
Abstract
Study Design:
Retrospective database study.
Objective:
Tobacco use is associated with complications after surgical procedures, including poor wound healing, surgical site infections, and cardiovascular events. We used the Nationwide Readmissions Database (NRD) to determine if tobacco use is associated with increased 30- and 90-day readmission among patients undergoing surgery for degenerative spine disorders.
Methods:
Patients who underwent elective spine surgery were identified in the NRD from 2010 to 2014. The study population included patients with degenerative spine disorders treated with discectomy, fusion, or decompression. Descriptive and multivariate logistic regression analyses were performed to identify patient and hospital factors associated with 30- and 90-day readmission, with significance set at P value <.001.
Results:
Within 30 days, 4.8% of patients were readmitted at a median time of 9 days. The most common reasons for 30-day readmission were postoperative infection (12.5%), septicemia (3.5%), and postoperative pain (3.0%). Within 90 days, 7.3% were readmitted at a median time of 18 days. The most common reasons for 90-day readmission were postoperative infection (9.6%), septicemia (3.5%), and pneumonia (2.3%). After adjustment for patient and hospital characteristics, tobacco use was independently associated with readmission at 90 days (odds ratio 1.05, 95% confidence interval 1.03-1.07, P < .0001) but not 30 days (odds ratio 1.02, 95% confidence interval 1.00-1.05, P = .045).
Conclusions:
Tobacco use is associated with readmission within 90 days after cervical and thoracolumbar spine surgery for degenerative disease. Tobacco use is a known risk factor for adverse health events and therefore should be considered when selecting patients for spine surgery.
Introduction
Cigarette smoking is a leading problem in public health that impacts an estimated 34.3 million adults in the United States.1,2 Increasing evidence has shown that tobacco use results in worse outcomes after surgery, and studies have sought to characterize the effect of tobacco use on perioperative morbidity and mortality.3,4 Such complications have been demonstrated in both institutional and database studies in a number of surgical disciplines, including general, 5 plastic,5,6 head and neck, 7 orthopedic,8,9 and cardiac. 10 Within cranial neurosurgery, tobacco use has been associated with increased intraoperative blood loss and wound complications.11,12 Furthermore, in the spine literature, tobacco use has been associated with increased rates of pseudoarthrosis, infection, and wound complications.13-16
Readmission is an important measure of patient outcome and hospital performance, and hospitals maybe be penalized for higher-than-average readmission rates through the Hospital Readmission Reduction Program (HRRP). 17 Accordingly, increasing attention has been paid to understand factors associated with readmission and to develop strategies to reduce readmission. Studies examining readmission after spine surgery have previously identified comorbid conditions, older age, and postoperative complications18-23 as factors associated with readmission.
This study used the Nationwide Readmissions Database (NRD) from 2010 to 2014 to measure 30- and 90-day readmission rates and identify factors related to readmission after degenerative spine surgery. We examined whether tobacco use was independently associated with readmission after adjusting for patient and hospital factors.
Methods
Database
This is a retrospective study utilizing the NRD, a nationally representative database that is maintained through the Healthcare Cost and Utilization Project. The NRD includes data on approximately 50% of all hospitalizations and readmissions in the United States. Each patient in the NRD has a unique identifier link that is used to determine patient hospitalizations and discharges within a calendar year. The NRD was queried from 2010 to 2014. The study period was selected to include the last 5 years of International Classification of Diseases, Diagnosis, and Procedure codes (ICD-9-CM, ICD-9-PCS), prior to the transition to ICD-10 in 2015. Institutional review board approval was not required for this review.
Study Population
Patients aged 18 and older who underwent elective decompression, discectomy, or fusion for cervical or thoracolumbar degenerative spine diseases were included in the study. Patients were identified using ICD-9 diagnosis and procedure codes (Table 1), in accordance with other studies. 24 Patients with traumatic injuries or nondegenerative spine diseases were excluded. Patients who died during index hospitalization were excluded. Patients with missing data for survival or length of stay were also excluded. To allow for sufficient follow-up time, patients discharged in January to November were included in the 30-day readmission cohort; patients discharged in January to September were included in 90-day readmission cohort. As such, fewer patients are represented in the latter group. For patients with multiple readmissions in the study period, only the first nonelective readmission was studied.
ICD-9 Diagnosis and Procedure Codes.
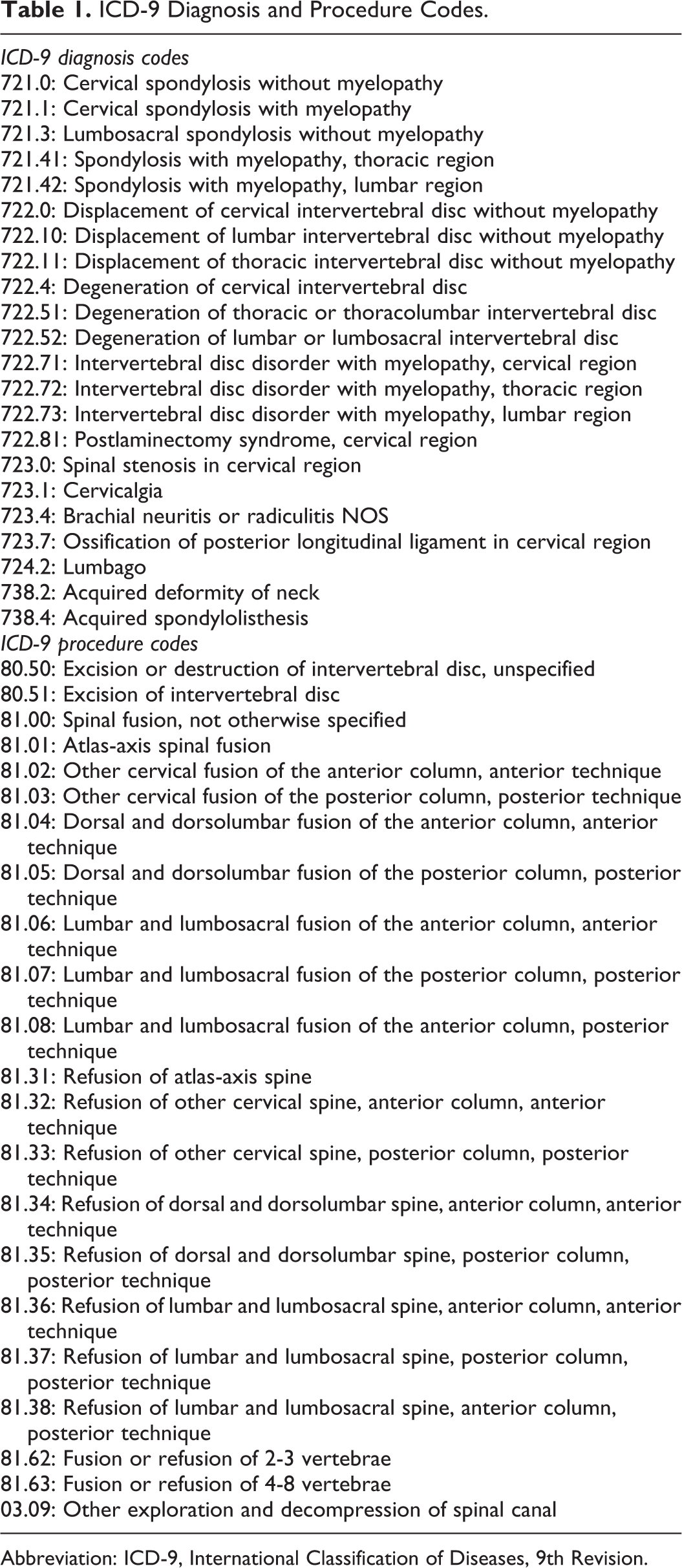
Abbreviation: ICD-9, International Classification of Diseases, 9th Revision.
Patient and Hospital Variables
Patient and hospital variables available in the database were chosen to include in the model based on relevant risk factors previously associated with readmission after spine surgery. Patient demographic factors included gender (male, female), patient age (18-44, 45-59, 60-74, or ≥75 years old), primary insurance type (Medicare, Medicaid, private insurance, self-pay, no-charge, other), median household income (0-25, 26-50, 51-75, 76-100 percentile), length of stay (0-1, 2, 3-4, ≥5 days), and discharge disposition (routine, short-term hospital, transfer, home health care, against medical advice).
In addition, patient comorbidities previously associated with readmission or poor surgical outcomes were identified using the NRD or ICD-9 codes and included presence of Elixhauser comorbidity (yes, no), presence of a medical or neurological complication during initial hospitalization (intracerebral hemorrhage [431 998.11-12], seizures [345.xx], neurological complications after procedure [997.01 997.09]), tobacco use (305.1, V15.82), obesity (278.0, V85.3-V85.4), steroid use (V58.65), systemic inflammatory response syndrome (995.9x, 785.52), chronic lung disease, ventilator dependence (V46.1x), history of chemotherapy (V58.11, V87.41), diabetes (250.xx), and hypercoagulable state (289.81). Hospital variables included procedure volume (>/<90th percentile), hospital bed size (small, medium, large), hospital location (urban, rural), and teaching status (teaching, nonteaching).
Statistical Analysis
Descriptive statistics were used to characterize patient and hospital factors. These factors were then included in a multivariate logistic regression analysis to determine which of these were associated with 30- and 90-day readmissions. Generalized Estimation Equation was used to account for hospital clustering. We used odds ratios (ORs) and 95% confidence intervals (CIs) to report these results, with statistical significance defined as P < .001. Statistical analyses were performed using SAS 9.4 (SAS Inc).
Results
Study Population
A total of 703 051 patients were identified in the 90-day model who underwent surgery for degenerative disease of the cervical or thoracolumbar spine (Table 2). Surgery for degenerative disease of the thoracolumbar spine comprised the majority of operations (61.5%). Overall, 29.0% of patients were tobacco users.
Demographics for Readmission Within 90 Days.
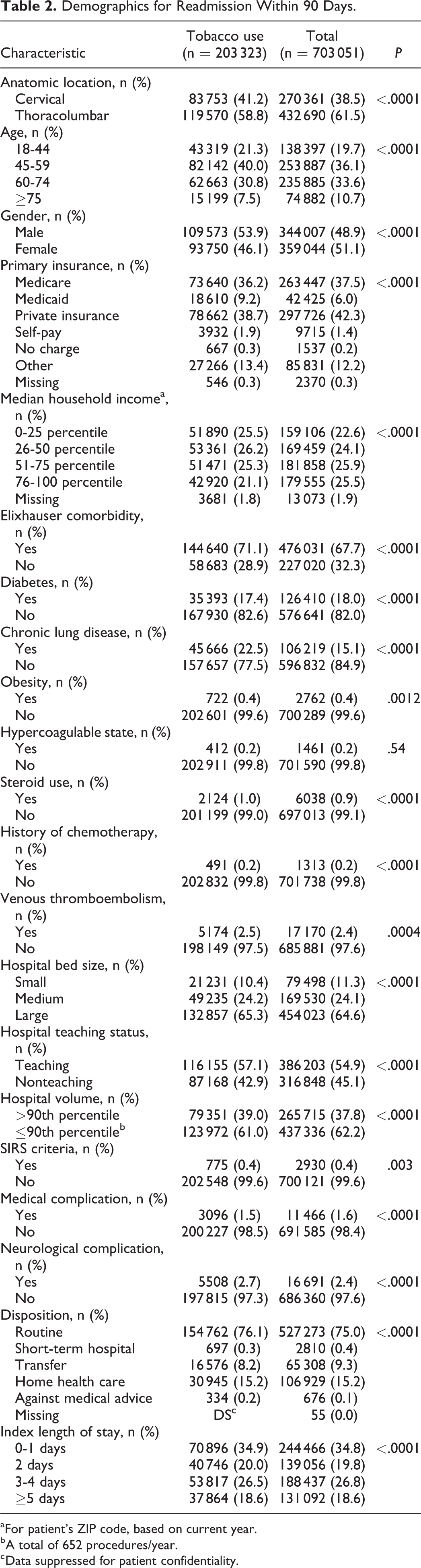
a For patient’s ZIP code, based on current year.
b A total of 652 procedures/year.
c Data suppressed for patient confidentiality.
The overall readmission rate was 4.8% within 30 days and 7.3% within 90 days. The most common reasons for readmission were postoperative infection (12.5% and 9.6% of primary readmission diagnoses, respectively), septicemia (3.5% and 3.5%, respectively), and pneumonia (2.4% and 2.3%, respectively; Table 3).
Primary Diagnoses for 30- and 90-Day Readmission.
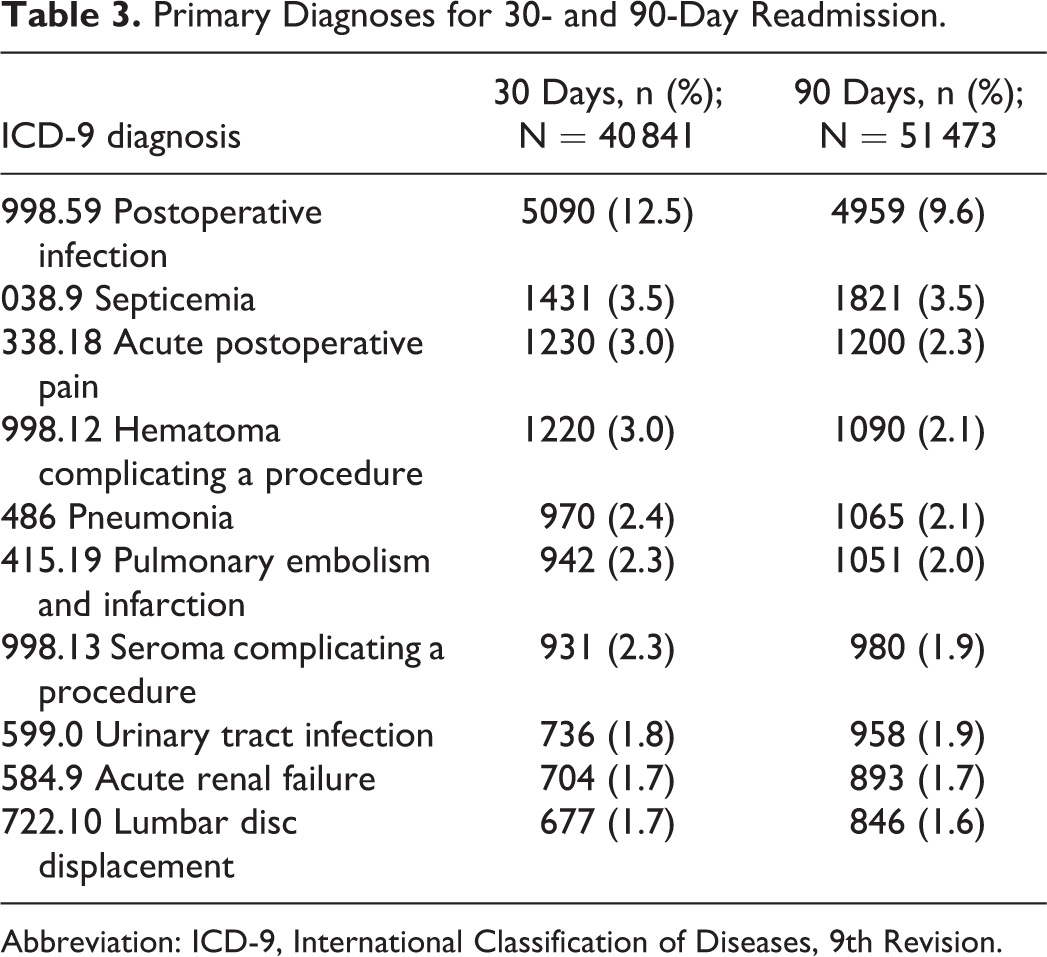
Abbreviation: ICD-9, International Classification of Diseases, 9th Revision.
Tobacco Use Is Associated With 90-Day Readmission
After adjustment for patient- and hospital-level factors, tobacco use was independently associated with increased likelihood of readmission within 90 days (OR 1.05, 95% CI 1.03-1.07, P < .0001). Tobacco use did not meet our preset threshold for significance at 30 days (OR 1.02, 95% CI 1.00-1.05, P = .045; Table 4).
Summary of Associations with 30- and 90-Day Readmission.
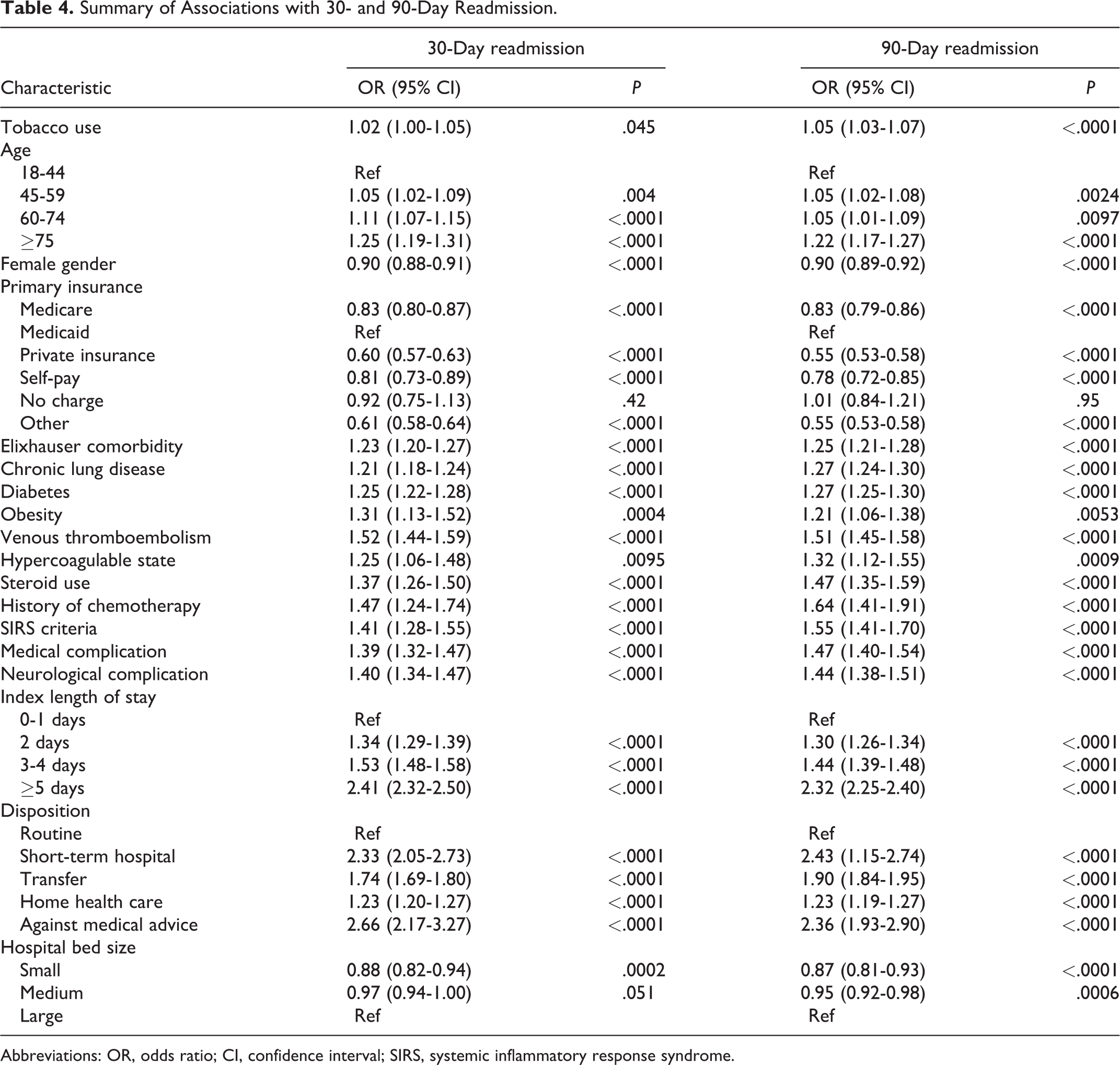
Abbreviations: OR, odds ratio; CI, confidence interval; SIRS, systemic inflammatory response syndrome.
Other comorbidities associated with readmission included older age, male gender, chronic lung disease, diabetes, obesity, venous thromboembolism, hypercoagulability, steroid use, and history of chemotherapy. Insurance other than Medicaid was associated with decreased readmission. Hospitalization factors included SIRS criteria, medical complications, neurological complications, increased index length of stay, and disposition other than routine were associated with increased readmission, while smaller hospital bed size was associated with decreased readmission.
Discussion
This study leveraged the NRD from 2010 to 2014 to investigate tobacco use and other factors associated with 30-day and 90-day readmissions following cervical and thoracolumbar degenerative spine surgery. In this cohort, 4.8% and 7.3% of patients were readmitted within 30 and 90 days, respectively. After adjusting for common causes of readmission, tobacco use was independently associated with readmission within 90 days but not 30 days based on our preset threshold for significance. Postoperative complications including infection contributed to readmissions.
Readmission rates in this study were similar to those reported in other studies for patients undergoing spine surgery. A previous NRD study from January to September 2013 reported a 30-day readmission rate of 5.4% and a 90-day readmission rate of 10% for patients following elective posterior cervical spine surgery for degenerative conditions. 25 Additional studies have estimated 30-day readmission rates between 3.2% and 12.9% and 90-day readmission rates between 5.6% and 12.7%.13,19-22,26-29 This study is the first to isolate the effect of tobacco use on readmission among spine patients.
Surprisingly, prior retrospective studies in specific subsets of patients have failed to find an association between tobacco use and readmission. For example, a single-institution analysis of 839 patients undergoing elective complex spinal fusion did not find an association between tobacco use and readmission. 26 Similarly, there was no association between tobacco use and readmission in 2207 patients undergoing surgery for spinal tumors. 19 Last, a study of 2761 patients readmitted within 90 days following spine surgery for degenerative disease found no association in multivariable analysis. 28 These studies differ from the current study in that the sizes of the cohorts were smaller, which may explain the difference.
Postoperative complications such as infection, septicemia, and pain were the most common reasons for readmission in this study. Tobacco use is a known risk factor for these adverse health events. Tobacco use has been shown to increase surgical site infections following spine surgery.15,30-33 The same trend has been noted in additional surgical specialties.6-8,10 When investigating all surgeries, tobacco use has been associated with increased rates of sepsis and 30-day mortality. 32 Given these reports, it is surprising that there was not a clear relationship between tobacco use and 30-day readmission in this study. Nonetheless, studies have suggested that factors intrinsic to tobacco use may contribute to delayed wound healing and increased risk of infection. For example, nicotine induces vasoconstriction and tissue hypoxia, disrupting angiogenesis, and cigarette smoke impairs neutrophil and monocyte migration and chemotaxis.26,34 A retrospective study leveraging the National Surgical Quality Improvement (NSQI) database from 2012 to 2014 found that surgical site infections were the most common cause for readmission after spine surgery. 20 Tobacco use thus likely contributes to readmissions by increasing the risk and incidence of infection.
Smokers also exhibit poorer outcomes, increased postoperative pain, and decreased satisfaction following spinal surgery.35,36 Two years following surgery for lumbar spine stenosis, smokers had a higher Owestry Disability Index (a marker of inferior quality of life), increased leg and back pain, and decreased walking ability compared to nonsmokers. 35 This suggests that long-term outcomes in smokers are also affected.
Some studies with smaller sample sizes have failed to identify an association between tobacco use status and postoperative complications. A retrospective study of patients following spinal fusion found no difference in 30-day complication rates including pain, wound dehiscence, and wound drainage in smokers compared to nonsmokers. 26 A study utilizing the NSQI from 2006 to 2010 found no association between tobacco use and major complications after elective spine surgery, but patients who were current smokers with more than 60 pack-year histories were more likely to die within 30 days of surgery. 37 This suggests that the adverse effects of tobacco use may to some extent be dose dependent. Unfortunately, the NRD does not stratify details of tobacco use such as pack-year history.
It has long been advocated that smoking cessation should be encouraged prior to spine surgery. Studies have suggested that up to 75% of tobacco users who undergo surgery have the desire to quit.3,38 Patients who quit tobacco use after surgery for longer than 6 months following spinal fusion had decreased rates of nonunion and increased patient satisfaction and return to work rates compared to those who continued to smoke.39,40 In one orthopedic study, preoperative smoking intervention 6 to 8 weeks before surgery, including cessation counseling and nicotine replacement therapy, was associated with decreased postoperative complication rates in patients undergoing hip or knee alloplasty. 41 Across surgical specialties, one meta-analysis found that preoperative tobacco use cessation was associated with a 41% risk reduction of postoperative complications. 42
Limitations
This retrospective study utilized the NRD, which is subject to coding errors and information bias. The NRD may underestimate true readmission rates, as it only contains data on patients who were readmitted in the same state. In addition, this study is limited by the ICD-9 diagnosis and procedure codes available through the NRD. To overcome this limitation, we included numerous diagnoses and surgical procedures in this study to ensure a heterogeneous group of patients undergoing degenerative spine surgery were included in the analysis. As a result of this, conclusions cannot be drawn regarding the effects of tobacco use on specific spine surgeries and patient conditions. Relatedly, the lack of granularity on surgical details precludes the specific study of factors such as surgical time and incision size which are related to complication rates. Additionally, due to the transition in ICD coding between the 9th and 10th editions, our analysis does not include the most recent years (2015-2017) of NRD data.
As both current and former tobacco users were included in this study, the effect of tobacco use cessation cannot be quantified by this type of analysis. Given that pre- and postoperative smoking cessation have been shown to decrease rates of postoperative complications, it is possible that the effect of tobacco use on rates of readmission may be even higher in active smokers. Finally, this study did not separately assess the use of e-cigarettes. More study is warranted for this increasingly prevalent condition.
Conclusions
This study identified tobacco use as a modifiable risk factor for readmission after elective spine surgery for degenerative conditions. These data be used to aid in patient selection and perioperative planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Mack—Consultant: Rebound Therapeutics, Viseon Imperative Care, Q’Apel, Medtronic, Stryker, Stream Biomedical, Spartan Micro; Investor: Cerebrotech, Endostream, Viseon, Rebound, Q’Apel, and Spartan Micro. Dr Liu—Viseon (consultancy). The authors declare no additional disclosures or conflicts of interest related to this work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.