
Abstract
Study Design
Retrospective cohort study.
Objective
Cavernous malformations (CMs) and hemangioblastomas (HBs) of the spinal cord exhibit distinct differences in histopathology but similarities in the neurological course. The aim of our study was to analyze the clinical differences between the vascular pathologies and a benign tumor of the spinal cord in a perioperative situation.
Methods
We performed a retrospective analysis of patients who had undergone surgery for lesions in the spinal cord between 1984 and 2015. Patients were screened for CMs and HBs as the primary inclusion criteria. General patient information, surgical data, and disease-specific data were collected from the records. Cooper–Epstein scores for clinical symptoms were evaluated preoperatively, at discharge, and at the 6-month follow-up.
Results
A total of 112 patients were included, of which 46 had been diagnosed with CMs and 66 with HBs. Patients with CMs often demonstrated more preoperative neurological deterioration compared to those with HBs (P < .05); accordingly, in took longer to diagnose HBs. Complete resection was possible for 96.8% of all patients with CMs and 90% of those with HBs. At the 6-month follow-up, patients with HBs more often presented with persisting neurologic impairment of the upper extremities compared to the CM patients (P < .001).
Conclusion
CMs and HBs of the spinal cord have similarities but also exhibit significant differences in neurological presentation and perioperative course. Surgical therapy is the treatment of choice for symptomatic lesions, and complete surgical resection is possible in the majority of cases for both entities. Neurologic outcomes are usually favorable, although patients with HBs retain neurologic deficits more often.
Introduction
Cavernous malformations (CMs) and hemangioblastomas (HBs) are both lesions of the central nervous system. Cerebral CMs are vascular pathologies that occur with a prevalence of .4%-.6%, mainly in a supratentorial manifestation.1-3 Only 5% are located in the spinal cord, but, with a 5%-12% representation of all spinal cord lesions, they still comprise the most common spinal vascular lesion1-3. In addition, up to 40% of patients with CMs of the spinal cord have other manifestations in the central nervous system (CNS).4,5 This combined occurrence strongly suggests a genetic predisposition and should be investigated. 5 In the remaining cases with sporadic occurrence, the lesions are mainly congenital but can also occur de novo, for example, after radiation. CMs are characterized as well-circumscribed lesions with abnormally dilated, irregularly thick, and thin-walled sinusoidal vascular channels without infiltration into the surrounding parenchyma. 6 Although CMs are angiographically occult, there are some small feeding arteries and low-flow draining veins. Furthermore, CMs are frequently associated with venous abnormalities. There is often gliotic and hemosiderin-stained neural tissue parenchyma surrounding the lesion, and signs of thrombosis and calcification may be visible on magnetic resonance imaging (MRI), which is the diagnostic modality of choice.1,6,7 The natural course of CMs is difficult to predict, as they can grow, shrink, or remain unchanged. 8 The reported annual rate of hemorrhage is between 1.4 and 6.8%,9-12 but the risk of neurological decline for each patient is unpredictable, as neurological impairment due to hemorrhaging varies significantly.7,13 The main recommended treatment options are observation with serial imaging in asymptomatic patients or surgical resection for symptomatic patients; localization of the CM permits resection with an acceptable risk to neurological functioning.7,13 Stereotactic radiosurgery is controversial and seems to have results that are comparable to the natural course of the lesion, but it is associated with significant morbidity.14-16 The risk of CMs rebleeding is eliminated after total resection, whereas incomplete resection increases the risk for further episodes of hemorrhaging. 16
HBs are rare benign tumors (CNS WHO grade 1) that arise from undifferentiated mesenchymal cells, are most commonly located in the cerebellum, and account for 1.6%-5.8% of all spinal cord lesions. 3 Of these, 75% are sporadic lesions, and 25% are associated with the von Hippel–Lindau syndrome (VHL).3,4 HBs are usually non-infiltrating and well-demarcated but highly vascularized benign tumors. The recently published World Health Organization classification of CNS tumors categorizes this entity as CNS WHO grade 1. As previously mentioned, contrast-enhanced MRI is the diagnostic modality of choice and usually shows isointensity on T1-weighted images and hyperintensity on T2-weighted images. There is frequently also an associated cyst or syrinx and intramedullary edema, which is responsible for the neurological symptoms. Asymptomatic spinal HBs can be followed with serial imaging, but microsurgical en bloc resection of the tumor is recommended in cases with neurological deterioration.17,18
There is a significant amount of literature on spinal cord CMs and many case reports of spinal cord HBs, but, to the best of our knowledge, a comparison study on the various aspects of these vascular pathologies and tumors of the spinal cord has not yet been conducted. In addition to the similarities that may exist on imaging of small pathologies, such as those found in the spinal cord, there are significant differences, especially in terms of outcome but also in terms of surgery. Even though these lesions are fundamentally different pathological entities, initial neurological symptoms are often similar, although differentiation on imaging diagnostics can also be difficult for small lesions that occur in the spinal cord. Therefore, our study aims to evaluate the clinical courses of the entities and analyze the perioperative symptoms and postoperative neurological course to pinpoint the similarities and differences in detail. Ultimately, we aim to provide more information for clinical practice to facilitate the complex management of these pathologies that are often challenging to distinguish preoperatively.
Material and Methods
Ethics
The study was presented to the relevant ethics committee (local Ethical Review Board of Hamburg, Germany [2022-300260-WF]) and was performed in accordance with the ethical standards laid down in the Declaration of Helsinki and its latter amendments. Because the data were anonymized and the study was retrospective, informed consent was waived.
Data Acquisition
We retrospectively reviewed the medical records of all patients with spinal cord pathologies who had undergone surgery at our institution between 1984 and 2015. The primary inclusion criterion for enrollment in our study was a histopathologically confirmed diagnosis of (1) CMs or (2) HBs on the basis of the neuropathological reports on the intraoperatively harvested tissue. The medical reports were screened for the neurological symptoms at initial presentation and the time period between diagnosis and surgery. The Cooper–Epstein score was evaluated preoperatively, at the time of discharge from the hospital, and 6 months postoperatively (Cooper, 1985 #54). In the Cooper–Epstein grading system, the motor function of the upper extremities is graded from grade 0 (intact) to grade 4 (no function) and that of the lower extremity from grade 0 (intact) to grade 5 (plegia). The neurological status of the upper and lower extremities in the 2 entities was analyzed separately and compared. MRI images of the site and extent of the lesion on sagittal and axial T1 slides with and without contrast agents were reviewed (Figure 2). HBs that were only a small portion in the spinal cord were excluded, so that the 2 entities studied can be considered true spinal cord pathologies (Figure 1). Lesions were categorized according to their location in the (1) cervical spinal cord (Csc), (2) thoracic spinal cord (Tsc), or (3) conus medullaris (Cm). The surgical procedures were extracted from the surgical reports. Complete resection was defined as both the absence of residual tumor mass based on the report of the intraoperative inspection the absence of any residual on contrast-enhanced initial postoperative MRI images. Imaging findings of HB (A1/A2) and CM (B1/B2) on axial and sagittal MRI slices with contrast enhancement. Both lesions are located within in cervical spinal cord at the level of C1/2 respectively C2/3. HB in this case present as cystic lesions with a contrast-enhanced nodule as a solid tumor mass. A syrinx is absent (A1/A2). In comparison to schematic HB in Figure 1, this case does not show any epidural vessels in proximity of the tumor mass. CM present with heterogenous signal intensity on MRI images, resulting in a characteristic “popcorn appearance” (B1). T2 weighted show a hyperintensity signal around the tumor mass as a sign of intramedullary edema (B2). In addition to the spinal cord HB, the patient with HB (A1) shows multiple intracranial masses (n = 1/66).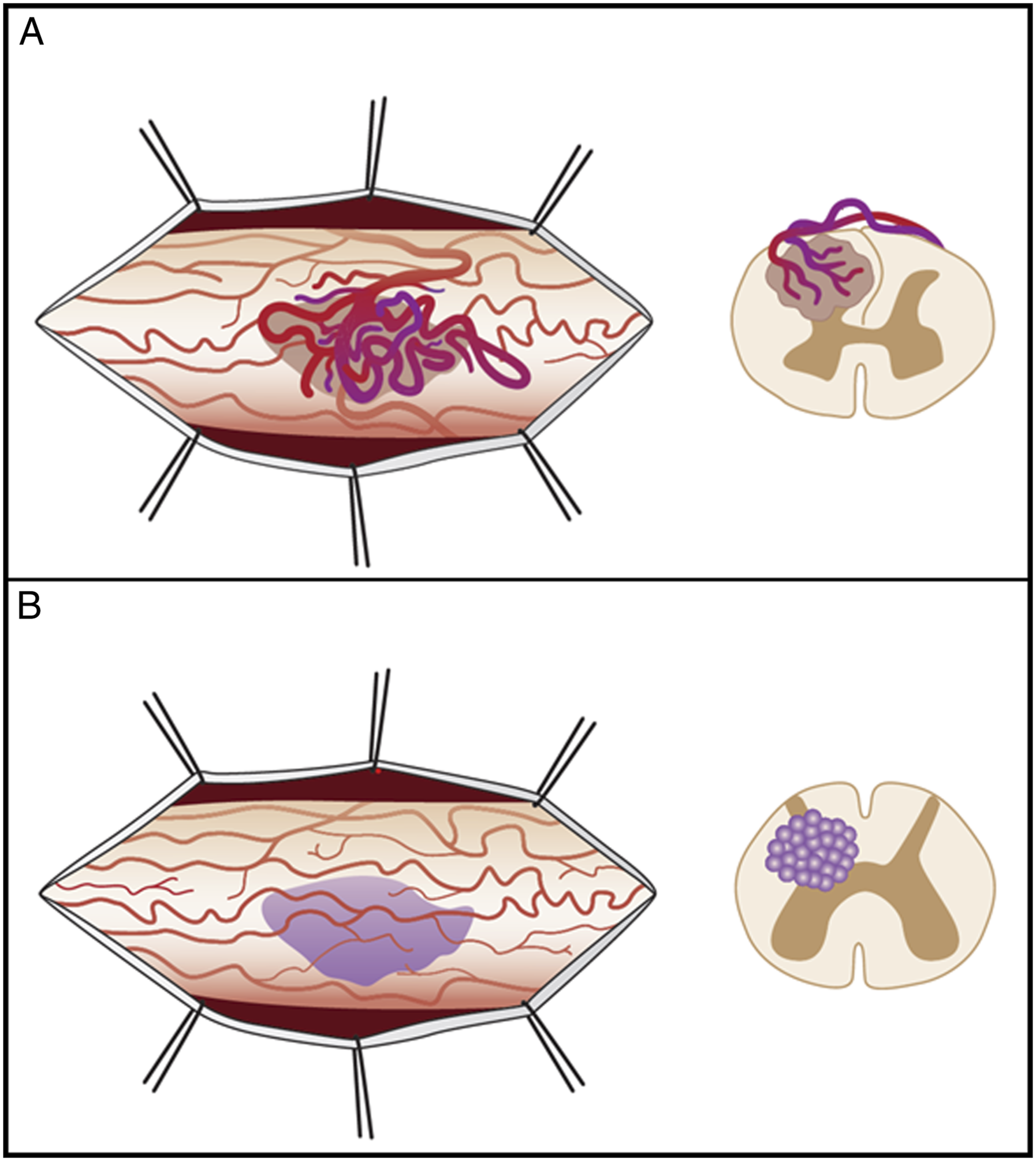
Surgical Procedure
All procedures were performed under general anesthesia in the prone position. Access to the space was gained via laminoplasty. The lesions were approached via a midline myelotomy and resected under operating microscope illumination. The patients were neuromonitored during the procedures (IONM) 26 .
Statistics
Student’s t-test, Wilcoxon signed-rank test, and Chi2 test were used for the evaluation of significant differences on a 95% confidence interval, depending on the type of data and Gaussian data distribution. All analyses were performed using IBM Inc. SPSS version 24 (Chicago, IL, USA).
Results
Patient data
Population Characteristics of Patients With CMs and HBs.

Genetic Predisposition, Clinical Presentation, and Postoperative Neurological Course
Overview of Neurologic Status Preoperatively, at Discharge, and at the Time of 6-Month Follow-Up Improved or Equal to Preoperative Status.

Radiological and Histopathological Features
The time period between diagnosis and surgery varied significantly, with 51.3 ± 59.6 weeks for patients with CMs and 129.2 ± 153.9 weeks for those with HBs (P < .01). Overall, 40% of the pathologies were located in the cervical spinal cord, 54.7% in the thoracic spinal cord, and 5.3% in the conus medullaris, with CMs (Csc 41.3%; Tsc 56.5%; Cm 2.2%) and HBs (Csc 40.6%; Tsc 50.0%, Cm 9.4%) subdivided almost equally between these locations. All the lesions were generally small and localized, spanning a mean of 1.7 segments in CMs and 2.2 segments in HBs. CMs showed heterogeneous signal intensity on weighted images of T1 and T2 due to blood products of varying ages and a low signal intensity rim on weighted images of T2 (hemosiderin). On T1-weighted images with contrast agents, CMs occasionally demonstrate minimal enhancement. In contrast, HBs most commonly presented with a hypointense to isointense to normal spinal cord. In T2-weighted images, HBs presented isointense to hyperintense focal flow voids in larger lesions, usually with an associated syrinx. The tumor nodule is enhanced in T1-weighted images with contrast agents. Gross total resection was achieved in 95.7% of patients with CMs and 89.4% of those with HBs (NS, P = .478; Table 1, Figure 2). In cases with complete resection, no tumor recurrence was seen for either entity at follow-up. Figure 3 shows exemplary illustrations of the histopathological characteristics of HBs and CMs. HB (A) and CM (B) are often comparable in size and can both reach the surface of the spinal cord and shine through the pia mater. Nevertheless, both lesions show distinct differences to each other. In HB (A), epidural vessels may be present in some cases with close proximity to the tumor mass, which can reach an enormous diameter and blood flow. These ensure that HBs can be visualized in some cases on angiography. If present, these vessel have impact on the surgical approach. In CM (B), pathological vessels are absent and therefore these lesions cannot be visualized on angiography. Hematoxilin-and-eosin-stained section of a hemangioblastoma in the craniocervical junction of a 32-year-old female showing a capillary-rich tumor consisting of characteristic vacuolated stroma cells with mildy pleomorphic medium-sized nucleoli (arrow; scale bar = 100 µm) (A1). The stroma cells in hemangioblastoma typically stain positive in an immunohistochemical stain with an antibody against inhibin-alpha. Same case as above (scale bar = 100 µm) (A2). Elastica-van-Gieson’s stain of a cavernoma in the cervical spinal cord of a 52-year-old male featuring closely juxtaposed thin-walled capillary-like vessels with wide lumina and moderate periadventitial fibrosis (scale bar = 250 µm) (B1). The parenchyma of the spinal cord adjacent to a cavernoma typically shows marked regressive changes with rarefication and signs of prior microbleedings with siderophages and free parenchymal siderin (arrows). Same case as above (scale bar = 100 µm) (B2).

Therapeutic procedure
Overview of the Lesion Location and the Various Aspects of Microsurgical Therapy.

Discussion
We investigated the perioperative clinical features of CMs and HBs of the spinal cord in this single-center retrospective study. The key results of our study are as follows: (1) Females were more commonly affected by both lesions in midlife compared to males. (2) Patients with CMs were significantly more likely to become symptomatic as a result of neurological deterioration, whereas HBs were usually diagnosed incidentally. (3) Surgical treatment achieves good resection results, and the neurological outcome at the 6-month follow-up is favorable, even though patients with HBs are at a greater risk for prolonged neurological impairment.
Overview of Specific Features of HBs and CMs.

In addition to the initial neurological symptomatology, acute or gradual neurological deterioration is possible with both lesions and can manifest as both motor and sensory deficits. 19 In patients with CMs, acute neurologic deterioration is often due to relevant hemorrhages in the spinal cord, whereas slow progressive deterioration is usually associated with repeated microbleeds. 20 In contrast, neurologic symptoms are often milder and more non-specific in patients with HBs.11,16,20 The symptomatology depends on the location of the lesion and may be associated with radiculopathy, myelopathy, hypesthesia, weakness, hyperreflexia, pain, and incontinence.17,20 The rather mild and non-specific symptoms often cause a delayed diagnosis compared to patients with spinal cord CMs. 3 The data in our study ultimately confirm these statements in the current literature in the sense that the majority of patients with CMs became acutely symptomatic, which leads to a significantly shorter time to diagnosis and treatment compared to patients with HBs. We could not detect any significant differences in the gender distribution among the patients, although women were slightly more frequently affected by both lesions.1,13,19 With a mean age of 41 years, our patient collective had the same peak age as in previous studies.1,13,19 An important aspect of HBs is genetic predisposition due to the VHL syndrome, which is thought to be causative in up to 30% of HB lesions.4,21,22 We identified 5 patients in our cohort with HBs who had VHL and also suffered from multiple lesions. These patients were also younger than the other patients. This incidence is essentially the same as reported in the literature, but significantly lower than the approximately 20% reported in some studies. 21
The most important diagnostic tool, and the gold standard in the further evaluation of these patients, is MRI, which provides important information regarding the shape of the lesion, which is crucial for further treatment planning.3,23 CMs often present with gliotic and hemosiderin-stained neural tissue parenchyma and signs of thrombosis and calcification around the lesion, as previously outlined.1,6,9 HBs often demonstrate isointensity on T1-weighted images and hyperintensity on T2-weighted images, as well as an associated cyst or syrinx and intramedullary edema.11,23 The MRI scans of our reviewed cohort showed these above-mentioned characteristics of CMs and HBs. Nevertheless, the differences are usually so striking that, in most cases, the distinction on imaging is effortless. However, a histopathological diagnosis based on these findings is clearly not possible. Therefore, for an accurate diagnosis, histopathological examination is mandatory; this was done in all our cases, and, therefore, it is the basis of our further analyses.
A question that often arises is when to operate on a patient with a newly diagnosed but probably non-malignant vascular pathology, especially if they are not currently experiencing neurological symptoms. For spinal CMs and HBs, there is widespread consensus that surgery is indicated in cases where there is neurological deterioration or lesion progression, shown on repetitive imaging controls.11,19 In cases with only mild neurologic symptomatology and a stable lesion according to repetitive MRI scans, a “watch-and-wait” strategy with frequent radiological and clinical follow-ups is possible. In our department, we followed these recommendations and adopted a “watch-and-wait” strategy for asymptomatic patients. The approach of imaging assessment to detect risk factors to predict the neurological development of individual patients has been selected, but an accurate prediction of the clinical course is impossible. Evidence of microbleeds, which can explain or cause neurological deterioration, can only be obtained for CM patients. 24 A special feature of HBs is that dilated and partly thrombosed vessels often occur in their immediate vicinity, which, on the 1 hand, support the imaging classification of the mass, but, on the other hand, must be considered with regard to surgical treatment. In these special cases, spinal angiography may be considered for further diagnostic evaluation, and it has several potentially positive aspects. The anatomy of the lesions can be assessed in more detail, which is significant with regard to surgical treatment. In addition, the intraoperative blood loss can be reduced and duration of surgery shortened by preoperative embolization. 25 In line with these recommendations, in our cohort, only 2 HBs were embolized preoperatively. Neither patient demonstrated any clinical deterioration after the intervention. In general, however, it should be possible to perform the surgical procedure directly after the intervention to rapidly counteract any deterioration. 26
In cases of acute or progressive neurologic deterioration, microsurgical resection is the treatment of choice for both lesions.16,17,26 The surgical procedure is an individual decision and depends on the clinical condition of the patient as well as the location and extent of the lesion. 27 Regardless of the type of lesion, in our cohort, the microsurgical approach was chosen via targeted myelotomy to access the most direct surgical corridor and minimize tissue damage. 26 It is important to achieve complete resection of CMs in microsurgical treatment because there is a risk of rebleeding if there is residual tissue. 16 One aspect that must be considered in the treatment of hemorrhaged CMs is the recommendation to not perform surgery during the acute phase after a hemorrhage but to wait until the surrounding nerve tissue recovers and the formation of gliotic tissue has been completed.28,29 Therefore, a waiting period after the last symptomatic bleeding is currently recommended to minimize the risk of perioperative neurologic deterioration. 19 In our cohort, we studied 46 patients with spinal CMs, all of whom were treated surgically, sometimes immediately after diagnosis and sometimes after a period of a “watch-and-wait” strategy. The goal of gross total resection was achieved in 45 patients. Compared to those with HBs, patients with CMs demonstrated preoperative neurological deterioration much more frequently, usually caused by sudden or repeated hemorrhaging. in our review of the neurologic examinations, we found that, immediately post-operatively, patients demonstrated persisting neurological functional impairment, but the majority of patients had recovered at the 6-month follow-up. In a comparison of our results with data from the literature, we found that the findings regarding neurological recovery after surgery are within a comparable range.9,11,30 It is also worth mentioning that the rate of neurological deterioration described in the literature varies significantly, ranging from 4%-50%, although it should be noted that, in some cases, no neurological classification system was used, which makes it difficult to understand the basis of the surveys reliably.16,17 In summary, we regard the surgical treatment of CMs as an approach to prevent further neurologic deterioration and a safe procedure when performed at a high-volume center. For patients with HBs, microsurgical resection is also the treatment of choice and the only curative approach currently. In this context, we should discuss the finding that a significantly higher number of patients with HBs (16.7%) had had previous surgery compared to patients with CMs. A possible explanation for this is the finding that complete resection is more likely for CMs than for HBs, and, thus, the potential for recurrence is greater. Unlike CMs, there is usually a delay in the diagnosis of HBs because their clinical course is progressive over time rather than acute. 23 Ultimately, this is due to the fact that with HBs, syrinx and edema account for the neurologic deterioration, and hemorrhaging typically does not occur. 23 Accordingly, the time to diagnosis of patients with HBs was significantly prolonged in our cohort compared to that of the patients with CMs. En bloc resection of the solid tumor mass through microsurgical dissection is also the treatment of choice for this lesion and usually results in the collapse of the cystic formation.18,23,26 In our study, data analysis showed that patients with HBs often had significantly better neurological function preoperatively than patients with CMs but experienced a comparatively poorer and prolonged recovery after surgery. The risks of neurological deterioration with persistent functional impairment are described in the literature. A recovery period of 6 months has been reported for the neurologic impairment that occurs immediately after surgery, with the majority of patients recovering satisfactorily with only mild residual functional impairment .22,31 It should be noted that there was no difference in the neurologic recovery of patients with sporadic HBs and patients with HBs associated with VHL in our cohort. The different locations of the tumors represent a factor that may also contribute to a poorer postoperative functional outcome in HB patients. Although we could not find a statistically detectable difference, HBs are more frequently localized in the conus medullaris. Furthermore, the fact that there is not always clear tumor boundary to the spinal cord may cause difficult resectability and, thus, a poorer functional outcome.
The auxiliary tools that can be used in surgery are a factor that can enhance patient safety. There is indisputable and absolute consensus on the use of intraoperative neuromonitoring (IONM), which is standard in surgical interventions on the spinal cord.26,32 In our hospital, this monitoring is also standard in each of these surgeries to enable detection of any possible deterioration in neurological functions at an early stage. Some studies have investigated the use of ICG angiography during the resection of HBs with their associated vascular pathologies and have demonstrated a positive effect on the understanding of the vascular anatomy and assessment of the perioperative spinal cord perfusion, which makes it a useful tool.
In addition to the new insights and results provided by our study, there are, of course, limitations to our study that should be noted. First, our study is retrospective and monocentric, which has resulted in a smaller number of cases and only allows conclusions to be drawn regarding treatment procedures that had already been performed. The retrospective nature of this study also means that the evaluation is dependent on the quality of the documentation and completeness of the patient records, which can lead to problems with data collection and analysis. The data presented here were collected for a 31-year period, which means that the above-mentioned arguments regarding data quality become even more important. To ensure that the statistical analysis was based on valid data, the final analysis incorporated data that were reliably available for all patients. Due to the long period of patient data collection, we had to accept a trade-off between a detailed analysis and valid data quality in the belief that we could perform a reliable analysis. This meant that we did not have to exclude any patients from the study due to missing data. Furthermore, as mentioned at the start of the discussion, we compared 2 entities that have different histopathological natures and, to the best of our knowledge, have not yet been compared in any systematic study. We are aware that there may be differences in comparability with regard to the outcome of the underlying disease, but we note that there are advantages of comparing 2 benign lesions that occur in the spinal cord. These entities can serve as differential diagnoses and sometimes have similarities in neurological symptoms and imaging features, which should be examined in more detail to be able to better classify the specific characteristics.
Conclusion
CMs and HBs are lesions that can regularly occur spinally, although their histopathological genesis is different. Patients with spinal CMs initially show acute neurological deterioration much more frequently than HBs. In symptomatic lesions, complete microsurgical resection is the treatment of choice in both cases. In the majority of patients, this can be achieved, preventing further neurologic deterioration in many cases. The risk of postoperative neurologic deterioration during surgery exists for both s and HBs. The latter have a greater risk of neurologic deterioration in the postoperative course, but in the short- and medium-term course, both show a recovery trend. These findings must be considered in decision-making for the best surgical timing and approach, ultimately meaning that an individual approach will be required in each surgery.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by T. Pantel, K.C. Mende and T. Mohme. The first draft of the manuscript was written by T. Pantel and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.