
Abstract
Study Design:
Retrospective cohort study.
Objective:
To identify disparities in surgical decision making for lumbar disc pathologies based on patient demographics, hospital characteristics, and temporal characteristics of admission.
Methods:
A retrospective analysis of patients admitted for surgical intervention of disc herniation or degeneration was performed to observe the effect of demographic, hospital, and admission-related factors on the decision to perform an isolated decompression or decompression with single level fusion using the National Inpatient Sample.
Results:
Of 84 953 patients with lumbar disc pathologies, 69 975 patients were treated electively, and 14 978 patients were treated nonelectively. Hispanic and Asian/Pacific Islander patients were less likely to receive a fusion for elective cases compared with White patients (odds ratio [OR] 0.88, P = .004; OR 0.70, P < .001, respectively). In elective cases, privately insured and self-paying patients were less likely to receive a fusion compared with Medicare patients (OR 0.83, P < .001; OR 0.66, P < .001, respectively), while this effect was limited to self-pay patients in nonelective cases (OR 0.44, P < .001). Urban teaching and nonteaching hospitals were less likely to perform fusions compared with rural hospitals in nonelective cases (OR 0.47, P < .001; OR 0.58, P < .001, respectively). Private for-profit hospitals were associated with higher rates of fusion in both elective and nonelective cases (OR 1.16, P = .003; OR 1.94, P < .001).
Conclusion:
This study illustrates disparities in the modality of surgical intervention for lumbar disc pathologies in terms of demographics, hospital characteristics, and temporal characteristics of admission. The development of more evidence-based guidelines is warranted to reduce variability seen in treatment regimens for these conditions.
Introduction
Approximately one quarter of US adults reported back pain lasting at least 1 day in the past 3 months. 1 It is anticipated that the prevalence of back pain is on the rise, likely attributed to the aging population and the rise in obesity within the population. 2 Disc herniation and resultant nerve root irritation is one of the main causes for low back pain with radiculopathy.3,4 Patients with persistent symptoms of radiculopathy, who do not experience spontaneous gradual improvement or fail conservative nonsurgical management, can benefit from surgical removal of the herniated disc and nerve root decompression, known as lumbar discectomy. Trends in surgery show that lumbar discectomy is the most common spine surgical procedure performed in the United States. 3
In cases of lumbar instability resulting in chronic low back pain, surgeons may choose to perform instrumented spinal fusion in addition to discectomy. 5 The updated 2014 guidelines for degenerative spine diseases recapitulated the lack of evidence for the inclusion of lumbar fusions in routine discectomies. 6 Lumbar fusions are associated with increased length of recovery, loss of range of motion, likelihood of adjacent level disease, longer operation time, higher surgical cost, and greater overall complication rates.7-9
Although previous studies have examined socioeconomic factors related to back pain and geographical variation in rates of lumbar fusions, no studies have investigated variation in surgical management of primary disc herniation based on patient income, patient race/ethnicity, or temporal characteristics of admission. This study seeks to discern if disparities in surgical management of elective and nonelective disc pathologies exist based on patient demographics, hospital characteristics, and temporal characteristics of admission through the National Inpatient Sample (NIS).
Methods
Study Sample
The Healthcare Cost and Utilization Project (HCUP) NIS database was utilized to perform a retrospective analysis using data collected from 2012 to 2015. The NIS inpatient data was used to identify case-level data on individual inpatient stays from patients across nearly all states in the United States. The NIS dataset contains de-identified individual-level data including patient demographic factors, hospital demographic factors, temporality of admission, patient diagnosis, patient procedures, and hospital stay metrics; therefore, it did not require review from our institutional review board. Admissions for 2015 only included patients through the first 3 quarters of the year due to a change in the International Classification of Diseases (ICD) coding at the start of the fourth quarter.
ICD, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes were used to identify 84 953 adult patients who had degenerative lumbar disc pathologies that were surgically intervened upon. Patients with diagnoses of cervical disc pathologies or treatments suggesting treatment of cervical disc pathologies were excluded. Also excluded were patients with inflammatory or infectious disorders of the spine as well as those with diagnoses that indicated clear instability of the spine. Patients were limited to those who did not have a history of a prior fusion to reduce bias toward the use of fusions in those patients. Patients were divided into nonelective and elective cohorts for analysis. Full inclusion and exclusion criteria used are outlined in Supplementary Materials.
Baseline Characteristics
Patient demographics assessed in this analysis included age (and age squared for elective patients), sex (female, male), race (Black, White, Hispanic, Asian/Pacific Islander, Native American, Other), location of patient’s residence (central counties of metro areas of ≥1 million population, fringe counties of metro areas of ≥1 million population, counties in metro areas of 250 000 to 999 999 population, counties in metro areas of 50 000 to 249 999 population, micropolitan counties, or not metropolitan/micropolitan counties), median household income quartiles for patient’s ZIP code ($1-$38 999; $39 000-$47 999; 48 000-$62 999; and $63 000 or more), and payer (Medicare, Medicaid, private, self-pay, no charge, other).
Hospital demographics assessed included census division of hospital (New England, Middle Atlantic, East North Central, West North Central, South Atlantic, East South Central, West South Central, Mountain, Pacific), bed size (small, medium, large), control/ownership of hospital (government, nonfederal; private, nonprofit; private, investor-own), and location/teaching status of hospital (rural, urban nonteaching, urban teaching). US Census Bureau Divisions were used; however, not every state reported data to the NIS during the years queried. Alabama, Delaware, Idaho, and New Hampshire had no data for any of the years queried. Other states only had data available for certain years in the analysis. For example, Alaska had data for 2012 and 2015, District of Columbia had data for 2013 through 2015, Maine had data for 2014 and 2015, and Mississippi had data for 2015.
Temporal characteristics of admission studied included admission on weekday/weekend, admission month, and admission year.
Patient medical comorbidities that were controlled for include presence of alcohol abuse, deficiency anemias, chronic blood loss anemia, congestive heart failure, chronic pulmonary disease, coagulopathies, depression, uncomplicated diabetes, diabetes with chronic complications, hypertension, liver disease, fluid and electrolyte disorders, other neurological disorders, obesity, paralysis, peripheral vascular disorders, psychoses, pulmonary circulation disorders, renal failure, valvular disease, and weight loss as coded through the Elixhauser Comorbidity Software and provided in the NIS. All Patient Refined Diagnosis Related Group (APR-DRG) risk of mortality subclass and severity of illness subclass were also controlled for.
Statistical Analysis
Patients were grouped based on whether their admission was elective or nonelective. Patient demographics, hospital demographics, and day, month, and year of admission included in the analysis are summarized. Effects of these factors on the treatment regimen (decompressive surgery or decompressive surgery with lumbar fusion) were evaluated using a multiple logistic regression model for each group. The regression models controlled for patient-level medical comorbidities outlined above. Only patients who received, at a minimum, a laminectomy or discectomy (decompressive surgery) were included in the analysis. Holm-Bonferroni correction was applied to correct for multiple testing. The significance level was set at α = .05 for all regressions and odds ratios, 95% confidence intervals, and P values were calculated. R software, version 3.4.3 (R Foundation), was used to perform all data analysis. This study complies with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results
Baseline Sample Characteristics
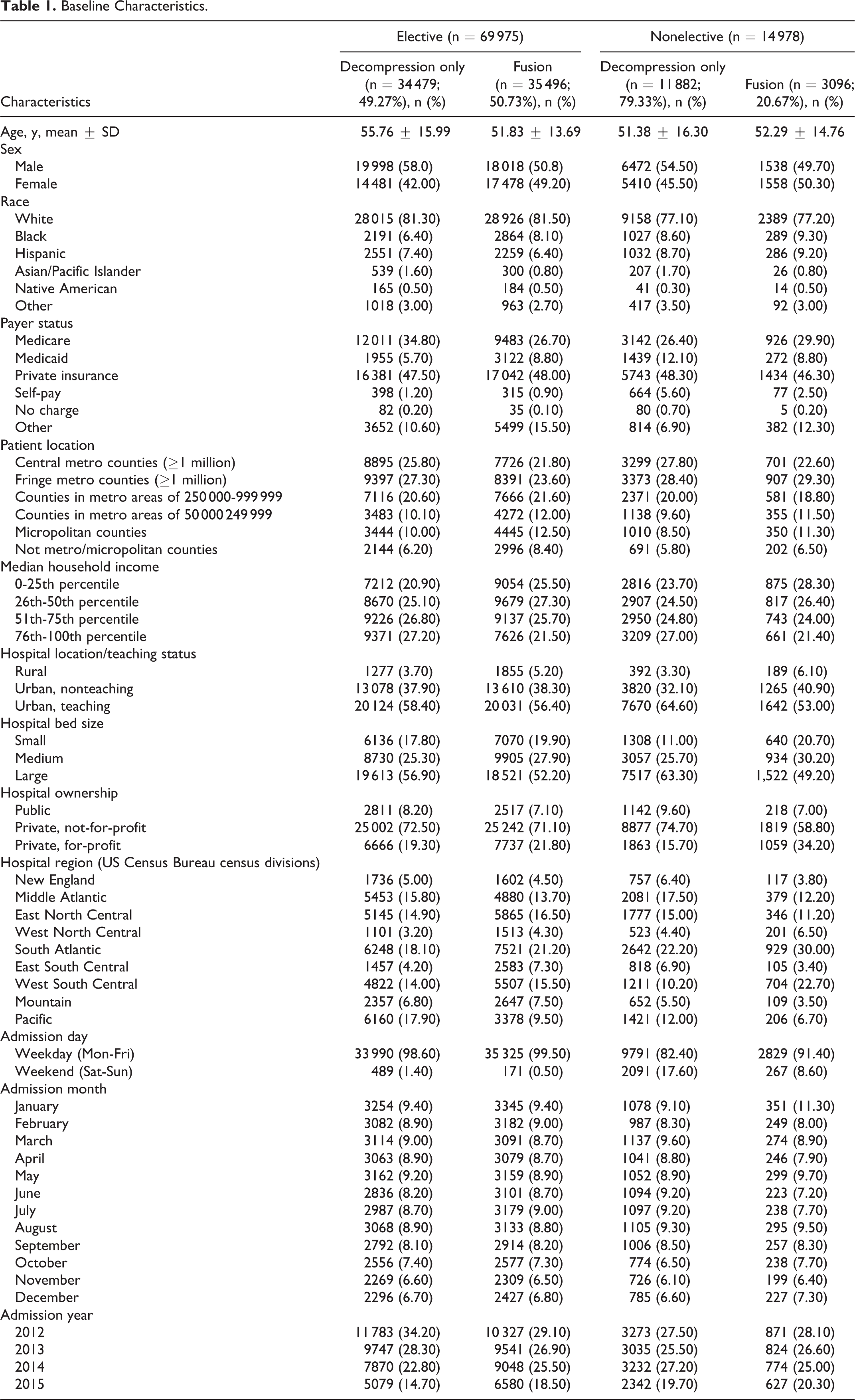
A total of 84 953 patients were included in the analysis of predictors for fusion after elective and non-elective surgical intervention for lumbar disc pathologies. A total of 69 975 patients were treated electively, 35 496 (50.73%) of whom received a fusion after decompression, and 14 978 patients were treated on a nonelective basis, 3096 (20.67%) of whom received a fusion after decompression. The baseline characteristics of the study population are shown in Table 1.
Baseline Characteristics.
Patient Characteristics Associated With Fusion
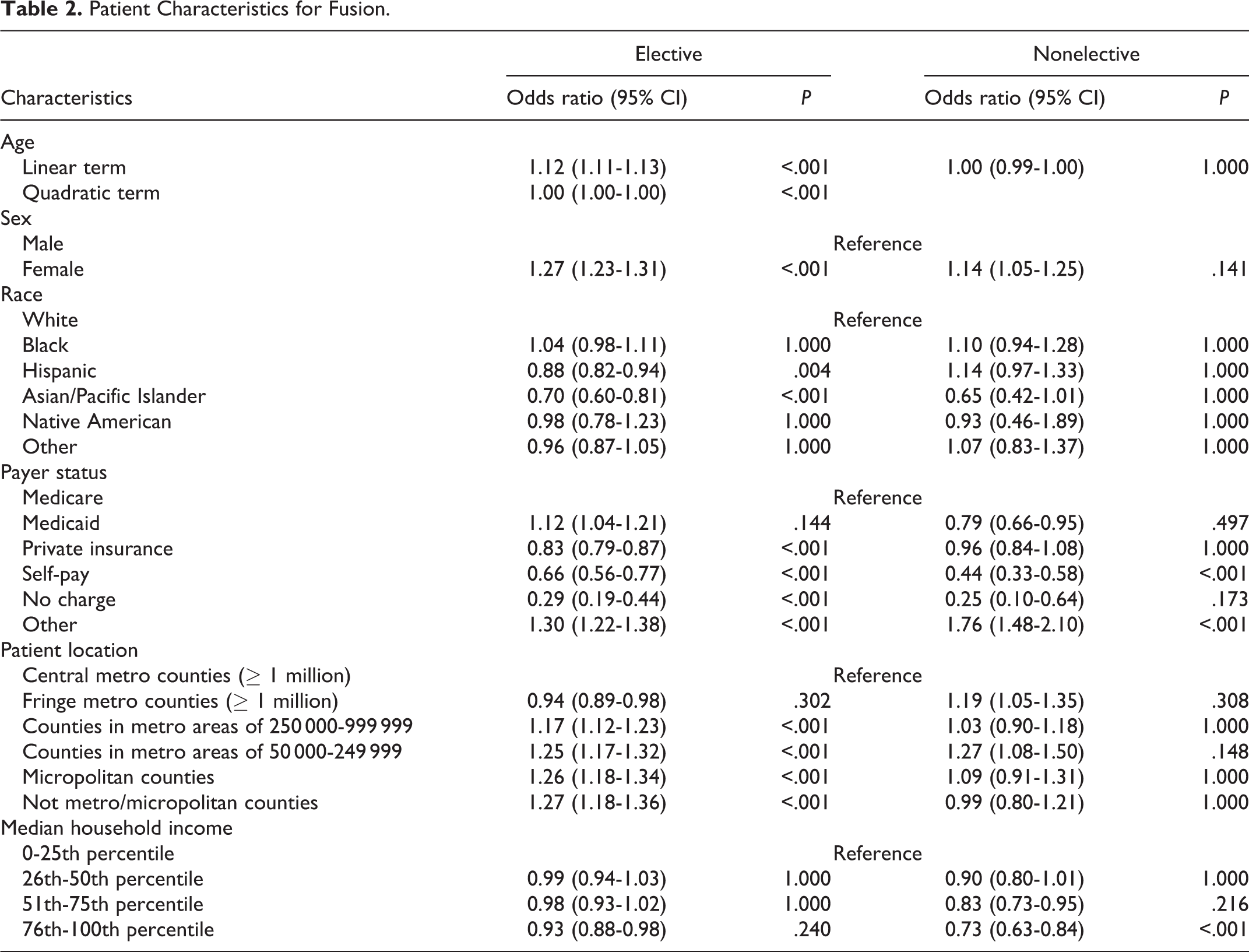
In a multivariable analysis of patient-related predictors for fusion, patient age, race, sex, insurance status, residence, and median household income were found to be associated with an increased fusion after decompression (Table 2). In elective cases, Hispanic and Asian/Pacific Islander patients were more likely to receive fusions compared with White patients (odds ratio [OR] 0.88, P = .004; OR 0.70, P < .001, respectively). Female patients were more likely to receive fusions in elective cases (OR 1.27, P < .001). In elective cases, privately insured, self-paying, and charity care patients were less likely to receive a fusion compared with Medicare patients (OR 0.83, P < .001; OR 0.66, P < .001; OR 0.29, P < .001, respectively), while this effect was limited to self-pay patients in nonelective cases (OR 0.44, P < .001). Compared with patients residing in central metropolitan counties, those in smaller counties with populations of <1 million were more likely to receive a fusion in elective cases (OR 1.17-1.26, P < .001 for all). In nonelective cases, patient location of residence had no effect on rates of fusion. Median household income had no effect on rates of fusion in elective cases, while patients in the 75th to 100th percentile of median household income had lower rates of fusion in nonelective cases (OR 0.73, P < .001).
Patient Characteristics for Fusion.
Hospital Characteristics Associated With Fusion
Hospital-related predictors of fusion were identified according to hospital location and teaching status, bed size, and ownership (Table 3). Hospital location and teaching status had an effect on rates of fusion in nonelective cases, in which urban teaching and non-teaching hospitals were less likely to perform a fusion compared with rural hospitals (OR 0.47, P < .001; OR 0.58, P < .001, respectively). In elective cases, fusions were less likely at urban teaching hospitals only (OR 0.83, P < .001). The rates of fusion had an inverse relationship with the size of the hospital for both elective and nonelective cases. Private hospital ownership, regardless of for-profit status, was seen as a predictor for higher rates of fusion in elective cases when compared with public hospitals (OR 1.21, P < .001, not-for-profit; OR 1.16, P = .003, for-profit). In nonelective cases, however, fusion rates were observed to be higher in for-profit private hospitals only (OR 1.94, P < .001).
Admission Characteristics for Fusion.
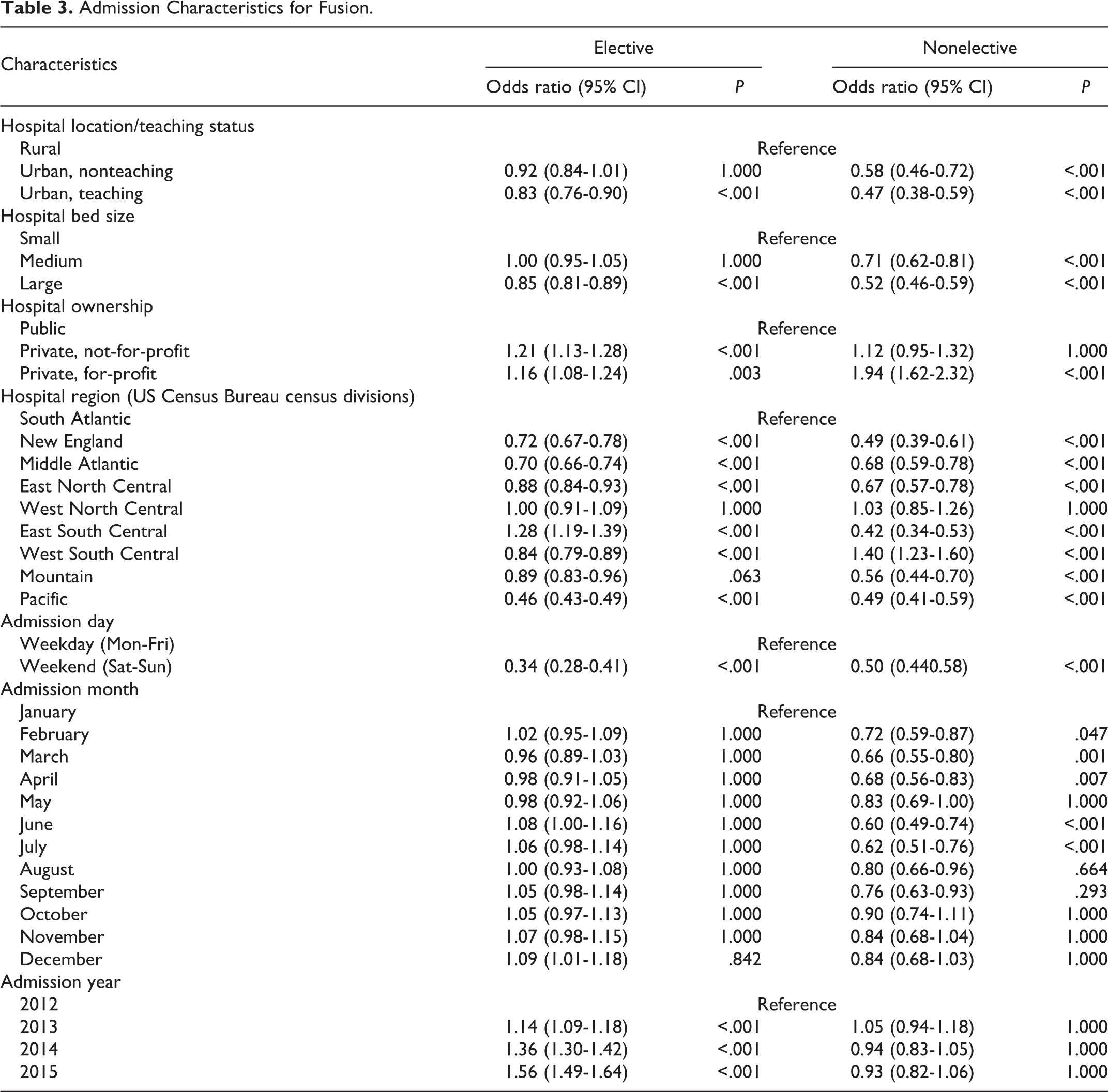
Hospital region, defined by the US Census Bureau, showed varying unique rates of fusion in both elective and nonelective cases (Table 3, Figure 1). In elective cases, hospitals in New England, Middle Atlantic, East North Central, West South Central, and Pacific regions had lower rates of fusions compared with hospitals in the South Atlantic region (OR 0.72, P < .001; OR 0.70, P < .001; OR 0.88, P < .001; OR 0.84, P< .001; OR 0.46, P < .001, respectively). On the other hand, hospitals in the East South Central region were more likely to perform a fusion (OR 1.28, P < .001). In nonelective cases, hospitals in New England, Middle Atlantic, East North Central, East South Central, Mountain, and Pacific regions performed less fusions compared with the South Atlantic region (OR 0.49, P < .001; OR 0.68, P < .001; OR 0.67, P < .001; OR 0.42, P < .001; OR 0.56, P < .001; OR 0.49, P < .001, respectively), while hospitals in West South Central performed more fusions (OR 1.40, P < .001).
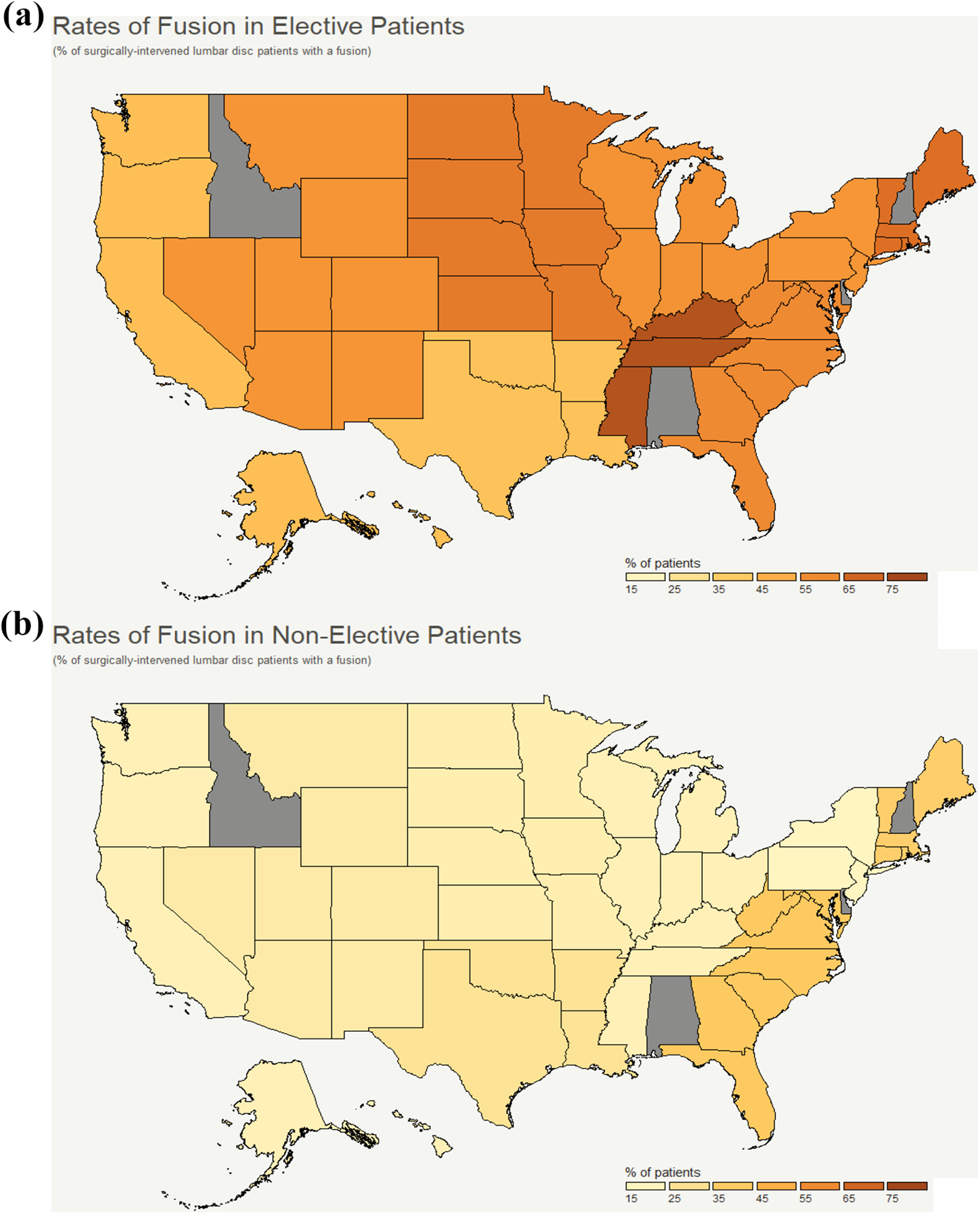
Geographical rates of fusions in elective (a) and nonelective (b) lumbar disc patients.
Temporal Characteristics Associated With Fusion
The day, month, and year of admission had significant effects on whether a fusion was performed or not (Table 3). Weekend admissions were twice as less likely to receive a fusion compared to weekday admissions in both elective and nonelective cases (OR 0.34, P < .001; OR 0.50, P < .001, respectively). In addition, decreased rates of nonelective fusions were observed in February, March, April, June, and July compared with January (OR 0.72, P = .047; OR 0.66, P < .001; OR 0.68, P = .007; OR 0.60, P < .001; OR 0.62, P < .001, respectively). Finally, progressively increased rates of fusion in elective cases were seen in 2013, 2014, and 2015 compared with 2012 (OR 1.14, P < .001; OR 1.36, P < .001; OR 1.56, P < .001, respectively).
The main findings of the multiple logistic regression analysis of nonmedical factors in surgical decision-making are displayed in Figure 2.
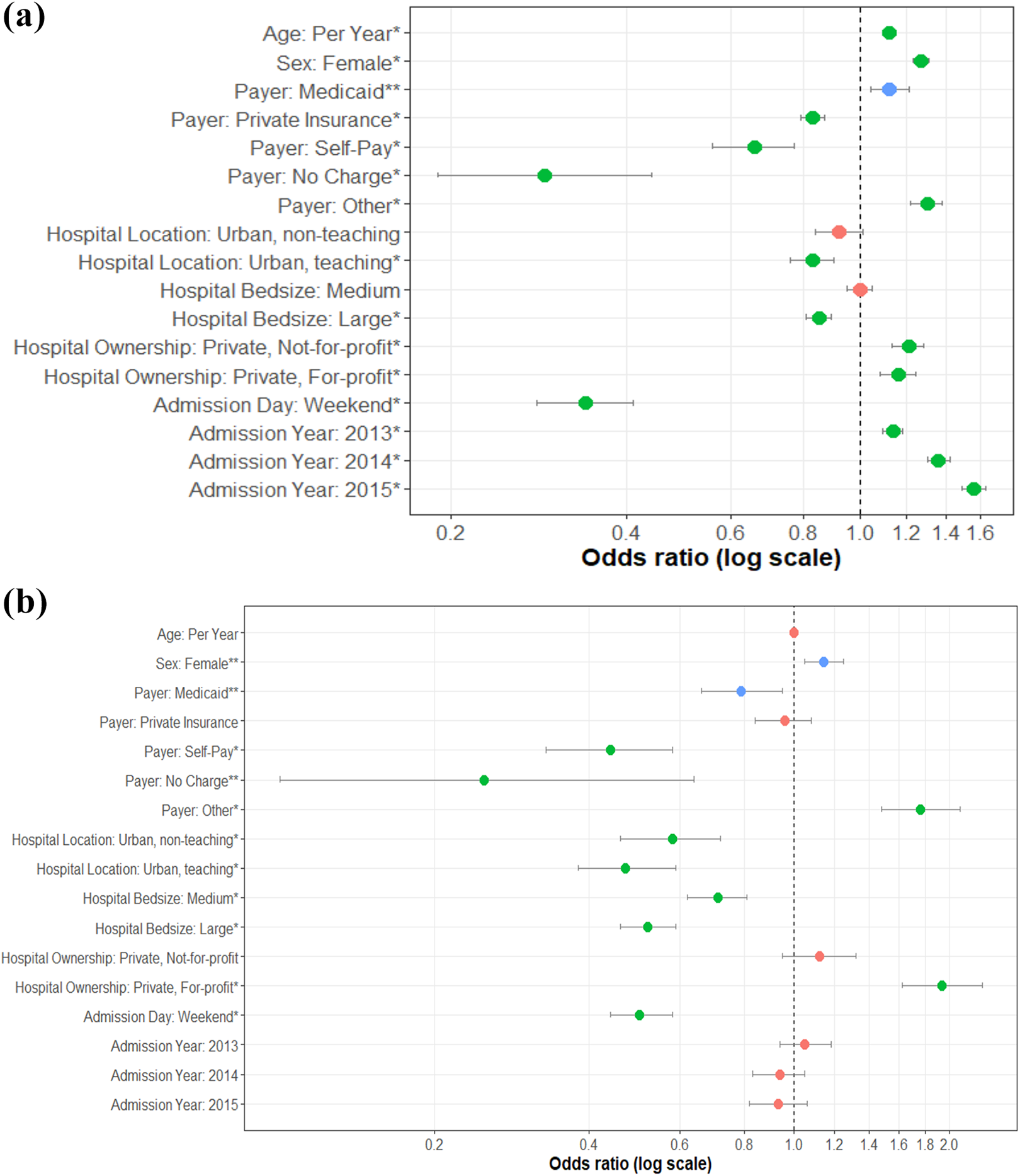
Nonmedical factors in the decision to perform fusion for lumbar disc pathologies. (a) Key findings for elective lumbar disc patients. (b) Key findings for nonelective lumbar disc patients. The figure shows a forest plot of various nonmedical factors and their associated odds of performing a fusion over a baseline decompression in lumbar disc pathologies. Data points represent the odds ratios (OR) of such factors, while the horizontal lines represent 95% confidence intervals of the respective variables. ORs with 95% confidence intervals which do not cross OR = 1.0 (horizontal dotted line) are considered statistically significant. To aid interpretation, data points have been color-coded by the following: green= statistically significant after correction for multiple testing, blue = statistically significant without correction for multiple testing, but no longer statistically significant after correction, red = not statistically significant.
Discussion
Patients with lumbar disc pathologies and subsequent radiculopathy or debilitating back pain unresponsive to conservative therapies are primarily treated via discectomy and decompression of the affected nerve root. Additionally, the surgeon may opt to administer a subsequent fusion to prevent recurrent disc herniation secondary to micromotion across the joint, late-onset instability, or progressive chronic low back pain. However, the literature regarding fusions for lumbar discectomy patients remains controversial with significant variation in clinical practice. 10 Several studies have reported the inefficacy of an additional fusion in improving functional outcomes compared with discectomy alone.11-14 Our study attempts to identify ingrained practice pattern biases that exist amongst surgeons performing isolated discectomies versus discectomy and fusion for management of lumbar disc herniation with radiculopathy.
Patient Characteristics Associated With Fusion
Our study found age and sex to be predictive of a subsequent fusion with decompression of lumbar disc pathologies. An analysis of the distribution of the residuals showed that age had a nonlinear relationship with rate of fusion, when looking at the elective population (a linear relationship was confirmed in the nonelective group). Therefore, a quadratic term was added to better characterize the nonlinear effects of age on the likelihood of receiving an elective fusion, which is consistent with previous literature showing reduced rates of fusion in younger and older cohorts. 15 Previous research has shown that the proportion of women who received lumbar fusion increased significantly between 1998 and 2008, 16 and this gender trend is recapitulated in our data from 2012 to 2015. The increased rates of fusion in the female population can be potentially explained by a higher risk of lumbar instability due to greater prevalence of central obesity in women and worsening lumbar lordosis during and after pregnancy.17-19 Women suffer from progressive back pain and limited mobility more often preoperatively; therefore, they may see greater improvements from baseline following fusions compared to men. 20
Insurance status was a large predictor for fusion in our analysis. Cost comparisons of treatment for degenerative disc diseases have shown that fusions are associated with higher surgical costs.21,22 The lower rates of fusions for self-paying patients in both elective and nonelective cases seen in our analysis may be explained by the increased cost associated with fusion procedures. The lower rates of fusion in elective cases among privately insured patients illustrated in our study contradicts the general trends in spinal surgery, in which disproportionately higher rates of spinal fusions have been observed in privately insured patients.23,24 A potential explanation for our results pertaining to elective cases among privately insured patients may be related to the patient’s ability to seek multiple opinions ranging from most conservative to most invasive modes of surgical intervention. This provides the opportunity for the patient to weigh recovery duration, likelihood of recurrent disc herniation versus adjacent segment disease, and morbidity and mortality associated with each intervention prior to committing to an educated surgical decision. Additionally, in elective cases, individuals needing to return to work may have a commitment to speedy recovery. Given that the majority of private insurance in the United States is sponsored by a form of employment, 25 it can be postulated that privately-insured patients may opt to address their pathology via the least invasive route, which in this case is isolated decompression without fusion.
Hospital Characteristics Associated With Fusion
Fusions were performed with a greater rate on patients in smaller, rural hospitals compared with those at larger, urban hospitals in our analysis, which is consistent with a previous study. 26 This also corresponds with our finding that rates of fusion procedures were inversely correlated with population density of patient residence. The observed results highlight disparities in surgical decision making, suggesting differing surgical protocols between physicians at rural and urban institutions. The drivers behind this finding cannot be thoroughly studied by the current database; however, further evaluation of this finding is crucial in standardizing care between rural and urban institutions.
Geographic variation in rates of lumbar fusion in our analysis were found to be similar to previous studies, in which higher proportions of fusion were reported in the South and Midwest regions, and lower proportions were reported in the Northeast and West region from 1990 to 2000.27,28 Among Medicare beneficiaries, the geographic variation in reported rates of lumbar fusion during 2002 to 2003 was nearly 20-fold in comparison to an 8-fold variation in lumbar discectomy 8 . This variation was the largest observed of any surgical procedure. Surgeon-specific characteristics may also account for observed variations in fusion rates. Such variation includes surgeon age, which may indirectly reflect training in a fusion versus nonfusion modality of treatment, as well as physician’s subspecialty training in spine.29,30 Overall, these findings further suggest a lack of consensus on indications for fusions in disc pathologies.
Temporal Characteristics Associated With Fusion
Our findings of lower odds for fusion during weekend admissions may reflect logistical barriers in planning and performing complex surgeries during time periods of limited resources. When evaluating fusion rates over weekends, it is appropriate to evaluate elective and nonelective cases separately given their differences in terms of innate nature of pathology and urgency. Overall occurrence of elective weekend admission is uncommon, which was reflected in this study. In the rare instances that elective admissions are carried out over the weekend, coordination for complex procedures with specialty staff is taxing on the surgeon, operative team, and administration, which deters complex and prolonged elective fusions at these times. By the same token, the emergent nature of non-elective weekend admissions may not allow sufficient time to gather clinical context for a fusion procedure or prepare appropriate staffing. The provider may decide to relieve the primary discogenic problem without fusion, unless there is clear evidence of instability in addition to disc herniation and nerve root irritation.
A previous NIS study on lumbar fusions observed a decrease in the overall volume of fusions for disc herniation and degeneration in the same time frame, suggesting that providers are performing less fusions for disc pathologies. 31 Although our analysis confirms this decreasing trend in the number of fusions performed during 2012-2015, the odds of fusion and decompression compared with receiving an isolated decompression actually increased over time, which indicates that standard of practice is shifting toward more fusions per surgical intervention for disc pathologies. Our observed trend is incongruent with the lack of evidence supporting the efficacy of instrumentation in lumbar disc pathologies 10 and may reflect evolving practice patterns that are not based on the available evidence.
Limitations
The results of this study must be interpreted with caution due to limitations that arise with retrospective analysis using the National Inpatient Sample. First, although the NIS contains many comorbidities, which were controlled for in the present study, many confounding variables were not captured by the database such as smoking status, level of pain, or extent of conservative therapy previously administered. As such, certain justifiable clinical circumstances may indicate the need for a fusion despite the unsupportive summary of evidence. Second, the NIS only provides data of inpatient admissions, limiting our analysis. Lumbar fusions are generally not performed on an outpatient basis; however, outpatient discectomies are more routine. 32 The lack of inclusion of outpatient discectomy cases in our analysis may bias findings reported in our study. Our study used ICD-9 diagnosis and procedure codes, which may introduce significant confounding due to errors in coding and coding variability between institutions. Although we made an effort to maintain equipoise in surgical decision making by selecting lumbar disc pathologies that do not typically present with spinal instability (Supplementary Material), our patient population may not be homogenous due to the heavy reliance on ICD-9 codes. It should be noted that the lumbar disc pathologies assessed in the current study contain a broad range of diverse clinical presentations and associated indications for surgery. Even after filtering out for patients with spinal instability, there are aspects of clinical presentation and subsequent surgical decision making that are not readily elucidated with the NIS dataset, and thus were not sufficiently controlled for. This limitation is inherent to large database analyses using nonspecialized data sources such as the NIS. Therefore, our analyses warrant further inquiry into whether the hospital and demographic factors identified as being associated with rates of fusion are explained by differences in the clinical presentation of patients based on these factors or the providers’ decision making based on such factors. An analysis using a more specialized database would help answer this particular inquiry. Finally, ICD-9-CM diagnosis codes do not distinguish between primary and repeat procedures, which may have varying surgical indications.
Conclusion
The increase in number of patients affected by disc herniation, correlating radiculopathy, and back pain highlight the need for more evidence-based guidelines to the selection of surgical interventions regarding discectomy versus discectomy and fusion. The current study illustrates disparities in surgical decision making pertaining to management of this pathology that are widely affected by age, sex, demographics, and hospital characteristics. Inevitably, patient preference and a surgeon’s capabilities and preferences play a large role in the ultimate decision-making regarding mode of surgical intervention. However, more evidence-based guidelines are needed to be explored to bridge the gap in variability of treatments offered, which can result from evaluation of postoperative outcomes of the groups described in this study.
Supplemental Material
sj-docx-1-gsj-10.1177_2192568220951137 - Disparities in Rates of Fusions in Lumbar Disc Pathologies
sj-docx-1-gsj-10.1177_2192568220951137 for Disparities in Rates of Fusions in Lumbar Disc Pathologies by Soobin Kim, James S. Ryoo, Philip B. Ostrov, Abhinav K. Reddy, Mandana Behbahani and Ankit I. Mehta in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Mehta has been a consultant for Depuy Synthes and Globus Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.