
Abstract
Study Design
Retrospective case-control study.
Objectives
The purpose of this study is to assess whether cannabis use disorder (CUD) patients undergoing primary 1- to 2-level lumbar fusion (1-2LF) for the treatment of degenerative lumbar spine disorders have higher rates of: (1) in-hospital lengths of stay (LOS), (2) medical complications, and (3) healthcare expenditures.
Materials and methods
A retrospective case-control study of the MSpine dataset of the PearlDiver claims from January 2007 to March 2018 was performed. Patients with CUD undergoing 1-2LF were queried and matched to a comparison group in a 1:5 ratio by age, sex, and various medical comorbidities yielding 22, 815 patients within the study (CUD = 3805; control = 19 010). Outcomes analyzed included LOS, 90-day medical complications, and costs. A P-value less than .004 was considered significant.
Results
This study found CUD patients undergoing primary 1-2LF experience longer in-hospital LOS (4- vs. 3-days, P < .0001). Additionally, CUD patients were found to have significantly higher frequency and odds-ratios (OR) (31.88 vs. 18.01% OR: 1.41, P < .0001) of adverse events within ninety days following their procedure. CUD patients also had significantly higher day of surgery ($18,946.79 vs. $15,691.02, P < .0001) and 90 days healthcare expenditures ($21,469.01 vs. $19,556.71, P < .0001).
Conclusion
Patients with CUD can prepare for increased LOS, complications, and costs following primary 1-2LF. The study can be used to educate these patients of the potential outcomes following their procedure.
Keywords
Introduction
Increased cannabis or marijuana usage can be attributed to increased legalization, decreased public stigma, and increased availability for medical and recreational use.1,2 Global substance abuse studies reported 3.8% of the global population and 12.4% of the North American population aged 15 to 64 years old use cannabis in 2015. 2 Studies analyzing cannabis use show that the prevalence has doubled from 2002 to 2013 and that nearly 3 out of 10 users experience cannabis use disorder (CUD). 3 The term CUD was also included in The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) from the American Psychiatric Association and combines both cannabis dependance and abuse. 4 Per the DSM-V, CUD is further defined as a problematic pattern of cannabis use leading to clinically significant impairment or distress occurring within a 12-month period, cannabis is consumed in larger amounts or over a longer period of time, persistent desire or unsuccessful efforts in consumption, a great deal of time is spent in activities associated with obtaining cannabis, and continued use despite having persistent or recurrent social or interpersonal problems exacerbated by cannabis use. 5 With increased cannabis abuse among the United States population, it is essential to understand its further effects on disease states and surgical outcomes. While neurologic effects of cannabis have been studied extensively, new research focuses on pain management and recreational use. Cannabis for orthopedic patients has largely been used for management of musculoskeletal pain, specifically back pain. 6 A study of the National Inpatient Sample (NIS) from 2011 to 2015, showed that 247 949 chronic pain patients were cannabis users, and that cannabis use increased from .57% to 1.2% among patients with spondylosis in these 4 years alone. 7 Increased recreational use, potential for abuse, and prevalence of CUD highlights the need to analyze its affects specifically from an orthopedic surgery lens.
Studies about CUD and outcomes in orthopedic patients are limited and contradictory, most focusing only on use rather than abuse and rarely about spine procedures.7,8 A 2019 study demonstrated that peri-operative outcomes were similar in patients who used marijuana compared to non-marijuana users undergoing transforaminal lumbar interbody fusion (TLIF) performed by the same surgeon. Limitations of this study included the study being underpowered, being limited only to patients within their institutional patient registry, and marijuana use was self-reported by patients—which could potentially be underreported. 9 Other recent studies on cannabis as an alternative analgesic following orthopedic procedures yields unconvincing results making it is still unclear how to give patients standard dosing recommendations for cannabis as pain therapy.6,10-12 This encourages more unregulated recreational use for orthopedic pain and can increase abuse and CUD among patients over time.
The lack of literature showing the association of cannabis use disorder (CUD) and peri-operative complications following lumbar fusion surgery highlights the need for analyses and assessment, especially considering the increasing trends of cannabis use in patients with back pain. 13 Therefore, the purpose of this study is to assess whether CUD patients undergoing primary 1- to 2-level lumbar fusion (1-2LF) for the treatment of degenerative lumbar spine disorders have higher rates of: (1) in-hospital lengths of stay (LOS), (2) 90-day medical complications, and (3) healthcare expenditures.
Materials and Methods
Database
A retrospective level III case-control study of the MSpine dataset of the PearlDiver claims (PearlDiver Technologies, Fort Wayne, Indiana, United States) from January 1, 2007 to March 31, 2018 was performed. The PearlDiver database houses records of over 100 million patients from either the Mariner claims or the Medicare Standard Analytical Files (SAF). Due to the extensive number of patients housed within the database, PearlDiver has been used extensively for spine-related research and other orthopedic subspecialities. The database is reliant on a syntax-based language which uses International Classification of Disease, Ninth Revision (ICD-9), ICD-10, Current Procedural Terminology (CPT), National Drug Codes (NDC), and Diagnosis Related Group (DRG) codes. Information is subsequently downloaded as a Microsoft Excel (Microsoft Corporation, Redmond, Washington, United States) for further data analyses. As this information contains deidentified information, the study was deemed exempt from our institution’s Institutional Review Board (IRB) approvals process.
Cohorts
Patients who underwent primary lumbar fusion were initially identified using ICD-9 procedural codes 81.04 to 81.08. From this cohort, patients who underwent 1- to 2-level fusions were filtered using procedural code 81.62. The dataset was then queried for all patients who had degenerative lumbar spine conditions at the time of surgery using ICD-9 diagnostic codes: 722.10, 722.51, 722.52, 722.73, 724.02, 724.03, 738.4. Patients who had CUD were identified using ICD-9 diagnostic codes 304.31, 304.32, 305.21, and 305.22. Using Boolean command parameters (“AND,” “OR,” “NOT”), the inclusion for the study group consisted of patients who underwent primary 1-2LF who have CUD; whereas, patients without CUD served as the comparison cohort. Exclusions for the study included those patients who were undergoing surgery for trauma, infections, malignant etiologies, revision procedures, or any concomitant surgeries involving the cervical or thoracic areas, as described in previously published studies utilizing the same database.
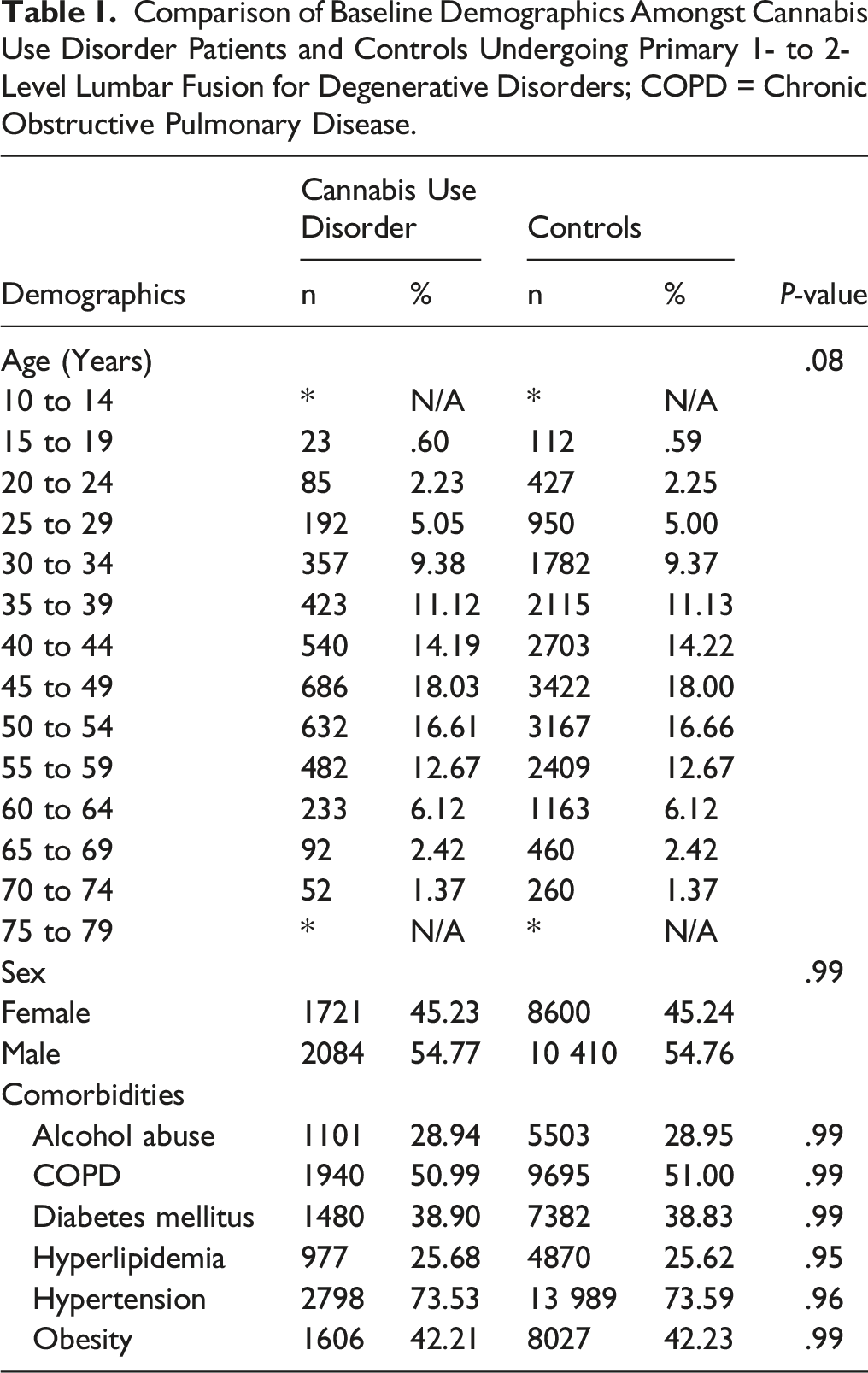
To reduce any potential confounding, study group cohorts were matched to a comparison group in a 1:5 ratio by age, sex, and the following medical comorbidities—alcohol use disorder, chronic obstructive pulmonary disease (COPD), diabetes mellitus, hyperlipidemia, hypertension, and obesity. Ratio matching was done to increase the overall sample size of the study to ensure the investigation was adequately powered for its analysis. These comorbid conditions were chosen as they have been commonly associated with CUD.
Study Endpoints
Endpoints of the study were to compare in-hospital LOS, medical complications, and healthcare expenditures. Ninety-day medical complications analyzed included acute kidney injuries, cerebrovascular accidents, deep vein thromboses, disruption of wound, hematomas, ileus episodes, myocardial infarctions, pneumoniae, respiratory failures, transfusion of blood products, urinary tract infections (UTIs), and venous thromboembolisms (VTEs). Healthcare expenditures were compared using reimbursement data from the database, as done in previously published studies. Economic data is aggregated from the time point of surgery up to a specified time interval per the researcher’s interest. Information collected can include prescription refills, physical therapy sessions, diagnostic tests, or procedures, as described by Cortez et al. Ninety days was chosen for the time interval of interest for the medical complications and healthcare expenditures as this is the defined time interval period set in place by the Center of Medicare and Medicaid Services.
Data Analyses
Demographic information of the two cohorts was compared using Pearson’s chi-square analyses or Fischer’s exact test, when applicable. It should be noted that PearlDiver provides age as a categorical variable and as such, the aforementioned data analyses were used to test for statistical significance between the two cohorts. In-hospital LOS and healthcare expenditures were compared using Welch’s t-tests. The association of CUD on medical complications were performed using multivariate logistic regression analyses adjusting for age, sex, geographic region, and the Elixhauser-Comorbidity Index (ECI). While studies generally utilize the Charlson-Comorbidity Index (CCI), ECI was used as the index contains twice as many comorbid conditions and has been shown to be a more accurate predictor of mortality following orthopedic procedures. Due to the ease of finding statistical significance with large database studies, Bonferroni-corrections were performed to reduce the probability of a type I error. As such, a statistically significant P-value was set at less than .004. This was calculated by taking .05 by the total number of comparisons made (n = 12). All statistical analyses were performed using R (R, Foundation for Computational Statistics; Vienna, Austria).
Results
Sample Size and In-Hospital Lengths of Stay
Comparison of Baseline Demographics Amongst Cannabis Use Disorder Patients and Controls Undergoing Primary 1- to 2-Level Lumbar Fusion for Degenerative Disorders; COPD = Chronic Obstructive Pulmonary Disease.
Medical Complications and Healthcare Expenditures
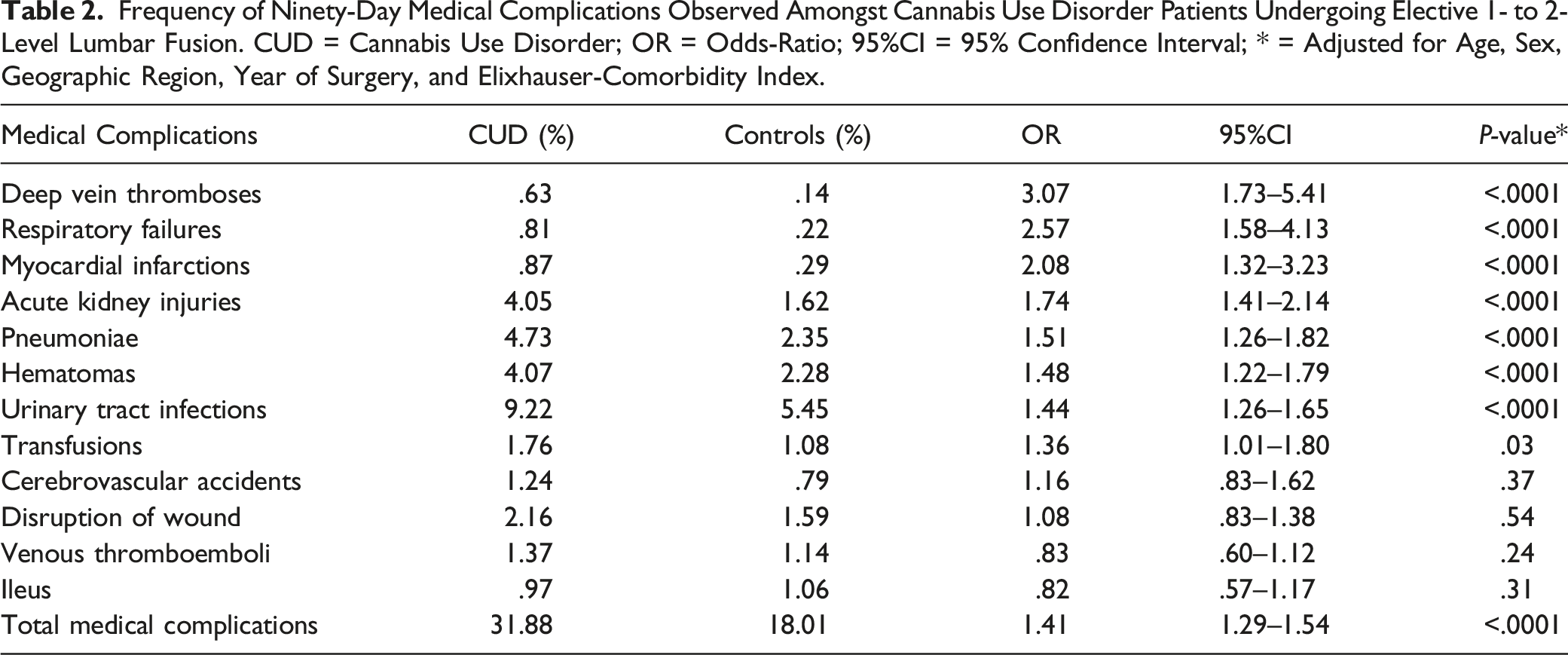
Frequency of Ninety-Day Medical Complications Observed Amongst Cannabis Use Disorder Patients Undergoing Elective 1- to 2-Level Lumbar Fusion. CUD = Cannabis Use Disorder; OR = Odds-Ratio; 95%CI = 95% Confidence Interval; * = Adjusted for Age, Sex, Geographic Region, Year of Surgery, and Elixhauser-Comorbidity Index.
Discussion
With more states decriminalizing cannabis possession and legalizing recreational use, prevalence of cannabis use will increase and have significant effects on the healthcare system, society, and the US economy.1,3,4,14-17 Studies evaluating the association of CUD on postoperative outcomes following primary 1-2LF are sparse. The purpose of this retrospective analysis was to utilize a large administrative claims database of private insurance claims to determine the impact of CUD on in-hospital LOS, medical complications, and healthcare expenditures on patients undergoing primary 1-2LF for degenerative lumbar disc disorders. Following randomized matching, this study shows CUD patients undergoing primary 1-2LF experience longer in-hospital lengths of stay, higher rates of medical complications, and have higher healthcare costs.
The results of this study coincide with the results of other previously published studies.18-21 This present study shows CUD patients have higher length of hospital stay following primary 1-2LF surgery (4- vs. 3-days, P < .0001). Chiu et al. 22 performed a study of the NIS from 2012 to 2015 and found that patients with CUD stayed in the hospital for nearly 2 more days compared to their counterparts following elective spine surgery, which combined decompression, fusion, and refusion. CUD is also shown to significantly increase LOS from 3 days to 4 days in other orthopedic procedures including primary total hip arthroplasty. 20 Although several studies have evaluated the relationship between CUD and LOS in patients undergoing various orthopedic surgeries, this study is the first to establish the correlation in CUD patients undergoing primary 1-2LF specifically. Given that cannabis use disorder and the number of primary 1-2LF procedures are both rising, future research should explore this trend further.
In addition to longer in-hospital LOS, this study showed CUD to be associated with higher rates of developing medical complications within 90 days following the index procedure (OR: 1.41, P < .0001). Specifically, it showed CUD to be associated with higher rates of cardio-pulmonary related complications such as deep vein thromboses (OR: 3.07, P < .0001), respiratory failure (OR: 2.57, P < .0001), and myocardial infarctions (OR: 2.08, P < .0001). These results support outside literature that has found increased rates of medical complications associated with cannabis use and CUD, largely cardiac, vascular, and respiratory issues. An NIS study by Moon et al. 23 from 2010 to 2014 demonstrations that for spinal fusions, cannabis use was associated with increased odds of stroke and cardiac disease. However, this study only looked at cannabis use, while the present study analyzes abuse and dependence. Additionally, the analysis of NIS from 2012 to 2015 by Chiu et al. 22 showed that active CUD patients undergoing any elective spine surgery, were found to have significantly worse postoperative respiratory complications (OR:2.0, P < .001), thromboembolic events (OR:2.2, P = .005), sepsis (OR:1.5, P = .031), and neurologic complications (OR:2.9, P = .007). This study combined decompression, fusion, and refusion under their analysis of elective spine surgery, while the current study only included 1-2LF patients. These CUD associated medical complication findings have also been significant in patients undergoing other orthopedic surgical procedures. Vakharia et al. 20 showed increased medical complications for CUD patients undergoing total hip arthroplasty and found a significantly higher incidence of pneumonia (OR:2.3, P < .001), respiratory failure (OR:2.2, P < .001), and cerebrovascular accidents (OR:2.3, P < .001). Additionally, Vakharia et al. found CUD patients have increased rates of developing VTEs within 90 days following their primary total knee arthroplasty which includes DVTs (OR: 1.68; P < .0001) and PEs (OR:1.58; P = 01). 19 These supporting results are especially significant given increasing cannabis use in patients with musculoskeletal pain.6,11,12 Our study further demonstrates cannabis use disorder has significant cardio-pulmonary and hematologic affects in orthopedic patients.24-27 Increased complications require frequent, expensive procedures and a longer stay following the initial surgery, which can contribute to the increased costs associated with CUD patients.
This study showed that CUD 1-2LF patients had significantly increased costs on their day of surgery and within 90 days following their procedure compared to controls (P < .0001). Costs associated with significant medical complications vary by study and have been evaluated individually, but they are not specific to 1-2LF procedures. Discharge summaries from orthopedic patients from 220 US hospitals showed that mean total costs of inpatient care were almost 2-fold higher for patients with VTEs, an additional $17,114 for DVTs only. 28 Furthermore, an international acute myocardial infarction registry showed the mean cost for MI hospitalization was found to be $9993 in the US. 29 A case-control study of elective orthopedic surgery patients who developed unanticipated respiratory failure necessitating transfer to the ICU showed that patients had an excess of $26,571 average hospitalization costs compared to controls. 30 These studies display costs that CUD patients are at risk of accumulating in addition to the expenditures of the 1-2LF procedure because of the high rate of associated medical complications. Additionally, Flisberg et al. showed that cannabis users needed increased pain medication administered to ensure proper anesthesia in surgery, which could also add to these accumulative costs.27,31 The present study supports the literature about increased healthcare expenditures for CUD patients undergoing surgery and highlights the importance of research on spinal procedures specifically 1-2LF.
Limitations of this study could be in the database used, as cannabis use is self-reported, which can cause a population in our controls with unreported or undiagnosed CUD, which could potentially underestimate the association of CUD on the dependent variables assessed within this investigation. The method of consumption (i.e., aerosolized inhalation or ingestion), strain, volume, and frequency were also not accounted for in the database, as studies with greater potency could be directly correlated with the incidence of complications observed within the study cohort. While the study relied on diagnostic coding to identify our cohorts, currently there is no information as to when recreational use of cannabis progresses to CUD unless patients meet the criterion for CUD per the DSM-V. Additionally, while CUD is defined by behavioral patterns within a 12-month period, the diagnosis does not rely on a specific quantified metric of cannabis use. As such, this could potentially introduce potential confounding within the study. Both could affect physiologic properties of patients, thus underestimating the medical complications and cost studied here. This study is also dependent on accurate diagnostic coding on behalf of physicians. With any administrative database, the patient cohorts are reliant on the accuracy of these codes, which can potentially skew patients into a cannabis use group rather than the CUD cohort. Additionally, while there are more than one insurance claims database for patients within the United States, this study analyzed a single claims registry, and the results of the study may not be generalizable to all patients within the United States. Due to the retrospective nature of the study, only an association can be made on the impact of CUD on the dependent variables which were analyzed within the investigation. To determine the relationship of CUD on in-hospital LOS, frequency of postoperative complications, and healthcare burden—large prospective randomized control trials would be needed. Despite these limitations, the literature evaluating the association of CUD on postoperative outcomes following spine surgery are limited. This report is the first to specifically study 1-2LF in CUD patients and offer significant insight into outcomes in patients who have CUD.
Conclusion
This study shows that patients with cannabis use disorder undergoing primary 1- to 2-level lumbar fusion experience longer in-hospital lengths of stay, have higher healthcare expenditures, and present with significantly higher rates of complications. Patients with cannabis use disorder can prepare for increased lengths of stay and costs, and physicians can council their patients about the effects of cannabis use disorder and prepare in advance for the increased chance of complications prior to surgery. As new research about the prevalence of cannabis use among patients with chronic pain emerges, it is essential to understand the impact that cannabis use disorder poses on patients undergoing orthopedic procedures considering increased legalization, use, and abuse among the United States population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB Approval: The study was exempt from our institution’s Institutional Review Board (IRB) approval process.