
Abstract
Study Design
Multicenter, international prospective study.
Objective
This study investigated the clinical outcome up to 2 years after multi-level spinal deformity surgery in the elderly by reporting the minimal clinically important difference (MCID) of EuroQol 5-dimensions (EQ-5D), EQ-VAS, and residential status.
Methods
As an ancillary study of 219 patients ≥60 years with spinal deformity undergoing primary instrumented fusion surgery of ≥5 levels, this study focuses on EQ-5D (3-L) as the primary outcome and EQ-VAS and residential status as secondary outcomes. Data on EQ-5D were compared between pre-operatively and postoperatively at 10 weeks, 12 months, and 24 months. An anchor-based approach was used to calculate the MCID.
Results
The EQ-5D index and EQ-VAS, respectively, improved significantly at each time point compared to pre-operatively (from .53 (SD .21) and 55.6 (SD 23.0) pre-operatively to .64 (SD .18) and 65.8 (SD 18.7) at 10 weeks, .74 (SD .18) and 72.7 (SD 18.1) at 12 months, and .73 (SD .20) and 70.4 (SD 20.4) at 24 months). 217 (99.1%) patients lived at home pre-operatively, while 186 (88.6%), 184 (98.4%), and 172 (100%) did so at 10 weeks, 12 months, and 24 months, respectively. Our calculated MCID for the EQ-5D index at 1 year was .22 (95% CI .15-.29).
Conclusions
The EQ-5D index significantly increased at each time point over 24 months after ≥5 level spinal deformity surgery in elderly patients. The MCID of the EQ-5D-3 L was .22. Patients living at home pre-operatively can expect to be able to live at home 2 years postoperatively.
Keywords
Introduction
According to the United Nations, the number of elderly persons over 60 years of age had more than doubled within the past 4 decades to 982 million in 2017. 1 Alongside, the prevalence of adult spinal deformity is increasing. The rate of scoliosis in the elderly has been reported to be as high as 68%. 2 The non-surgical and surgical treatment strategies are still debated. 3 Therefore, it is important to study the clinical outcomes after each treatment strategy.
Patient-reported outcome measures (PROMs), such as the Scoliosis Research Society- (SRS-) 22r or Oswestry Disability Index (ODI) are often disease-specific and do not allow comparison with other diseases through the calculation of a single utility value and quality-adjusted life years (QALYs). 4 Other PROMs, such as the Short Form- (SF-) 36 and -12, are disease-non-specific, but also do not allow calculation of QALYs and are time-consuming for patients to complete. 5 The EuroQol 5 dimensions’ questionnaire (EQ-5D) is a shorter questionnaire allowing calculation of a single utility score for QALYs and, to a certain extent, can actually be predicted from the SRS-22r, 6 ODI, 7 , and the SF-12. 8 It has become a commonly used, validated, standardized, generic (disease-non-specific) PROM that is even required for economic evaluation by the National Institute for Health and Care Excellence (NICE).6,9,10 It was designed in 1990 and the current version has been used for more than 10 years. It is also important to know the minimal clinically important difference (MCID) of the EQ-5D, which is the smallest relevant change for a specific disease, in order to interpret the results.11-15 Thus, the EQ-5D could potentially be a quick way to assess the health-related quality of life (HRQOL) after spinal deformity surgery and allow comparison with other disease entities.
There are very limited studies16-23 regarding the clinical outcome focusing on the EQ-5D and, to the best of our knowledge, no studies related to the MCID and residential status before and after multilevel spinal deformity surgery in the elderly. This study aimed to investigate the clinical outcome by providing an in-depth analysis of the EQ-5D and, to a lesser degree, the residential status up to 24 months after ≥5 level spinal deformity surgery in patients ≥60 years of age. A comparison of our data to the literature was undertaken regarding similar patient cohorts16-24 and common diseases (e.g., coronary artery disease 25 ). 26 The hypotheses were that the EQ-5D significantly improves after multilevel deformity surgery in the elderly with a certain MCID and that most of these patients reside at home 2 years postoperatively.
Materials and Methods
Study Design
The main methods and results of this study have been previously reported elsewhere. 27 This study focuses on the EQ-5D-3 L as the primary outcome and residential status as the secondary outcome. In brief, 12 different international centers prospectively enrolled 255 patients ≥60 years with spinal deformity undergoing primary instrumented fusion surgery of ≥5 levels after obtaining ethics approval from the Institutional Review Boards (Supplementary Table 0) and informed consent from patients. In this series, deformity was defined as any degenerative thoracic or lumbar spinal pathology that required fusion of greater than or equal to 5 levels. Surgeons were free to choose indications and surgical technique based on their current standard of practice. Exclusion criteria were previous surgery (except decompression ≤2 levels), neurodegenerative disease or paralysis, non-compliance, institutionalization or imprisonment, being medically unfit, recent substance abuse, interfering psychiatric disease, active tumor or infection, recent spinal tumor or fracture, participation in related trials.
The EQ-5D-3 L, with 3 levels of severity for each dimension, was chosen due to this being the most widely used version. 28 The 5 dimensions are mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 29 They are categorized as no problems, some problems, and extreme problems. They can be converted into a single number from worst health (33 333) to best health (11 111). This number can be transformed into a single summary index value from 0 (dead) to 1 (best health) with the aid of a value set, which depended on US population norms in our study. The EQ-VAS assesses the health state by asking patients to grade their health from 0 (worst) to 100 (best).
Ethics approval was given at each site. Informed consent was obtained from all patients. A central contracted research organization (CRO) gathered all forms and radiographs. The trial was registered at clinicaltrails.gov (NCT02035280).
Statistics
Descriptive statistics were used to represent demographic and EQ-5D data (mean and standard deviation (SD) or median and interquartile range (IQR) for continuous variables; absolute number and frequency for categorical variables) pre-operatively as well as postoperatively at 10 weeks (±6 weeks), 12 months (±2 months), and 24 months (±2 months). A sensitivity analysis on patients who have completed EQ-5D assessment at each timepoint was performed to verify the results. An unadjusted and adjusted mixed effects linear regression model with an unstructured covariance at patient level with a Wald test on change in least-square means to pre-operative value was performed. The adjusted model accounted for age, BMD, Charlson comorbidity score, depression and pre-operative cognitive impairment indication by animal fluency test. For 2 patients, who passed away within 24 months after surgery due to related adverse events, the EQ-5D index for subsequent time points was inputted as 0 (=death), but the EQ-5D items and the EQ-VAS data were not included. There were few missing data and a case approach was undertaken. The amount of missing data are provided in the tables. Furthermore, EQ-5D scores were grouped into improvement from baseline (substantial (≥20% of EQ-5D range) and marginal (≥10-<20%)), similarity to baseline (within 10%), and decrease from baseline (marginal (≥10-<20%) and substantial (≥20%)). Patients were also grouped in 5-year increments age classes (i.e., 60-64, 65-69, 70-74, and ≥75 years).
As anchors for the MCID calculation at 1 year, 2 items of SRS-22r questionnaire related to satisfaction with the results of the back management (1-very unsatisfied, 2-unsatisfied, 3-neither satisfied nor unsatisfied, 4-satisfied, 5-very satisfied) and willingness to undergo the same management again (1-definitely not, 2-probably not, 3-not sure, 4-probably yes, 5-definitely yes) were defined. The time point of 1 year was chosen for better comparisons with previous MCID calculations, as done for patients with degenerative lumbar spinal stenosis. 12 The points of both items were summarized and grouped into worsening (2-3 points), slight worsening (4-5 points), no change (6 points), slight improvement (7-8 points), and improvement (9-10 points). Afterwards, for the MCID calculation, descriptive statistics of EQ-5D index preoperatively, 1 year and the change to preoperatively were presented. . The MCID is given as the mean value of the change to pre-operative value of the slight improvement group. The significance level was defined as P ≤ .05. All analyses were performed using SAS 9.4 (SAS Institute, Cary, North Carolina, United States of America).
Results
Participants
219 patients met the inclusion and exclusion criteria. 32 patients dropped out (14 withdrew consent, 13 were lost to follow-up, and 5 died). Two deaths were related to the study intervention (cardiac arrest 1 day postoperatively and deep vein thrombosis 9 days postoperatively and subsequent cardiac arrest). The other 3 deaths were unrelated to the study intervention (death while sleeping, pancreatic cancer, carcinoma). 214 (97.7%) and 207 (94.5%) completed the EQ-5D index and EQ-5D VAS pre-operatively, 205 (93.6%) each completed it at 10 weeks, 187 (85.4%) and 183 (83.6%) completed it at 12 months, and 177 (80.8%) and 171 (78.1%) completed it at 24 months. 219 patients filled out the residential status pre-operatively, while 210 (95.9%), 187 (85.4%), and 172 (78.5%) did so after 10 weeks, 12 months, and 24 months, respectively.
The mean age of the study population was 67.5 (SD 5) years, 176 (80%) were female, and the median number of levels fused was 9 (IQR 8-14). The mean body mass index was 26.1 (SD 5), the majority of patients had American Society of Anesthesiologists (ASA) scores of II (61%) and III (34%), and the mean Charlson Comorbidity Index (CCI) was .5 (SD .8). The most common Charlson comorbidity index item was diabetes (n = 22 (10.0%), followed by chronic pulmonary disease (n = 16 (7.3%)), moderate or severe renal disease (n = 9 (4.1%)), peripheral vascuar disease (n = 7 (3.2%)), cerebrovascular disease (n = 6 (2.7%)), ulcer diseease (n = 6, (2.7%)), any tumor (n = 5 (2.3%)), connective tissue disease (n = 5 (1.8%)), myocardial infarct (n = 3 (1.4%)), mild liver disease (n = 2 (.9%)), diabetes with end organ damage (n = 1 (.5%)), dementia (n = 1 (.5%)), and moderate or severe liver disease (n = 1 (.5%)). The most common surgical approach was a posterior (n = 168 (76.7%)), followed by anterior/lateral (n = 45 (20.6%)), and combined posterior with anterior/lateral (n = 6 (2.7%)). The mean fused levels were 8.9 (SD 4.8). The mean duration of surgery was 407 minutes (interquartile range 330-476). The mean thoraco-lumbar Cobb angle was 31.9° (SD 23.6°, minimum (min) 1.7°, maximum (max) 102.5°), the sagittal vertical axis was 91.9 mm (SD 74.2 mm, min -76.3 mm, max 327.2 mm), and the pelvic incidence minus lumbar lordosis was 28° (SD 21°, min -25.9°, max 86.3°). 30
Main Outcome (EQ-5D)
The mean EQ-5D index and mean EQ-VAS increased at each time point (from .53 (SD .21) and 55.6 (SD 23.0) pre-operatively to .64 (SD .18) and 65.8 (SD 18.7) at 10 weeks, .74 (SD .18) and 72.7 (SD 18.1) at 12 months, and remained as .73 (SD .20) and 70.4 (SD 20.4) at 24 months. These changes remained similar in the sensitivity analysis (Supplementary Table 1).
EuroQol 5 Dimensions’ (EQ-5D) Over the Course of Follow-Up.
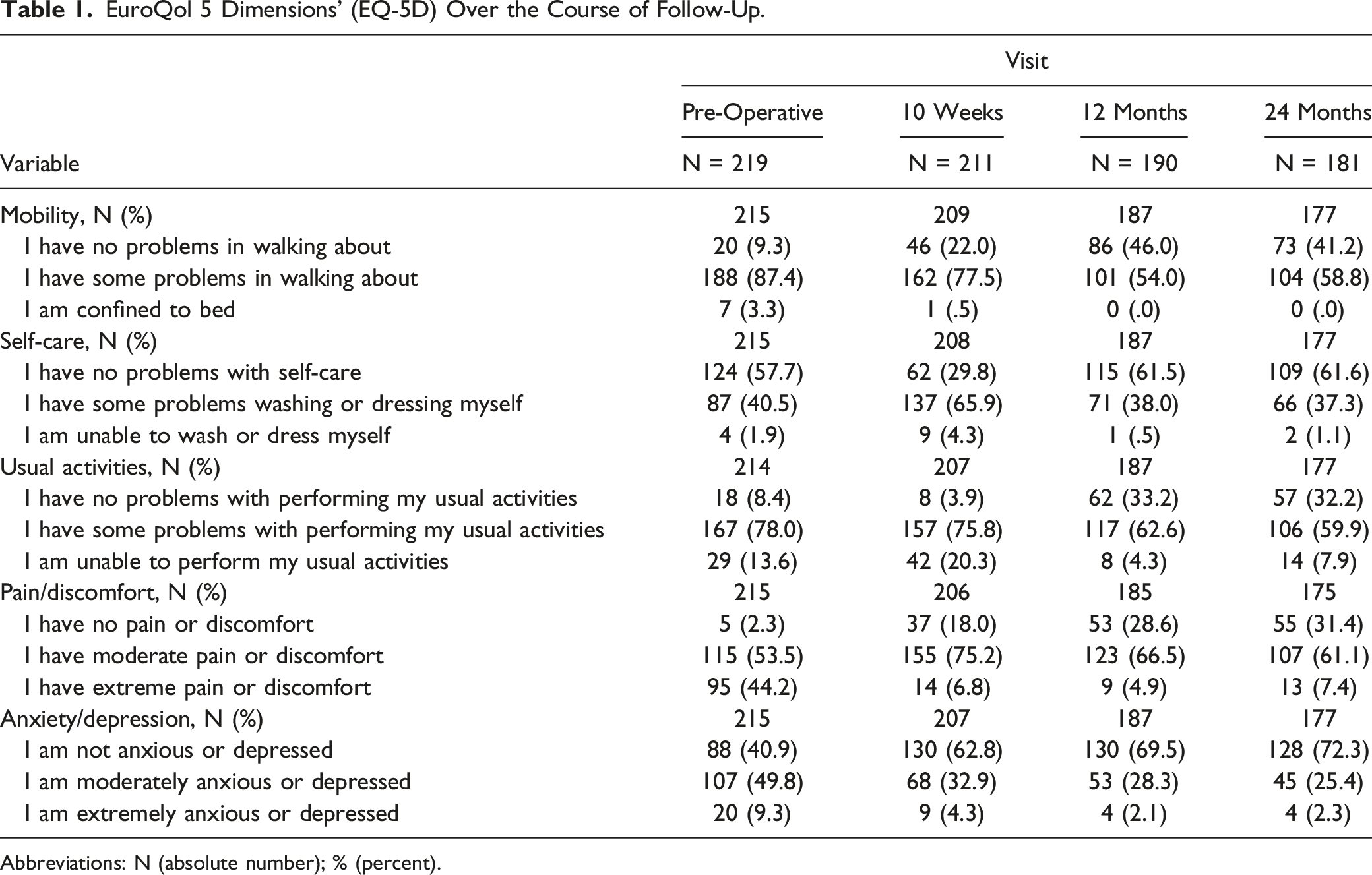
Abbreviations: N (absolute number); % (percent).
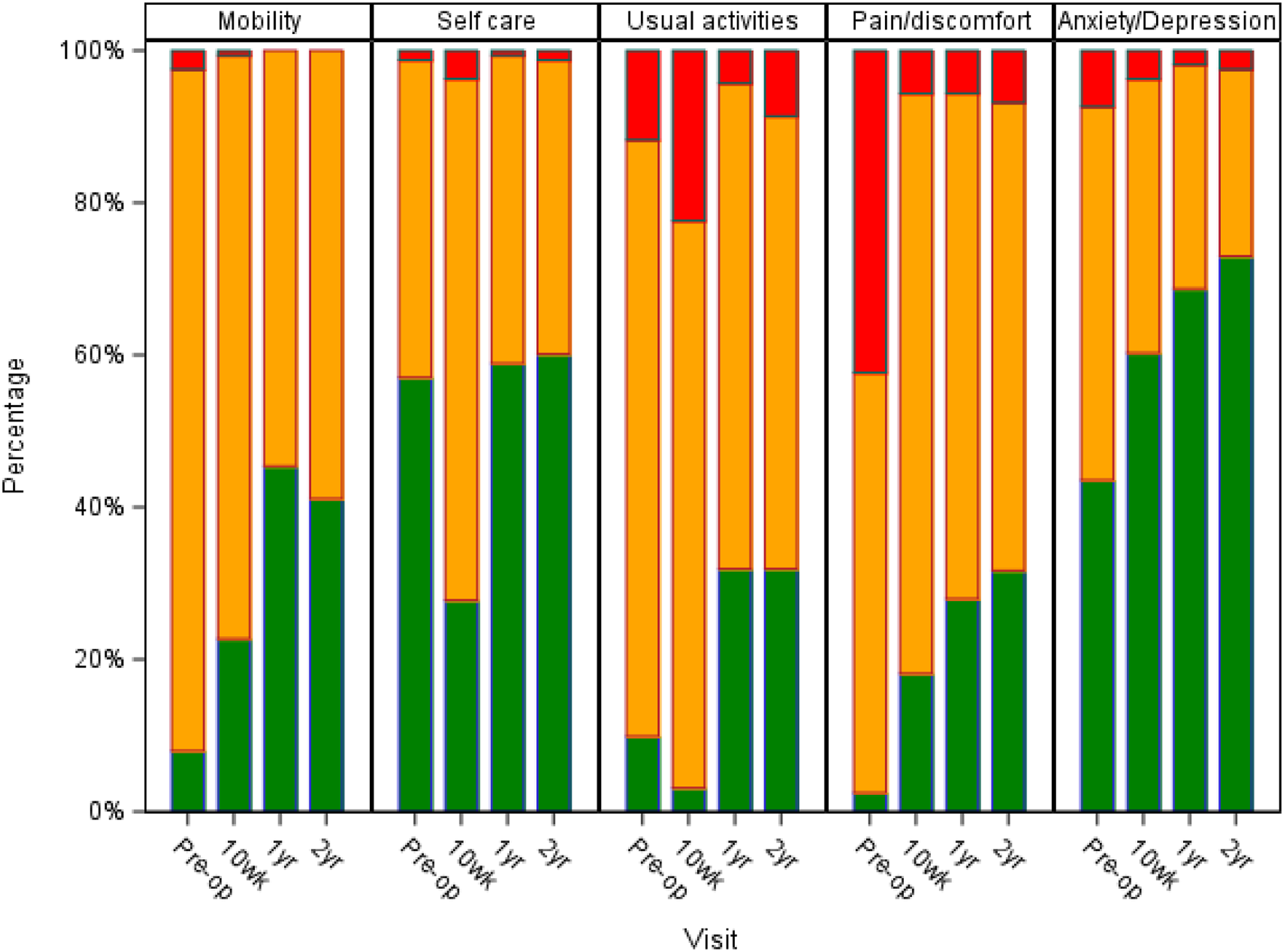
Stacked bar chart of the EuroQol 5 dimensions’ (EQ-5D) dimensions as sensitivity analysis on patients with complete data pre-operatively (pre-op) and during follow-up visits at ten weeks (wk), 1 year (yr), and 2 years (N = 163).
Changes in EuroQol Visual Analogue Scale (EQ-VAS) and 5 Dimensions’ (EQ-5D) Index Over the Course of Follow-Up; Unadjusted Mixed-Effects Modeling.
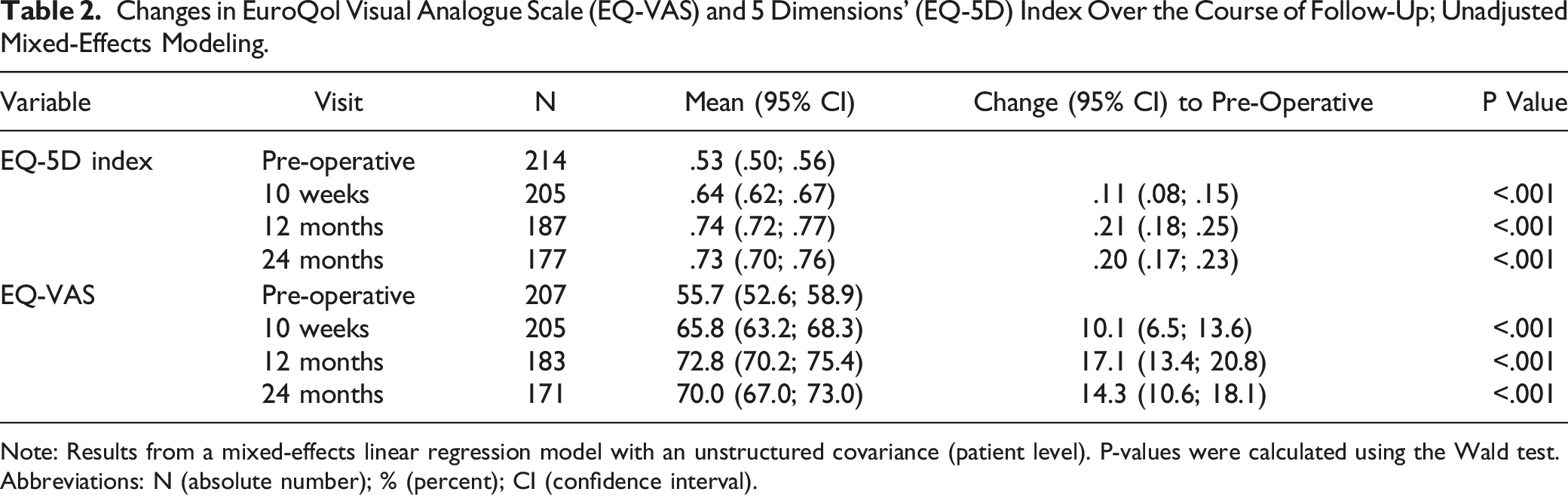
Note: Results from a mixed-effects linear regression model with an unstructured covariance (patient level). P-values were calculated using the Wald test.
Abbreviations: N (absolute number); % (percent); CI (confidence interval).
Changes in EuroQol Visual Analogue Scale (EQ-VAS) and 5 Dimensions’ (EQ-5D) Index Over the Course of Follow-Up; Adjusted Mixed-Effects Modeling.
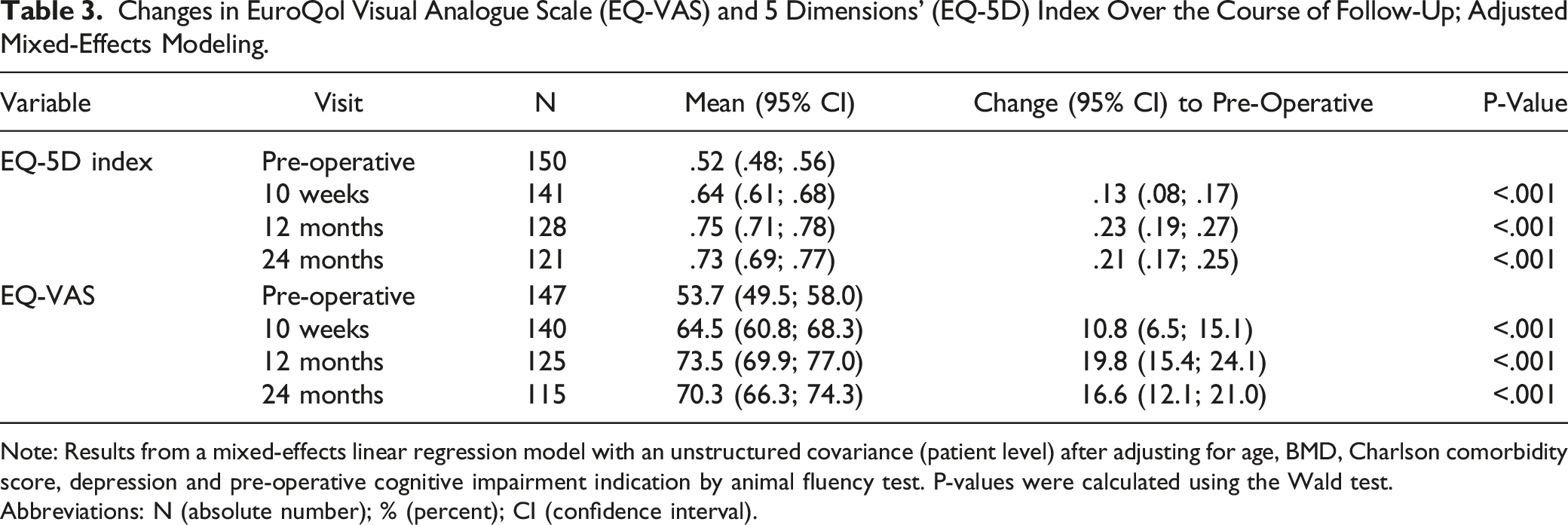
Note: Results from a mixed-effects linear regression model with an unstructured covariance (patient level) after adjusting for age, BMD, Charlson comorbidity score, depression and pre-operative cognitive impairment indication by animal fluency test. P-values were calculated using the Wald test.
Abbreviations: N (absolute number); % (percent); CI (confidence interval).
EuroQol 5 Dimensions’ (EQ-5D) Index Change to Pre-Operative Over the Course of Follow-Up.
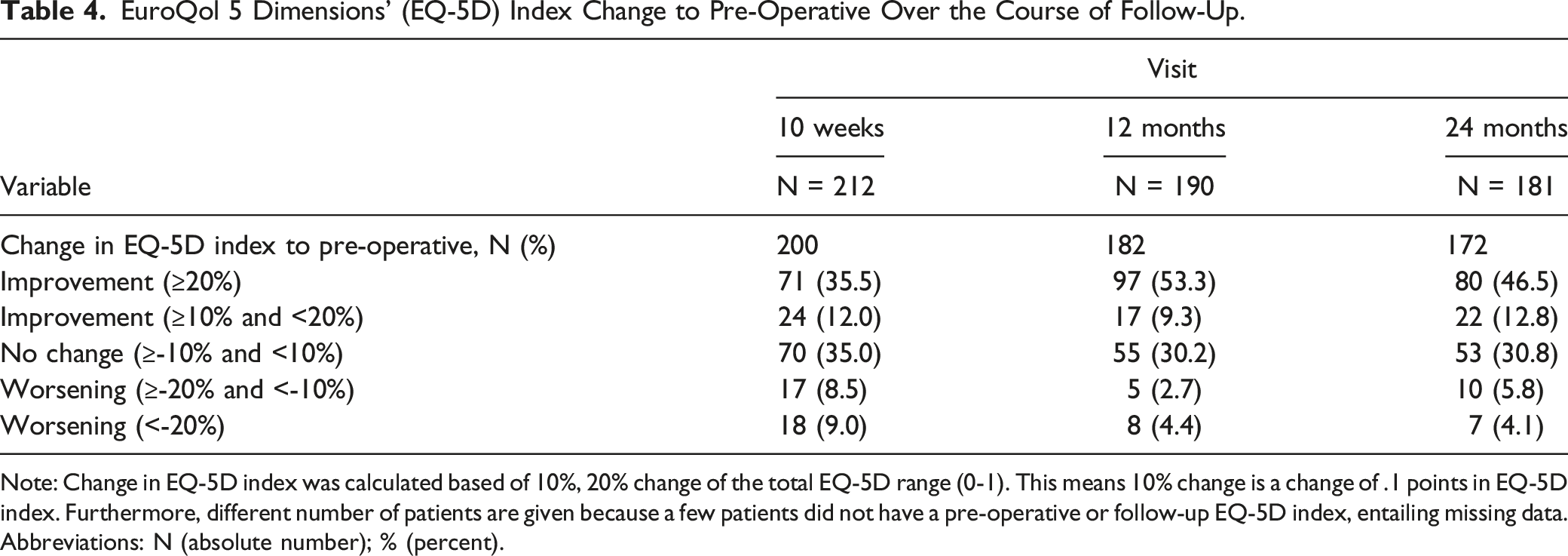
Note: Change in EQ-5D index was calculated based of 10%, 20% change of the total EQ-5D range (0-1). This means 10% change is a change of .1 points in EQ-5D index. Furthermore, different number of patients are given because a few patients did not have a pre-operative or follow-up EQ-5D index, entailing missing data.
Abbreviations: N (absolute number); % (percent).
Changes in EuroQol Visual Analogue Scale (EQ-VAS) and 5 Dimensions’ (EQ-5D) Index Over the Course of Follow-Up After Unadjusted Mixed Effects Modeling for Age Class.
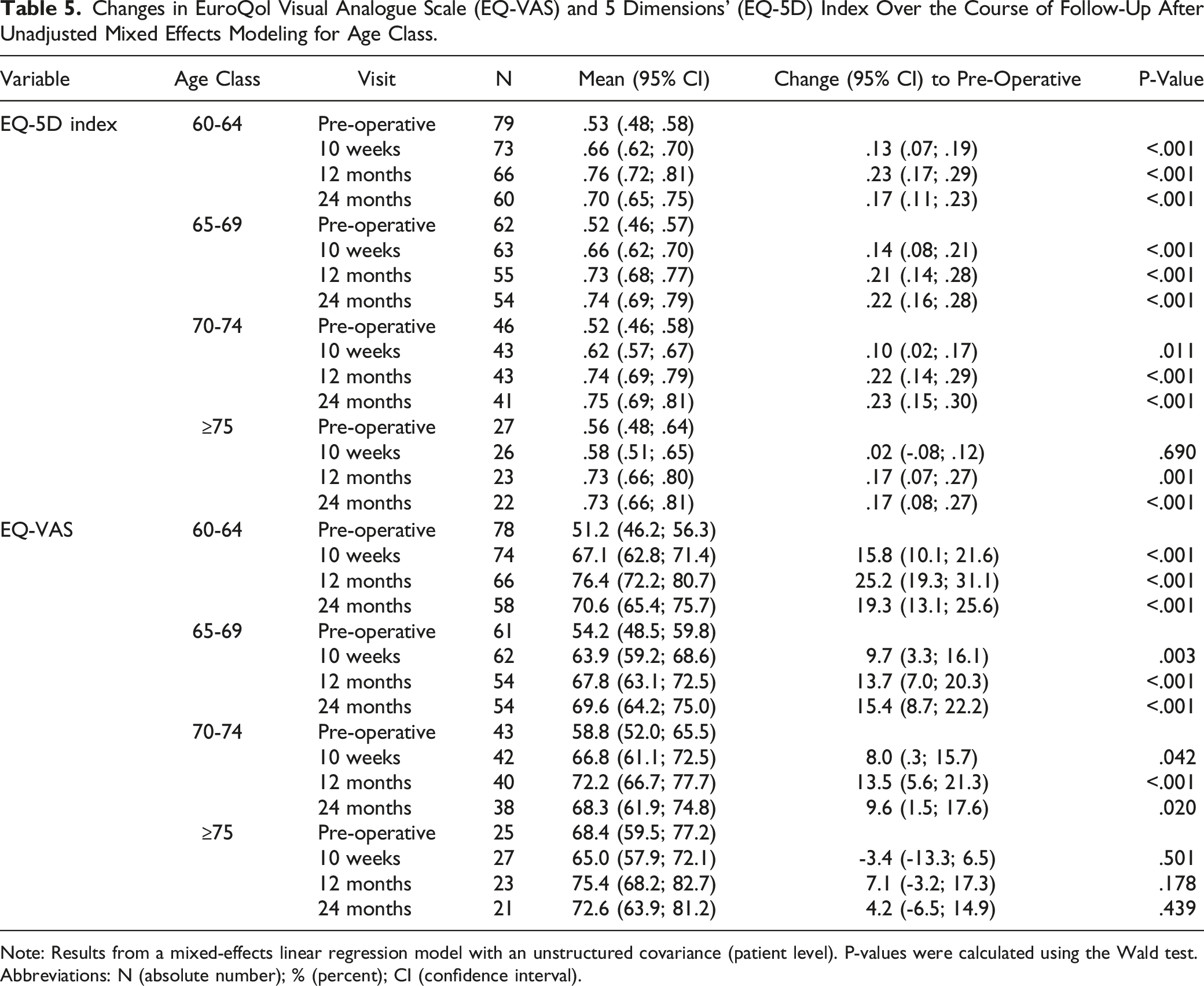
Note: Results from a mixed-effects linear regression model with an unstructured covariance (patient level). P-values were calculated using the Wald test.
Abbreviations: N (absolute number); % (percent); CI (confidence interval).
The MCID for the EQ-5D index at 1 year calculated for our patient population was .22 (95% CI .15-.29) (Supplementary Tables 3-5).
EQ-5D in Comparison to Other PROMS
Improvements were seen in all PROMS in this cohort. From pre-operative to 24 months post-operative, the overall mean EQ-5D index improved by 20% and the EQ-VAS improved by 15%. In comparison, the SRS-22r total improved by 18% (2.8 to 3.7 points), the ODI by 19% (46% to 27%), the NRS back improved by 34% (2.7 to 6.1), and the NRS leg improved by 20% (2.3 to 4.3).
Residential Status
Residential Status Over the Course of Follow-Up.
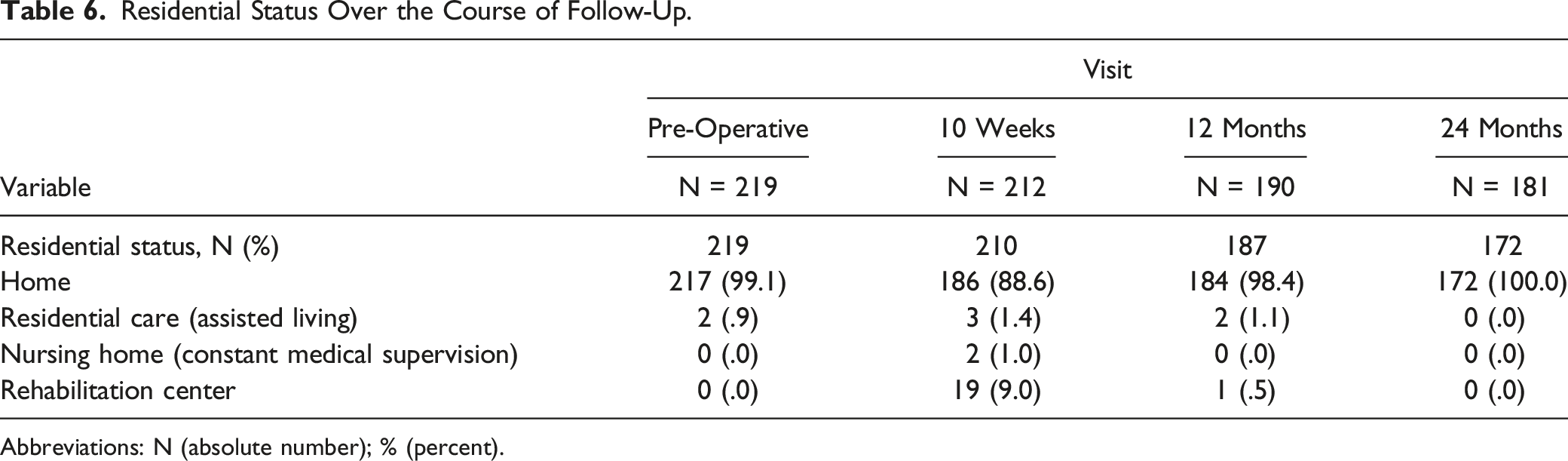
Abbreviations: N (absolute number); % (percent).
Discussion
In this multicenter, international, prospective study of patients ≥60 years with spinal deformity undergoing primary instrumented fusion surgery of ≥5 levels, the EQ-5D index significantly increased at each time point. The mean EQ-5D index and mean EQ-VAS improved from .53 and 55.6 points pre-operatively, to .74 and 72.7 at 12 months and .73 and 70.4 points at 24 months. At 24 months, the majority of patients scored their disability as mild or moderate, with very few patients grading their disabilities as severe. Most extreme problems were found in usual activities and pain/discomfort, where 8.6% of patients were unable to perform usual activities and 6.8% had extreme pain/discomfort at 24 months. Despite this, the patients in this cohort had significantly lower baseline index scores than those seen in chronic diseases that include stroke, heart failure, diabetes, and angina. Worsening of the EQ-5D at 24 months was observed in only a few patients (i.e., 9.9%, of which 4.1% was categorized as substantial worsening). The calculated MCID for the EQ-5D index was .22, which appears to be the first calculation for these patients with multilevel surgery for degenerative scoliosis. While most patients (i.e., 88.6%) lived at home after 10 weeks, most patients (98.4%) lived at home after 12 months and all surviving patients that reported for follow-up at 24 months lived at home.
The EQ-5D provides a quick disease-non-specific measuring instrument that allows calculation of QALYs and comparison to other diseases. This is a potential benefit over the SRS-22r and SF-12.4,5 A previous study by Wong et al 6 has shown that around 62% of variance of the EQ-5D can be predicted by the SRS-22r in patients with adolescent idiopathic scoliosis. In our study the EQ-5D index and EQ-VAS showed similar postoperative improvements (20% and 15%, respectively) to the SRS-22r (18%) and ODI (19%), which could indicate that it is a useful tool in assessing HRQOL of patients with adult spinal deformity. Being a much shorter and quicker questionnaire for patients to complete makes it appealing.
In order to understand the reported EQ-5D values for the reported cohort, it is important to understand the general risk of death in the elderly and to know normal values and scores for various chronic conditions. According to Statistics Canada, the mortality annual rate per 1’000 population was 7.2 for age group 60-64 years, 11.1 for age group 65-69 years, 17.2 for age group 70-74 years, 29.0 for age group 75-79 years, 50.6 for age group 80-84 years, 91.5 for age group 85-89 years, 190.4 for age group>90 years in 2018. 31 Janssen et Szende reported EQ-5D index population norms for several countries/regions and age groups. 32 Using European VAS value sets, the values ranged from .69 (Armenia, 5 regions) to .95 (China) for the total of all age groups, .52 (Armenia, 5 regions) to .93 (Canada, Alberta) for the 65-74 age group and .47 (Armenia) to .87 (Canada) for the ≥75 age group. Using country-specific TTO (time trade-off) value sets, the values ranged from .83 (Zimbabwe, Harare district) to .96 (Korea) for the total of all age groups, .66 (Zimbabwe) to .90 (Italy) for the 65-74 age group and .59 (Spain, Catalunya) to .84 (Germany and Italy) for the ≥75 age group. Mean EQ-VAS scores ranged from 70 (Hungary) to 83 (Denmark). Furthermore, a population-based study by Diarbakerli et al 33 reported normative data for individuals ≥60 years. The EQ-5D 3-L index ranged around .87 in the United Kingdom and .93 in Sweden.
It appears that the current study is 1 of the first calculations of the MCID regarding the EQ-5D for patients with multilevel surgery for degenerative scoliosis. Since the EQ-5D is a quick assessment tool that allows the comparison with other diseases, it is important to know the MCID for the EQ-5D in addition to the previously known MCID for the SRS-22r34,35 in adult spinal deformity. Although Ibrahim stated that 41% of 101 patients >70 years with ≥5 level fusion surgery reached the EQ-5D MCID of .15 at 2 years, the MCID value was based on lumbar revision surgery for pseudarthrosis. 14 Despite the fact that a study by Passias et al 36 reported that 19% of 63 patients after cervical deformity correction reached the EQ-5D MCID of .1 at 1 year, they based their MCID value on patients with post-traumatic stress disorder. 37 There is previous literature on the MCID on degenerative lumbar spinal stenosis with a value of .19 (range, .30-.52) as described by Burgstaller et al. 12 The MCID for other spine-related diseases ranged around .14-.24 for symptomatic pseudarthrosis, 14 .27-.54 for adjacent-segment disease, 13 and .17 for chronic low back pain. 15 The presented MCID for the EQ-5D index at 1 year was .22 in patients >60 years undergoing ≥5 level spinal deformity fusion surgery.
The mean EQ-5D has also been reported for other common diseases and varies across different regions.26,38,39 For example, a study by Sullivan et Ghushchyan reported several EQ-5D index mean and median scores for chronic diseases in the United States. For example, diabetes mellitus (.751) had higher EQ-5D index scores than depression (.732), renal failure (.651), and heart failure (.636) in middle aged and elderly populations (Table 5). 38 The EQ-5D of .74 at the final follow-up in our study is in line with these results and slightly better than other musculoskeletal diseases in the UK and Japan (Supplementary Table 6).
EuroQol 5 Dimensions’ (EQ-5D) Index and EQ-VAS in the Literature.
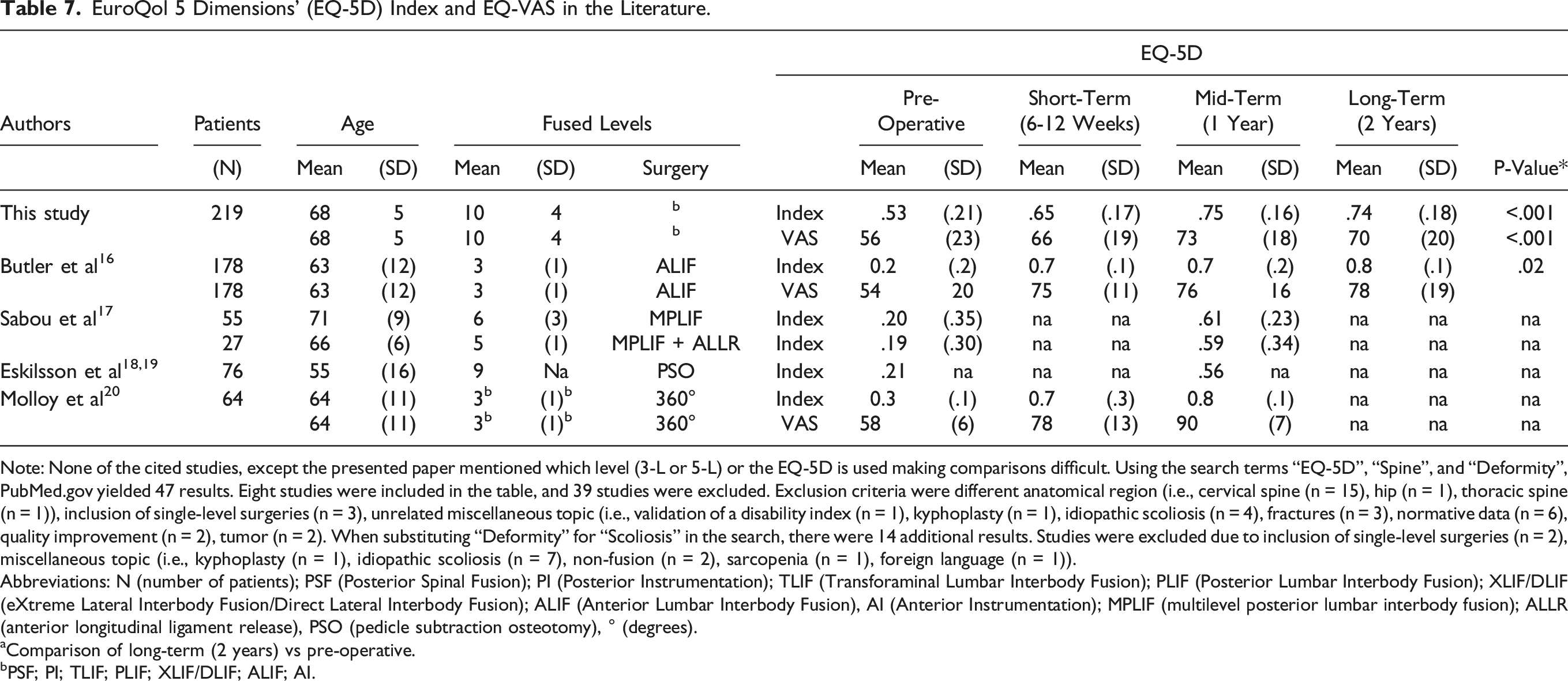
Note: None of the cited studies, except the presented paper mentioned which level (3-L or 5-L) or the EQ-5D is used making comparisons difficult. Using the search terms “EQ-5D”, “Spine”, and “Deformity”, PubMed.gov yielded 47 results. Eight studies were included in the table, and 39 studies were excluded. Exclusion criteria were different anatomical region (i.e., cervical spine (n = 15), hip (n = 1), thoracic spine (n = 1)), inclusion of single-level surgeries (n = 3), unrelated miscellaneous topic (i.e., validation of a disability index (n = 1), kyphoplasty (n = 1), idiopathic scoliosis (n = 4), fractures (n = 3), normative data (n = 6), quality improvement (n = 2), tumor (n = 2). When substituting “Deformity” for “Scoliosis” in the search, there were 14 additional results. Studies were excluded due to inclusion of single-level surgeries (n = 2), miscellaneous topic (i.e., kyphoplasty (n = 1), idiopathic scoliosis (n = 7), non-fusion (n = 2), sarcopenia (n = 1), foreign language (n = 1)).
Abbreviations: N (number of patients); PSF (Posterior Spinal Fusion); PI (Posterior Instrumentation); TLIF (Transforaminal Lumbar Interbody Fusion); PLIF (Posterior Lumbar Interbody Fusion); XLIF/DLIF (eXtreme Lateral Interbody Fusion/Direct Lateral Interbody Fusion); ALIF (Anterior Lumbar Interbody Fusion), AI (Anterior Instrumentation); MPLIF (multilevel posterior lumbar interbody fusion); ALLR (anterior longitudinal ligament release), PSO (pedicle subtraction osteotomy), ° (degrees).
aComparison of long-term (2 years) vs pre-operative.
bPSF; PI; TLIF; PLIF; XLIF/DLIF; ALIF; AI.
In addition to the previous studies, the following studies also reported on similar topics. Cheng et Gerdhem 23 retrospectively analyzed 209 patients with a mean age of 66 years with lumbar fusion surgery to compare single-level (n = 45) vs ≥2-level (n = 164) fusions. They reported that the EQ-5D improved significantly in both groups at 2 years. They did not provide absolute values, but according to a box plot figure, the median EQ-5D index was approximately .15 pre-operatively and .65 for the multi-level group at 2 years. Li et al 24 retrospectively followed up on 83 patients with a mean age of 75 (range 65-88) years with a mean of 7 (±2) level fusion surgeries at a mean follow-up of approximately 2.5 years. No pre-operative EQ-5D values were provided. The EQ-5D was significantly better in the operative group (.79 (±.16)) than the conservative group (.67 (±.19)). The EQ-VAS showed a trend toward being better in the operative group (79 (±18)) than the conservative group (68 (±20)). In addition to these studies, Ibrahim et al 21 retrospectively studied 101 patients >70 years with ≥5 level fusion surgeries. They reported an improvement in HRQOL of at least 1 MCID (using .15) in the EQ-5D in 41%. Furthermore, Sharma et al 22 retrospectively analyzed 191 patients with a mean age of 64 (±11) years with ≥2 level (mean of 8 (±4)) fusion surgeries. They reported an improvement in HRQOL of at least 1 MCID (using .15) in the EQ-5D in 47%.
No study, to the best of our knowledge, has reported the residential status after multilevel spinal surgery in the elderly. However, Eastlack et al 40 undertook a retrospective review of patients treated with minimally invasive surgery for adult spinal deformity. Of 182 patients, 62% were discharged home and 37.9% were discharged to a nursing home or rehabilitation. They also found that elderly patients >70 years were 6 times more likely to be discharged to a nursing home or rehabilitation. Patients that were discharged home were less likely to have complications (40 vs 58%). Additionally, Bozic et al 41 have shown that discharge to post-acute care (e.g., rehabilitation) may account for up to 55% of the total costs. In an endeaver to decrease costs, Jubelt et al 42 have shown that >10% of patients may be discharged home without increasing readmission rates. In our series, 88.6% patients resided at home after 10 weeks and that all surviving patients were able to live at home after 24 months. Pre-operatively almost all of the patients lived at home, which is substantial in this age group. Furthermore, a high portion were still recovering in rehab at 10 weeks, which suggests that the recovery from this surgery is very long, and these patients had access to substantial resources that are not available everywhere. However, at 1 and 2 years virtually all of the patients successfully made it home.
The main limitations of this study are the lack of standardized definition of spinal deformity, surgical indication and surgical techniques. However, due to the sparse literature on this topic, the current study adds helpful insights into the EQ-5D in elderly patients with multilevel surgery for spinal deformity. Another limitation is the use of the EQ-5D-3 L instead of the 5-level (5-L) version. Compared to the 5-L version, the 3-L version depicts population health as having fewer, but more severe health problems. 43 The 5-L has been shown to have increased sensitivity and precision due to superior because of distributional evenness, scale use efficiency, and face validity. 44 The anchor-based approach for MCID calculation is the most commonly used approach. It depends on the criterion scale and its levels, which makes it dependent on the number of levels with smaller differences leading to smaller MCIDs. 45 It also carries the risk of cognitive dissonance regarding decision regret. Other approaches may yield somewhat different values, but, for example, the distribution-based appraoch does not consider the actual clinical importance and depends of the variability of the investigated sample. 46 Satisfaction is a different measure as to whether a patient has improved or not. A static MCID does not take into account the baseline health-related quality of life, which affects the quantity of possible change and relevance of smallest change, which is why it needs to be interpreted with care. The external validity of this study may be limited by differences in indications and surgical treatments between other surgeons and other populations. Future studies may investigate QALYs and the cost-effectiveness as well as calculations of the substantial clinical benefit of multilevel adult spinal deformity surgery in the elderly. Lastly, the EQ-5D is a generic measure and not specific for spine pathology, which makes it prone to be influenced by other general co-morbidities. We provided baseline data for comorbidities in order to put the baseline EQ-5D values into perspective. Future studies may also record changes in these comorbidities over time. Radiological data, such as overall spinal alignment and junctional failure may also have an impact on the EQ-5D, but radiological outcomes of this study population were not the focus of this study.
Of note, we did not calculate the MCID for the EQ-VAS because the prerequisite for MCID calculation, not significant baseline values, was not met (P = .05). This means the MCID for EQ-5D VAS (MCID = 13.9 (95% CI 6.9 – 20.9)) is questionable.
Conclusion
This study provides in-depth analysis up to 24 months after ≥5 level spinal deformity surgery in elderly patients, providing a value of .22 for the MCID calculation of the EQ-5D, and a comparison to the previous sparse literature regarding similar patient cohorts. This value could be considered an indicator for sucessful deformity surgery in the elderly. Overall, the EQ-5D is an efficient questionnaire to assess patients with adult spinal deformity. The EQ-5D index significantly increased at each time point over 24 months. Only few patients had extreme problems and substantial worsening of the EQ-5D was observed in only 4.1% of patients. Patients living at home prior to surgery can expect to be able to live at home 2 years following multilevel spinal fusion for spinal deformity. In this series, the EQ-5D showed similar results to the SRS 22r, the ODI, and the NRS while allowing for QALY calculations and comparisons to other disease conditions.
Supplemental Material
Supplemental Material - The Influence of Multilevel Spinal Deformity Surgery on the EuroQol 5 Dimensions’ (EQ-5D) Questionnaire and Residential Status in the Elderly: A Prospective, Observational, Multicenter Study
Supplemental Material for The Influence of Multilevel Spinal Deformity Surgery on the EuroQol 5 Dimensions’ (EQ-5D) Questionnaire and Residential Status in the Elderly: A Prospective, Observational, Multicenter Study by Thorsten Jentzsch, Stephen J. Lewis, Colby Oitment, Anna Rienmüller, Allan R. Martin, Christopher J. Nielsen, Hananel Shear-Yashuv, Marinus de Kleuver, Yong Qiu, Yukihiro Matsuyama, Lawrence G. Lenke, Ahmet alanay, Ferran Pellisé-Urquiza, Kenneth M. C. Cheung, Maarten Spruit, David W. Polly, Jonathan N. Sembrano, Christopher I. Shaffrey, Justin S. Smith, Michael P. Kelly, Benny Dahl, Sigurd H. Berven, and AO Spine Knowledge Forum D in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international spine deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department and the AO Innovation Translation Center, Clinical Evidence.
Ethical Approval
Comité Ético de Investigación Clínica del Hospital Universitari Vall d’Hebron; 38121226Z, University of Virginia Institutional Review Board for Health Sciences Research; 17323, The Committees on Health Research Ethics Benny Dahl is supported by a grant for The Alfred Benzon Foundation for the Capital Region of Denmark; H-2-2014-FSP18, Ethics Committee of Hamamatsu University School of Medicine; 25-253, 17-049, Ethics Committee of Hamamatsu University School of Medicine; 17-049, Institutional Review Board of The Hong Kong/Hospital Authority Hong Kong West Cluster; UW 14-109, Acıbadem Maslak Hospital, Turkey; 2013-567, 2016-16/18, 2017-6/20, Institutional Review Board, University of Minnesota; 1312M46667, Nanjing University Ethics Committee; 2013-079, Medical Ethics Committee, Slotervaartziekenhuis, The Netherlands; U/14.066/P1425, University Health Network Research Ethic Board, Toronto; 13-6942, Human Research Protection Program, Committee on Human Research, University of California, San Francisco; 13-12727, and The Washington University in St. Louis Institutional Review Board; 201312094.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.