
Abstract
Study Design
Modified DELPHI Consensus Process
Objective
To agree a single unifying term and definition. Globally, cervical myelopathy caused by degenerative changes to the spine is known by over 11 different names. This inconsistency contributes to many clinical and research challenges, including a lack of awareness.
Method
AO Spine RECODE-DCM (Research objectives and Common Data Elements Degenerative Cervical Myelopathy). To determine the index term, a longlist of candidate terms and their rationale, was created using a literature review and interviews. This was shared with the community, to select their preferred terms (248 members (58%) including 149 (60%) surgeons, 45 (18%) other healthcare professionals and 54 (22%) People with DCM or their supporters) and finalized using a consensus meeting. To determine a definition, a medical definition framework was created using inductive thematic analysis of selected International Classification of Disease definitions. Separately, stakeholders submitted their suggested definition which also underwent inductive thematic analysis (317 members (76%), 190 (59%) surgeons, 62 (20%) other healthcare professionals and 72 (23%) persons living with DCM or their supporters). Using this definition framework, a working definition was created based on submitted content, and finalized using consensus meetings.
Results
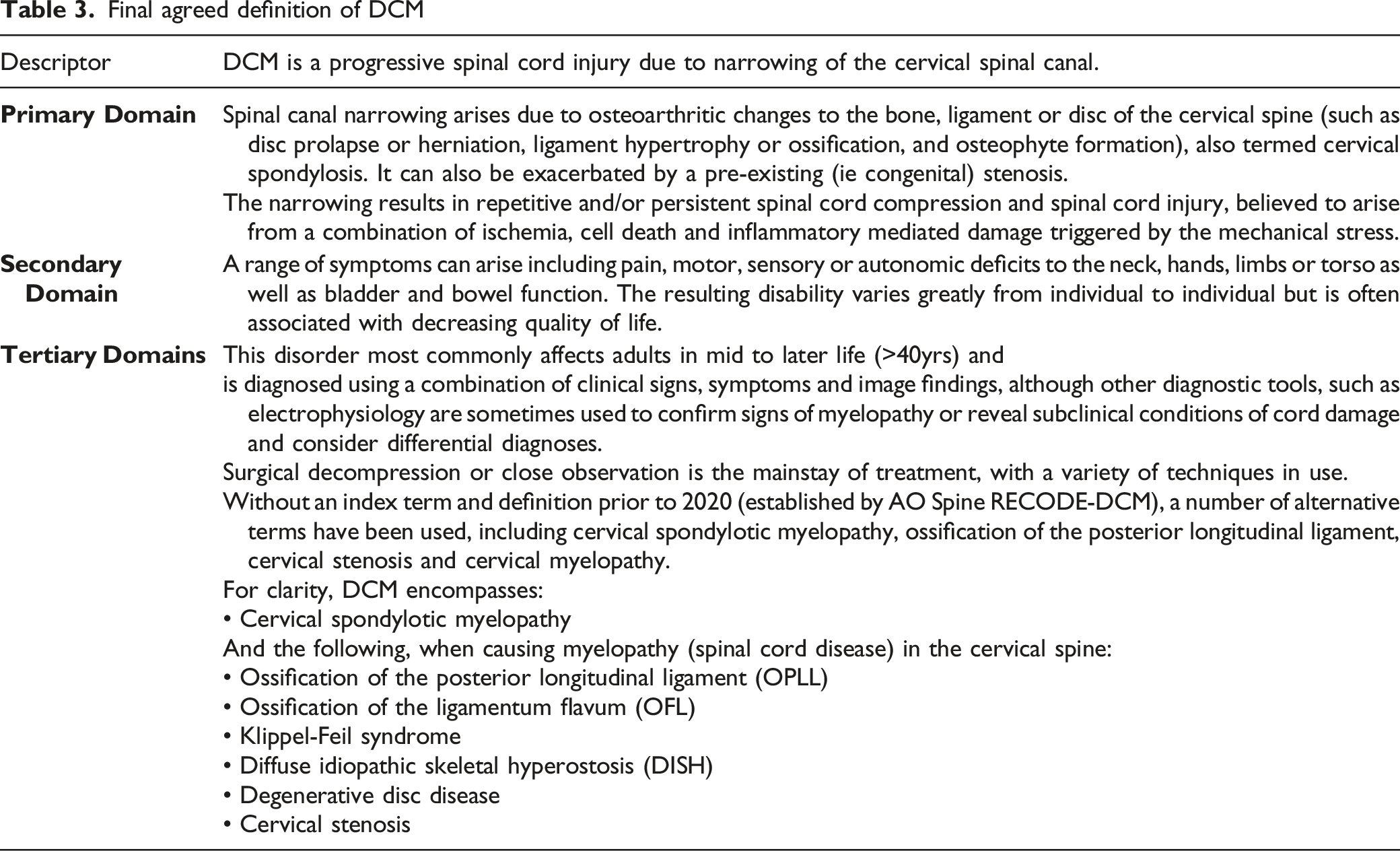
Degenerative Cervical Myelopathy was selected as the unifying term, defined in short, as a progressive spinal cord injury caused by narrowing of the cervical spinal canal
Conclusion
A consistent term and definition can support education and research initiatives. This was selected using a structured and iterative methodology, which may serve as an exemplar for others in the future.
Keywords
Introduction
Imagine trying to diagnose, treat, research, or educate in a disease without a common name. Degenerative cervical myelopathy (DCM), is a progressive spinal cord injury 1 estimated to affect 1 in 50 adults; 2 it is a heterogeneous condition known by at least 11 different names. 3 DCM is the most common form of cervical myelopathy 4 triggered by degenerative and/or congenital changes to the structure of the cervical spine that exert mechanical stress on the spinal cord and result in a progressive spinal cord injury. 5
The condition was first recognized in 1839 by C Aston-Key, 6 encompasses multiple spinal pathologies, and is referred to as: cervical spondylotic myelopathy, cervical stenosis, ossification of the posterior longitudinal ligament, non-traumatic spinal cord injury and cervical degenerative myelopathy and other conditions. These terms lack definitions and are variable used.7,8
This, and low awareness or comprehension of the disorder, 9 even amongst health professionals, 10 contributes to the challenges DCM patients face: DCM is often undiagnosed, or diagnosed late, which can result in delay of care, often by years.1,2,11,12 As DCM is often progressive, treatment must be optimally timed to offer maximal patient benefit.11,13 These delays therefore translate into greater disability, dependency, and some of the poorest quality of life scores of any chronic disease.11–14
The approach to naming and defining disease is much debated, including what even constitutes a disease.15–19 However, no standardized framework has emerged. Diseases can be known by descriptive terms or proper nouns, including eponymous names. 20 Definitions too are variable, ranging from a description of common symptom patterns to those incorporating the findings of diagnostic tests and/or aetiology. 21
The approach to defining disease has often been classed as either essentialist or nominalist. 22 The former indicates a true certainty to a disease (X is….), whereas the latter reflects a description that remains open to interpretation.15,23 In reality these represent 2 opposite ends of a spectrum. JG Scadding, from whom many of these perspectives arose, favored a more nominalist approach, acknowledging its flexibility to handle uncertainty or as yet unknown facts. The definition of the disease in this context is distinct from its diagnostic criteria,16,18 and traditionally focusses on anatomical and physiological features. 16 Disease nomenclature was historically driven by professionals; however, more recently lasting terminology has been closely influenced by the perspective of patients and families. 20
This article outlines a multistakeholder consensus process to agree a single name and definition for cervical myelopathy caused by degenerative spinal column pathology (AO Spine RECODE DCM). 24
Method
This individual project is part of a wider initiative called the AO Spine RECODE-DCM (aospine.org/recode), for which the protocol has been published.
24
This defined 3 key stakeholder groups: spinal surgeons, other healthcare professionals (oHCP), and DCM patients or carers (PwCM).
25
The project was overseen by an international steering committee (Supplementary Data 1), but day-to-day by a management group. Ethical approval was granted by University of Cambridge. The process is summarized in Figure 1. Overview of process to agree a single index term and definition.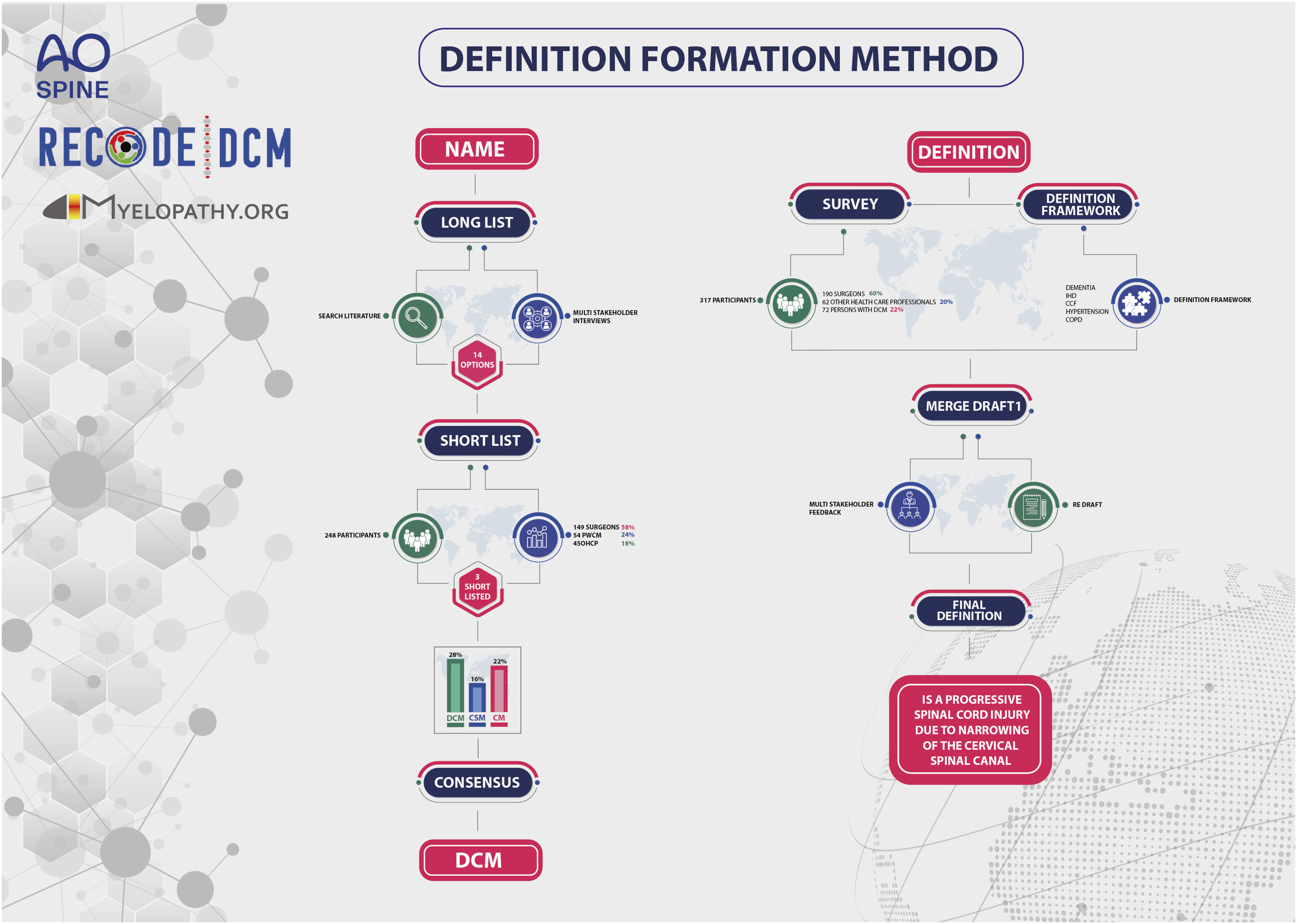
Index Term
A list of candidate terms was taken from the literature using a scoping review of 2 clinical trial registers (Clinicaltrials.gov and EU Trials) and MEDLINE (Supplementary Data 2). An inclusive search was built around the terms ‘Cervical’ and ‘Myelopathy’ based on prior validated filters.26,27 The search was performed from database inception to 1st December 2019. MEDLINE articles were searched for systematic reviews or meta-analysis, clinical trial protocols or clinical practice reviews. These latter sources were selected on the basis that preferred disease terms would most likely have been named and defined. In total, 11 different terms were used in the clinical trials registry and 7 different terms in the published literature. These were supplemented during discussion at a steering committee meeting into a longlist of 14 different and unique terms.
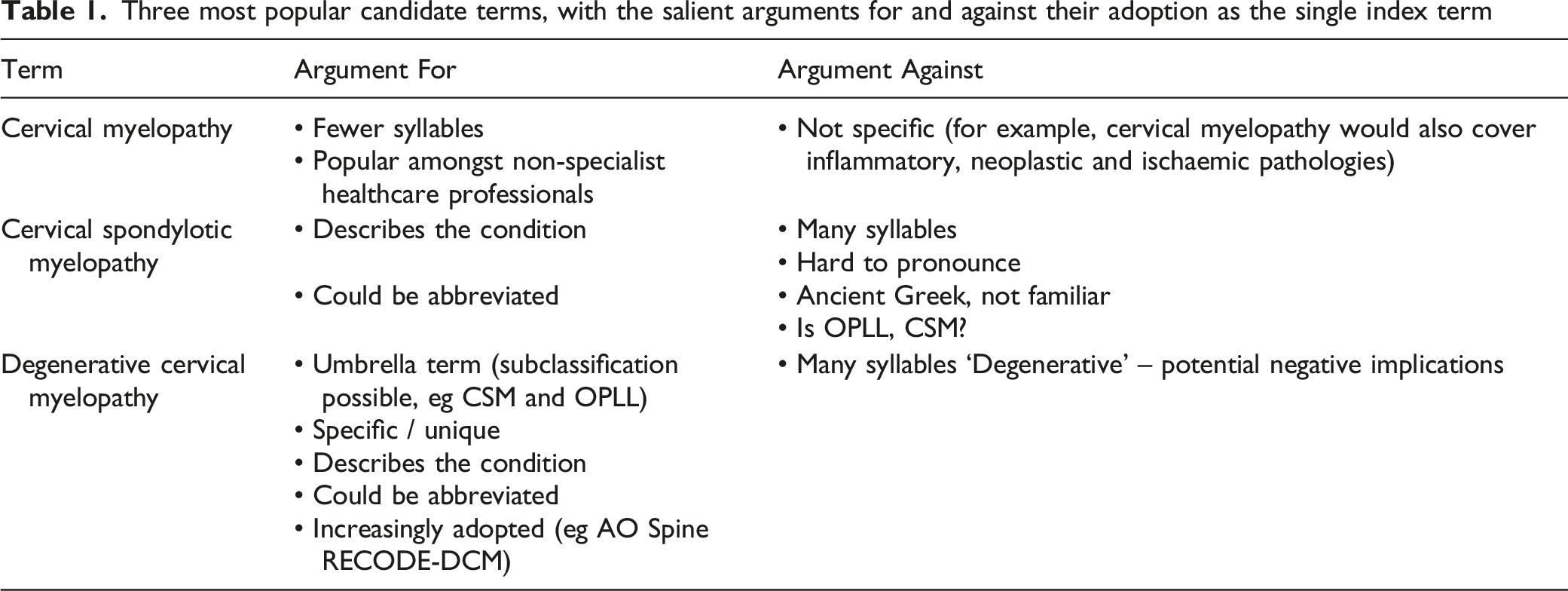
A mixed methods approach was taken to establish potential drivers of individual preference. Quantitative analysis of the scoping review identified ‘cervical spondylotic myelopathy’ (‘CSM’) as the most common term used (51%), with ‘degenerative cervical myelopathy’ (‘DCM’) the second most common (19%). The use of ‘DCM’ was only found in the published literature after its proposal by Nouri et al (2015), 8 increasing from 0% to 27%. However, this was predominantly within neurosurgical publications (95%) and by authors with affiliations to those individuals on the original manuscript (70%).
Three most popular candidate terms, with the salient arguments for and against their adoption as the single index term
These findings were used to form a series of infographics (Supplementary Data 3), incorporated into a survey (SurveyMonkey, California USA) and distributed to the AO Spine RECODE-DCM community (see below). Following review of the infographics, participants were asked to select their preferred term. The sequence in which participants viewed the infographics was randomly allocated to minimize bias. Participants were given the option to justify their selection using a comment box, but also a list of predefined reasons identified during interviews. Results were descriptively analyzed. Free text responses underwent inductive analysis. Findings of the survey were then reviewed at a quorate AO Spine RECODE-DCM steering committee meeting, for a final consensus decision, chaired by an independent facilitator.
The AO Spine RECODE-DCM community is an international network of professionals and people with lived experience. It was originally formed at the start of AO Spine RECODE-DCM, to conduct a James Lind Alliance research priority setting partnership and form a minimum data set for research. The detailed recruitment process and sampling demographics are described separately.
Definition
A medical definition framework was formed by inductive analysis of existing definitions held within the International Classification of Disease (ICD) register. The ICD register was chosen as a reference framework, on the basis that it is an international standard employed around the world and an intended target for dissemination.28,29 A choice of 10 general and well-known conditions were selected by the management group, specifically: congestive heart failure, cerebral ischemic stroke, chronic obstructive pulmonary disease, chronic insomina, diabetes, dementia, cirrhosis, pneumonia, hypertension and osteoarthritis. In addition, 5 conditions, within the ICD register, more closely related to myelopathy (multiple sclerosis, amyotrophic lateral sclerosis, hereditary spastic paraplegia, syringomyelia and transverse myelitis) and spondylosis (spondylolisthesis, spinal stenosis, intervertebral disc degeneration of the cervical spine without prolapsed disc, inflammatory spondyloarthritis and rheumatoid arthritis) were also selected.
Their respective definitions were extracted from ICD, version 11 and underwent inductive analysis by an individual with no prior knowledge, or experience of DCM or AO Spine RECODE-DCM (KB). This was felt important to avoid the introduction of any pre-conceptions. The principal objective was to identify a framework for a definition’s structure. Differences and technical nuances between types of definition were also compared.
As part of the second-round survey of the AO Spine RECODE-DCM Priority Setting Partnership, participants were asked to select their top research priorities (termed ‘interim prioritisation’), as well as to submit their definition of DCM. The survey was hosted on SurveyMonkey (California, USA) and was disseminated to participants of the first-round survey, but also via a single open call through AO Spine and Myelopathy.org.
Data was imported into NVivo software (version 10, 2012; QSR International Pty Ltd, Victoria, Australia) and underwent pre-processing. Specifically, spelling mistakes corrected, duplicate words combined (eg bodily and body) and conjunctions or prepositions removed. The principal focus was nouns, as these would provide the descriptive content for the definition. Adverbs and adjectives underwent context analysis and were included with their partner noun if they were considered of relevance to interpreting it (eg ‘decreased function’ or ‘significant compression’). These processed words then underwent inductive analysis, to identify a framework of categories that effectively sorted all submitted words. This was completed by 2 reviewers (BMD, and DZK) independently, with any disagreement settled through mutual discussion. Reviewers were not aware at the time of the definition framework based on ICD definitions.
The identified frameworks were then merged (ICD framework, and DCM framework), and using the content from submitted descriptions, a working definition formed by the AO Spine RECODE-DCM management group. The definition was then presented for discussion and feedback at a quorate AO Spine RECODE-DCM steering committee meeting, chaired by an independent facilitator. A process of iteration and re-review continued, until a quorate consensus had been reached.
Results
Index Term
Of the 417 registered email addresses, 248 individuals responded (58% participation) including 54 (22%) PwCM , 149 (60%) surgeons, and 45 (18%) oHCP, with worldwide representation (Supplementary Data 4). With the exception of ‘Ossification of the Posterior Longitudinal Ligament’ (OPLL), all terms received at least 1 vote. CSM, DCM and cervical myelopathy were the 3 most popular terms, across key stakeholder groups (Supplementary Data 5). Thematic analysis of free text comments left by 41 respondents (19 [46%] Surgeons, 13 [32%] PwCM or their supporters and 9 [22%] oHCP) identified 4 prevailing themes, categorised as “Momentum” (for DCM) (3 [7%]), “Against Degenerative” (3 [7%]), in favour of “Simple Language” (4 [10%]) and in favour of a “Specific Term” (7 [17%]) (Figure 2, Supplementary Data 6). On 2nd November 2020, a virtual consensus meeting was convened to agree the index term. The meeting was attended by 17 representatives (7 Surgeons, 4 oHCP and 6 PwCM) and chaired by an independent facilitator. The pre-meeting process and findings were presented. Comments were invited, which were unanimously in favor of the most popular term ‘DCM’, for reasons of momentum, specificity, simple terminology, and an easier-to-say acronym. The term was selected by poll, with 100% support. Radar plot, outlining the common arguments and their relative frequency amongst the 3 shortlisted index terms.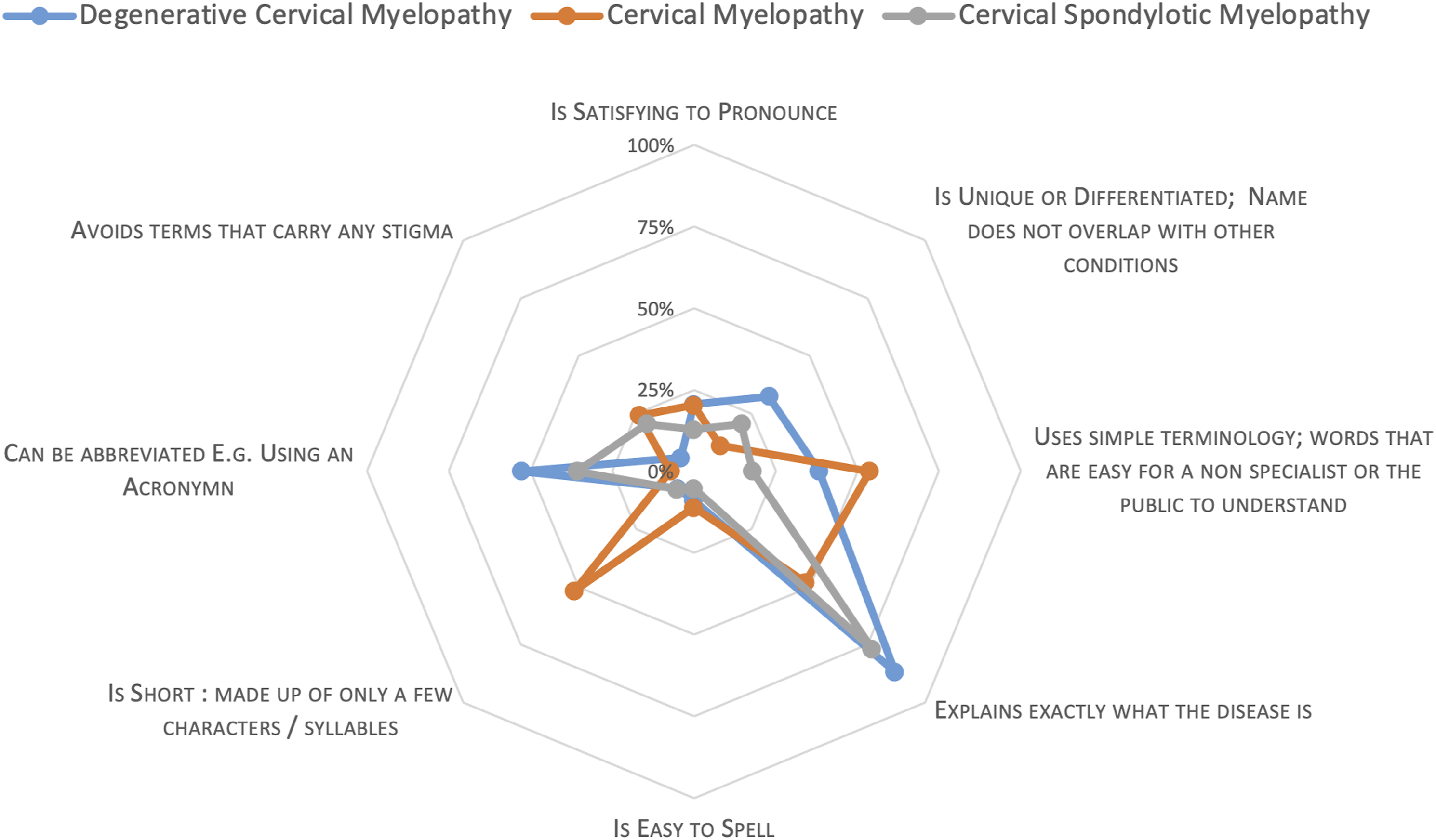
Thematic Analysis of Existing Disease Definitions
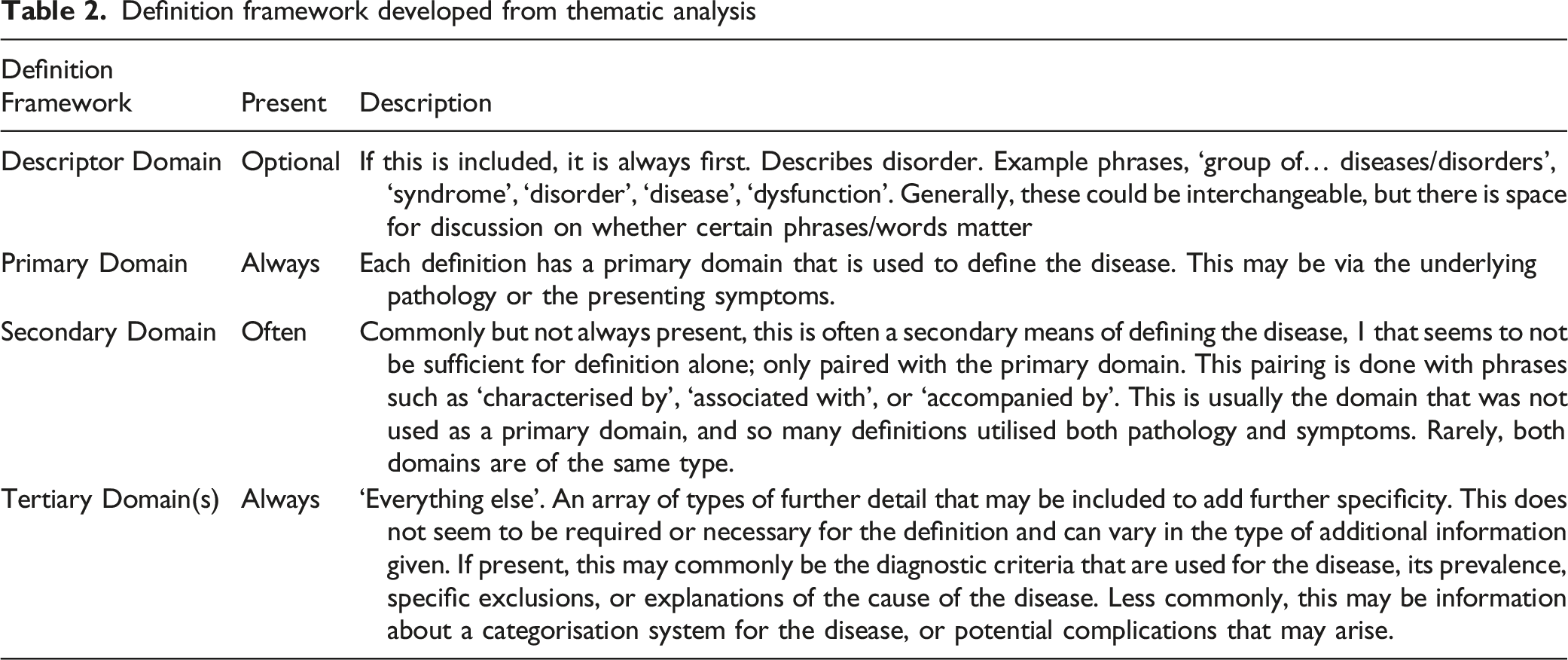
Definition framework developed from thematic analysis
Selecting a Definition for Degenerative Cervical Myelopathy
Of the 417 participants who performed interim prioritisation, 317 (76%) completed the definition question, specifically 190/214 (89%) Surgeons, 62/96 (65%) oHCP and 72/107 (67%) persons living with DCM or their supporters.
Across groups, ‘spinal’, ‘cord’ and ‘compression’ were consistently prevalent terms, and to a lesser extent ‘degenerative’. Other common descriptors included reference to examination findings (eg ‘signs’, ‘findings’, ‘motor’, ‘sensory’) and investigations (eg ‘imaging’, ‘MRI’ or ‘electrophysiology’). The choice of words, and their popularity, appeared consistent between stakeholder groups.
Content was grouped independently by 2 reviewers, into themes with or without sub-themes. The process was iterative, with informal discussion used to resolve inconsistencies and develop a framework that was able to categorise content across descriptions that is shown in Supplementary Data 8. Specifically, themes of pathology, impact, population, diagnosis and treatment were identified. When subsequently comparing this to the framework identified from general condition definitions, the DCM framework was well aligned: primary (pathology), secondary (impact) and tertiary domains (population, diagnosis and treatment).
Final agreed definition of DCM
Discussion
AO Spine RECODE DCM has used a modified DELPHI process, informed by the literature and broad international and multistakeholder perspectives, to agree a single index term and produce its first consensus definition. This appears consistent with definitions used for existing conditions and based on the process, suitable for inclusion within ICD. 30
Whilst there were significant strengths to the process, including its global 31 multistakeholder perspective and iterative approach, an important limitation to acknowledge is that the term ‘DCM’ was used from the outset, for example within the supporting and explanatory information, as well as the project title AO Spine RECODE-DCM, as having a term to identify the condition was unavoidable. The inclusion of contrasting terms, alongside their prominence within voting and discussion, is a reassuring suggestion at least, that this did not confer an unconscious bias.
The term DCM was introduced by Nouri et al (2015). 8 The authors had deliberately proposed a new term to reconcile a history of confusion for the disease.32,33 Although first described in 1839, 6 the distinction of DCM from related neurological disease was difficult until its aetiology had been better defined. DCM was initially proposed to be the result of chondromas, 34 however these were subsequently recognized instead as intervertebral disc prolapses 35 The spectrum of related pathology that could cause spinal canal narrowing and injury was extended, and collectively termed ‘spondylosis’; the condition often called ‘cervical spondylosis with myelopathy’, which later became ‘cervical spondylotic myelopathy’. 36 However the term ‘spondylosis’ remained poorly defined and variably interpreted 7 . OPLL for example was considered by some as a distinct entity and others just 1 of the spectrum of pathologies that can cause cervical spondylotic myelopathy. 7 Both views have their basis. For example OPLL has been observed more frequently amongst Asian populations, with several candidate gene mutations linked to its development.37,38 However OPLL frequently co-exists with other degenerate pathology, 39 the clinical phenotype and operative goals are also the same. 5 Moreover its prevalence amongst non-asian populations may-be underrecognized. 40 As Nouri et al (2015) first proposed, this is therefore more likely an important subtype of a common disease. 8 The European League against Rheumatism in 1995 recommended moving away from ‘spondylosis’ in any context due to this collective ambiguity. 41 For DCM, where congenital pathology, such as congenital cervical stenosis or Klippel Fleil syndrome can also contribute, 42 this problem is likely amplified.8,39
Whilst resolving this ambiguity underpinned this initiative, the eventual selection of DCM specifically, was informed by more specific arguments that emerged during the modified DELPHI process. Firstly, as a condition with widespread under-recognition, capitalising on an increasing momentum shift since its proposal 8 (for example with international guidelines 43 ) was considered prudent. Further as a new term, it did not carry any legacy of misinterpretation. This would obviate the need to change existing views (for example on the definition of CSM), instead presenting a new solution 44 which would still be recognised as a disease (as opposed to a syndrome such as ‘cervical myelopathy’). Finally, the term ‘degenerative’ was popular amongst PwCM. Whilst there were concerns raised by professionals about the impact that such terms can have on patient expectation and engagement with rehabilitation, 45 PwCM felt it faithful to their disease and likely to help them bring acknowledgement of its implications to a lay audience, who can often underestimate their disability. 46
These arguments have precedent from other conditions. For example, the selection of a new name or definition has been used to re-educate around a condition. 20 An ongoing example is that of the International Association for the Study of Pain’s efforts to redevelop the classification of chronic pain, which has subsequently entered ICD version 11 with positive endorsements.29,47,48 Likewise the choice of terminology has implications for how a disease is perceived or prioritised.19,49,50 Whilst previous evidence has suggested this is more likely for descriptive terms (“chronic fatigue”) as opposed to those that are perceived as a disorder (“chronic fatigue syndrome”), this is also informed by the perception of the disease itself, with chronic conditions, affecting multiple systems, of uncertain aetiology and without treatment or requirement for a doctor, less likely to be prioritised.51–53 An example of well adopted change is overactive bladder syndrome, previously known as ‘urinary incontinence’ or ‘detrusor instability’. 54 Here its combined recognition as a disorder that could be easily interpreted contributed to a dramatic change in awareness. 55 This was likely well supported by industry and the arrival of new medical therapies.55,56
This therefore indicates that the terms themselves still require a definition to guide their interpretation. Our definition has attempted to reconcile the need to offer clarification on what DCM is (an essentialist approach) with the acknowledgement that exactly what defines DCM remains uncertain (a nominalist approach). Striking this balance is important, to ensure the definition can remain timeless and relevant. Whilst subclassification of DCM is undoubtedly relevant, the knowledge to inform such a taxonomy is yet to be determined. 5 Spinal disorders in general have likely suffered from adoption of an essentialist approach. The advent of imaging has enabled detailed visualisation of structural changes to the spine, which have become represented within ICD frameworks given their anatomical basis. 21 Often this pathology however is incidental, but its recognition will still lead to its attachment to an individual. A recognisable example is disc degeneration and lower back pain,57,58 which as evaluated in a recent trial from North America, may have detrimental implications for their outcomes. 59
DCM is a condition with many critical uncertainties. Creating a single unifying term, with a more nominalist definition should help address these. However, for this to occur, the next challenge will be ensuring widespread adoption. One hopes that the inclusive and iterative approach taken here, alongside the strong rationale for adopting a single term, will give the community confidence in its choice and aid implementation.60,61 However, additional measures will likely be crucial, such as its integration within ICD framework.20,22
Conclusions
A global, multistakeholder consensus process involving those with lived experience has selected DCM as the single unifying term for a progressive spinal cord injury due to narrowing of the cervical spinal canal.
Supplemental Material
Supplemental Material - We Choose to Call it ‘Degenerative Cervical Myelopathy’: Findings of AO Spine Research objectives and Common Data Elements Degenerative Cervical Myelopathy, an International and Multi-Stakeholder Partnership to Agree a Standard Unifying Term and Definition for a Disease
Supplemental Material for We Choose to Call it ‘Degenerative Cervical Myelopathy’: Findings of AO Spine Research objectives and Common Data Elements Degenerative Cervical Myelopathy, an International and Multi-Stakeholder Partnership to Agree a Standard Unifying Term and Definition for a Disease by Benjamin M. Davies, Danyal Z Khan, Kara Barzangi, Ahmad Ali, Oliver D. Mowforth, Aria Nouri, James S. Harrop, Bizhan Aarabi, Vafa Rahimi-Movaghar, Shekar N Kurpad, James D. Guest, Lindsay Tetreault, Brian K. Kwon, Timothy F Boerger, Ricardo Rodrigues-Pinto, Julio C. Furlan, Robert Chen, Carl Moritz Zipser, Armin Curt, James Milligan, Sukhivinder Kalsi-Rayn, Ellen Sarewitz, Iwan Sadler, Shirley Widdop, Michael G. Fehlings, and Mark R.N. Kotter in Global Spine Journal
Footnotes
Acknowledgements
This study forms part of a wider initiative to accelerate knowledge discovery that can improve outcomes in degenerative cervical myelopathy. This initiative was organized and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international spinal cord injury experts. More information can be found at ![]() . AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
MRNK is supported by the National Institute for Health Research (NIHR) Brain Injury MedTech Co-operative based at Cambridge University Hospitals NHS Foundation Trust and University of Cambridge, and BMD a NIHR Clinical Doctoral Research Fellowship. DZK is supported by an NIHR Academic Clinical Fellowship. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
This report is independent research arising from a Clinician Scientist Award, CS-2015-15-023, supported by the National Institute for Health Research. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.