
Abstract
Study Design
Retrospective Cohort Analysis.
Objectives
Extended hospital length of stay (LOS) poses a significant cost burden to patients undergoing adult spinal deformity (ASD) surgery. The purpose of this study is to investigate the relationship between late-week surgery and LOS in patients undergoing ASD surgery.
Methods
256 patients who underwent ASD surgery between January 2018 and December 2021 by a single fellowship-trained orthopedic spine surgeon comprised the patient sample. Demographics, intraoperative, and perioperative data were collected for the 256 patients who underwent ASD surgery. Patients were divided into two groups based on surgical day of the week: (1) Early-week (Monday/Tuesday) n = 126 and (2) Late-week (Thursday/Friday) n = 130. Descriptive statistics, T-tests, and linear and logistic regression models were used to analyze the data.
Results
Surgical details and sociodemographic characteristics did not differ between the groups. When controlling for TLIF/DLIF status and PSO status there was no difference in mean length of stay between the groups. The late-week group was associated with a greater risk of 30-day readmission, but there was no difference in complications, infections, or intraoperative complications.
Conclusions
We found no difference in mean length of stay between surgeries performed early in the week vs late in the week. Although late-week surgeries had higher 30-day readmission risk, all other outcomes, including complication rates, showed no significant differences. When adequate weekend post-operative care is available, we do not advise restricting ASD surgeries to specific weekdays.
Introduction
Adult spinal deformity (ASD) surgery is a complex procedure that has the potential to substantially enhance patients’ quality of life.1-6 Despite its potential benefits, ASD surgery poses a significant financial burden to both patients and the health care system of the United States. Previous studies have shown that primary ASD surgery can cost over $100,000, while revision surgeries cost around $55,000.7,8 Between 2000 and 2010, approximately $290 billion was spent on fusion-related spinal procedures in the United States. This expense is expected to rise as the prevalence of ASD increases with the country’s aging population. 9 As an example, Zygrouakis et al found that the rate of fusions for ASD increased by 273% between 2001 and 2013. 10
Hospital length of stay (LOS) is a major driver of the cost of hospitalization following ASD surgery.11,12 Additionally, extended LOS puts patients at risk of developing iatrogenic illness. Opportunistic infections, adverse side effects of medications, ulcer formation, and venous thromboembolisms have all been associated with prolonged hospital stays.13-15 As such, it is important to identify the factors that contribute to extended LOS in ASD surgery.
Surgeries performed later in the week have been associated with prolonged hospital stays in various surgical subspecialties, including total hip and knee arthroplasty and elective spine surgery.16-21 However, little is known about the impact of late-week surgery on LOS for patients undergoing ASD surgery. A better understanding of this relationship could help reduce both the financial burden and risk of iatrogenic illness associated with extended LOS. Hence, the purpose of this study is to provide novel information on the effects of late-week ASD surgery on LOS by comparing demographics, surgical details, and post-operative outcomes between patients undergoing early vs late-week surgery.
Methods
Data Source and Collection
Data was collected from a retrospective chart review of patients undergoing ASD surgery at a single institution by a single fellowship-trained orthopaedic spine surgeon. This study was approved by the Institutional Review Board (00006727) with a waiver for informed consent. 377 ASD surgeries were performed between January 2018 and December 2021. 256 surgeries were included (>18 years old, non-traumatic, non-revision of index procedure during study period). 121 surgeries were excluded: (88) revision surgery, (16) pediatric population, (8) fracture, (8) extended length of stay (greater than fifteen days), (3) infection. Patients with extended hospital stays were considered outliers, as it is unlikely that such a prolonged hospital course could be explained by surgical day alone. They were excluded to prevent skewing of the data.
Patients were divided into two groups based on surgical day of the week: (1) Early-week surgeries (Monday/Tuesday) and (2) Late-week surgeries (Thursday/Friday). No surgeries were performed on Wednesdays or over the weekend. There were no indications for doing certain procedures on specific days. Baseline demographic variables were collected such as age, gender, smoking status, body mass index (BMI), Charlson Comorbidity Index (CCI) score, and American Society of Anesthesiology (ASA) class. Intraoperative factors were collected including operating room (OR) time, the number of fusion levels, whether the surgery was a revision of a another procedure prior to the study period, the use of Smith Peterson Osteotomy (SPO), the number of SPO levels, the use of pedicle subtraction osteotomy (PSO), the use of transforaminal lumbar interbody fusion (TLIF) or direct lateral interbody fusion (DLIF), the number of interbody fusions, intraoperative complications, and estimated blood loss (EBL). Hospital LOS was collected as the primary outcome measure. 30-day and 1-year postoperative readmission rates, unplanned revision surgery rates, complication rates, and infection rates were collected as secondary outcome measures. All major and minor complications were based on criteria established by Glassman et al. 22
Statistical Analysis
Differences in baseline patient demographics, ASA classification, CCI score, and comorbidity rates in patients with early-week and late-week surgeries were detected using bivariate analyses, with categorical variables being assessed using Chi-squared tests and parametric continuous variables with Student t tests. To control for different rates of diabetes mellitus, as well as differing proportions of TLIF, DLIF and PSO surgeries among patients with early-week and late-week surgeries, multivariate regression models were constructed for our outcome measures of interest (length of hospital stay, interoperative complication rate, 30-day complication, readmission, and infection rates, and 1-year complication rate). Logistic regression models were used to predict binary outcome variables and linear regression models were used to predict parametric continuous outcome variables. These models included predictor variables accounting for DM status, TLIF and PSO surgeries, as well as early-vs-late week status. Results from the logistic regression models are reported as odds ratios (OR), and results from linear regression models are reported as t-statistics. Statistical significance was set at P < .05. All analyses were carried out in Matlab R2022b.
Results
Patient Demographics
Sociodemographic characteristics and comorbidities of study sample (by early-vs-late week).
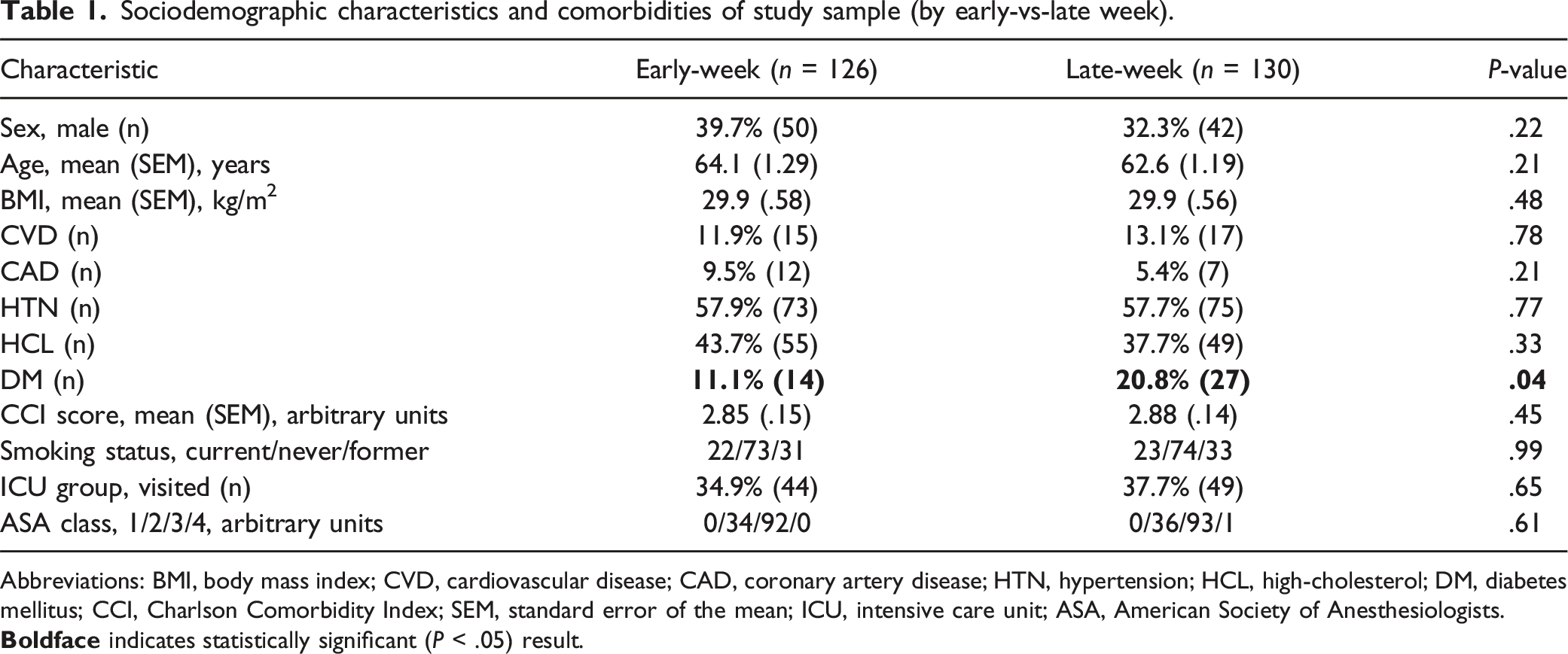
Abbreviations: BMI, body mass index; CVD, cardiovascular disease; CAD, coronary artery disease; HTN, hypertension; HCL, high-cholesterol; DM, diabetes mellitus; CCI, Charlson Comorbidity Index; SEM, standard error of the mean; ICU, intensive care unit; ASA, American Society of Anesthesiologists.
Surgical Details
Surgical procedure variables in study sample (by early-vs-late week).
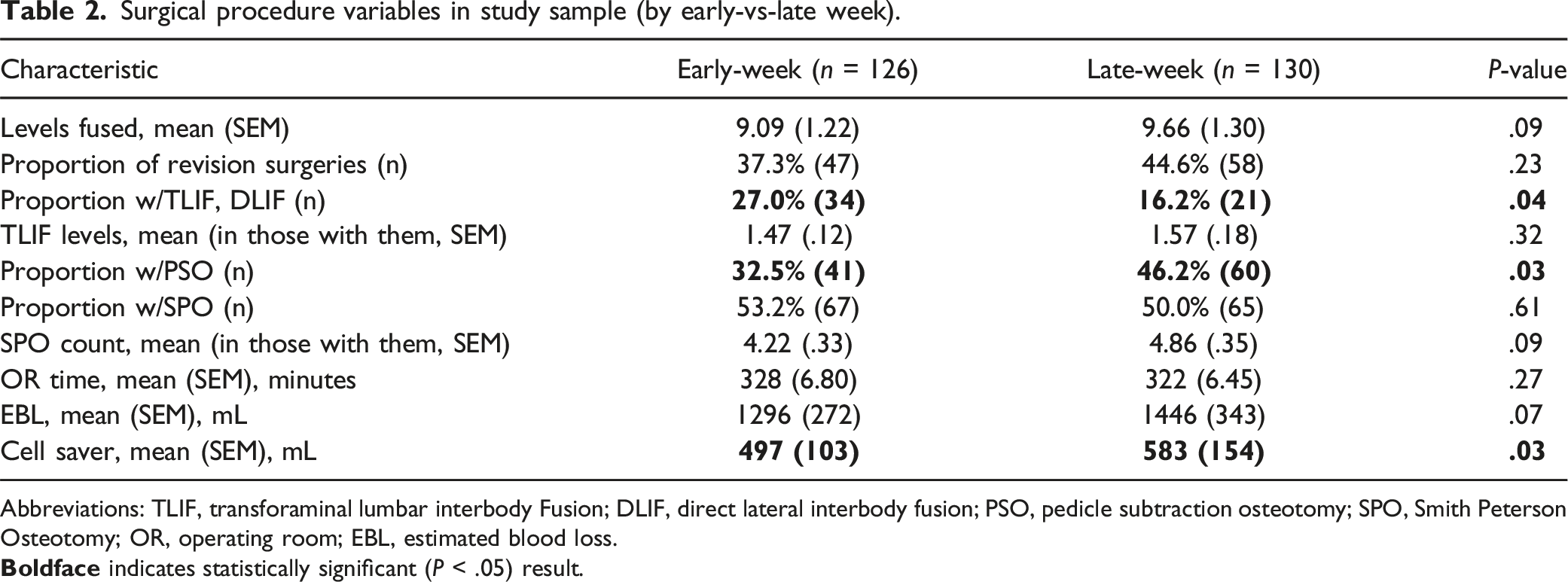
Abbreviations: TLIF, transforaminal lumbar interbody Fusion; DLIF, direct lateral interbody fusion; PSO, pedicle subtraction osteotomy; SPO, Smith Peterson Osteotomy; OR, operating room; EBL, estimated blood loss.
Post-Operative Outcomes
Surgical outcome variables in study sample (by early-vs-late week).
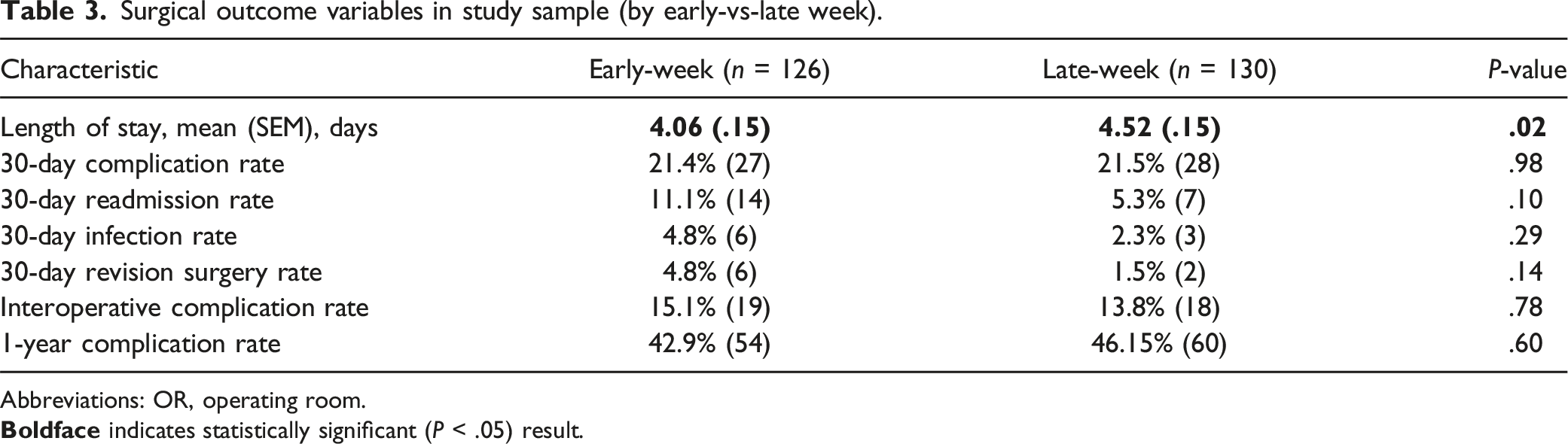
Abbreviations: OR, operating room.
11.1% of patients (n = 14/126) in the early-group were readmitted to the hospital within 30-days of surgery: PE or DVT (4), infection (3), pain (3), constipation (2), fall (1), cirrhosis (1). 5.3% of patients (n = 7/130) in the late-week group were readmitted to the hospital within 30-days of surgery: PE or DVT (2), UTI (1), infection (2), weakness (1), clostridium difficile. (Table 3).
Predicting selected surgical outcome variables with linear/logistic regression models.
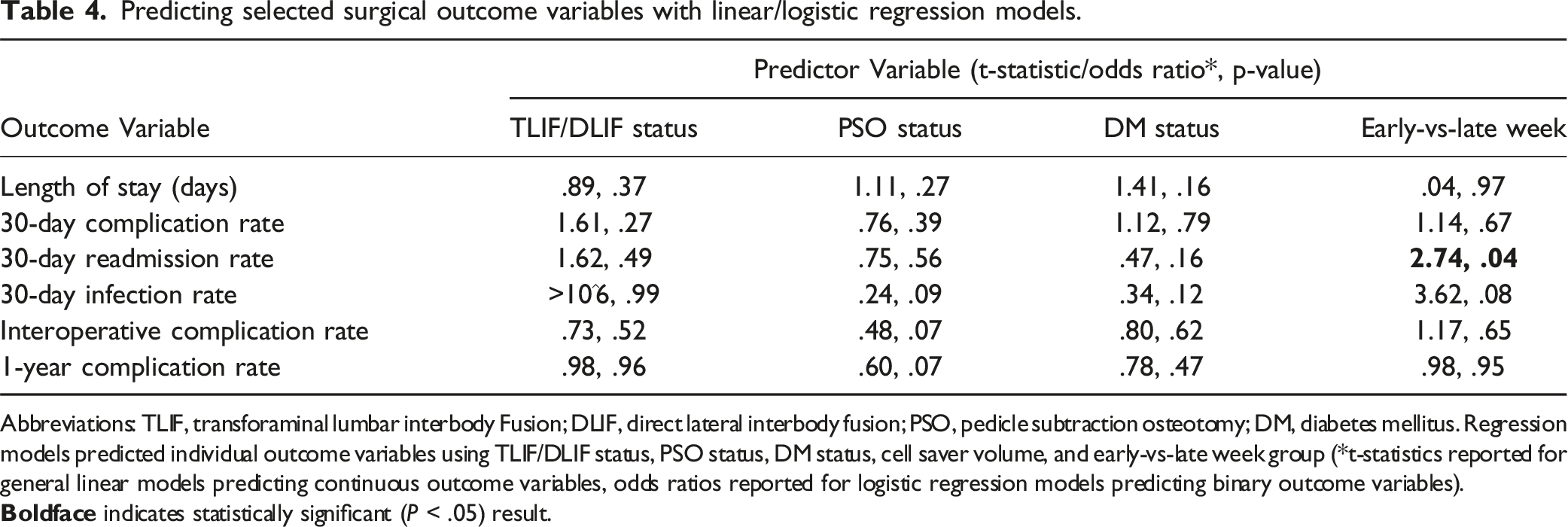
Abbreviations: TLIF, transforaminal lumbar interbody Fusion; DLIF, direct lateral interbody fusion; PSO, pedicle subtraction osteotomy; DM, diabetes mellitus. Regression models predicted individual outcome variables using TLIF/DLIF status, PSO status, DM status, cell saver volume, and early-vs-late week group (*t-statistics reported for general linear models predicting continuous outcome variables, odds ratios reported for logistic regression models predicting binary outcome variables).
Discussion
ASD surgery is a complicated procedure that can improve a patient’s quality of life, while also posing a significant financial burden on the patient and the health care system. Extended hospital stays are a major contributor to the cost burden of surgery, with each inpatient day typically averaging between $1200 and $4,000, according to Kaiser State Health facts. 23 Additionally, hospitalization carries an increased risk of developing iatrogenic disease.13-15 As such, it is important to identify the factors that contribute to prolonged hospital stays in ASD surgery. In other surgical specialties, late-week surgery has been associated with extended hospital LOS. It is unclear if this phenomenon occurs in ASD surgery. Accordingly, this study aimed to investigate the relationship between late-week surgery and extended hospital LOS following ASD surgery.
Before controlling for differences in baseline surgical characteristics, we did see greater lengths of stay for patients undergoing surgery later in the week. This results is unsurprising since there were more complex surgeries (PSOs) performed later in the week. However, after controlling for differences in baseline surgical characteristics, our study found no difference in hospital LOS between patients who had early-week vs late-week surgery (t-statistic −.08, P > .05). This suggests that the initial difference was likely a factor of having more complex surgeries later in the week and not surgical day of the week itself.
Dinizo et al previously investigated whether the specific day of the week on which surgery was performed impacted post-operative outcomes in 1040 patients undergoing ASD surgery. They found no association between surgical day of the week and hospital LOS or 90-day complication, readmission, or reoperation rates after controlling for patient and case characteristics. 24 Similar to their study, we performed a sub-analysis with each day of the week modeled as a categorical variable and found no difference LOS and post-operative complication rates between each specific day of the week.
However, Dinizo et al did not dichotomize surgeries into early-week and late-week groups for comparison. Additionally, the patients in their sample underwent surgery performed by a diverse set of surgeons, which raises the possibility that the reported outcomes could have been influenced by the specific days on which each surgeon operated. Our study has a key advantage: all surgeries were performed by a single, experienced orthopedic spine surgeon. Furthermore, by distinguishing between “early week” and “late week” surgeries, we were able to provide crucial insights for surgeons who don’t operate daily, but instead, perform surgeries both early and later in the week.
Other studies in the orthopedic literature have also reported a lack of association between late week surgeries and extended LOS. Khechen et al investigated the relationship between late-week surgery and post-operative outcomes following anterior cervical discectomy and fusion. Their study included 153 patients in the early-week (Tuesday) group and 142 patients in the late-week (Friday) group. There was no difference in hospital LOS, post-operative complications, or hospital costs between the two groups (30.1 hours vs 30.5 hours and 11.8% vs 9.2% and $8157 vs $7,985, P > .05). 25 Rathi et al performed a retrospective study of 273 patients who underwent total hip arthroplasty and found no significant difference in length of stay for patients who underwent surgery on Monday vs Friday (3.7 days vs 3.8 days, P > .05). 26 Similarly, Pakzad et al. retrospectively reviewed 343 patients who underwent ankle fusion or total ankle replacement and found that patients who underwent surgery on Friday had a similar length of stay to patients who underwent surgery earlier in the week (P > .05). 27
In contrast to our findings, other studies in the orthopedic literature found late-week surgeries to be associated with extended hospital LOS. Sivaganesan et al investigated the effect of surgical day of the week on LOS for 11,897 patients undergoing lumbar surgery. Among patients discharged home, patients undergoing surgery on Friday had significantly higher odds of longer LOS as compared to Monday (OR = 1.36, P < .001). Among those discharged to a facility, patients undergoing surgery on Wednesday, Thursday, and Friday had significantly higher odds of longer LOS as compared to Monday. 20 Keswani et al studied the effects of surgical day of the week on post-operative outcomes in 580 patients undergoing total hip arthroplasty. The early-week cohort had a significantly lower LOS than the late-week cohort (3.7 days vs 3.4 days, P < .05). 28 Similarly, Muppavarupu et al found that patients undergoing total joint arthroplasty on Thursday and Friday had significantly longer LOS when compared to Monday and Tuesday. 18
Numerous theories have been proposed in attempt to explain the relationship between late-week surgery and extended LOS. Patients undergoing ASD surgery require extensive post-operative physical therapy to prevent major complications and promote mobilization. It has been theorized that reduced staffing of physical therapists on the weekend can delay mobilization and preparedness for discharge.19,28 Additionally, many patients undergoing ASD surgery require discharge to a rehabilitation facility. Disposition to rehabilitation facilities may be delayed by a relative lack of resources required for coordinating transfer on the weekends. 20 For example, patients who undergo late-week surgery may have to wait longer for discharge if the necessary paperwork is not initiated during the weekend or if the rehabilitation facility does not accept patients on the weekend. Our findings suggest that any potential staffing issues during the weekend did not affect our cohort of patients undergoing ASD surgery. As such, we do not recommend limiting ASD surgery to specific days of the week in cases where these resources can be adequately provided on the weekend.
Our study showed that late-week ASD surgery had no effect on 30-day and 1-year complication rates after controlling for differences in baseline surgical characteristics. The late-week group was associated with a greater risk of readmission within 30-days (OR 2.78, P < .04). The overall complications rates reported in this study are comparable to that found in the literature.29-31 Accordingly, we do not recommend modifying surgical day of the week to reduce overall post-operative complications following ASD surgery.
Our study is not without limitations. First, the retrospective nature of our study could contribute to some degree of selection and reporting bias. While we controlled for differences in baseline demographics and surgical differences, we did not account for differences in severity of spinal imbalance. However, our consideration of baseline demographics and surgical characteristics should help reduce variability in the severity of imbalance. Next, this study was performed at a single-institution by a single-surgeon, and our findings might not hold true at other institutions where access to postoperative resources is more limited on the weekend. However, our findings are more generalizable in demonstrating the feasibility of operating both early and late in the week as long as post-operative protocols are standardized throughout the weekend. Also, our study did not investigate surgeries performed over the weekend, as these surgeries are not routinely performed over the weekend at our institution. Future studies would need to be performed at other institutions to examine the outcomes of ASD surgeries performed over the weekend. Next, our study did not look at hospital costs associated with early vs late-week ASD surgery, and additional studies would be needed evaluate the cost implications of surgical day of the week. Finally, our study did not track postoperative outcomes beyond 1-year. Future studies should look examine the effect of late-week surgery on long-term outcomes in patients with ASD.
Conclusion
ASD surgery is a complex procedure that requires extensive postoperative physical therapy and mobilization to prevent major complications. In other orthopedic procedures, late-week surgeries have been associated with extended hospital LOS. After controlling for differences in baseline and perioperative variables, we found no difference in mean length of stay between surgeries performed early in the week vs late in the week. While the late-week group was associated with a greater risk of readmission at 30 days, there was no significant difference in other outcomes including 30-day complication rate, 30-day infection rate, intraoperative complication rate, or one year complication rate. We attribute these findings to extensive postoperative physical therapy and mobilization for our patients, even during the weekend. In cases where sufficient postoperative care can be provided during the weekend; we do not recommend limiting ASD surgeries to specific days of the week. Prospective multicenter studies with a larger sample size should be done to further evaluate the effects of early vs late week surgery on long-term post-operative outcomes following ASD surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.