
Abstract
Study Design
Systematic Review
Objective
To perform a systematic review assessing the relationship between functional somatic syndromes (FSSs) and clinical outcomes after spine surgery.
Methods
A systematic review of online databases (PubMed and Web of Science) through December 2021 was conducted via PRISMA guidelines to identify all studies investigating the impact of at least one FSS (fibromyalgia, irritable bowel syndrome (IBS), chronic headaches/migraines, interstitial cystitis, chronic fatigue syndrome, multiple chemical sensitivity) on outcomes after spine surgery. Outcomes of interest included patient reported outcome measures (PROMs), postoperative opioid use, cost of care, complications, and readmission rates.
Results
A total of 207 records were identified. Seven studies (n = 40,011 patients) met inclusion criteria with a mean MINORS score of 16.6 out of 24. Four studies (n = 21,086) reported postoperative opioid use; fibromyalgia was a strong risk factor for long-term opioid use after surgery whereas the association with chronic migraines remains unclear. Two studies (n = 233) reported postoperative patient reported outcome measures (PROMs) with mixed results suggesting a possible association between fibromyalgia and less favorable PROMs. One study (n = 18,692) reported higher postoperative complications in patients with fibromyalgia.
Conclusion
Patients with fibromyalgia and possibly migraines are at higher risk for prolonged postoperative opioid use and less favorable PROMs after spine surgery. There is limited research on the relationship between other Functional somatic syndromes (FSSs) and outcomes following spine surgery. Growing evidence suggests the variation in outcomes after spine procedures may be attributed to non-identifiable organic patient factors such as FSSs.
Introduction
Functional somatic syndromes (FSSs) are conditions in which physical symptoms cannot be fully explained by an established medical disorder. Historically, FSSs were broken down into somatic symptoms such as pain and fatigue. These common symptoms accounted for approximately 400 million outpatient clinic visits in the United States in 1989.1,2 The term “functional somatic syndromes” was first described by Barsky et al in 1999 as “several related syndromes that are characterized more by symptoms, suffering, and disability than by disease specific, demonstrable abnormalities of structure or function”. 3 These conditions often involve chronic pain and include fibromyalgia (FM), chronic fatigue syndrome, irritable bowel syndrome (IBS), chronic whiplash, interstitial cystitis, tension headaches, and others.3-5 While the pathophysiology of FSSs remains unclear, patients with FSSs tend to have worse health outcomes, significant disability, higher healthcare costs, and greater pain than those without FSSs.3,6-12 For example, patients with FM have higher healthcare utilization and are more likely to retire early due to disability than patients without FM. 9
The relationship between FSSs and outcomes after spine surgery is currently unclear. A growing body of evidence suggests that patients with specific FSS conditions experience worse outcomes and greater pain following arthroplasty procedures.6,13-16 However, examining the association between one condition and outcomes instead of considering FSSs a group of conditions may hinder our understanding of this association. Since patients with these conditions tend to have similar risk factors and symptoms, researchers have argued that these conditions should be grouped together and viewed as a continuum.3-5,17
The aim of this study was to perform a systematic review assessing the relationship between FSSs and outcomes after spine surgery. We looked at 6 diagnoses - fibromyalgia, irritable bowel syndrome, chronic headaches, interstitial cystitis, chronic fatigue syndrome, and multiple chemical sensitivity - that constitute FSSs. We hypothesized that the presence of at least one FSS is associated with worse patient reported outcome measures (PROMs) and greater opioid use after these procedures.
Materials and Methods
This study includes a systematic review of literature conducted according to guidelines from the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 18 Due to the nature of this study being a systematic review, informed consent or Institutional Review Board approval were not necessary.
Eligibility Criteria and Search Strategy
Online databases (PubMed and Web of Science) were used to identify clinical studies examining the relationship between at least one FSS and clinical outcomes after spine surgery. Two authors (R.M., M.F.) independently completed the search of the literature published from 1955-2021 that examined the relationship between at least one FSS and clinical outcomes after spine surgery. The inclusion and exclusion criteria were determined a priori. Combinations of the following search terms were used: functional somatic syndrome, fibromyalgia, irritable bowel syndrome, IBS, chronic migraines, chronic headaches, interstitial cystitis, chronic fatigue syndrome, multiple chemical sensitivity, spine or spinal surgery, discectomy, laminectomy, fusion, opioid, narcotic, factors, and patient reported outcome. In conjunction, the bibliographies of relevant systematic reviews were examined for additional relevant studies.
Titles, abstracts, and full text were screened for inclusion. Studies were included if they: (1) were written in the English language, (2) involved subjects who underwent spine surgery, (3) compared outcomes of patients with pre-treatment diagnosis of at least one of 6 well recognized FSSs (fibromyalgia, irritable bowel syndrome, chronic headaches/migraines, interstitial cystitis, chronic fatigue syndrome, multiple chemical sensitivity) to patients without a pre-treatment diagnosis of at least one FSS. While low back pain and chronic whiplash are also well-documented FSSs, they were excluded because of the difficulty of delineating the etiology of low back or cervical pain in patients who are candidates for spine surgery. Any discrepancies regarding the inclusion and/or exclusion of a given study were to be resolved by discussion among the 2 authors (R.M., M.F.) and the senior author (M.J.S.); however, no discrepancies remained after discussion during the selection process.
Evaluation of risk of bias was performed using the Methodological Index for Non-Randomized Studies (MINORS) criteria. The MINORS criteria is a validated tool that contains twelve items, each scored from 0-2. 19 The maximum score for non-comparative studies is 16 and the maximum score for comparative studies is 24 19 .
Data Extraction
Data pertaining to patient demographics (age, sample size, gender, etc.), type of procedure, follow-up, loss to follow-up, PROMs, postoperative analgesic use, cost of care, complications, and readmission rate were recorded.
Results
Study Identification
The search identified a total of 743 records, of which 7 studies met the inclusion criteria. A PRISMA flow diagram is shown in Figure 1. PRISMA flow diagram.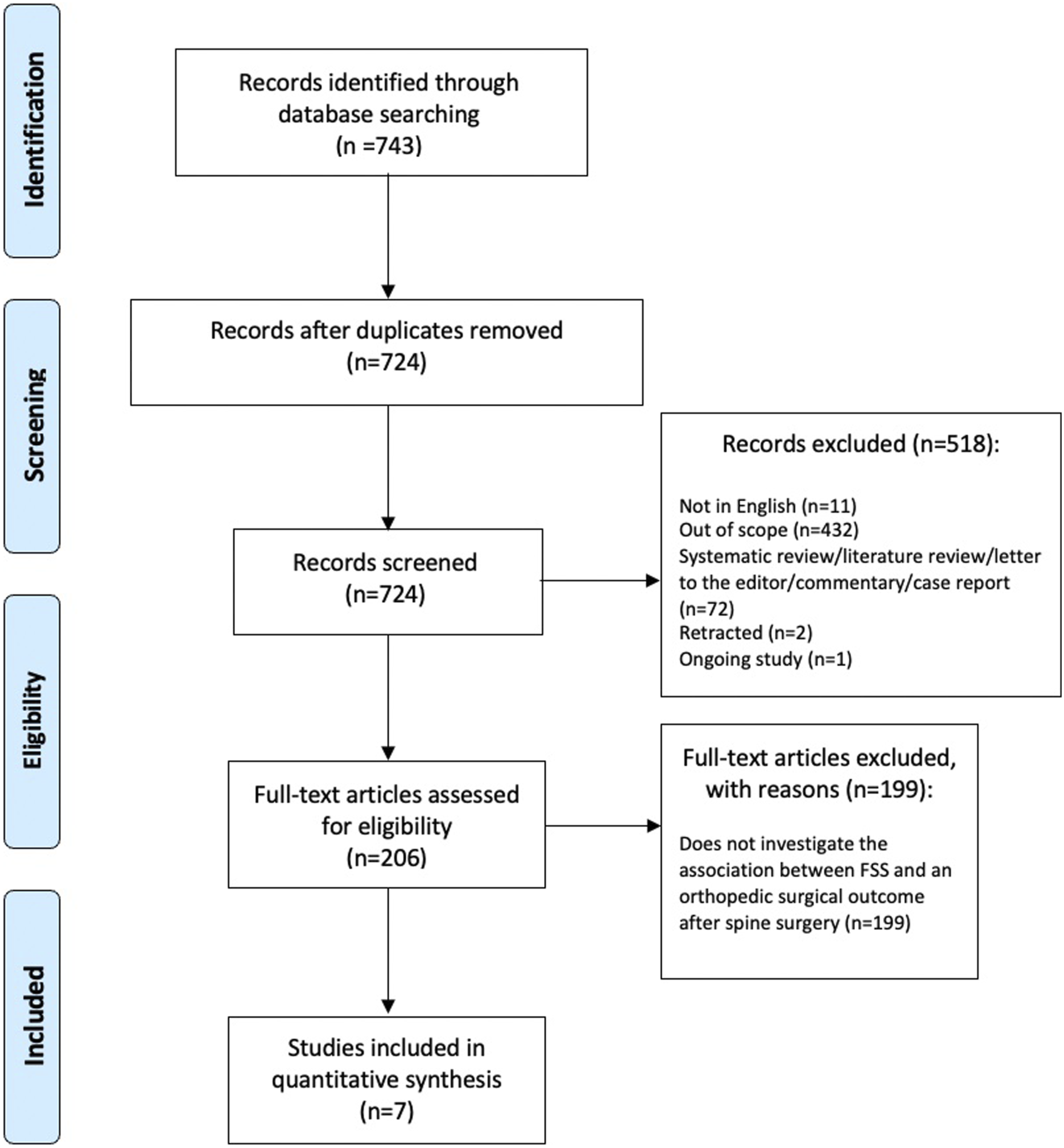
Study Characteristics
Summary of all Studies Included in Systematic Review.
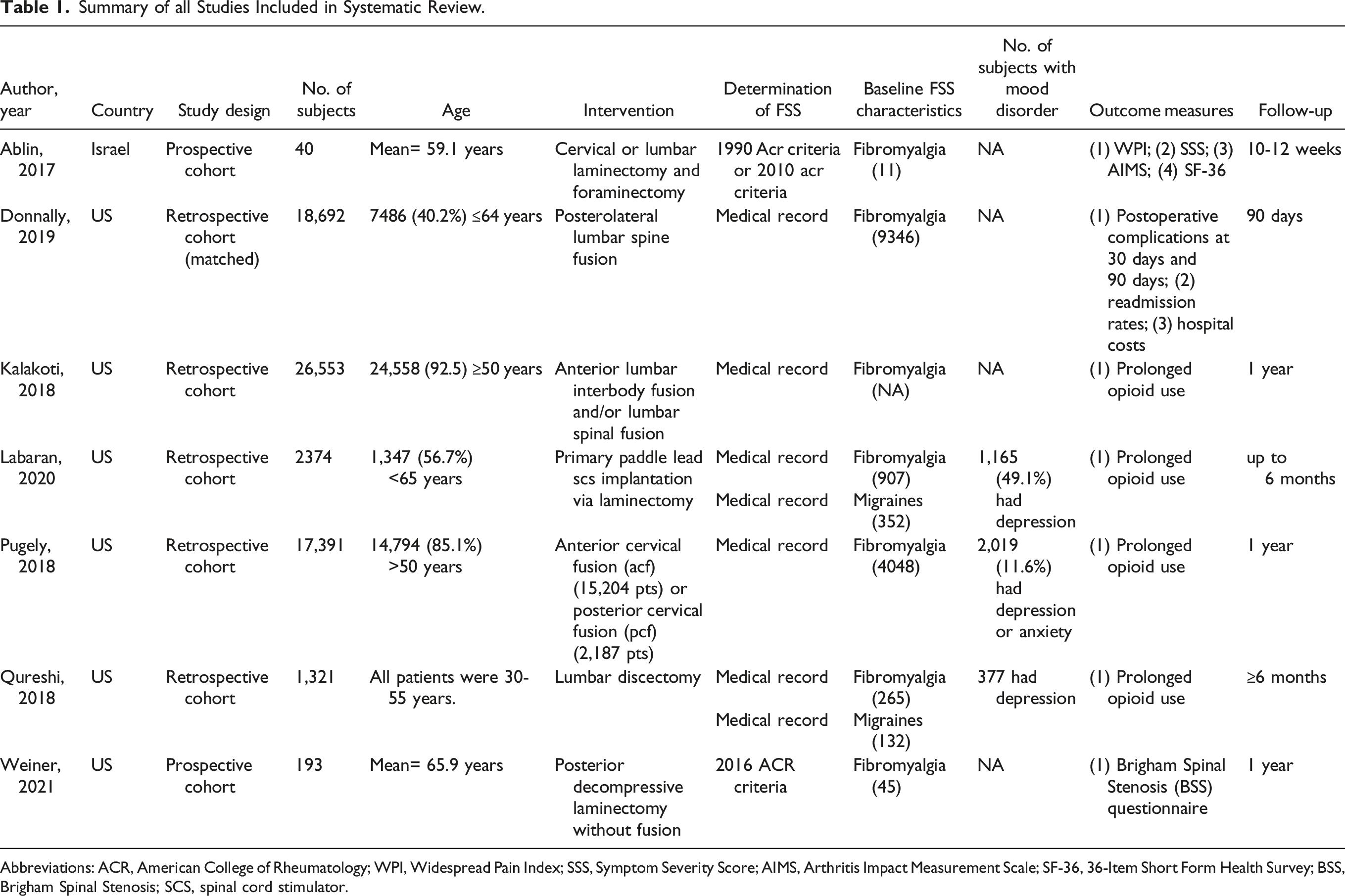
Abbreviations: ACR, American College of Rheumatology; WPI, Widespread Pain Index; SSS, Symptom Severity Score; AIMS, Arthritis Impact Measurement Scale; SF-36, 36-Item Short Form Health Survey; BSS, Brigham Spinal Stenosis; SCS, spinal cord stimulator.
The total number of subjects was 40,011. All 7 studies assessed fibromyalgia, 2 studies assessed migraines, and no studies assessed IBS, interstitial cystitis, chronic fatigue syndrome, or multiple chemical sensitivity. Determination of fibromyalgia was made using American College of Rheumatology (ACR) criteria (2) and medical records (5), whereas chronic migraine determination was made using medical records (2) only.
The included studies reviewed outcomes following spine surgery, including laminectomy (3), spine fusion (2), discectomy (1), and spinal cord stimulator (SCS) implantation via laminectomy (1). 14,622 patients had FM and 484 had chronic migraines. One study (Kalakoti et al) did not report number of patients with FM. Using the 2 papers that reported mean age, the weighted mean age of patients was 64.7 years. All 7 studies reported gender distribution, and 62.0% (n = 41,086) of subjects were female. The mean time to follow-up was 7.7 months.
Outcomes
Opioid Use
Four studies (n = 21,086) reported postoperative opioid use at various time points (Figure 2). Of these, 3 reported that a diagnosis of at least one FSS was a strong risk factor for long-term opioid use among patients undergoing spine surgery. Qureshi et al
24
reported that patients with FM are 2.12 times more likely to use opioids for greater than 3 months following lumbar discectomy compared to controls (OR = 2.12, 95% CI: 1.56, 2.89).
24
Pugely et al and Kalakoti et al found similar results.22,25 While Qureshi et al also suggested patients with migraines are more likely to use opioids for greater than 3 months following lumbar discectomy, Labaran et al found that patients with migraines are not more likely than controls to have prolonged opioid use following SCS placement.23,24 Visual Representation of Postoperative Opioid Use Abbreviations: PLF, posterolateral fusion; P/TLIF, posterior/transforaminal lumbar interbody fusion; ALIF, anterior lumbar interbody fusion; PCF, posterior cervical fusion; ACF, anterior cervical fusion Multivariable regression estimates are shown unless otherwise stated.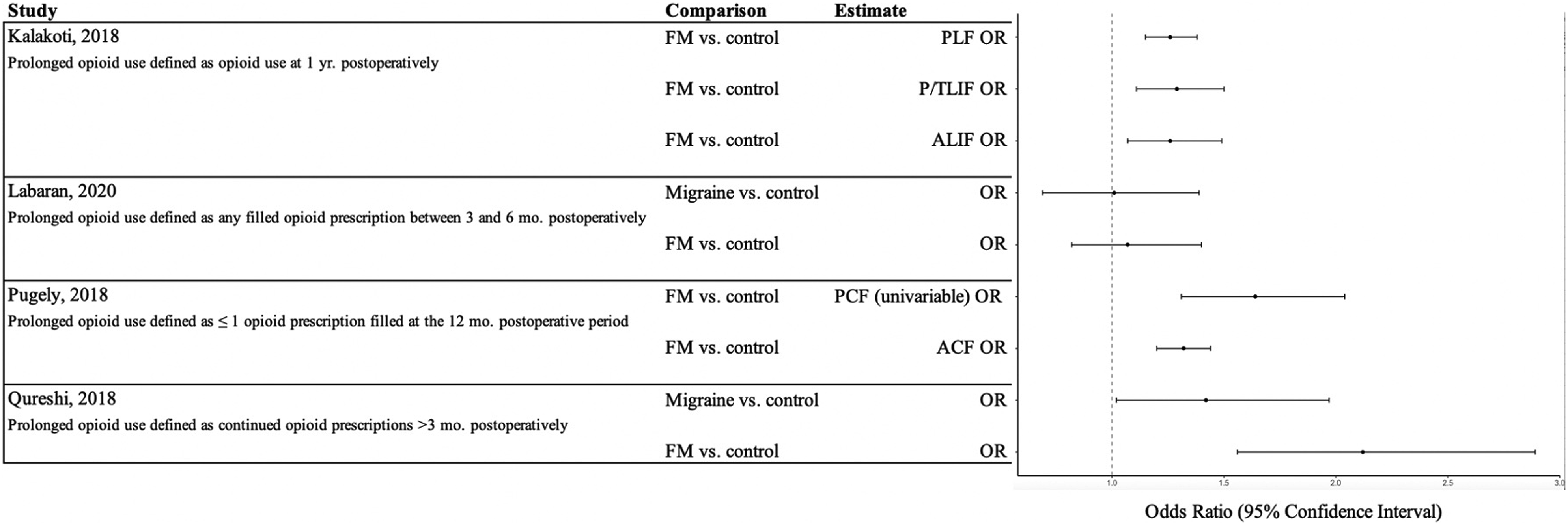
Patient Reported Outcome Measures
Summary of Patient Reported Outcome Measures (PROMs).
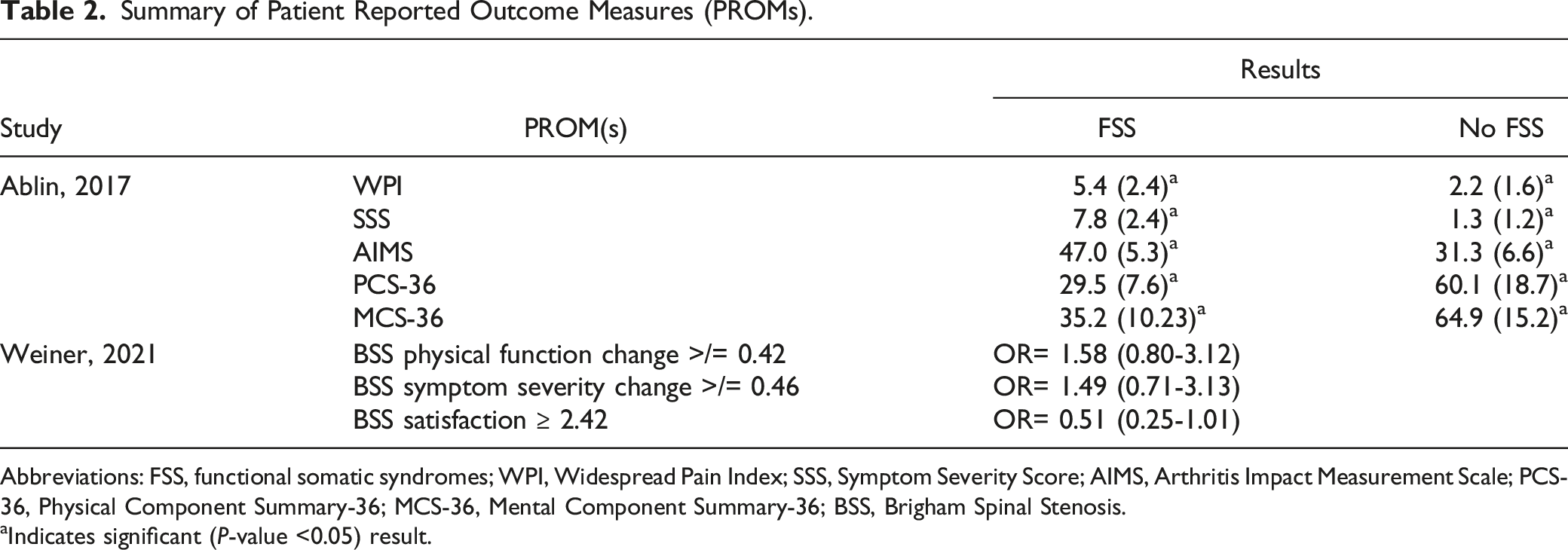
Abbreviations: FSS, functional somatic syndromes; WPI, Widespread Pain Index; SSS, Symptom Severity Score; AIMS, Arthritis Impact Measurement Scale; PCS-36, Physical Component Summary-36; MCS-36, Mental Component Summary-36; BSS, Brigham Spinal Stenosis.
aIndicates significant (P-value <0.05) result.
Other Outcomes
One study (n = 18,692) reported postoperative complications, readmission rates, and hospitalization costs. Donnally et al found that among patients who underwent lumbar spine fusion, those who had FM had significantly higher rates of acute post hemorrhagic anemia, wound-related complications, and pneumonia postoperatively. 20 In addition, this study reported a significantly higher readmission rate among patients with FM at 30 days postoperatively, however this association was no longer present at 90 days postoperatively. 20 Patients with FM also incurred greater in-hospital charges but also had higher reimbursements. 20
Discussion
Our primary findings revealed that patients with the individual FSS conditions of fibromyalgia and possibly migraines consume significantly more opioids postoperatively, have higher postoperative complications, and may have less favorable PROMs after spine surgery. Three out of 4 included studies that examined postoperative opioid use in patients with FM found patients with FM use significantly more opioids than those without.22,24,25 In addition, one study reported that patients with FM have poorer postoperative outcomes across several PROMs, such as the 36-Item Short Form Health Survey. 26
Historically, FSSs were broken down into somatic symptoms. These somatic symptoms, such as headache and fatigue, are common. 1 Clusters of somatic symptoms are known as FSSs and more current estimates suggest nearly one-third of patients presenting to primary care physicians suffer from at least one FSS. 7 Patients with FSSs tend to be similar in terms of symptoms, case definitions, sex, prognosis, and treatment response to their FSS treatment.5,27 In fact, Wessely et al suggests viewing FSSs as individual conditions may be “an artifact of medical specialization.” 5 Thus, authors have argued that viewing these conditions collectively will enhance our knowledge.5,17 This collection of conditions are not only found within primary care, but within numerous medical subspecialties, including neurology, rheumatology, and gastroenterology. Given how common these conditions are, FSSs also affect orthopaedic patients undergoing spine surgery. It is important to recognize that these conditions have been associated with psychological distress and higher healthcare utilization rates.3,5 Future studies need to address the psychiatric components of these syndromes. The psychological diagnoses that many patients with FSSs carry need to be controlled for in future analyses. Furthermore, literature suggests that FSSs may be better understood on a continuum, with patients who have more functional symptoms, have more severe disease states.28-32
The use of prescription opioids in the U.S. increased fourfold between 1997 and 2010. The increase in consumption of opioids has been associated with increased misuse of these medications, diminished healthcare quality of life, increased pain intensity and pain-related disability, and increased morbidity and mortality.33-36 Numerous studies have explored opioid consumption in patients with FSSs and have found that these patients consume significantly more opioids postoperatively, suggesting this subpopulation undergoes a different pain experience than patients without FSSs.22,24,25 It is important to consider the unique pain considerations of patients with FSSs while treating these patients and potentially prescribing opioids for postoperative pain control. This finding is consistent with previous literature showing that patients with FSSs have less pain improvement and prolonged postoperative opioid use.28,37-39
Across several types of orthopaedic surgeries, there are now multiple studies suggesting patients with FSSs have worse pain postoperatively.6,22,24,25,28,37-40 While the reasons for this are unclear, it may be due to how these patients respond to painful stimuli. 41 For example, patients with IBS report hyperalgesia. 42 In addition, catastrophizing, which is “a set of negative emotional and cognitive processes”, is related to the chronic pain experienced in FM and is associated with higher pain severity.43,44 More studies that look at FSSs collectively are needed to understand the mechanisms behind these conditions so that they can be adequately addressed and counseled preoperatively. Moverman et al. looked at FSSs as a collective, rather than as individual diagnoses, and found that more of these disorders lead to worse outcomes in a stepwise manner after surgery. 6 In addition, studies found that postoperative complications are higher among patients with FSSs.20,45,46
Ablin et al found that patients with fibromyalgia have less favorable PROMs across 4 measures following spine surgery, while Weiner et al found no relationship between fibromyalgia and Brigham Spinal Stenosis scores. Optimizing PROMs after orthopaedic surgery is especially important given the shift from “volume-based to value-based orthopaedic care”. 47 Thus, further study is needed to better understand and characterize the recovery process of patients with FSSs after spine surgery. Due to the similarity in symptoms, treatment response, and prognosis, these future studies should include patients with a variety of FSSs so we can widen our understanding beyond the impact of fibromyalgia and migraines on recovery. Additionally, since FSSs, and especially FM, are known to be age-related phenomena, future investigations need to attempt to control for age. It is possible that some of the findings cited here are age-related, as FM and FSSs have been shown to increase in older populations.
In our literature review, we included irritable bowel syndrome, interstitial cystitis, chronic fatigue syndrome, multiple chemical sensitivity in our search. However, we found no studies that examined the impact of these conditions on outcomes after spine surgery. Our search revealed that the individual FSSs, fibromyalgia and chronic migraines, lead to worse postoperative outcomes. Thus, more research in patients with other FSS diagnoses, such as IBS and chronic fatigue syndrome, will elucidate if these patients similarly have suboptimal recovery after spine surgery.
Addressing FSSs preoperatively may result in improved outcomes and decreased pain postoperatively. Some treatments following a biopsychosocial approach, such as antidepressant medications, regularly scheduled appointments, appropriate referrals, and relaxation techniques, have been found to be effective in managing FSSs. 48 A qualitative review suggested managing FSSs with a multi-component approach comprising of both more general interventions, such as motivational interviewing, and more specific interventions, such as pharmacotherapy. 49 Referral to psychotherapists or mental health specialists prior to surgery and perhaps including them as part of the team postoperatively may improve postoperative results in this subset of patients. 48
We recognize the limitations to our review. While our literature search was performed systematically using 2 online databases, it is possible that studies that met our inclusion criteria were omitted. In addition, most studies included in this review were of low quality according to the MINORS criteria. Further, due to the retrospective design of many of the included studies, misclassification bias could have occurred. Confounding bias also could have occurred since not all studies controlled for potential confounders. In addition, amongst our selected FSSs, FM was well-represented but few or no studies looked at IBS, chronic headaches, chronic fatigue syndrome, interstitial cystitis, and multiple chemical sensitivity.
Conclusion
This systematic review is the first to explore the relationship between FSS and spine surgery. We found that patients with fibromyalgia and chronic migraines consume more opioids postoperatively, have more postoperative complications, and may have less favorable PROMs. Further research is needed to explore the relationship between FSSs collectively and outcomes in spine surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.