
Abstract
Study Design
Retrospective cohort.
Objective
To compare the characteristics of the minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) metrics when interpreting Neck Disability Index (NDI) following cervical spine surgery.
Methods
Patients who underwent primary cervical fusion, discectomy, or laminectomy were included. NDI and global rating change (GRC) data at 6 months/1 year/2 years were analyzed. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of MCID and PASS in predicting improvement on GRC were calculated for the overall cohort and separately for patients with minimal (NDI <30), moderate (NDI 30 – 49), and severe (NDI ≥ 50) preoperative disability. Two groups with patients who achieved PASS but not MCID and patients who achieved MCID but not PASS were analyzed.
Results
141 patients (206 responses) were included. PASS had significantly greater sensitivity for the overall cohort (85% vs 73% with MCID, P = .02) and patients with minimal disability (96% vs 53% with MCID, P < .001). MCID had greater sensitivity for patients with severe disability (78% vs 57% with PASS, P = .05). Sensitivity was not significantly different for PASS and MCID in patients with moderate preoperative disability (83% vs 92%, P = .1). 17% of patients achieved PASS but not MCID and 9% of patients achieved MCID but not PASS. Most of these patients still reported improvement with no significant difference between the 2 groups (89% vs 72%, P = .13).
Conclusion
PASS and MCID are better metrics for patients with minimal and severe preoperative disability, respectively. Both metrics are equally effective for patients with moderate preoperative disability.
Keywords
Introduction
For patients with cervical spine disorders, patient disability is most commonly assessed with the Neck Disability Index (NDI). 1 While patient reported outcome measures (PROMs) such as NDI provide a validated metric to evaluate a patient’s disability, understanding the patient’s level of disability requires the interpretation of numerical values in conjunction with clinical examination. 2 To that end, minimal clinically important differences (MCID) and patient acceptable symptom state (PASS) have been described for the clinical interpretation of NDI. MCID is a common metric to assess patient outcomes following spine surgery, defined as the smallest change in NDI after surgery that is clinically significant for the patient. 3 However, MCID has the drawbacks of dependence on the preoperative baseline and a lack of consistency in cut-off values reported in the literature.4,5 To overcome these limitations, the concept of PASS was introduced. It is defined as an absolute postoperative NDI score, unlike MCID which is a change score, below which patients can be expected to achieve an acceptable symptom state. 6 PASS does seem to address some of the issues with MCID, but its utility for spine surgery has only recently been described.7-11 While we have these 2 metrics for the clinical interpretation of NDI, it is not known which is the better 1 and how the preoperative symptom severity affects their utilization. It is vital to answer these questions to substantiate our understanding regarding the clinical interpretation of NDI as an outcome measure. The objective of this study was, therefore, to compare the characteristics and predictive power of MCID and PASS when interpreting NDI following cervical spine surgery. To the best of our knowledge, this is the first comparative study of the 2 metrics in assessing outcomes after cervical spine surgery.
Methods
Study Design and Patient Cohort
This retrospective cohort study was approved by the Institutional Review Board (IRB) (IRB number 2018-1142) and was exempt from the informed consent requirement. Patients who underwent primary cervical spine surgery in form of anterior cervical discectomy and fusion (ACDF), cervical disc replacement (CDR), or laminectomy for the treatment of degenerative conditions of the cervical spine between April 2017 and October 2021 and had a minimum of 6-month follow-up were included. Revision surgeries were excluded. Surgeries were performed as previously described12-18 by fellowship-trained spine surgeons at a single academic institute.
Data Collection
Following data were collected and managed using REDCap (Research Electronic Data Capture)19,20 hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384: 1. Preoperative data: age, gender, body mass index (BMI), Charlson Comorbidity Index (CCI), NDI. 2. Postoperative data: NDI and Global Rating Change (GRC) at 6 months, 1 year, and 2 years after the surgery.
Anchor Question
The anchor used to assess patient improvement 6 months/1 year/2 years after surgery was the response on the GRC scale:21,22 “Compared to preoperative, you feel (1) much better, (2) slightly better, (3) same, (4) slightly worse, or (5) much worse.” The 5-point Likert scale was collapsed to a dichotomous outcome variable for analyses and 2 patient cohorts were developed: (a) improved = response of 1 or 2, (b) not improved = response of 3 or 4 or 5, as previously described in the literature.6,9
Statistical Analysis
A difference between preoperative and 1-year NDI of
Results
Demographics, Surgical Data, Proportion of Improved Patients, and the NDI Scores.
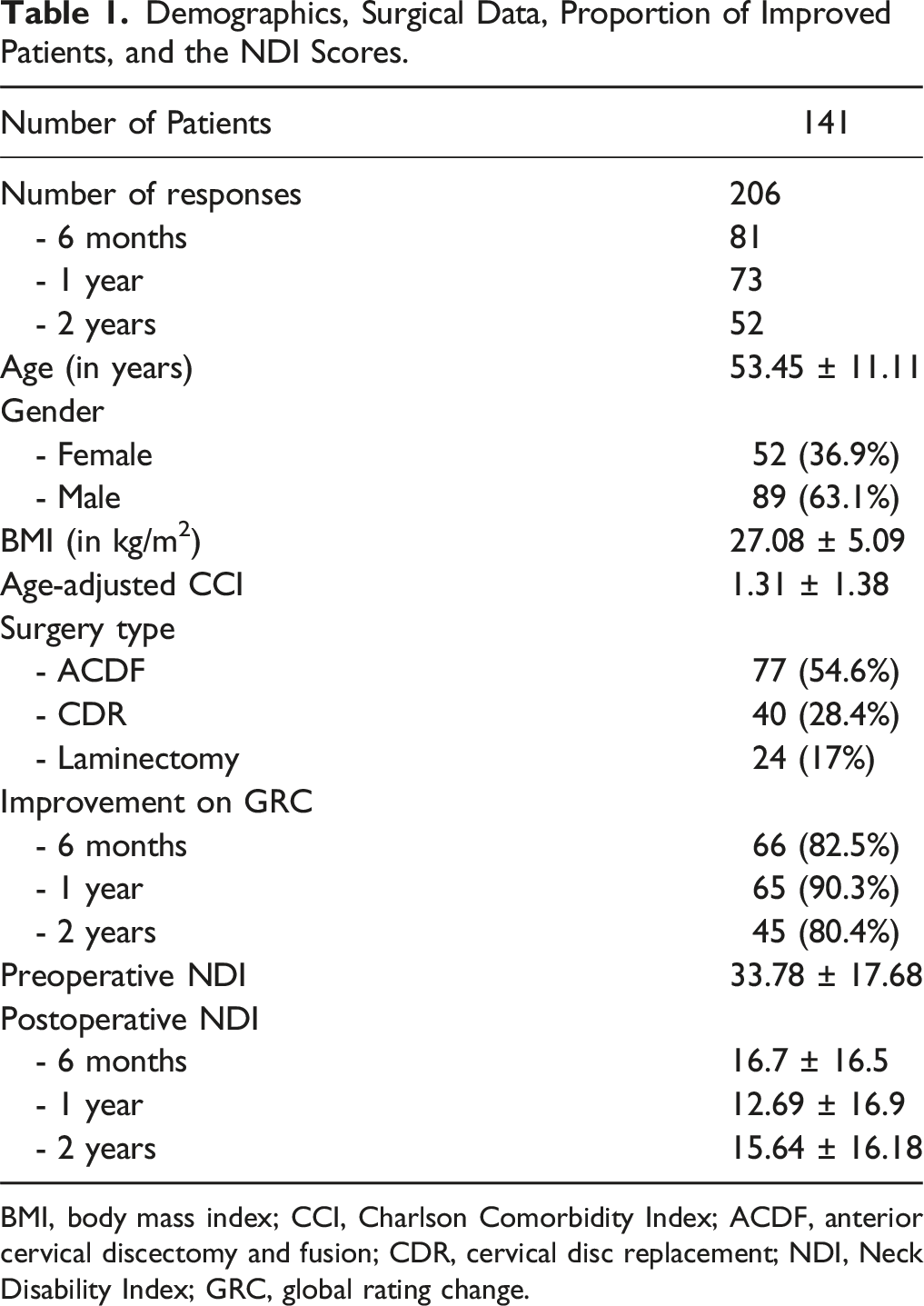
BMI, body mass index; CCI, Charlson Comorbidity Index; ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement; NDI, Neck Disability Index; GRC, global rating change.
PASS vs MCID: Overall Cohort
Comparison of PASS and MCID in the Overall Cohort.
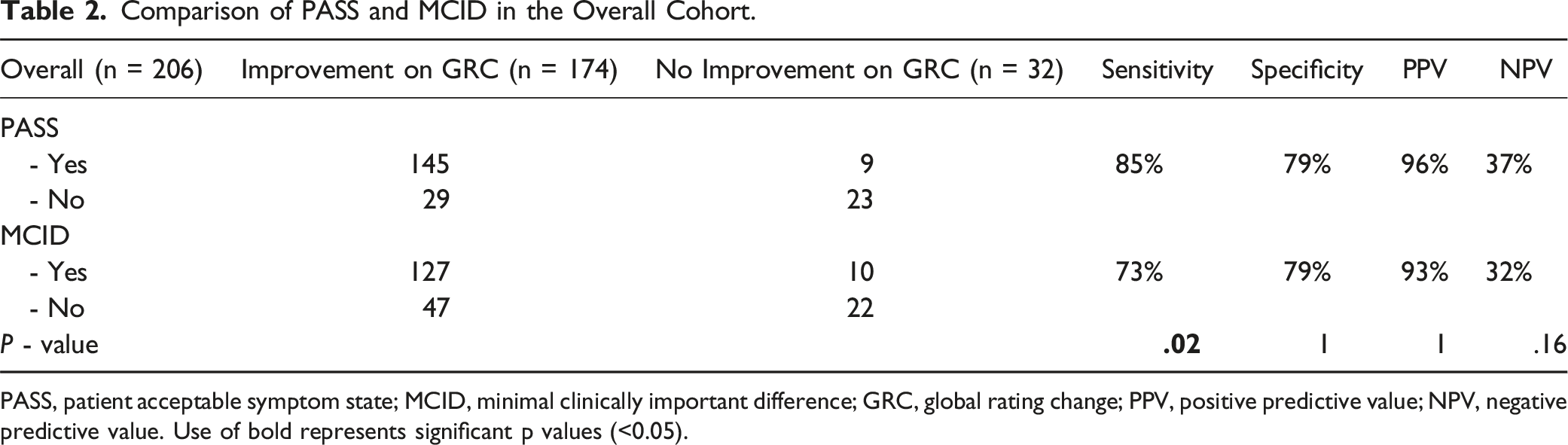
PASS, patient acceptable symptom state; MCID, minimal clinically important difference; GRC, global rating change; PPV, positive predictive value; NPV, negative predictive value. Use of bold represents significant p values (<0.05).
PASS vs MCID: Minimal Preoperative Disability
Comparison of PASS and MCID in Patients With Minimal Preoperative Disability (NDI <30).
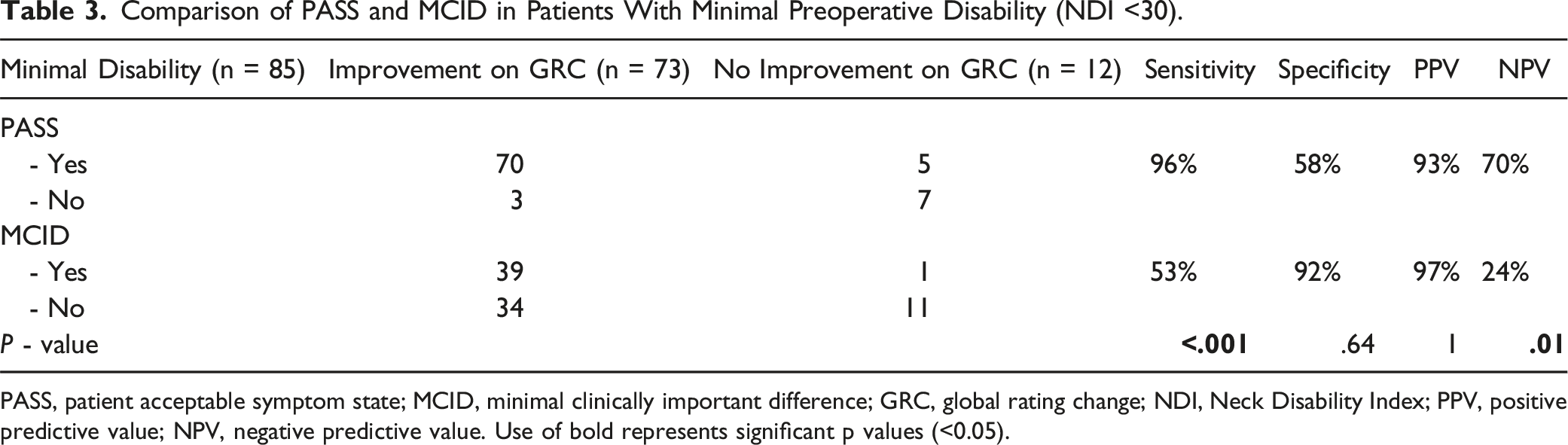
PASS, patient acceptable symptom state; MCID, minimal clinically important difference; GRC, global rating change; NDI, Neck Disability Index; PPV, positive predictive value; NPV, negative predictive value. Use of bold represents significant p values (<0.05).
PASS vs MCID: Moderate Preoperative Disability
Comparison of PASS and MCID in Patients With Moderate Preoperative Disability (NDI 30 – 49).
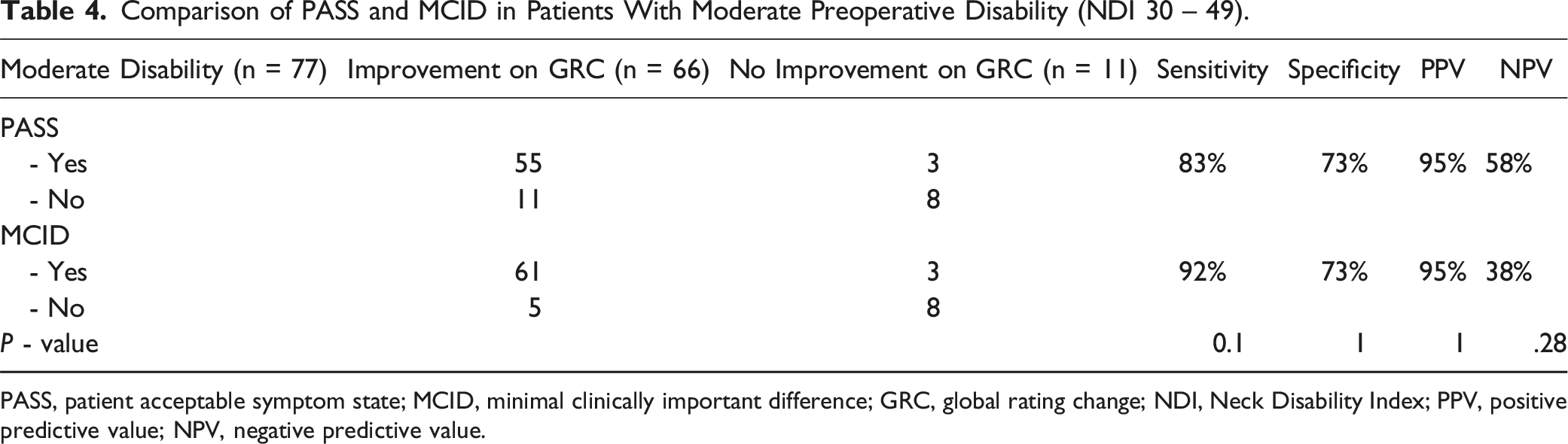
PASS, patient acceptable symptom state; MCID, minimal clinically important difference; GRC, global rating change; NDI, Neck Disability Index; PPV, positive predictive value; NPV, negative predictive value.
PASS vs MCID: Severe Preoperative Disability
Comparison of PASS and MCID in Patients With Severe Preoperative Disability (NDI ≥50).
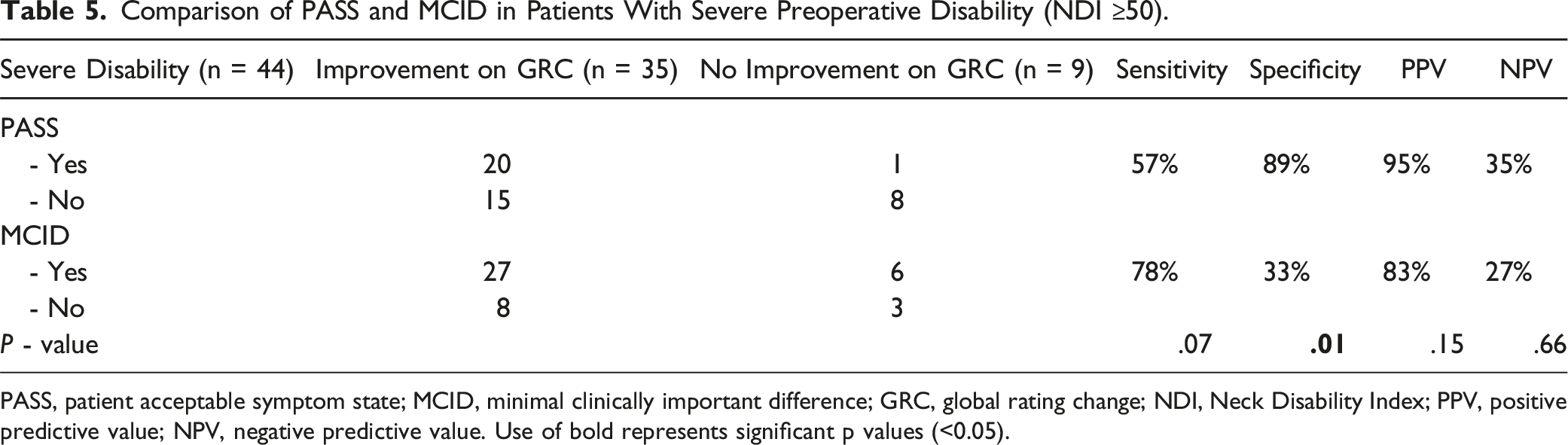
PASS, patient acceptable symptom state; MCID, minimal clinically important difference; GRC, global rating change; NDI, Neck Disability Index; PPV, positive predictive value; NPV, negative predictive value. Use of bold represents significant p values (<0.05).
Achieved PASS but Not MCID vs Achieved MCID but Not PASS
Comparison of Patients Who Achieved PASS but Not MCID and Patients Who Achieved MCID but Not PASS.
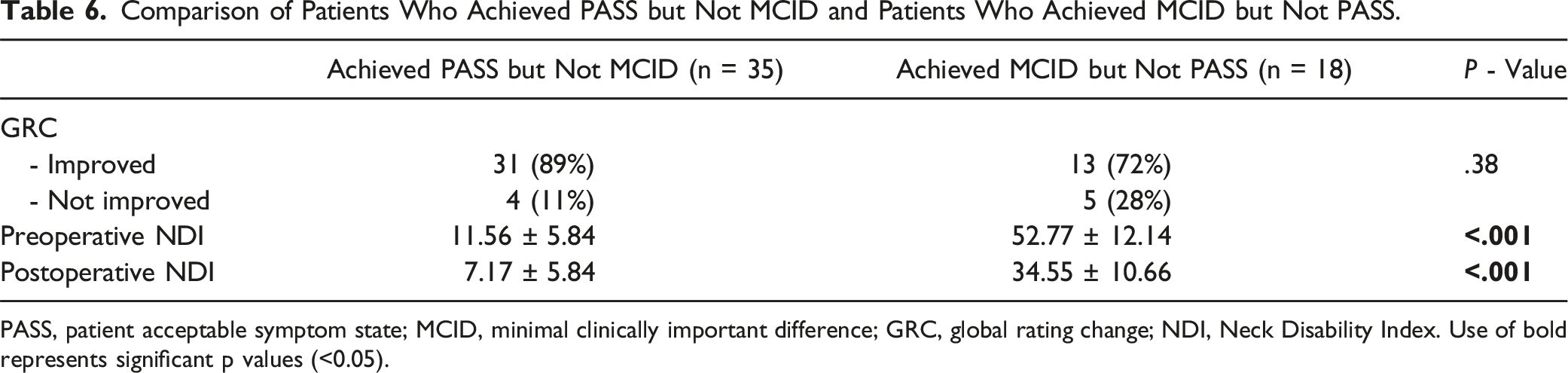
PASS, patient acceptable symptom state; MCID, minimal clinically important difference; GRC, global rating change; NDI, Neck Disability Index. Use of bold represents significant p values (<0.05).
Discussion
The current study compared MCID and PASS and reported that PASS is a better measure for patients with minimal preoperative disability (NDI <30) and MCID a better measure for patients with severe preoperative disability (NDI >50). Both were found to be equally effective for patients with moderate preoperative disability. These findings suggest that there is no superior metric between the 2 and their appropriate utilization needs to be done on an individualized basis depending the on preoperative baseline of disability.
In patients with minimal disability who reported improvement on the GRC scale (n = 73), 96% achieved the PASS threshold whereas only 53% achieved the MCID threshold. Hence, the sensitivity of the PASS metric was significantly higher compared to MCID in this patient cohort. was found to have higher sensitivity and NPV compared to MCID, hence a better metric for NDI. The rationale behind this finding is that since these patients all had a preoperative NDI <30, they were likely to reach the PASS threshold of 21 with some degree of improvement. On the other hand, since the preoperative NDI was <30 in these patients, they were less likely to achieve a drop in their NDI significantly enough to achieve MCID (cut-off 10.9) even with significant improvement after surgery. We believe that there is a need to have a lower threshold of MCID in order to gauge improvement for this subset of patients with minimal preoperative disability. Tetreault et al. described different MCID thresholds for mJOA (1 for mild, 2 for moderate, and 3 for severe patients) depending on the preoperative severity of the disease in patients with degenerative cervical myelopathy. 25 Alternatively, a percentage change in NDI rather than an absolute value can be used as the MCID threshold in patients with mild disability. It is also important to note the limitation of the PASS metric in patients with preoperative NDI ≤21. These patients are already around or below the PASS threshold at the preoperative baseline and will qualify for PASS = 1 with just maintenance of their baseline (if preoperative NDI was around 21), or even slight worsening (if preoperative NDI was <21).
In patients with moderate disability before surgery, no significant differences were observed between the MCID and PASS metrics. This was the only disability group where both the metrics had fair sensitivities (PASS 83%, MCID 92%). It is pertinent to note that the preoperative NDI score in this group (30 – 49) does not preclude or favor these patients to achieve either MCID or PASS. This group, therefore, serves as a fair comparison of the 2 metrics as surrogates of improvement after surgery as it is not skewed due to the preoperative baseline.
MCID was more sensitive than PASS in predicting improvement on the GRC when baseline NDI was ≥50. In other words, achieving MCID (a decrease in NDI of ≥10.5) rather than PASS (postoperative NDI ≤21) is sufficient for patients with severe preoperative disability to convey symptomatic improvement. Several previous studies demonstrate a similar trend and reflect the nature of MCID as a measure of change. Cha et al. concluded that while patients with severe neck disability are limited in their overall quality of life, they tend to perceive relatively limited degrees of improvement as significant changes from their preoperative baselines. 24 Jacob et al showed that patients with preoperative NDI ≥50 exhibited significantly greater MCID achievement rates at both the 6-week and 2-year timepoints. Yet, this cohort had inferior postoperative NDI scores at all timepoints compared to patients with NDI <50. 26 It is therefore evident that patients with greater preoperative disability are more likely to experience significant decrements in NDI postoperatively and achieve MCID. However, they are also more likely to exhibit worse absolute NDI values due to their suboptimal baselines, rendering them less likely to achieve PASS compared to individuals with lower preoperative disability. Thus, a change metric (MCID) rather than an absolute threshold (PASS) is preferable in evaluating symptomatic improvement among patients with greater disability.
We also assessed patients who demonstrated a mutually exclusive achievement of either PASS or MCID, both of which exhibited similar rates of improvement on the GRC scale. Patients who achieved MCID alone had a significantly higher preoperative NDI (mean 52.8) compared to those who achieved PASS alone (mean 11.6). This finding suggests that patients do not necessarily have to achieve both MCID and PASS in order to report clinical improvement. Rather, patients with severe preoperative disability can be expected to report improvement upon achievement of MCID alone and patients at the milder end of the disability spectrum can be expected to report improvement upon achievement of PASS alone. Patients with moderate disability are more difficult to distinguish in this manner since both metrics demonstrate comparable results.
PASS and MCID are intended to provide a clinically meaningful interpretation of NDI by contextualizing patient progression following surgery. The present study is the first to demonstrate that the usefulness of these measures in patients undergoing cervical spine surgery varies greatly by the degree of preoperative disability and must therefore be applied on a case-by-case basis. Yet, there are several limitations. All procedures were performed at a single institution, which reduces the external validity of the results. The retrospective nature of the study limits the level of evidence. Similar investigations entailing an assessment of outcomes from multiple centers and surgeons would be beneficial. Additionally, increased stratification would have allowed for the assessment of more precise cohorts of interest, such as patients with NDI of 30-40 and ≥70. However, our current method of stratification into groups with minimal, moderate, and severe disability was based on previously established thresholds in the literature. The GRC anchor question has likewise been criticized for being subjective and having suboptimal reliability over time due to recall bias. Our inclusion of ACDF, CDR, and laminectomy patients mars the homogeneity of the cohort but simultaneously represents a broader population of patients with degenerative cervical conditions. Another factor causing heterogeneity is that both myelopathic and non-myelopathic patients were included in the study cohort. The degree of improvement can vary significantly depending on whether the surgery was done for myelopathy or radiculopathy. In our defence, however, the previous study done by our group defining PASS following degenerative cervical spine surgery did not show any significant difference between the myelopathic and non-myelopathic groups in the proportion of patients achieving PASS and the NDI threshold required to achieve it. 6 Lastly, the extent of degeneration and specific types of diagnoses involved have not been accounted for and potentially act as confounding variables.
Conclusion
Clinical improvement among patients with severe disability (NDI ≥50) is best assessed by MCID whereas PASS appears to be the superior metric for patients with minimal disability (NDI <30). Contrastingly, both MCID and PASS are equally effective in patients presenting with moderate preoperative disability (NDI 30-49). Overall, the utility of the MCID and PASS metrics is highly reliant on preoperative disability and requires individualization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, the study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health (NIH) under award number: UL1 TR002384.