
Abstract
Study design
Prospective cohort study.
Objectives
The purpose of this study was to identify preoperative factors associated with clinically meaningful improvement, patient satisfaction and expectation fulfilment at 2 years follow-up in patients undergoing single-level TLIF for degenerative spondylolisthesis.
Methods
Patients who underwent a primary, single-level TLIF for degenerative spondylolisthesis between 2006 and 2015 were identified from a prospectively maintained institutional spine registry. Baseline characteristics and PROMs including the Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS), Visual Analogue Scale (VAS) back pain, and VAS leg pain were collected preoperatively, at 1 month, 3 months, 6 months, and 2 years.
Results
A total of 997 patients were included. Multivariate analyses showed that increasing age (OR 1.039, P < .001) and better preoperative ODI (OR .984, P = .018) were associated with achieving minimal clinically important difference (MCID) for VAS Back. Increasing age (OR 1.032, P = .007) and better preoperative VAS Back (OR .783, P < .001) were associated with achieving MCID for VAS Leg. Lower BMI (OR .952, P = .024) and better preoperative ODI (OR .976, P < .001) were associated with achieving MCID for SF-36 PCS. Importantly, a better preoperative SF-36 MCS was associated with MCID attainment for ODI (OR 1.038, P < .001), satisfaction (OR 1.034, P < .001) and expectation fulfilment (OR 1.024, P < .001).
Conclusion
Patients who were older, have less preoperative disability and better preoperative mental health were significantly more likely to attain clinically meaningful improvement in PROMs and postoperative satisfaction after single-level TLIF. Identification of these factors would aid surgeons in patient selection and surgical counselling for single-level TLIF.
Introduction
Transforaminal lumbar interbody fusion (TLIF) is a successful surgical procedure to treat degenerative spondylolisthesis and spinal stenosis.1,2 As healthcare systems transition towards value-based care, patient-reported outcome measures (PROMs) have become the gold-standard for determining the effectiveness of any surgical intervention,3,4 and PROMs such as the Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS) and Visual Analogue Scale (VAS) have been increasingly used to assess clinical efficacy in spine surgery. 5 A commonly used threshold to determine meaningful improvement in PROMs is the minimal clinically important difference (MCID), 6 which is defined as the smallest difference that patients perceive as beneficial or harmful and would justify a change in management. 7 The MCID is an important concept used to determine the clinical relevance of a change in outcome score and is believed to be a more rigorous measure of functional improvement for a given intervention. 8
Importantly, a subgroup of patients do not experience a clinically significant improvement in PROMs or attain MCID after lumbar spine surgery. 6 Similarly, some patients do not report satisfaction after surgery, which is an important measure of patients’ perception of the outcome of the surgery 4 and has been shown to influence long-term outcomes, patient compliance and incidence of malpractice suits.9,10 Although minimally invasive (MIS) TLIF has been associated with lower blood loss, length of hospitalization and tissue injury than open TLIF, previous studies have shown that both groups of patients achieve comparable clinical and functional outcomes in the long-term11,12 Several preoperative factors may contribute to poor postoperative outcomes after spine surgery, including smoking, poor preoperative neurological status, and a longer duration of symptoms.13-15 Several perioperative factors such as longer operative duration, longer hospitalization duration, surgical complications and need for revision surgery have also been shown to affect postoperative TLIF outcomes.16,17 However, there remains a paucity of literature regarding the factors affecting PROMs and attainment of MCID following lumbar fusion, despite the growing recognition of their importance. 5 Such information would help surgeons to identify optimal surgical candidates, so as to improve outcomes and contain costs. 18
The purpose of this study was to identify preoperative factors associated with clinically meaningful improvement, patient satisfaction and expectation fulfilment at 2 years follow-up in patients undergoing single-level TLIF for degenerative spondylolisthesis.
Methods
Study Design
This study was approved by a centralized institutional review board (2020/2311) and all patients provided informed consent to participate in this study. We retrospectively identified 1223 patients who underwent a primary, single-level TLIF for degenerative spondylolisthesis between 2006 and 2015, of which 997 patients (82%) had minimum 2-year follow-up and were available for analysis. All patients had grade 1 or 2 degenerative spondylolisthesis. Exclusion criteria were patients who had surgeries at more than one spinal level, and spinal procedures for trauma, tumor, infection or revision surgery. All surgeries were performed by one of 5 fellowship-trained spine surgeons. Degenerative spondylolisthesis was evaluated using dynamic flexion and extension lumbar spine radiographs as well as magnetic resonance imaging.
All the patients included in the study underwent open or minimally invasive (MIS) TLIF after failure of conservative management. Instrumentations used were posterior pedicle screws, rods and interbody fusion cages with autologous bone graft. Patients were placed on a standardized postoperative clinical pathway for lumbar spine surgery and underwent supervised physical therapy postoperatively.
Patient-Reported Outcomes
Baseline characteristics including age, gender, BMI, diabetes status, comorbidity burden and surgical approach (open vs MIS) were recorded. PROMs such as the Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS), Visual Analogue Scale (VAS) back pain, and VAS leg pain were prospectively collected at baseline, 1 month, 3 months, 6 months and 2 years for all patients. The proportion of patients who attained MCID at 2 years was also determined. Published values of 12.8 for ODI, 1.2 for VAS back pain, 1.6 for VAS leg pain, and 4.9 for SF-36 PCS 19 were used as the threshold for MCID for the respective PROMs. Expectation fulfilment and satisfaction scores were recorded using 7-level and 6-level Likert scales respectively, adapted from the NASS Lower Back Pain instrument, respectively, with a higher score indicating a poorer result. The scores were then categorized into satisfied (score 1-3) or unsatisfied (score 4-6), and expectations fulfilled (score 1-3) or unfulfilled (score 4-7). 20
Statistical Analysis
Continuous variables were expressed in terms of mean and standard deviation, while categorical variables were expressed in terms of count and percentage. Repeated measures analysis of variance was used to compare the change in PROMs from pre- to postoperatively. Multivariate logistic regression was used to identify preoperative characteristics associated with achieving MCID for each PROM, patient satisfaction, and expectation fulfilment while adjusting for confounders. The variables included in the models were age, sex, BMI, comorbidity burden, diabetic status, surgical approach (open vs MIS), preoperative ODI, VAS back pain, VAS leg pain, SF-36 PCS and SF-36 MCS. A bidirectional stepwise variable-selection model builder based on the optimal Akaike Information Criterion (AIC) was used to build the ideal multivariable logistic regression model. 21 Statistical analyses were performed using the SPSS software package, version 20.0 (SPSS Inc, Chicago, IL). We defined statistical significance at the 5% level (P < .05).
Results
Baseline Characteristics by Surgical Procedure.
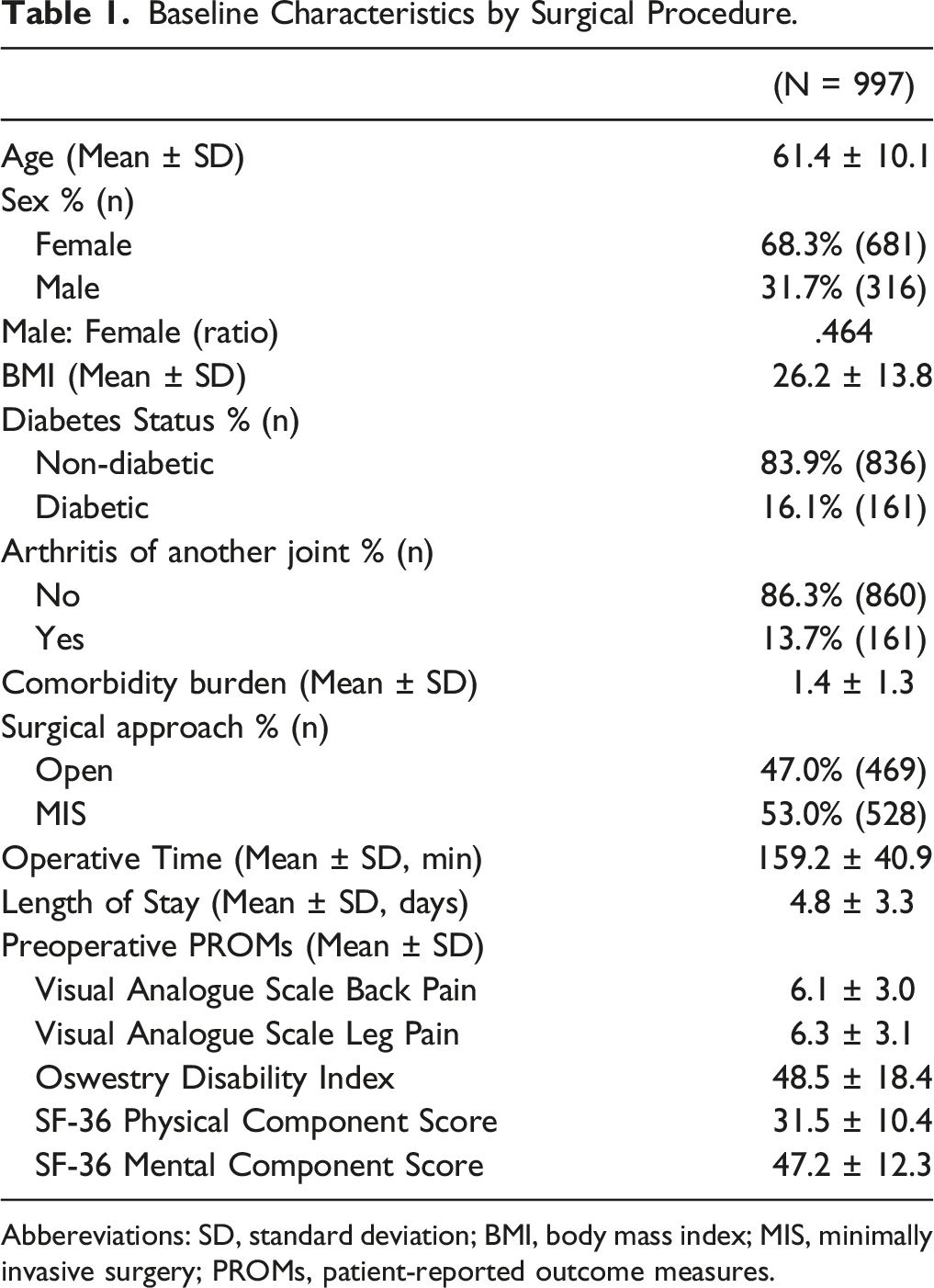
Abbereviations: SD, standard deviation; BMI, body mass index; MIS, minimally invasive surgery; PROMs, patient-reported outcome measures.
Changes in Patient-Reported Outcomes over 2 years.
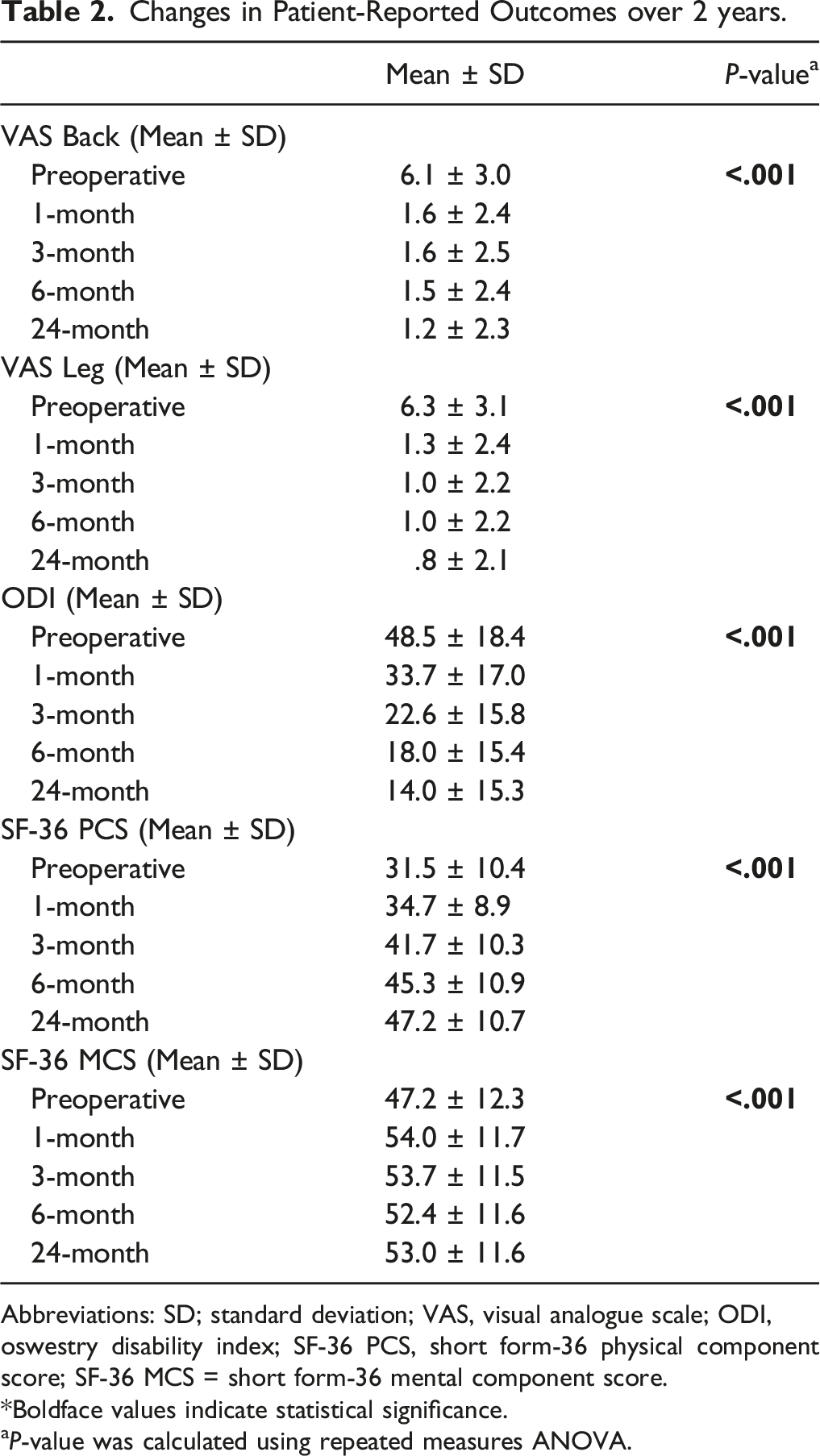
Abbreviations: SD; standard deviation; VAS, visual analogue scale; ODI, oswestry disability index; SF-36 PCS, short form-36 physical component score; SF-36 MCS = short form-36 mental component score.
*Boldface values indicate statistical significance.
aP-value was calculated using repeated measures ANOVA.
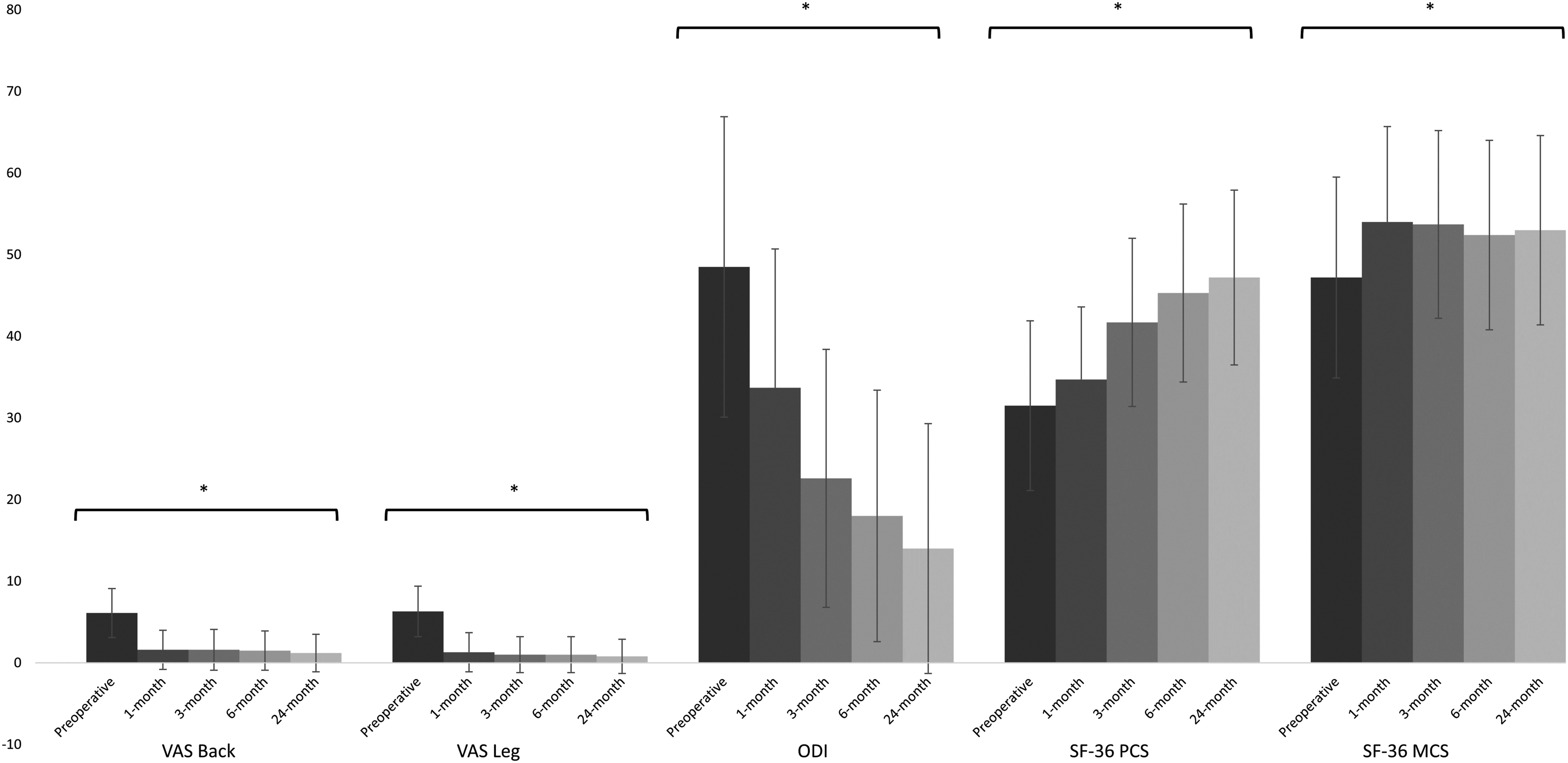
Changes in patient-reported outcomes at 1 month, 3 months, 6 months and 2 years after TLIF surgery.
MCID Achievement, Satisfaction and Expectation Fulfilment at 2 years.
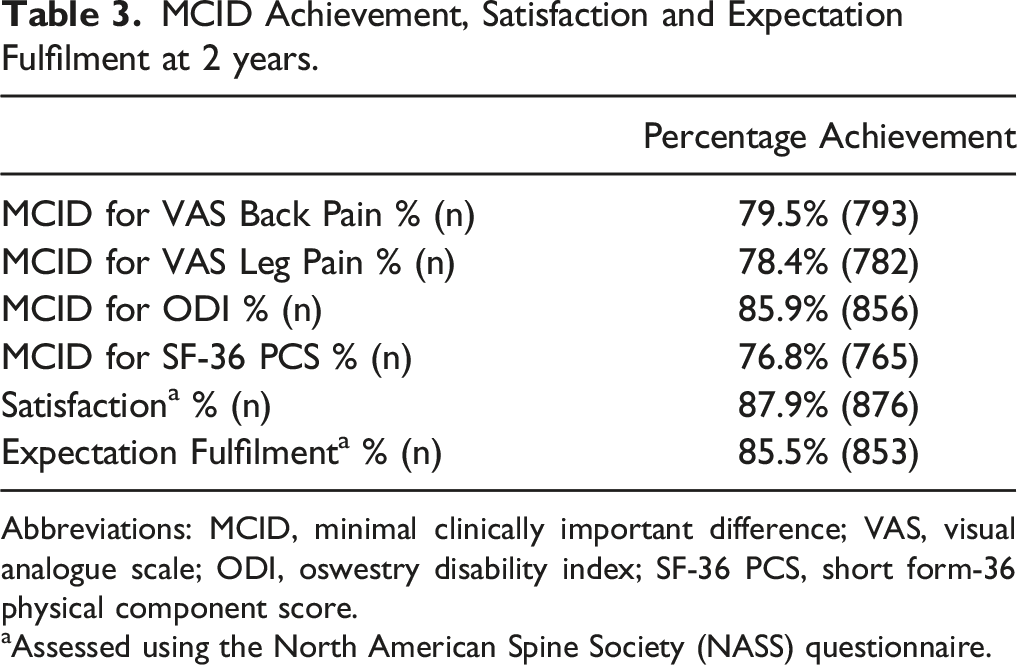
Abbreviations: MCID, minimal clinically important difference; VAS, visual analogue scale; ODI, oswestry disability index; SF-36 PCS, short form-36 physical component score.
aAssessed using the North American Spine Society (NASS) questionnaire.
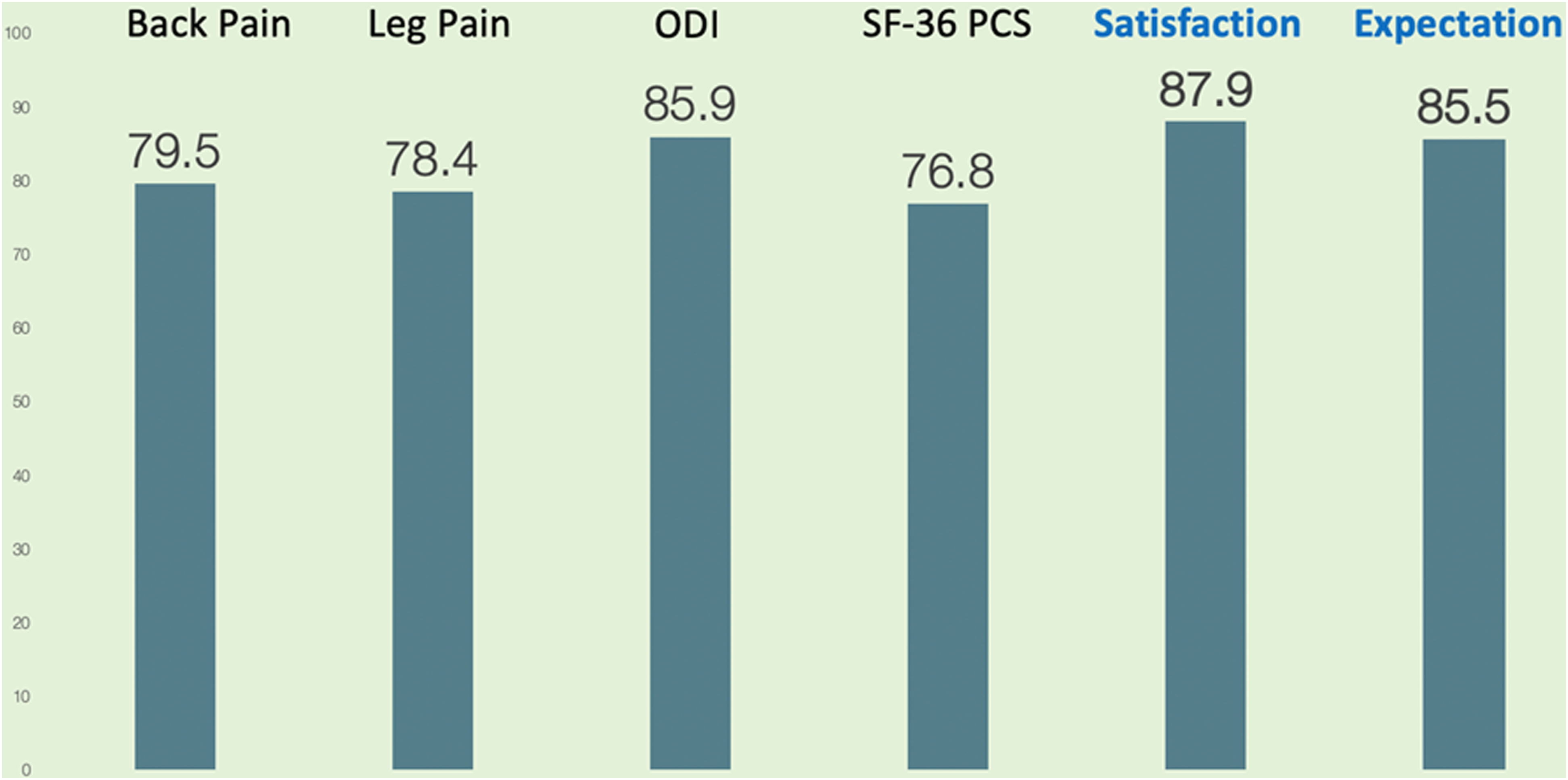
Percentage of patients achieving MCID and patient satisfaction at 2 years. ODI, oswestry disability index; SF-36 PCS, short form-36 physical component score.
Preoperative Variables Independently Associated with Outcomes at 2 years.
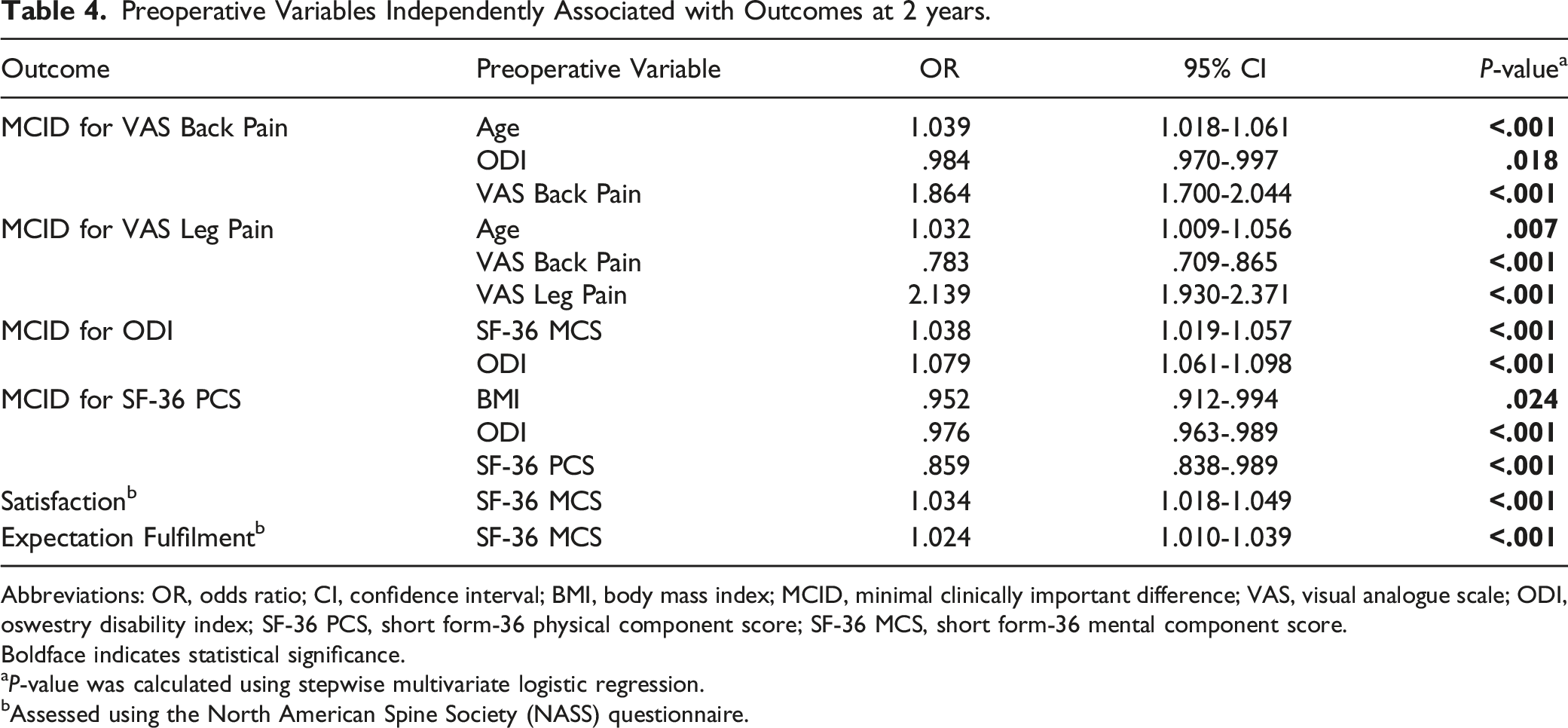
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; MCID, minimal clinically important difference; VAS, visual analogue scale; ODI, oswestry disability index; SF-36 PCS, short form-36 physical component score; SF-36 MCS, short form-36 mental component score.
Boldface indicates statistical significance.
aP-value was calculated using stepwise multivariate logistic regression.
bAssessed using the North American Spine Society (NASS) questionnaire.
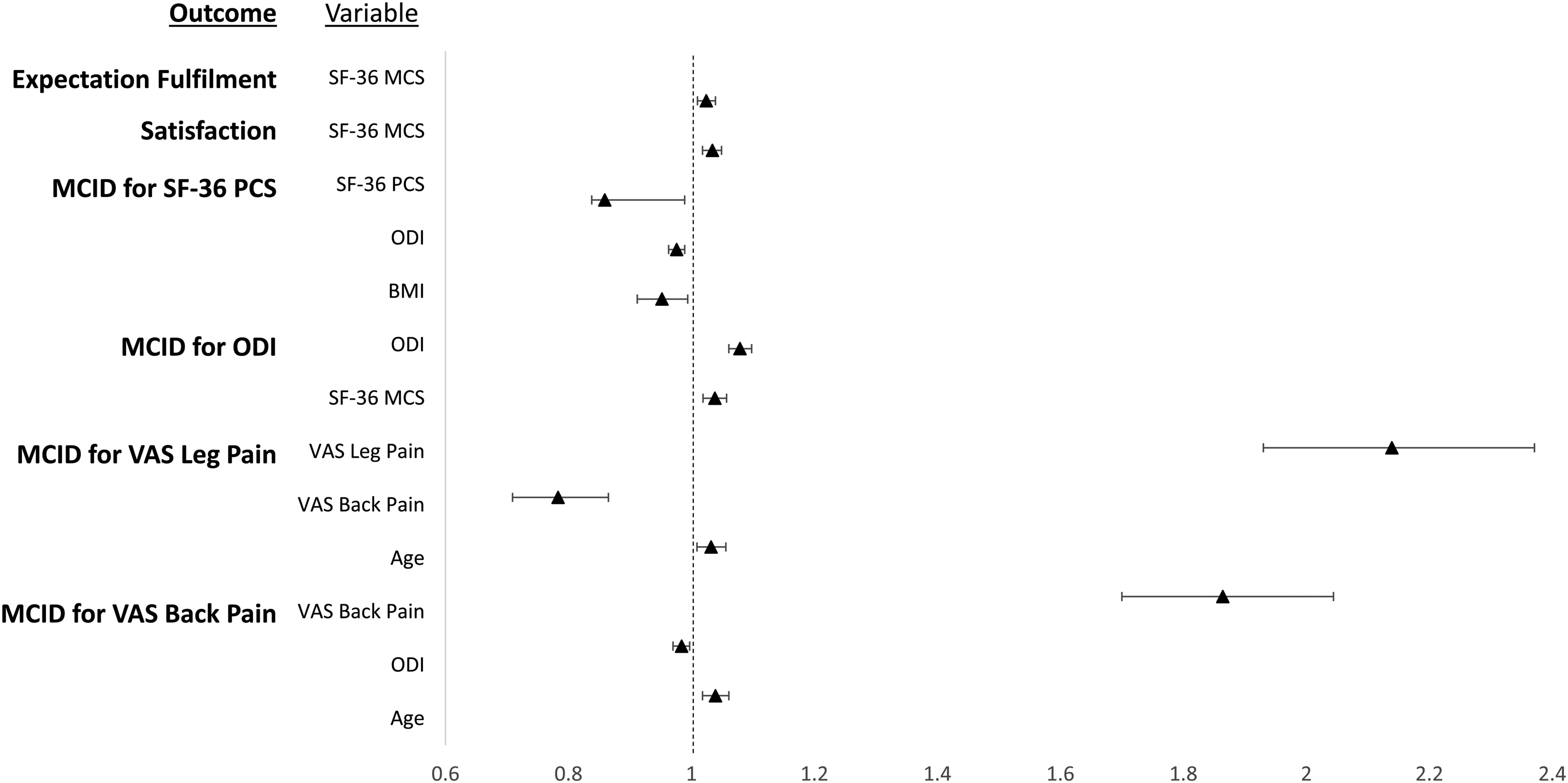
Odds of perioperative variables on achieving clinically meaningful outcomes at 2-years after TLIF surgery.
Discussion
This study has identified preoperative factors associated with clinically meaningful improvement, patient satisfaction and expectation fulfilment at 2 years in patients undergoing single-level TLIF for degenerative spondylolisthesis. Older patients were more likely to experience a clinically significant improvement in back or leg pain, while patients with less disability preoperatively were more likely to experience an improvement in back pain and quality of life. Of note, a patient’s preoperative mental health was independently associated with multiple outcomes such as a clinically meaningful improvement in functional disability, postoperative satisfaction and expectation fulfilment at 2 years.
The proportion of patients attaining MCID for VAS Back, VAS Leg, ODI and SF-36 PCS was 79.5%, 78.4%, 85.9% and 76.8%. respectively. This was comparable to MCID attainment rates in other studies. In a similar study by Hijji et al. 6 of 165 patients undergoing MIS TLIF for spondylolisthesis, the MCID attainment rates for VAS back, VAS Leg, and ODI were 75.76%, 71.05%, and 61.64%, respectively. In another study by Glassman et al. 22 of 80 patients with spondylolisthesis who underwent posterolateral fusion, the proportion of patients achieving MCID for VAS back, VAS Leg, and ODI were 70%, 73.8%, and 73.8% respectively. Overall, these findings reiterate the clinical efficacy of lumbar fusion in appropriately selected patients with degenerative spondylolisthesis. 23
The effect of age on postoperative outcomes has previously been studied in patients undergoing lumbar surgery, notably by Crawford et al. 21 , who reported that an older age range was predictive of best outcomes in a cohort of 396 patients. In contrast, Sigmundsson et al. 24 investigated 5100 patients undergoing surgery for spinal stenosis and found that older age was associated with slightly lower odds of satisfaction. While these results may differ, a study by Goh et al. 25 of 168 patients undergoing single-level MIS TLIF found that elderly patients experienced similar improvements in pain, function, and quality of life after surgery as their younger counterparts. Studies have found an age-related enhancement in pressure pain sensitivity, predisposing older patients to an increased perception of musculoskeletal pain compared to their younger counterparts. 26 Consequently, we postulate that the pain relief gained after lumbar fusion was more likely to be perceived by these older patients, explaining the positive association between MCID attainment for pain scores and increasing age. Nonetheless, these processes are complex and multifactorial, and further studies are required to better understand the impact of advanced age on postoperative outcomes after spinal surgery. 27
Another key finding of the present study was that patients with less disability and lower BMI were more likely to experience a clinically meaningful improvement in back pain and quality of life. Supporting these findings, another study by Elsayed et al. 28 of 99 patients undergoing lumbar spine surgery found that patients with poorer preoperative function and activity reported greater back pain, lower quality of life, and higher disability postoperatively. In a study of 529 patients who underwent surgery for lumbar spinal stenosis, Hebert et al. 29 found that those with greater preoperative disability were more likely to have poor overall outcomes after surgery as well. Some existing studies have suggested that BMI does not significantly influence functional and clinical outcomes after TLIF surgery.30,31 Nonetheless, other studies have shown that patients with higher BMI undergoing spine surgery tend to have significantly greater leg pain and disability and poorer patient-reported outcomes and satisfaction than their counterparts with lower BMI.32,33 It is likely that patients with lower BMI and better functional status at baseline can better engage in postoperative rehabilitation, so as to achieve clinically significant improvement in function and quality of life. This in turn may have value with respect to patient selection, preoperative counselling, and managing patient expectations when considering lumbar spine surgery. 28
Existing literature has shown that psychiatric conditions, such as anxiety and depression, significantly influence postoperative expectation fulfillment and patient satisfaction after spine surgery.34,35 In a study of 919 patients undergoing lumbar decompression or fusion surgery, Miller et al. 36 found that preoperative depression was significantly associated with reduced improvement in postoperative quality of life, as measured by the EuroQol five-dimensions (EQ-5D) outcome measure. Likewise, another study by Chapin et al. 37 of 166 patients who underwent lumbar spine surgery found that patients with depression had significantly worse ODI and EQ-5D scores at 3 and 12 months postoperatively. In a study of the US National Hospital Discharge Survey database from 1990 to 2007, Menendez et al. 38 found that the prevalence of diagnosed depression, anxiety, and schizophrenia increased over time, and that patients with such psychiatric disorders had significantly higher risk of perioperative adverse events and posthospitalization care. Consistent with previous studies, the present study also found that patients with lower preoperative SF-36 MCS, a validated screening tool for depression,39-41 had poorer subjective outcomes in terms of satisfaction and expectation fulfilment. As such, it is essential that surgeons counsel patients regarding the influence of preoperative depression and mental health on postoperative outcomes after spinal surgery. 42 Furthermore, the present findings support recommendations that preoperative optimization of mental health should be pursued to improve patient satisfaction after spinal surgery. 20 Preoperative psychological screening of patients undergoing spine surgery might also ultimately lead to better postoperative outcomes, given the increasing prevalence of psychiatric disorders in the general population. 38
A recent study by Schneider et al. 43 identified several patient-related, radiographic and surgeon-dependent factors significantly associated with the decision to perform fusion surgery in patients with lumbar degenerative spondylolisthesis. The authors found that the decision for fusion surgery was based on multiple factors, including patient demographics, regional preferences and surgeons’ renumeration model. 43 However, it remains unclear if decisions guided by such factors would lead to significantly meaningful improvement in outcomes for patients postoperatively. Previous Quality Outcomes Database (QOD) studies on patient with lumbar spondylolisthesis have shown that older age, preoperative active employment, and decompression and fusion surgery are associated with reduction in disability, higher odds of patient satisfaction and clinically meaningful improvement44,45. The demographic and patient-reported outcomes investigated in this study may aid in tailoring decision-making, and help improve patient satisfaction and quality of life.
Nonetheless, the present study has several limitations. First, this was a retrospective review of a consecutive series of patients. However, several steps were taken to limit bias: Independent assessors who were blinded to the study design evaluated functional outcomes at each follow-up visit; all functional outcome scores were prospectively recorded as part of our institutional spine registry; and all patients were treated at the same tertiary hospital and received standardized perioperative care. Second, the present study did not include factors such as preoperative active employment, 46 duration of symptoms, percentage of patients with neurological deficits/ disabling pain, degree of radiographic spinal stenosis 47 and other parameters such as proximal spinal cord signal changes, which have been shown to affect postoperative outcomes.48-50 Although we found that increasing age was significantly associated with clinical improvement in back pain and leg pain, it is possible that this could be confounded by the duration of preoperative symptoms as we did not routinely collect this data in our registry. The present study also did not include perioperative factors such as the operation duration, postoperative complication rates, postoperative hospitalization duration and fusion rates. Future studies should incorporate such factors to better determine predictors of clinically significant improvement after spine surgery. Nonetheless, recent studies have shown that perioperative outcomes51,52 and radiographic fusion rates53,54 do not influence patient-reported outcomes at 1 to 4 years post-surgery. Third, the present study did not include subgroup analysis of patients undergoing MIS and open surgery despite possible differences in clinical outcomes, complication rates and predictors between these subgroups.55,56 However, a previous study by Seng et al. 57 found that both MIS TLIF and Open TLIF had comparable clinical outcomes with no significant differences in PROMs at 5 years follow-up. Fourth, the predictive factors identified in this study differed from previous studies, possibly due to differences in outcome variables and statistical methods. 58 Nonetheless, we utilized well established outcome scores such as the ODI and SF-36, as well as the validated NASS questionnaire, thus allowing for a comprehensive assessment of the results following lumbar spine surgery. Fifth, a proportion of patients who were lost to follow-up could have experienced poor outcomes, thus introducing attrition bias into the study. While this is important, authors have cautioned against the assumption that patients lost to follow-up have poorer results 59 , and there is still no consensus regarding the adequate follow-up rate for PROM studies. The current follow-up rate of 70.2% is above the minimum threshold of 60-70% reported in the literature60,61 and is close to the 80% gold standard for clinical trials.
Conclusion
In conclusion, patients who were older, have less preoperative disability and better preoperative mental health were significantly more likely to attain clinically meaningful improvement in PROMs and postoperative satisfaction after single-level TLIF. Identification of these factors would aid surgeons in patient selection and surgical counselling for single-level TLIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained from the local institutional review board