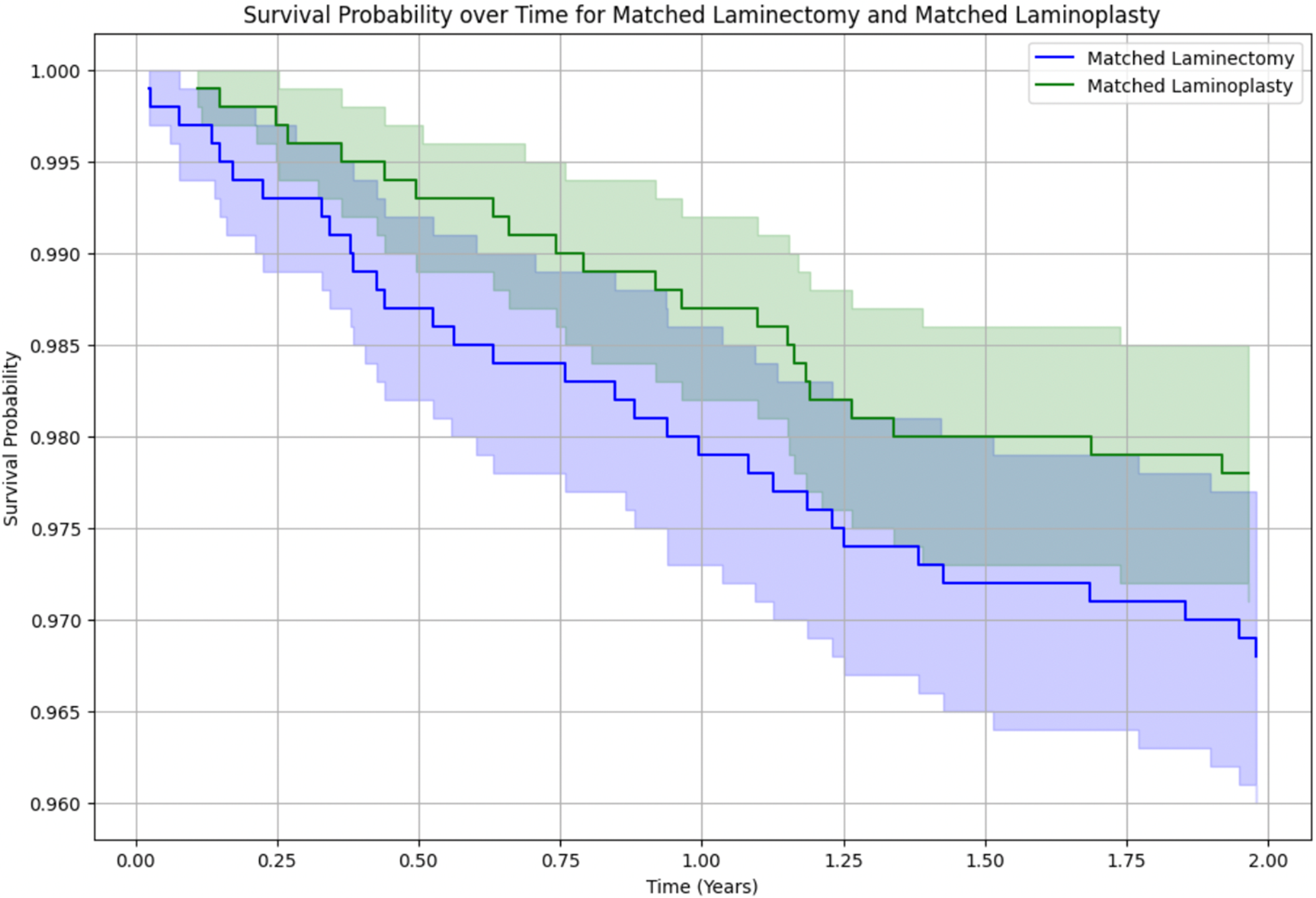
Discussion
Cervical laminectomy without fusion and laminoplasty allow for the decompression of neurological elements while maintaining motion in the cervical spine. This is the largest study comparing patient outcomes between cervical laminectomy and laminoplasty. In patients with cervical degenerative disease, we found a higher rate of subsequent fusion surgery in the laminectomy group after 3-year post-surgery.
Previous literature comparing cervical laminectomy and laminoplasty have reported conflicting results. Ishida et al, found no significant difference in pain improvement in both laminectomy and laminoplasty patients. 6 However, they reported a higher rate of postoperative kyphosis in laminectomy patients. 6 Conversely, Besnick et al. reported significantly worse neck pain and quality of life following laminoplasty compared to cervical laminectomy. 7 Post-laminoplasty axial neck pain has been reported to affect between 6%–60% of patients.8,9 Cadaveric studies have found that laminectomy significantly improved range of motion and decompression of stenosis compared to laminoplasty. 10 There are limited studies comparing long-term outcomes between cervical laminectomy and laminoplasty. In our study, we found no significant difference in subsequent fusion surgery at 2 years after surgery (laminectomy: 3.2% vs laminoplasty: 2.2%) in a matched analysis. Interestingly, while cumulative incidence analysis showed a higher rate of conversion to fusion after 3 years in laminectomy patients, Kaplan-Meier survival curves did not reach statistical significance in time-to-event comparison (log-rank P = 0.23). At 10-year after surgery, the rate of subsequent fusion surgery for laminectomy and laminoplasty were 5.5% and 3.6%, respectively.
Fusion following cervical decompression is typically indicated for insufficient decompression, kyphosis, instability, or continued neck pain. Our analysis found lower rates of postoperative fusion than previous studies. A study of 130 laminoplasty patients reported a 10-year fusion rate of 7.7%. 11 Jentzsch et al. reported a 15% revision surgery rate in 46 cervical laminectomy patients. 12 The primary concern for cervical laminectomy is development of post operative cervical kyphosis. Initial studies that fueled this concern reported postoperative kyphosis rates up to 47%. 13 However, subsequent studies have had more moderate findings ranging between 8%–14%.4,14 In addition, a measurement of alignment, while important for clinical monitoring as it can result in cord compression, does not always necessarily correlate to patient clinical outcomes or require surgical intervention. Our findings, like other more recent studies, demonstrate similar revision rates in cervical laminectomy and laminoplasty patients. 6
In our study, we found obesity to be a significant risk factor for fusion following laminectomy. Age, on the other hand, was inversely correlated with fusion for both laminectomy and laminoplasty. Other factors considered but not significantly associated with fusion risk included diabetes, tobacco use, gender, Elixhauser comorbidity index, and osteoporosis. A systematic review by Yoon et al. on risk factors impacting laminoplasty outcomes, similarly, found that age was not a risk factor for poor outcomes. 15 On the other hand, disease severity and duration of symptoms were associated risk factors. 15 It is unclear why older age is associated with reduced risk of fusion. One potential reason is the pathophysiology of cervical spondylosis. As the cervical spine degenerates reactive bone formation is observed. 16 This process results in formation of osteophytes and autofusion of the vertebral bodies.16,17 This paradoxically reduces motion in the spine and increases the stability of the cervical spine.16-18 Another potential reason is that older patients may be less likely to be offered fusion surgery after laminectomy or laminoplasty due to increased morbidity associated with cervical fusion in elderly patients. 19
A majority of the patients in our study were over 50 years of age. This age demographic reflects the primarily age driven processes of cervical degenerative disease. Prior studies on laminectomy and laminoplasty patients similarly had a study population average of 51-60 years old.20,21 Our results also indicated that while the majority of both procedures are performed in an inpatient setting, laminectomies were more commonly performed as an outpatient procedure than laminoplasties (47.7% vs 9.7%). Similarly, Olumuyiwa et al. found that from 2003 to 2014 the proportion of laminectomies performed as an outpatient procedure increased from zero to 46.7%. 22 Laminoplasties continue to be performed largely as an inpatient procedure, potentially due to increased operative time and use of instrumentation.
This study has inherent limitations similar to that of other large retrospective analysis. Firstly, our findings are limited to the accuracy to the data inputted. Although Medicare estimates provider entry error to be approximately 1.3%, 23 there is likely a wide variation in accuracy depending on the variable. For example, 1 of the major limitations with ICD codes is the unreliability of the coding. Presence or absence of an ICD code does not always correlate with whether a patient has a diagnosis clinically. For example, in this study we excluded patients with a diagnosis of cervical kyphosis, as defined by ICD-10 codes; however, there are likely patients who clinically have cervical kyphosis who may not have an ICD-10 diagnosis of cervical kyphosis in the database. Another major limitation is that the Pearldiver database lacks granular clinical and radiographic data. We were unable to determine whether the fusion surgery was at the same surgical levels as the index surgery or at an adjacent level. Additionally, we were unable to determine the indication for subsequent cervical fusion surgery, which could include iatrogenic kyphosis, adjacent segment disease, or instability. Therefore, limiting the ability to interpret the necessity for reoperation and underlying pathological mechanism leading to reoperation. We were unable to determine the precise number of laminectomy and laminoplasty levels performed, or whether individual patients underwent proximal or distal laminectomies in conjunction with laminoplasty. These factors may influence subsequent cervical fusion rates; however, we could not account for them due to limitations in the available data. While radiographic parameters could add valuable insight into how cervical alignment changes over time after these procedures and how this impacts subsequent cervical fusion surgery rates, unfortunately, radiographic data is not captured in the Pearldiver database. We acknowledge this is a major limitation. Third, consistent with its retrospective nature, this study cannot draw causative conclusions and all findings are correlative. Lastly, we are unable to control for selection bias associated with large administrative studies. However, despite these limitations, this study, to our knowledge, is the largest study comparing long-term fusion rates between cervical laminectomy and laminoplasty in the treatment of CDD. We found no difference in fusion rates at 2-year after surgery between laminectomy and laminoplasty patients. However, after 3-year we found a significantly higher rate of subsequent fusion surgery in the laminectomy cohort. Although the difference in rate of fusion was statistically significant between the 2 groups after 3-year, the rates of requiring subsequent fusion for both groups were relatively low. The 10-year rate of fusion for laminectomy and laminoplasty patients were only 5.5% and 3.6%, respectively. Our findings add to a newly growing body of literature that suggests laminectomy alone may be an appropriate surgical approach for cervical degenerative disease due to lower kyphosis and subsequent fusion rates than previously anticipated. Laminoplasty was associated with a reduced rate of subsequent fusion; however, the absolute difference compared to laminectomy alone was small.
Conclusions
In conclusion, in the treatment of cervical degenerative disease, patients who received a laminectomy had a significantly higher rate of subsequent fusion surgery starting at 3 years post procedure. However, absolute rates of fusion following laminectomy and laminoplasty remain low.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Andy Liu and Vivien Chan. The first draft of the manuscript was written by Andy Liu and Vivien Chan and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declarations
This study is IRB exempt as it uses anonymized insurance claims data.
Ethical Statement
Data Availability Statement
The data that supports the findings of this study are available from the corresponding author upon reasonable request.