
Abstract
Study Design:
Retrospective comparative study.
Objective:
Assessment of difference in clinical and computer tomographic outcomes between the 2 cohorts.
Methods:
Computer tomographic evaluation by Bridwell’s grade, Kim’s stage, Kim’s subsidence grade and clinical evaluation by VAS, ODI and McNab’s criteria on both cohorts.
Results:
33 levels of Endo-TLIF and 22 levels of TLIF were included, with a mean follow up of 14.3 (10-24) and 22.9 (13-30) months respectively. Both Endo-TLIF and TLIF achieved significant improvement of pain and ODI at post-operative 4 week, 3 months and at final follow up with VAS 4.39 ± 0.92, 5.27 ± 1.16 and 5.73 ± 1.21in Endo-TLIF and 4.55 ± 1.16, 5.05 ± 1.11 and 5.50 ± 1.20 in TLIF respectively and ODI at post-operative 1 week, 3 months and final follow up were 43.15 ± 6.57, 49.27 ± 8.24 and 51.73 ± 9.09 in Endo-TLIF and 41.73 ± 7.98, 46.18± 8.46 and 49.09 ± 8.98 in TLIF respectively, P < 0.05. Compared to TLIF, Endo-TLIF achieved better VAS with 0.727 ± 0.235 at 3 months and 0.727 ± 0.252 at final follow up and better ODI with 3.88 ± 1.50 at 3months and 3.42 ± 1.63 at final follow up, P < 0.05. At 6 months radiological evaluation comparison of the Endo-TLIF and TLIF showed significant with more favorable fusion rate in Endo-TLIF of −0.61 ± 0.12 at 6 months and −0.49 ± 0.12 at 1 year in Bridwell’s grading and 0.70 ± 0.15 at 6 months and 0.56 ± 0.14 at 1 year in Kim’s stage.There is less subsidence of 0.606 ± 0.18 at 6 months and −0.561 ± 0.20 at 1 year of Kim’s subsidence grade, P < 0.05.
Conclusion:
Application of single level uniportal endoscopic posterolateral lumbar interbody fusion achieved better clinical outcomes and fusion rate with less subsidence than microscopic minimally invasive transforaminal lumbar interbody fusion in mid-term evaluation for our cohorts of patients.
Keywords
Introduction
Evolution of endoscopic spine surgery has brought more types of minimally invasive techniques to lumbar spine surgery. 1 There are variable options of lumbar decompression and discectomy surgery through the transforaminal and interlaminar approaches.2-6 Endoscopic Lumbar Transkambin fusion is popular for being facet preserving lumbar fusion surgery and having the potential of being done under local anesthesia with monitored sedation. However, there are doubts about the increased subsidence rate and exit nerve root injury related to Transkambin route of endoscopic fusion technique. There is also the concern of the limitation on the usage of small width footprint cage recommended for fusion cage introduction from Transkambin route of approach.7-9 Facet sacrificing transforaminal lumbar interbody fusion is a popular technique in open, minimally invasive approach and biportal endoscopic assisted fusion.10-12 There is limited literature on uniportal endoscopic posterolateral lumbar interbody fusion with complete facet resection. 13 Kim and Wu et al described the used of uniportal full endoscopic approach to perform posterolateral transforaminal lumbar interbody fusion(Endo-TLIF) with facet resection in grade 2 spondylolisthesis, scoliosis of less than 30degrees curve and severe foraminal stenosis patients .14-16 In this study, we aimed to perform comparative cohort study to evaluate the fusion rate, subsidence rate and clinical outcomes of Endo-TLIF in comparison to Microscopic Minimally Invasive Transforaminal Lumbar Interbody fusion (TLIF) for single level lumbar interbody fusion.
Materials and Methods
Indication, Inclusion and Exclusion Criteria
This retrospective study was reviewed by institutional review board of Nanoori Hospital, Seoul, Republic of Korea(NR-IRB 2020-008). Informed consent was obtained from all patients participated in study
The inclusion criteria of single level Uniportal Endoscopic Posterolateral Lumbar Interbody Fusion (Endo-TLIF) surgeries and Microscopic Minimally Invasive Transforaminal Lumbar Interbody Fusion (TLIF) were patients who presented with neurogenic claudication and back pain who had failed minimum 6 weeks of conservative treatment with either 1 or more of the following findings: 1) grade 2 and below spondylolisthesis 2) spinal stenosis with and without instability 3) adjacent segment disease 4) recurrent disc herniation.
The exclusion criteria were patients who had spinal fusion surgery due to trauma, revision spinal fusion surgery, tumor, infection, pseduoarthrosis, congenital spinal deformity, sagittal malalignment and coronal malalignment with more than 10 degrees coronal curve.
The cohort of patients who underwent single level TLIF was performed in the period of February 2018 to July 2019 while the cohort of patients who underwent single level Endo-TLIF was performed in the period of October 2018 to February 2020.
In the interim early learning curve period of Endo-TLIF from October 2018 to July 2019, the authors do single level fusion alternating between Endo-TLIF and TLIF to assess possible clinical outcomes and complications of this new technique before complete switch to Endo-TLIF from July 2019.
We collected baseline demographics data and analyzed clinical outcomes of Visual Analogue Scale and Oswestry Disability Index at preoperative, 4 weeks postoperative, 3months postoperative and final follow up. MacNab’s criteria was evaluated at final follow up.
Computer tomographic assessment was performed at preoperative, postoperative 1 day 6months and at 1 year. The stages of fusion were quantified by Bridwell classification and a novel classification of 4 stages of Kim’s classification. Bridwell grade I is fused with remodeling and trabeculae present; grade II is graft intact, not fully remodeled and incorporated, but no lucency present; grade III is graft is intact, potential lucency present at top and bottom of the graft; grade IV is fusion absent with collapse and graft resorption. 17 Kim’s stage 1 lumbar fusion classification is end plate preserved stage when end plate is clearly defined directly related to the top and bottom of the cage, graft in the cage is not continuous with bone at end plate; stage 2 is end plate opening stage showed there is an opening with no clear definition of the rim of endplate bone directly above and below the cage, graft in the cage is not continuous with the endplate bone; stage 3 is bilateral sclerosis stage when both the end plates adjacent to the cage showed some sclerosis, graft in the cage is partly continuous with the end plate; stage 4 is fusion bridge formations stage when there is extensive sclerosis on the superior and inferior endplate which is continuous with the graft within and/or adjacent to the cage.(Figure 1)
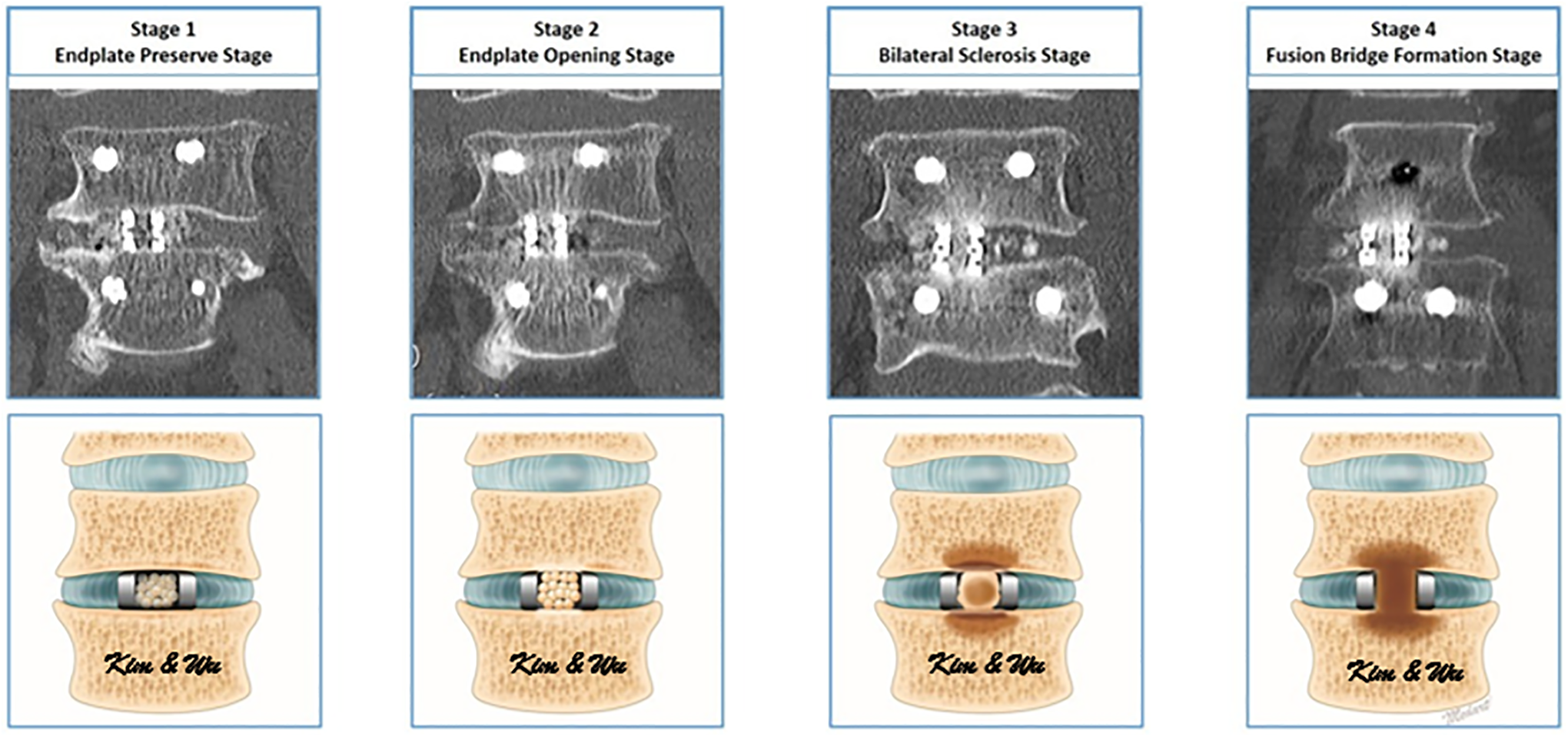
CT coronal view and illustrative drawing of Kim’s stages of interbody fusion. Kim’s stage 1 lumbar fusion classification is end plate preserved stage when end plate is clearly defined directly related to the top and bottom of the cage, graft in the cage is not continuous with bone at end plate; stage 2 is end plate opening stage showed there is an opening with no clear definition of the rim of endplate bone directly above and below the cage, graft in the cage is not continuous with the endplate bone; stage 3 is bilateral sclerosis stage when both the end plates adjacent to the cage showed some sclerosis, graft in the cage is partly continuous with the end plate; stage 4 is fusion bridge formations stage when there is extensive sclerosis on the superior and inferior endplate which is continuous with the graft within and/or adjacent to the cage.
CT evaluation for subsidence based on the amount of vertebral body height involvement of subsidence in either cephalad or caudal vertebra at the latest CT scan. Grade 0 is no subsidence with intact endplate and no loss of vertebral height caused by subsidence of cage. Grade 1 is mild subsidence with less than 10% of vertebral body in either cephalad or caudal vertebral body. Grade 2 is 10-24% subsidence in either cephalad or caudal vertebral body. Grade 3 is more than 25% subsidence in either cephalad or caudal vertebral body. (Figures 2 and 3)
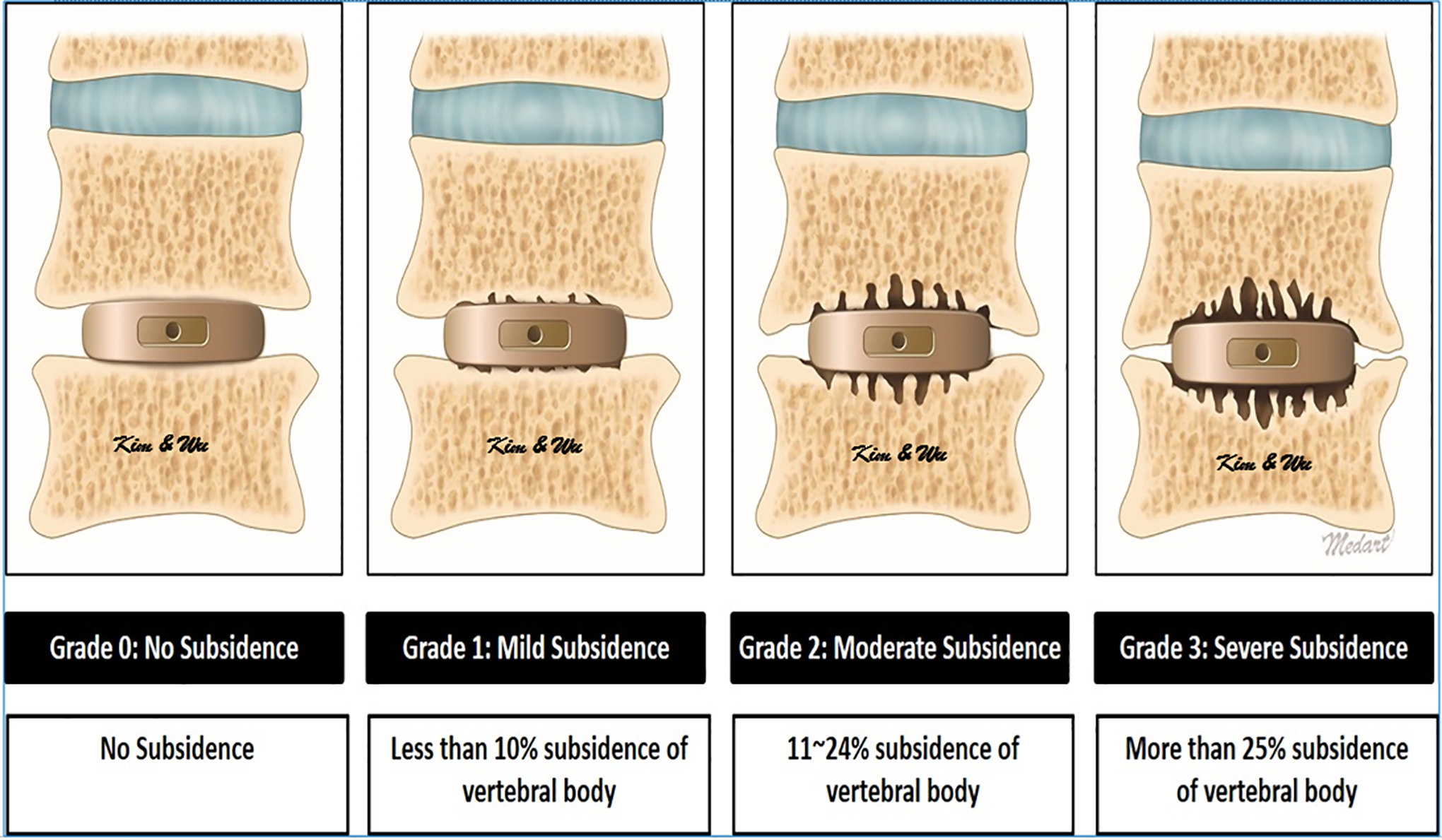
Illustrative drawing of grades of subsidence.
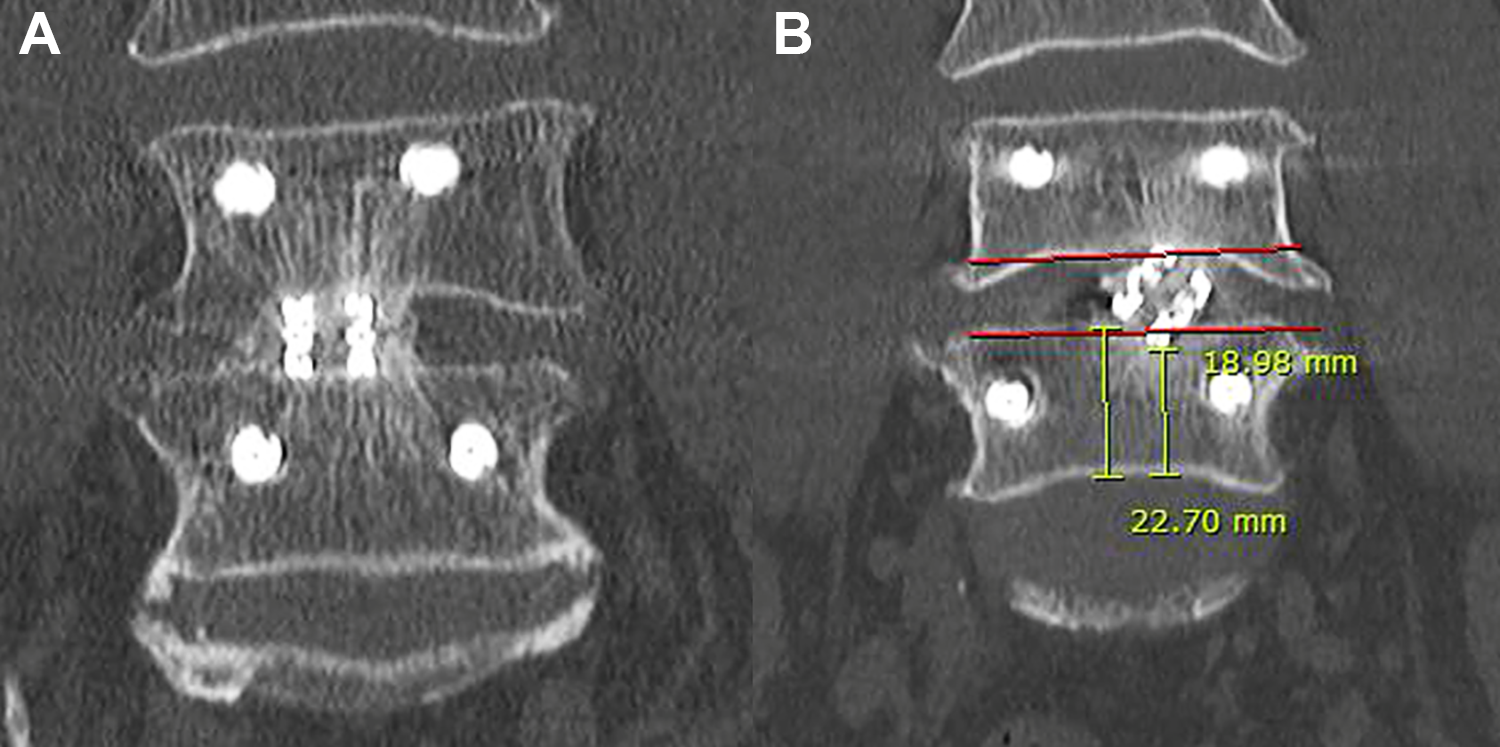
Mid coronal CT scan. Figure 3A showed no subsidence, grade 0 with intact end plate. Figure 3B showed subsidence of the endplate with cage tilted laterally, 16% subsidence (grade 2) was measured.
Surgical Technique of Endo-TLIF
Endo-TLIF technique had been described in 3 separate papers.14-16 A brief description is highlighted here.
Surgical Procedure
The procedure could be performed with either epidural anesthesia with sedation or general anesthesia. The patient was positioned prone on a Wilson Frame on top of a radiolucent operating table with the spine in slight flexion during end plate preparation and cage insertion. The flexion would be reversed after cage was inserted by lowering the height of Wilson frame prior to reduction maneuvers and rod insertion. The endoscopic procedure was performed under 25-40 mmHg of irrigation fluid pressure. The side of uniportal endo-TLIF was decided to be concordant to the patient’s symptomatic side. We used irrigation pump to achieve this pressure. We did Endo-TLIF with cage insertion prior to percutaneous pedicle screws fixation. We used skin incision on the cephalad vertebral pedicle of the symptomatic side and level for the uniportal endoscope work. A vertical 1.6 cm skin incision was made at the ipsilateral cephalad vertebral pedicle . A 3 cm fascia incision was made deep to the skin incision to allow mobility of the working channel. Guidewire was placed through skin and fascia incision and docked on isthmus. Serial dilations were made with obturators followed by insertion of a 13.7 mm outer diameter beveled tip working cannula. We performed an intraoperative anteroposterior and lateral view at this point of time to confirm the correct level of interbody fusion. We then inserted a outer diameter 10 mm,150 viewing angle, 6 mm diameter working channel and 125 mm working length endoscope to begin surgical procedure.
Facetectomy was performed with an endoscopic drill. We first completed inferior articular facetectomy. The bone was harvested as an autograft. We followed by harvesting superior articular facetectomy. We drilled the ipsilateral cranial lamina followed by caudal lamina to expose the margins of ligamentum flavum and removed the ligamentum flavum. We performed over the top decompression of contralateral side. The contralateral ligamentum flavum and ipsilateral ligamentum flavum were removed en bloc respectively with endoscopic forceps after bony decompression was completed. Hemostasis was achieved with radiofrequency ablator. The neural elements were inspected for adequacy of decompression. Disc was exposed. We rotated and advanced the open beveled working cannula of 13.7 mm outer diameter and 10.2 mm inner diameter and placed it directly on the disc while pointing the open bevel away from exiting and traversing nerve. Radiofrequency ablator was used to perform annulotomy. We performed complete denudation of the end plate cartilage and demonstrated punctate bleeding of subchondral bone while preserving as much subchondral bone as possible for optimal fusion bed preparation using endoscopic drill, probe and forceps. Once end plate preparation was complete, working cannula was further advanced into the intervertebral disc space with the tip of working cannula reaching to the dorsal third of the disc space. Endoscope was then withdrawn with the working cannula in place. We packed bone graft admixture of autograft and allograft to the ventral and contralateral disc space under fluoroscopic guidance. A trial was used to test the appropriate size of cage for insertion and to compact the bone graft in the intervertebral disc space. Under fluoroscopic guidance, we inserted the appropriate size GENOSS 3D PrintedCage™ Lumbar Cage(Gyeonggi-do South Korea) packed with autograft into the disc space through the same working cannula or a Harrison cage glider, which protected the exiting and traversing nerve root while gently retracting it to provide enough space for introduction of the cage. We checked on the status of neural decompression and the position of the cage with endoscope and further adjust the cage into optimal position using a punch under direct endoscopic vision. Drain was inserted under direct endoscopic vision and anchored with suture. Drain would be removed on post-operative day 1.
After cage insertion was completed, the Wilson frame was released, percutaneous pedicle screws were inserted under fluoroscopic guidance in standard fashions with or without cement augmentation. We introduced 2 bent rods of appropriate length and lordosis through the percutaneous rod. We performed compression and final tightening of the set screws and closed the wound in layers. (Figure 4)
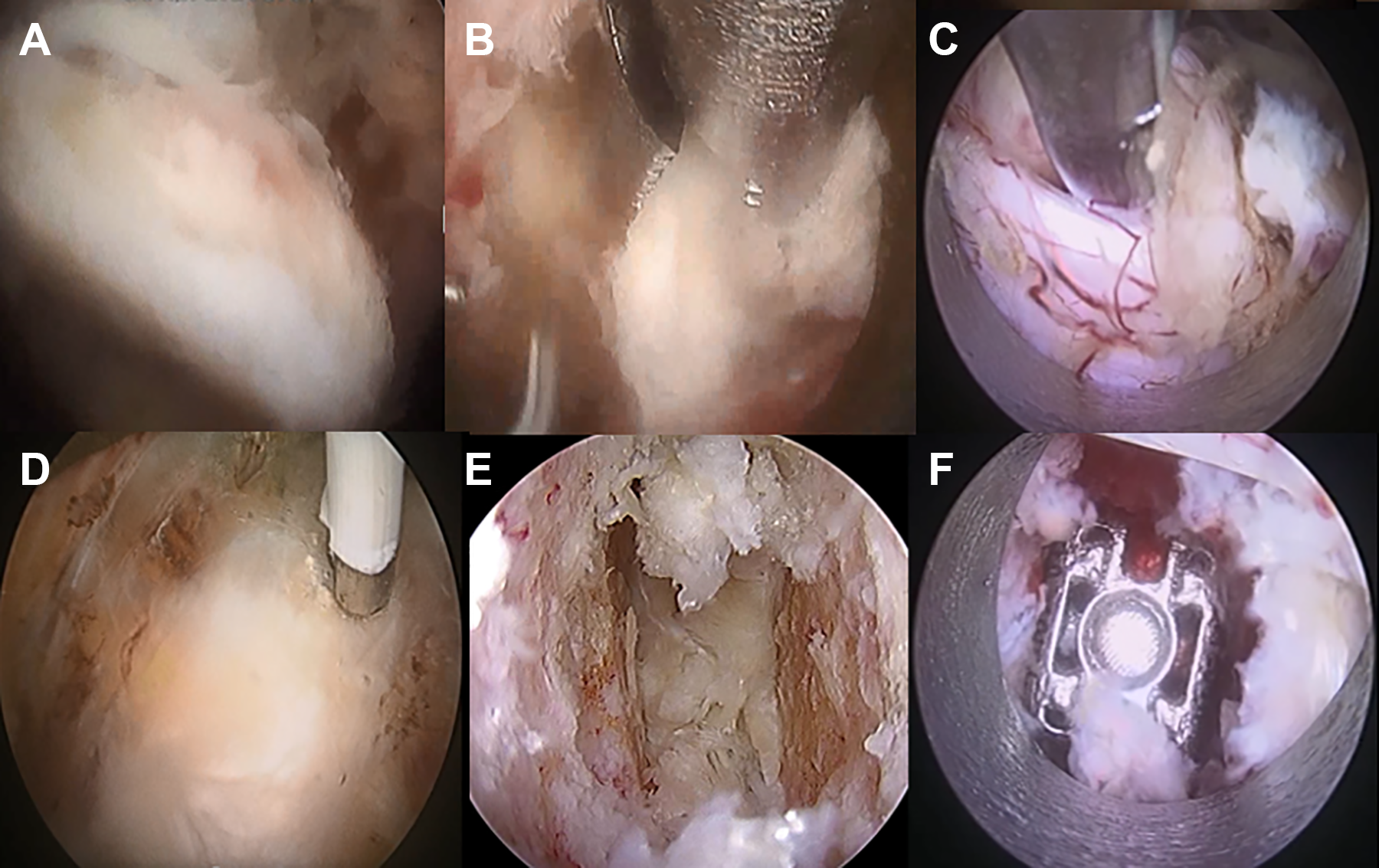
Steps of endo-TLIF. Figure 4A: Endoscopic inferior facetectomy. Figure 4B: Endoscopic superior facetectomy. Figure 4C: Exposure of traversing nerve root. Figure 4D: Discectomy . Figure 4E: Denudation of end plate cartilages. Figure 4F: 3 D printed cage inserted.
Surgical Technique of Microscopic Minimally Invasive Transforaminal Lumbar Interbody Fusion
Patient is positioned prone on Wilson frame and underwent general anesthesia. TLIF procedure was performed on the symptomatic side. After a vertical skin incision in midline, subdermal dissection to the lateral aspect of symptomatic pedicle. Wiltse paraspinal approach to the facet was performed using self-retaining retractors. After a complete facetectomy with burr and Kerisson rongeur, the ligamentum flavum was removed to expose the lateral border of the ipsilateral traversing nerve root. The retractor was angled medially, the patient was tilted laterally to decompress the contralateral side if necessary. Extensive decompression was performed, which included decompression of the central stenosis and contralateral side. A discectomy was also performed under microscopy. A polyetheretherketone banana cage filled with only autologous local bone was inserted. After interbody fusion, the retractor was removed, and the same procedure was repeated for each segment. Ipsilateral percutaneous pedicle screws were inserted through the same skin incision. Contralateral percutaneous pedicle screws were placed after subdermal dissection under fluoroscopic guidance. Epidural catheter insertion for postoperative pain control was done prior to closure. Closure in layers done with wound drain placed. All our cases we inserted percutaneous pedicle screws and rods under fluoroscopic guidance.
Statistical Analysis
Clinical data was analyzed with SPSS version 18 statistical analysis software (IBM corporation, New York). The continuous variables were expressed as mean and standard deviation (SD). The paired t test was used for comparison of pre-operative and post-operative radiological Cobb’s angle results. Clinical visual analogue scale(VAS), Oswestry Disability Index(ODI) were measured at pre-operative, 4 weeks post-operative, 3 months post-operative and final follow up as well as MacNab’s score at final follow up reported by the patients were analyzed with paired t test. A value of (P < 0.05) considered significant within each group of data. Independent T test was used to compare the clinical data of VAS and ODI and radiological Computer Tomographic Bridwell grades, Kim’s fusion stage and subsidence grade
Results
Baseline Demographics
During October 2018 to February 2020, a total of 33 single levels Endo-TLIF were performed in patients who met the inclusion and exclusion criteria. For Endo-TLIF cohort, the mean age was 63(39-82) years old with a mean follow up of 14.3 (10-24) months. There were 14 male and 19 female in this group of patients. Two L2/3, 4 L3/4, 20 L4/5 and 7 L5/S1 Endo-TLIF were done. 32 patients underwent general anesthesia and 1 underwent epidural anesthesia for the surgery. 1 level were fused for spinal stenosis, 28 levels were fused for spondylolisthesis, and4 levels were fused for instability
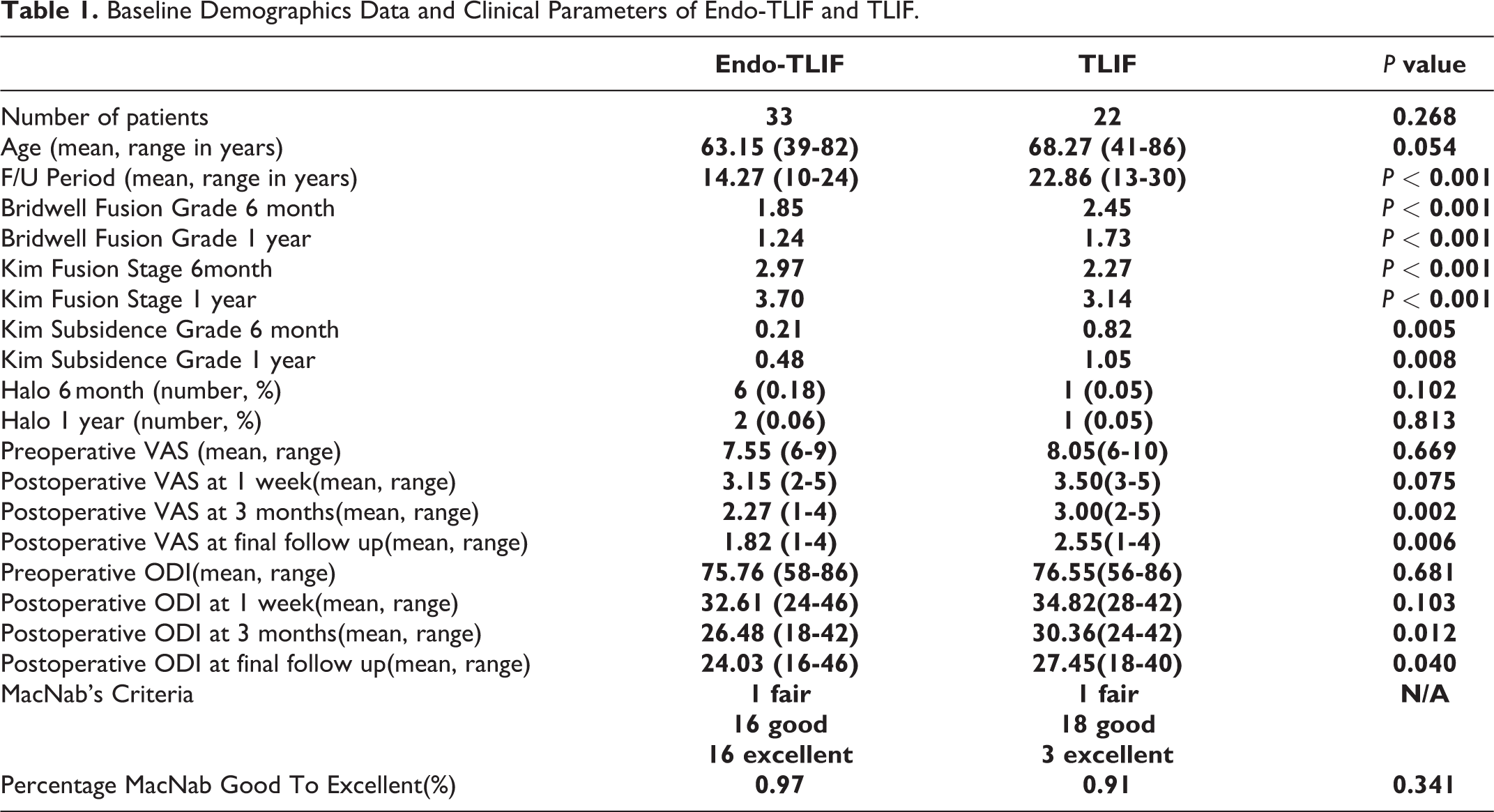
For TLIF cohort, a total of 22 patients with single level TLIF were performed during February 2018 to July 2019 in patients who met the inclusion and exclusion criteria. The mean age was 68(41-86) years old with a mean follow up of 22.9 (13-30) months. There were 7 male and 15 female in this group of patients. 2 L1/2, 1 L2/3, 5 L3/4, 12 L4/5 and 2 L5/S1 Endo-TLIF were done. 13 patients underwent general anesthesia and 22 patients underwent epidural anesthesia for the surgery. 3 patients were fused for spinal stenosis, 16 levels were fused for spondylolisthesis, 2 levels were fused for instability and 1 levels for disc herniation. The follow up for TLIF was longer than Endo-TLIF. There were no significant difference in baseline demographics between the 2 cohorts. (Table 1)
Baseline Demographics Data and Clinical Parameters of Endo-TLIF and TLIF.
Clinical Outcomes
In terms of complications for Endo-TLIF, we had 2 complications(6%) with one retained drain tip which was removed under local anesthesia and one incidental durotomy which required dural patch blocking repair. 18 No revision was required for this patient who had incidental durotomy. He achieved good McNab’s criteria outcome and had improvement of his preoperative symptoms without neurological sequelae. There were no neurological complications in the Endo-TLIF group of patients.
In terms of clinical results, preoperative, 1week post-operative, 3months post-operative and final follow up Visual Analog Scale score had the mean and range of 7.54(6-90), 3.15(2-5), 2.27(1-4) and 1.82 (1-4) respectively. The preoperative, 1 week post-operative, 3months post-operative and final follow up Oswestry Disability Index had the mean and range of 75.8 (58-86), 32.6 (24-46), 26.5(18-42) and 24.0 (16-46) respectively. In terms of MacNab’s criteria, 1 had fair, 26 had good and 20 patients with excellent scores with 97.0% good to excellent score. (Table 1)
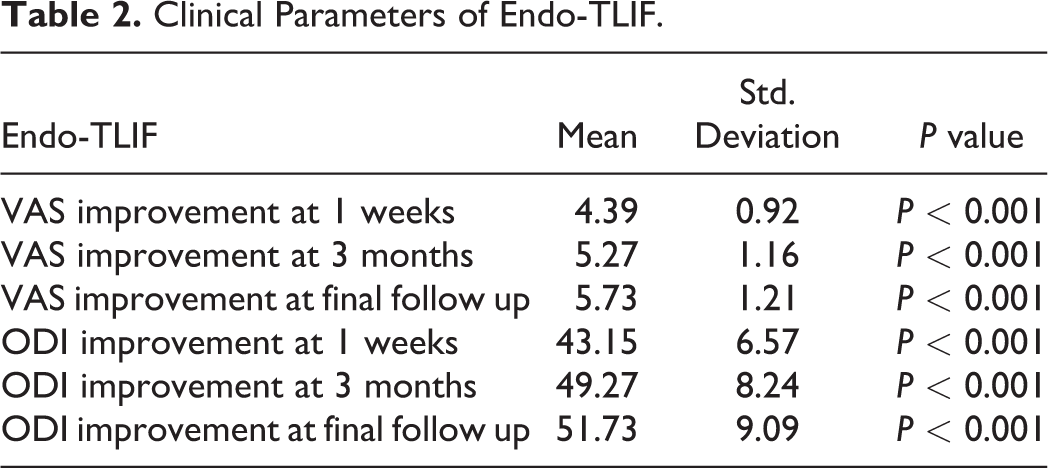
When we compared with preoperative VAS score, there was statistically significant improvement of VAS score with mean ± standard deviation of 4.39 ± 0.92at1week, 5.27 ± 1.16 at 3months and 5.73 ± 1.21 at final follow up, P < 0.05. When we compared with preoperative ODI score, there was statistically significant improvement of ODI score with mean ± standard deviation of 43.15 ± 6.57 at 1 week, 49.27 ± 8.24 at 3 months and 51.73 ± 9.09 at final follow up, P < 0.05. (Table 2)
Clinical Parameters of Endo-TLIF.
In terms of clinical evaluation for TLIF, we had 3 complications(13.6%) with one deep infection which was debrided under general anesthesia, one hematoma collection which required wash out procedure under general anesthesia and one incidental durotomy (1.8%) which required dural patch blocking repair. 18 There were no neurological complications.
In terms of clinical results, preoperative, 1 week post-operative, 3months post-operative and final follow up Visual Analog Scale score had the mean and range of 8.05 (6-10), 3.5 (3-5), 3 (2-5) and 2.55 (1-4) respectively. The preoperative, 1 week post-operative, 3months post-operative and final follow up Oswestry Disability Index had the mean and range of 76.5 (56-86), 34.8 (28-42), 30.4 (24-42) and 27.5 (18-40) respectively. In terms of MacNab’s criteria, 2 had fair, 30 had good and 3 patients with excellent scores with 95.5% good to excellent score. (Table 1)
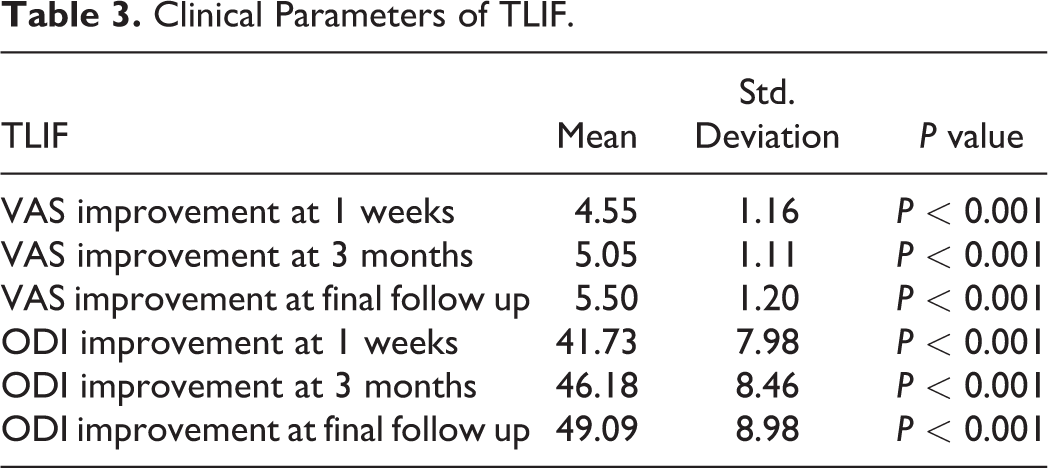
When we compared with preoperative VAS score, there was statistically significant improvement of VAS score with mean ± standard deviation of 4.55 ± 1.16 at 1 week, 5.05 ± 1.11 at 3months and 5.50 ± 1.20 at final follow up, P < 0.05. When we compared with preoperative ODI score, there was statistically significant improvement of ODI score with mean ± standard deviation of 41.73 ± 7.98 at 1 week, 46.2 ± 8.46 at 3 months and 49.1 ± 8.98 at final follow up, P < 0.05. (Table 3)
Clinical Parameters of TLIF.
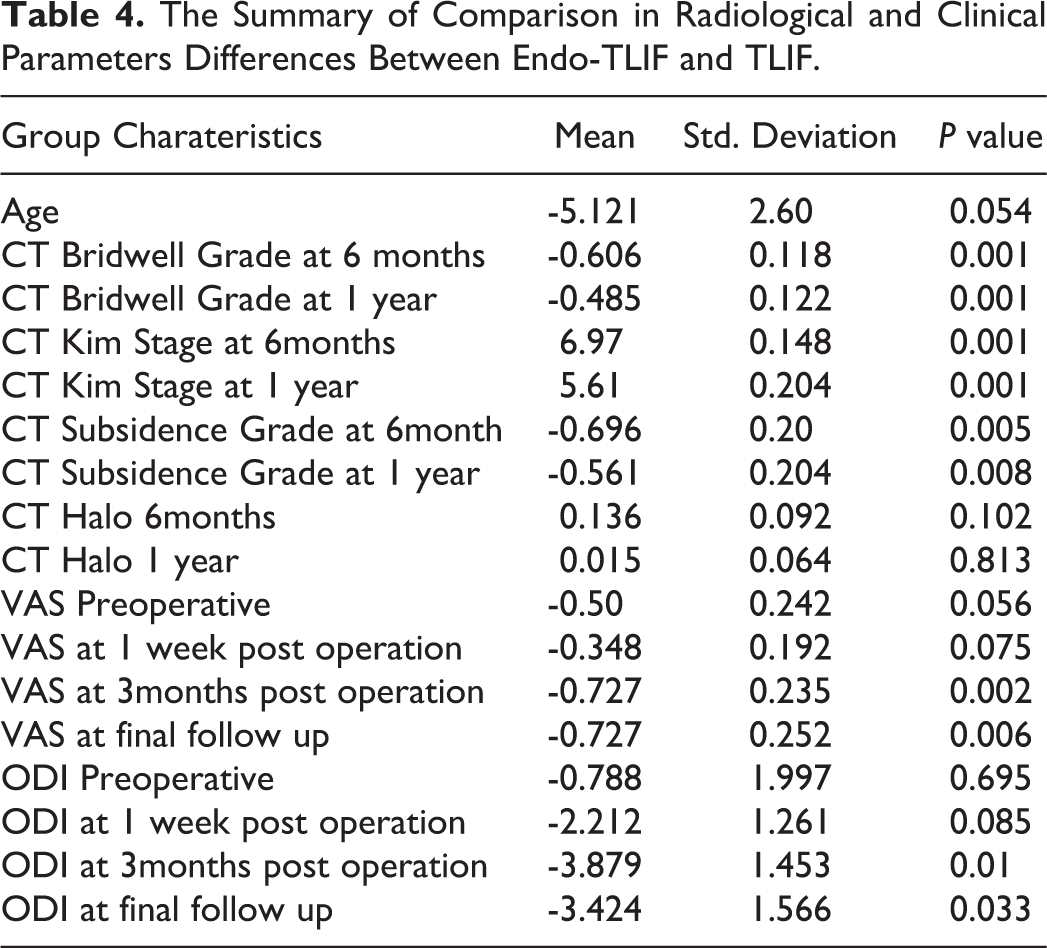
Comparing the clinical results of Endo-TLIF and TLIF, there was statistically significant improvement of Endo-TLIF performed better than TLIF in terms of VAS at 3months, 0.727(±0.235); at 1 year 0.727(±0.252) and ODI at 3months, 3.88(±1.45) and at 1 year, 3.42(±1.57), P < 0.05. There was no statistically significant difference between the 2 cohorts in terms of percentage of McNab’s score in good and excellent outcomes as well as VAS and ODI improvement in other periods. (Tables 1 and 4)
Radiological Outcomes
In terms of radiological results, in Endo-TLIF group, the position of implants are satisfactory in all cases, with no revision required. In follow up computer tomography scan, Bridwell Fusion grade were assessed to be 1.85(1-2) at 6 months and 1.24(1-2) at 1 year; at, Kim’s fusion stage of 2.97(2-4) at 6 months and 3.70(2-4) at 1 year and Kim’s subsidence grade of 0.21(0-2) at 6 months and 0.48(0-2) at 1 year . (Figure 5) There were 6 CT findings of halo phenomenon in Endo-TLIF groups at 6months and 2 at 1 year. (Figure 6)
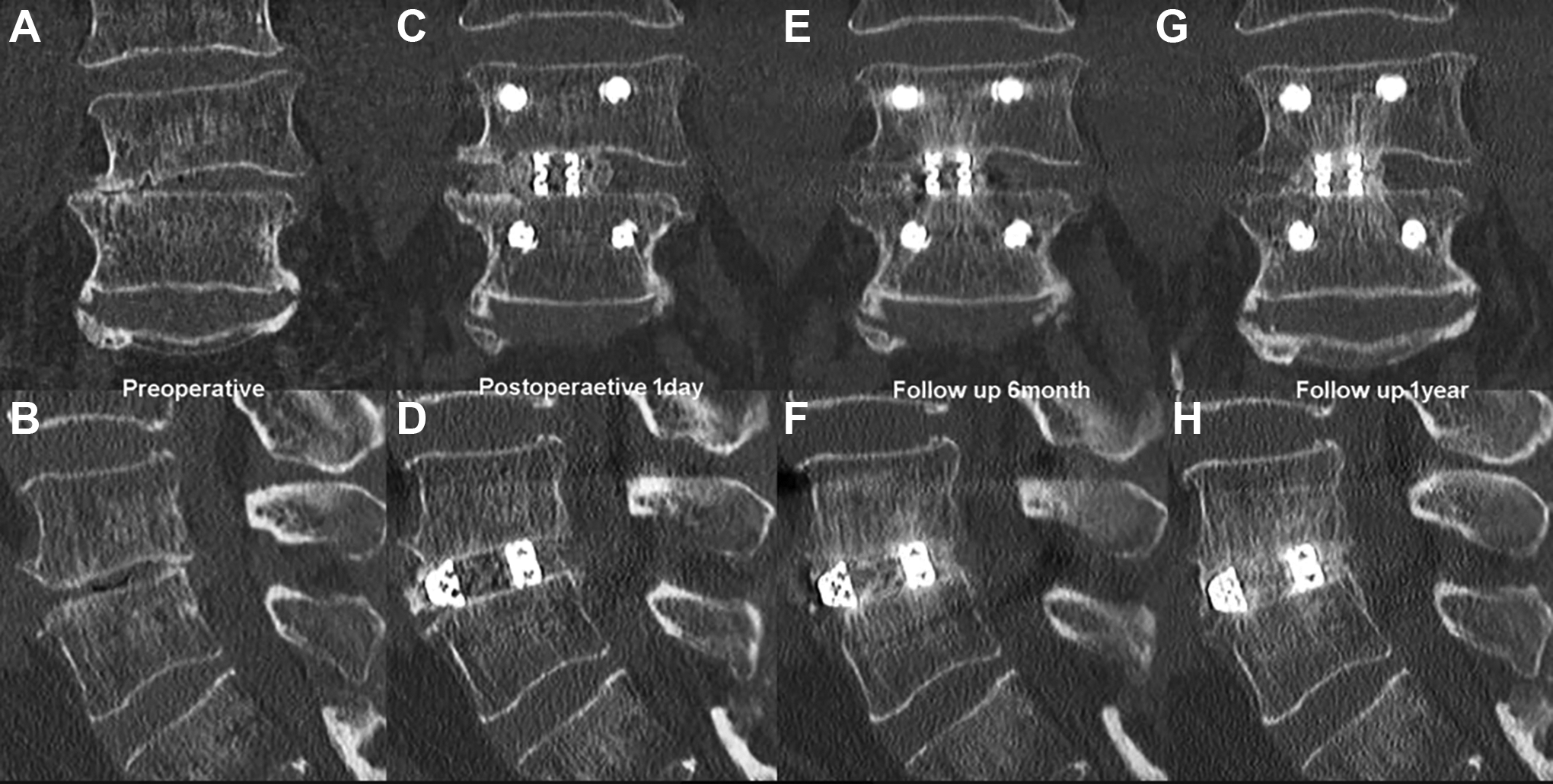
Computer tomographic scan sagittal and coronal views follow up evaluation of a 62 years old man with right L4/5 Endo-TLIF. Figure 5A and 5: preoperative sagittal and coronal view of L4/5 degenerative disc disease with foraminal stenosis. Figure 5C and D: postoperative day 1 CT sagittal and coronal view of a left L4/5 Endo-TLIF with a optimal size cage and sufficient bone graft. Figure 5 E and F: sagittal and coronal postoperative 6 months CT scan showed a Bridwell grade 2, Kim’s stage 3 fusion. Figure 5 G and H: sagittal and coronal postoperative 1 year CT scan showed a Bridwell grade 1, Kim’s stage 4 fusion without subsidence.
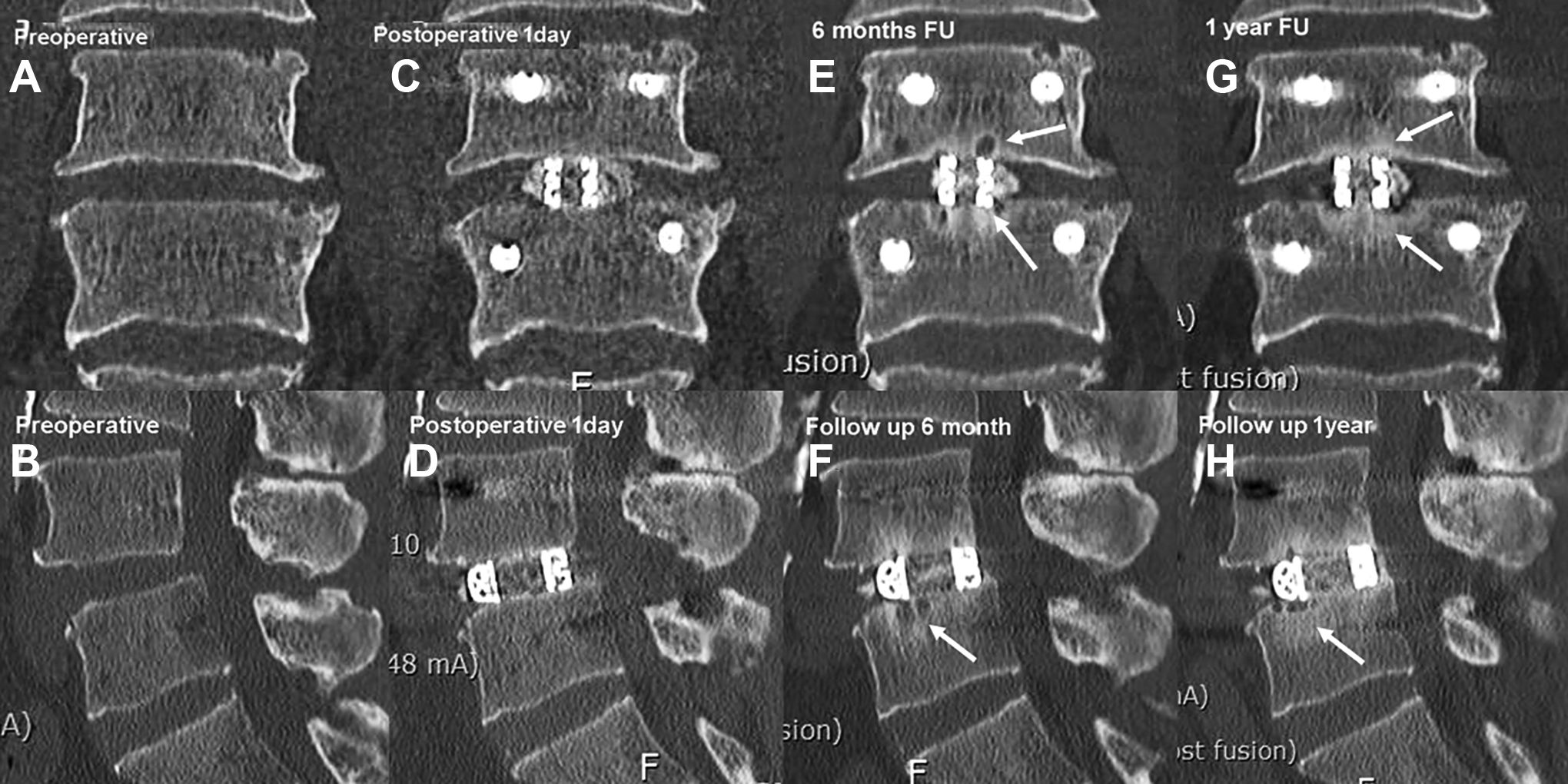
Fusion with Halo sign. Figure 6A and B: preoperative CT sagittal and coronal images with L4/5 spondylolisthesis. Figure 6C and D: postoperative day 1 CT sagittal and coronal images with interbody cage. Figure 6E and F: postoperative six months CT sagittal and coronal images with interbody cage with radiological sign of fusion and Halo sign (white arrow). Figure 6G and H: postoperative 1 year CT sagittal and coronal images with interbody cage with radiological sign of fusion and Halo sign resolving in 1 year.
In terms of radiological results, in TLIF group, the position of implants are satisfactory in all cases, with no revision required.
In follow up computer tomography scan, Bridwell Fusion grade were assessed to be 2.45(2-3) at 6 months and 1.73(1-2) at 1 year; at, Kim’s fusion stage of 2.27(2-3) at 6 months and 3.14(2-4) at 1 year and Kim’s subsidence grade of 0.82(0-3) at 6 months and 1.05(0-3) at 1 year. There were 1 CT findings of halo phenomenon in at 6months and one at 1 year.
Comparison of CT evaluation showed Endo-TLIF performed significantly better in Bridwell grade with −0.606 ± 0.118 at 6months and −0.485 ± 0.122 at 1 year; in Kim’s fusion stage with 6.97 ± 0.148 at 6months and 5.61 ± 0.204 at 1 year, P < 0.05. Endo-TLIF had significanltly less Kim’s subsidence grade of −0.696 ± 0.20 at 6months and −0.561 ± 0.204 at 1 year, P < 0.05.There is no statistical difference in terms of CT halo sign. (Table 4)
The Summary of Comparison in Radiological and Clinical Parameters Differences Between Endo-TLIF and TLIF.
Discussion
There is increasing literature on the benefits of lumbar endoscopic spine surgery in the treatment of degenerative spine conditions. Compared to conventional decompression, there were studies showing there was shorter hospital stay, blood loss, soft tissue damage and complications in endoscopic and microscopic tubular decompression than open decompression. With a trend of less complications in endoscopic surgical decompression.19,20 Endoscopic spinal surgery indications had expanded from disc discectomy to lumbar spinal decompression and fusion.1,2,21-23 There were several comparative studies between microscopic and endoscopic decompression showing promising results for spinal endoscopy.24-26 There are paucity of literature on endoscopic approach to fusion. The transkambin uniportal endoscope assisted facet sparing approach interbody fusion had produced good clinical outcomes overall but had reported high incidence of exiting nerve root complication and subsidence. The narrow safety window in Kambin’s triangle required small width foot print cage to be inserted, which might be a contributing cause of subsidence in patients with poor bone quality .7,8,27 Biportal endoscope assisted interbody fusion, which typically involved facetectomy was an alternative option to microscopic tubular transforaminal interbody fusion with promising clinical results. 28 Large size cage used in traditional and Microscopic Minimally Invasive TLIF can be used in biportal fusion surgery.10,29 Kim and Wu et al had demonstrated a technique of Endo-TLIF using large interbody cage after complete facetectomy in patients with scoliosis, spondylolisthesis and collapsed disc space with severe foraminal stenosis with good clinical result.14-16 Recent metanalysis of endoscopic fusion showed preoperative ODI and VAS scores for leg and back pain significantly improved after endoscopic TLIF with percutaneous pedicle screw fixation (P = 0.00). The ODI significantly improved by twice as much as the MCID. The mean change in the VAS for back and leg pain showed significant improvements over the MCID. The perioperative complications were usually minor. 13
There were comparison studies between biportal endoscopic fusion with open fusion procedures which showed significantly less blood loss and early postoperative pain control, there was a trend in lower complication rate but no difference in fusion rate.11,28
There is however no comparison study of our technique of Uniportal Posterolateral Facet Sacrificing Endo-TLIF with Microscopic Minimally Invasive Fusion. This comparative study evaluated Endo-TLIF and TLIF, computer tomographic fusion results and subsidence rate as well as clinical data in medium term follow up. In both cohorts, we had statistically significant improvement in clinical parameters of VAS and ODI with low complications rate in both Endo-TLIF and TLIF. Endo-TLIF showed statically significant improved final VAS compared to TLIF, there were trends of Endo-TLIF having better outcomes in ODI and VAS in 3 months and final ODI than TLIF but did not reach statistical significance.
In comparison of fusion data between Endo-TLIF and TLIF, Endo-TLIF had statistically significant better mean fusion grade in having a lower mean Bridwell grade (1.86 ± 0.35) than TLIF(2.48 ± 0.51), P < 0.05. CT Kim’s stage showed concordant statistically significant advanced stage of fusion with the mean Endo-TLIF stage (3.02 ± 0.52) than TLIF (2.20 ± 0.404), P < 0.05. The authors felt the reasons for better early fusion data are multifactorial. 1) Endoscopic preparation allow visualization of end plate under magnification. 2) Optimized size 3D printed cage can be achieved with assistance of endoscopic vision combined with fluoroscopic guidance. This provided stability of the end plate while avoiding subsidence as end plate was not violated. It also allowed osteoblastic cells and cells with fusion potential to invade the fusion bed without the need to overcome a gap in between the cage and end plate. 3) Autograft and allograft admixture aided to overcome the relative lower amount of autograft harvest from minimally invasive Endo-TLIF. We found an interesting CT Halo sign in some of 6 cases of Endo-TLIF and 2 cases of TLIF in our 6months CT scan series. We postulated that Halo sign is a sign of bone resorption due to increase vascularity adjacent to the cage prior to incorporation of the cage and bone graft for fusion. Similar hypothesis was found in Talar fracture known as Hawkin’s sign. 30 The different features between CT Halo sign and lucencies around cage secondary to loosening are: 1) bilateral bony sclerosis or bone bridge are found (Kim’s stage 3 or 4) in the end plate region directly adjacent to the cage with Halo of lucency next to the area of bone sclerosis/bone bridge at 2, 4, 8 and 10 O’clock position as compared to loosening with lucencies directly adjacent to cage at 6 and 12 O’clock position. 2) Cage position is stable without any change compared to previous image in Halo sign and cage malposition is seen in loosening. 3) Clinically good to excellent outcomes in patients with CT Halo sign as compared to symptomatic patients with loosening. All the cases with CT Halo sign was associated with good Bridwell grade and Kim’s fusion stage with good to excellent MacNab’s score. More studies on this CT Halo effect would be needed to evaluate the significance of this CT sign. (Figure 6E to H)
Subsidence of interbody cage is a major concern for all spine surgeons. 31 A key factor in preventing subsidence is the preservation of end plate without violation into the cancellous body. 32 We find a statistically significant lower mean grade of subsidence in Endo-TLIF (0.12 ± 0.38) compared to TLIF (0.70 ± 0.81), P < 0.05. One plausible reason was optimized visualization of end plate preparation and the use of blunt bent probe in the final stages of cartilage denudation, hence we avoided injury to end plate. Fluoroscopic and tactile guided curette usage in end plate preparation can lead to iatrogenic incidental end plate violation. We did not use curette in any of our cases of Endo-TLIF while we used curette in all cases of TLIF.
One of the technical difficulties in Endo-TLIF is to perform end plate preparation and cage insertion. The use of smaller endoscopic probe and drill due to limitation of the working channel in uniportal endoscope. It is technically challenging to ensure endoscopic drilling does not violate end plate and elevating the disc from end plate with bent endoscopic probe. Cage insertion is done under fluoroscopic guidance and intermittent endoscope inspection to ensure no nerve entrapment during cage insertion. Both of these technical difficulties have a steep learning curve. We felt that one should attempt endoscopic fusion after overcoming the learning curve in other lumbar endoscopic approaches.
Our primary objective of the operation was to provide stability of the spinal segment and to provide both direct decompression of central and lateral recess of neural elements. Both cohorts achieved statistically significant improved clinical outcomes within their own cohort. While there was a higher ratio of good to excellent outcomes in Endo-TLIF, it did not reach statistical significance. It is of note that we started doing endoscopic fusion after we were confident in performing endoscopic decompression technique using endoscopic drill. There was a steep learning curve with higher possible complication rate in early phase of practice. 33 Guidance from fluoroscopy and intraoperative navigation could aid to orientate the earlier cases of Endo-TLIF. 34 Fluoroscopy was used at the period of docking and during insertion of interbody cage and percutaneous pedicle screws fixation. Advantage of both TLIF and Endo-TLIF were direct decompression of the neural elements. As compared to Endoscopic Transkambin fusion through transforaminal approach which might require a separate additional decompression after completion of fusion procedure. We did over the top endoscopic decompression of the contralateral side with intact deep layer of ligamentum flavum to offer neural elements protection during bony drilling in our Endo-TLIF technique. 35 Learning curve of contralateral decompression was steep with good results significantly favored in more experienced surgeons. 36 There were favorable outcomes in various studies of endoscopic decompression compared to open and minimally invasive spinal decompression.37-41 The comparable clinical outcomes in both Endo-TLIF and TLIF were attributed to good decompression performed during the procedure.
Limitations
There are several differences and possible confounding factors with respect to non-surgical aspects in the 2 techniques: the performance of Endo TLIF was done under epidural with sedation or GA while TLIF was done under GA, the use of epidural catheter in the TLIF procedure while it was not done under Endo-TLIF procedure. These differences may have a confounding effect on the outcomes of the procedures. There is less autograft possibly harvested in Endo-TLIF compared to TLIF due to technical differences, hence we used an admixture of auto and allograft as sentinel graft along with graft stuffed in the cage in endo-TLIF, whereas only cage filled with autograft in TLIF, this is an inherent confounder in the fusion rate. The data was obtained as a retrospective comparative cohort study with patients who had undergone Endo-TLIF and TLIF. There could be inherent selection and performance bias in the study. Pre-operative data such as comorbidities, Charlson Morrison Index, comorbidities, BMI, smoking history and length of operations time were not collected which might introduce confounders in the study. We limited these confounding factors by having the same team of anesthetists and surgeons for all the operations performed in the data set. PEEK cage was used in TLIF and 3D printed titanium cage was used in Endo-TLIF which can be an important confounder. The follow up was medium term duration and we continued to follow up on these patients with a view to show the effect of a longer follow up in the future to evaluate the fusion data and subsidence rate in the long term. Kim’s fusion stages classification is a novel classification with no validation data available to test the reproducibility and inter-observer reliability. Further validation study would be required on this classification. A prospective study would be more ideal to eliminate these bias.
Conclusion
Application of Uniportal Endoscopic Posterolateral Lumbar Interbody Fusion achieved comparable clinical outcomes and better fusion with less subsidence than Microscopic Minimally Invasive Transforaminal Lumbar Interbody Fusion in mid-term evaluation in our cohorts of patients.
Footnotes
Authors’ Note
Acknowledgments
Both Dr. Hyeun Sung Kim and Dr. Pang Hung Wu contribute equally to be first co-author for the paper. We would like to acknowledge scientific team members Ms. Jae Eun Park, Ms Elin Lee and Mr. Kyeong Rae Kim for providing assistance in statistical support, acquiring full text articles and managing digital works.
Consent From Patients
All patients had given their informed consent for photographs, videos and images for publication.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Nanoori Hospital’s Ethics Committee and the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.