
Abstract
Study Design
Multicenter comparative cohort.
Objective
Studies have shown markedly higher rates of complications and all-cause mortality following surgery for adult cervical deformity (ACD) compared with adult thoracolumbar deformity (ATLD), though the reasons for these differences remain unclear. Our objectives were to compare baseline frailty, disability, and comorbidities between ACD and complex ATLD patients undergoing surgery.
Methods
Two multicenter prospective adult spinal deformity registries were queried, one ATLD and one ACD. Baseline clinical and frailty measures were compared between the cohorts.
Results
616 patients were identified (107 ACD and 509 ATLD). These groups had similar mean age (64.6 vs 60.8 years, respectively, P = .07). ACD patients were less likely to be women (51.9% vs 69.5%, P < .001) and had greater Charlson Comorbidity Index (1.5 vs .9, P < .001) and ASA grade (2.7 vs 2.4, P < .001). ACD patients had worse VR-12 Physical Component Score (PCS, 25.7 vs 29.9, P < .001) and PROMIS Physical Function Score (33.3 vs 35.3, P = .031). All frailty measures were significantly worse for ACD patients, including hand dynamometer (44.6 vs 55.6 lbs, P < .001), CSHA Clinical Frailty Score (CFS, 4.0 vs 3.2, P < .001), and Edmonton Frailty Scale (EFS, 5.15 vs 3.21, P < .001). Greater proportions of ACD patients were frail (22.9% vs 5.7%) or vulnerable (15.6% vs 10.9%) based on EFS (P < .001).
Conclusions
Compared with ATLD patients, ACD patients had worse baseline characteristics on all measures assessed (comorbidities/disability/frailty). These differences may help account for greater risk of complications and all-cause mortality previously observed in ACD patients and facilitate strategies for better preoperative optimization.
Keywords
Introduction
Spinal deformity includes a broad range of conditions that can involve all regions of the spine and can impact individuals across all ages. Deformities of the adult thoracolumbar spine have been well studied over the past several decades.1,2 These deformities are most commonly degenerative in nature, but may also result from untreated or residual deformities present in childhood or adolescence, arise from iatrogenic conditions, develop due to underlying neuromuscular or connective tissue disorders, or result from traumatic or neoplastic processes. Classification systems3-7 and strategies for treatment8-12 of adult thoracolumbar deformities (ATLD) have been proposed, and multiple studies of disease impact,13,14 treatment outcomes,15-21 and complications associated with surgical correction20,22-27 have been reported.
In contrast to ATLD, study of adult cervical deformity (ACD) has been far more limited. 28 Early reports of ACD surgery were primarily small case series of the most severe deformities, treated with what was considered high-risk procedures, and often associated with high rates of severe complications.29-31 With more recent advances in anesthesia, critical care, and surgical techniques, and perhaps spurred by progress in the care of ATLD deformity, there has been renewed interest in the study and treatment of ACD. These advances have included proposal of an ACD classification system, 32 description of surgical techniques,33,34 and studies focused on disease impact, 35 treatment outcomes,36-38 and operative complications.36,37,39
As study of ACD has progressed, it has become clear that operative treatment of ACD is associated with markedly higher rates of complications and all-cause mortality than operative treatment of ATLD. For example, all-cause mortality within 1-year of surgery to treat ACD has been reported to be 9-fold higher than for ATLD surgery (9.2% vs 1.0%, respectively).27,40 Although the explanation for these differences is often based on a perceived worse health state of ACD patients, this has not been previously demonstrated. Our objectives were to compare baseline measures of frailty, disability, and comorbidities between ACD and complex ATLD patients undergoing surgery based on 2 large prospectively-collected, multicenter cohorts, one focused on ACD and the other focused on complex ATLD.
Methods
Study Design and Patient Populations
This study is a retrospective review of patients drawn from 2 multicenter, prospective cohort studies, one focused on ACD and the other on ATLD, conducted to assess the outcome of adult spinal deformity among those who underwent surgical treatment at 13 centers across the United States.
The ACD study is registered through ClinicalTrials.gov (NCT01588054). All study participants signed informed consent, and the study received institutional review board approval at all participating sites. Eligible patients were at least 18 years of age and had a diagnosis of cervical deformity with plan for operative treatment. ACD was defined based on meeting at least one of the following radiographic/alignment criteria: (1) C2-C7 sagittal kyphosis (Cobb >15°, (2) T1-slope (T1S) minus cervical lordosis (CL) ≥ 35°, (3) segmental cervical kyphosis >10° between any 2 vertebra between C2 and T1 or >15° across any 3 vertebra between C2 and T1, (4) cervical scoliosis >10° with Cobb angle end vertebra within the cervical spine, (5) C2-C7 sagittal vertical axis (SVA) >4 cm, or (6) McGregor’s slope >20° or chin brow vertical angle (CBVA) > 25°. Exclusion criteria included active spinal infection or neoplasm, deformity due to acute trauma, prisoners, and pregnancy or immediate plans to get pregnant.
The complex ATLD study is registered through ClinicalTrials.gov (NCT04194138). All study participants signed informed consent, and the study received institutional review board approval at all participating sites. Eligible patients were at least 18 years of age and had a diagnosis of adult congenital, degenerative, idiopathic, or iatrogenic thoracolumbar spinal deformity with plan for operative treatment. In addition, for this study of complex thoracolumbar deformities, patients were required to meet any of the following criteria: (1) radiographic criteria (PI-LL ≥25°, TPA ≥30°, SVA >15 cm, thoracic scoliosis ≥70°, thoracolumbar/lumbar scoliosis ≥50°, or global coronal alignment >7 cm); (2) procedural criteria (posterior spinal fusion >12 levels, 3-column osteotomy (3-CO), or anterior-column reconstruction (ACR); or (3) geriatric criteria (age >65 years and minimum 7 levels of spinal instrumentation during surgery). Exclusion criteria included active spinal infection or neoplasm, deformity due to acute trauma, neuromuscular conditions, syndromic scoliosis, inflammatory arthritis/autoimmune diseases, prisoners, and pregnancy or immediate plans to get pregnant.
Data Collection
At preoperative baseline and at postoperative follow-up visits, demographic, clinical, radiographic, and functional frailty data were collected using standardized forms. The present study focuses on preoperative baseline assessments. Demographic and clinical data included patient age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), and American Society of Anesthesiologists (ASA) grade. Patient-reported outcomes measures included the Veterans RAND 12-item health survey (VR-12) with summary physical and mental component scores (PCS and MCS, respectively) and the Patient-Reported Outcomes Measurement Information System (PROMIS).
Assessments of patient frailty included the Edmonton Frail Scale (EFS), 41 the Canadian Study of Health and Aging (CSHA) Clinical Frailty Scale (CFS), 42 and hand grip strength. The EFS was developed as a practical tool to assess frailty in both the inpatient and outpatient settings. The EFS assesses 9 domains: cognition, general health status, functional independence, social support, medication use, nutrition, mood, continence, and functional performance. For the EFS, functional performance is assessed based on the time required to rise from a seated position in a chair, walk 3 meters, and return to and sit in the chair. An overall EFS score is tabulated with 0-5 reflecting “not frail”, 6-7 reflecting “vulnerable”, and scores of >7 reflecting progressively increasing decreases of frailty. The CFS is a judgement-based tool to screen for and broadly stratify varying degrees of frailty that was developed through the CSHA. The CFS score ranges from 1 (very fit) to 9 (terminally ill), with intermediate scores of 2 (well), 3 (managing well), 4 (vulnerable), 5 (mildly frail), 6 (moderately frail), 7 (severely frails), and 8 very severely frail). A hand grip dynamometer was used to assess hand grip strength. In the seated position with the elbow flexed at 90° and the hand in line with the wrist and forearm, the patient was asked to squeeze the dynamometer as hard as possible, first using the left hand, then using the right hand. The higher value (left or right) was recorded as the grip strength.
Full-length standing anteroposterior and lateral radiographs were obtained at the time of enrollment. Radiographs were analyzed at a central site using validated software (Spineview, ENSAM Laboratory of Biomechanics, Paris, France). 43 Standard techniques were used to assess C2-C7 lordosis, T1 slope, C2-C7 sagittal vertical axis (SVA), T4-T12 thoracic kyphosis (TK), C2-S1 SVA, C7-S1 SVA, pelvic incidence to lumbar lordosis mismatch (PI-LL), T1-pelvic angle, and pelvic tilt (PT).
Data Assessment and Statistical Analysis
Statistical analysis was performed using IBM SPSS (version 28.0). Descriptive statistics were reported using means and standard deviations (SD) for continuous variables and frequencies with percentages for categorical variables. Categorical variables were compared using the Pearson’s chi-squared test. Continuous data were assessed for normality using the Shapiro-Wilk test. Statistical comparisons of continuous data were performed using either Student’s t test for data with normal distribution or the Mann-Whitney U test for data without normal distribution. Factors that independently distinguished between ACD and ATLD patients were assessed with multivariate logistic regression analysis using the factors with a P ≤ .1 on univariate comparisons between the 2 patient groups. Correlations between VR-12 PCS and frailty measures were assessed using the Pearson correlation coefficient. All tests were two-tailed, with a significance level of P-value <.05.
Results
Patient Population
Baseline Demographics, Diagnosis, Radiographic Parameters, and History of Previous Surgery for 107 Adult Cervical Deformity Patients. a
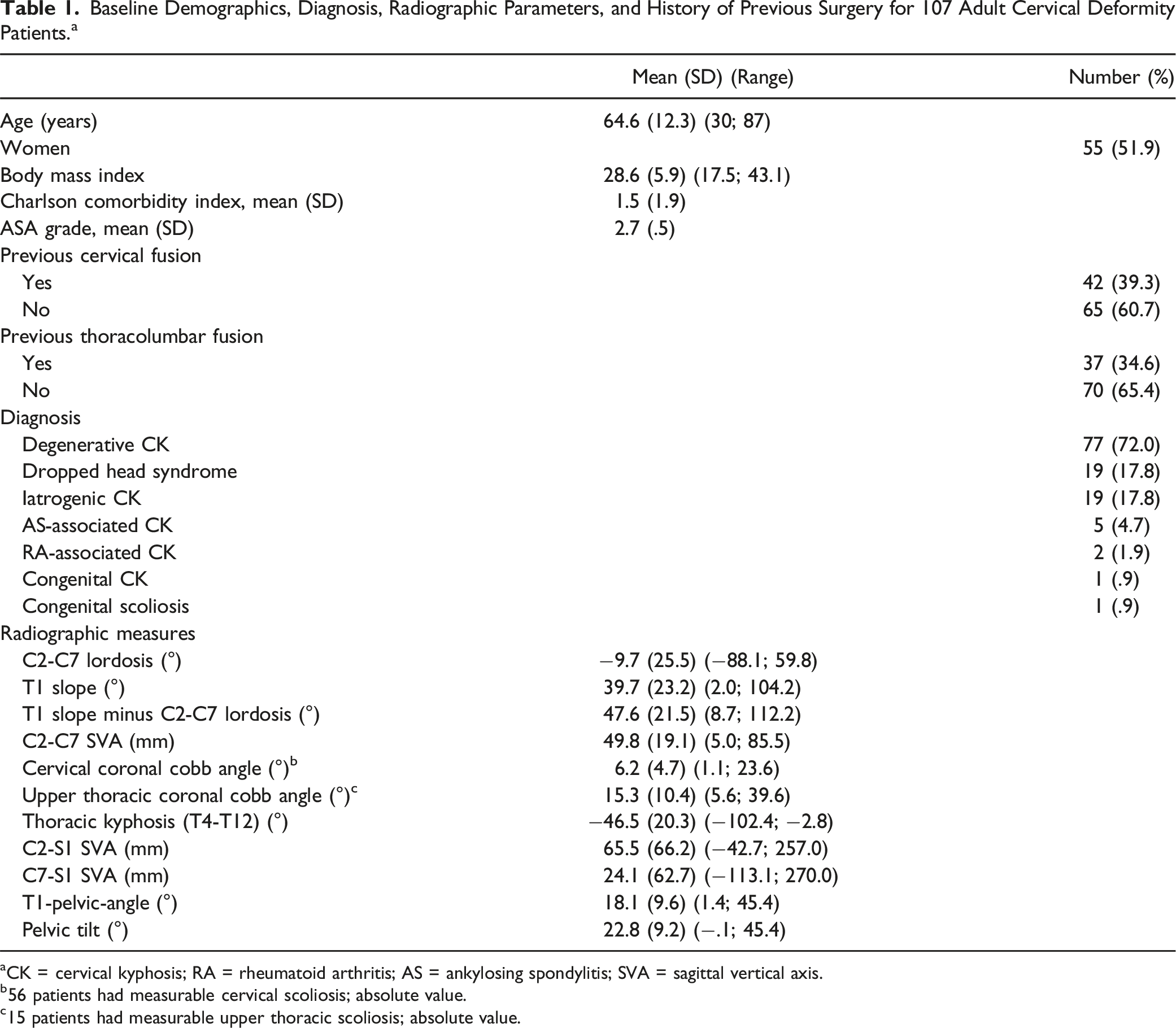
aCK = cervical kyphosis; RA = rheumatoid arthritis; AS = ankylosing spondylitis; SVA = sagittal vertical axis.
b56 patients had measurable cervical scoliosis; absolute value.
c15 patients had measurable upper thoracic scoliosis; absolute value.
Baseline Demographics, Radiographic Parameters, and History of Previous Surgery for 509 Adult Thoracolumbar Deformity Patients. a
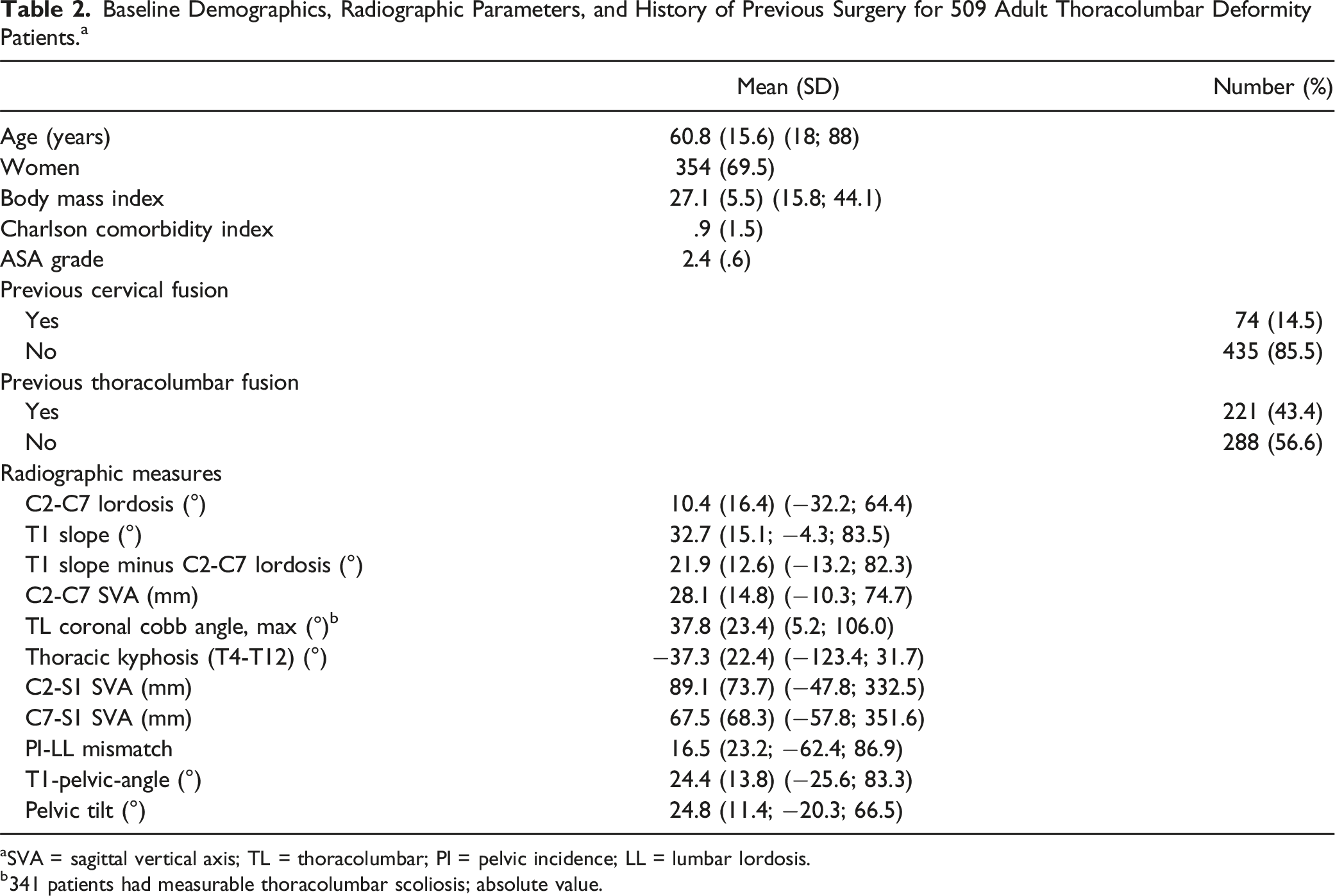
aSVA = sagittal vertical axis; TL = thoracolumbar; PI = pelvic incidence; LL = lumbar lordosis.
b341 patients had measurable thoracolumbar scoliosis; absolute value.
Comparisons of Clinical Parameters and Patient-Reported Outcomes Measures Between Adult Cervical Deformity and Adult Thoracolumbar Deformity Patients
Comparison of Baseline Demographics, Comorbidities, Disability, and Frailty Between Adult Cervical Deformity and Adult Thoracolumbar Deformity Patients. a
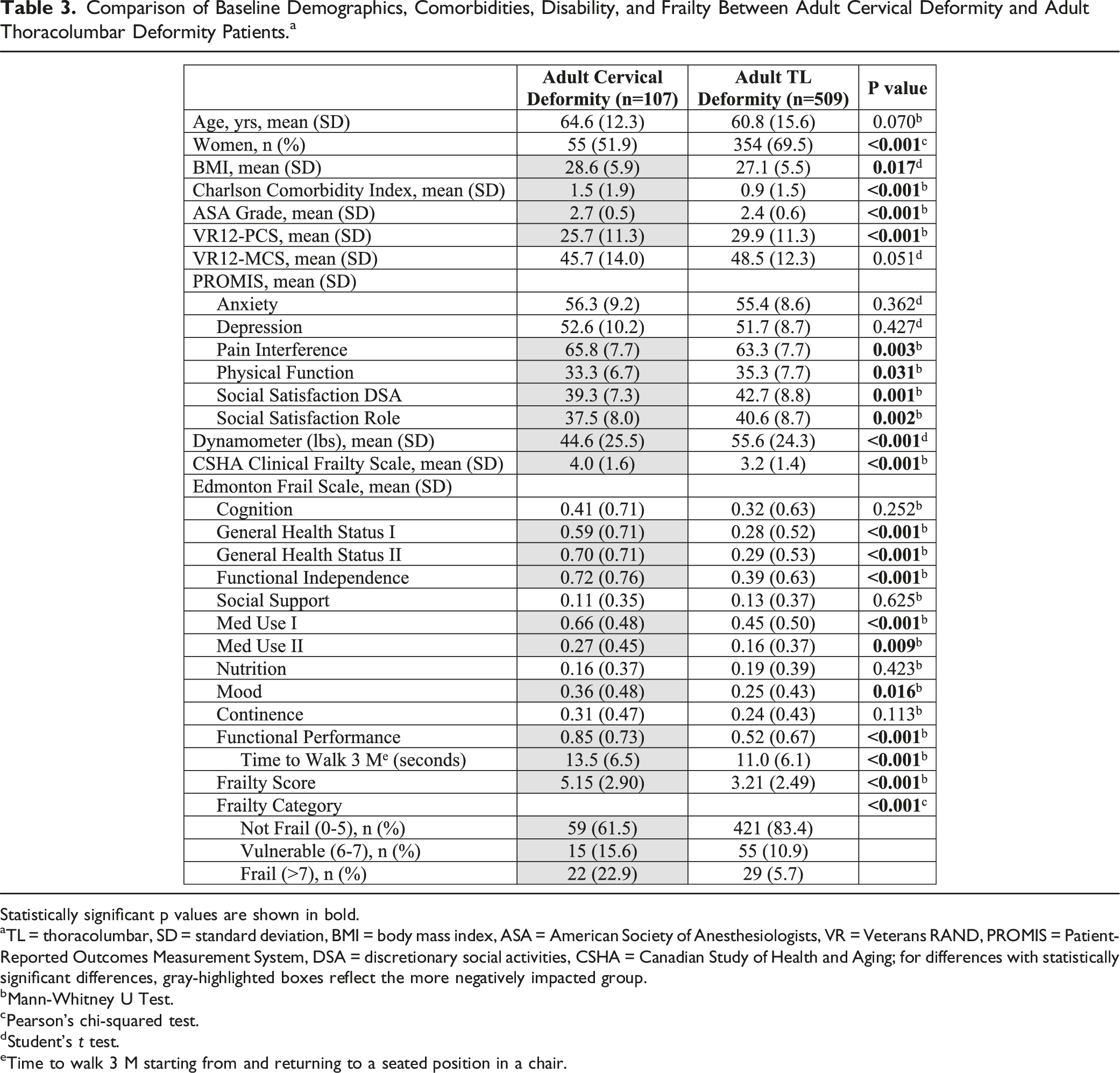
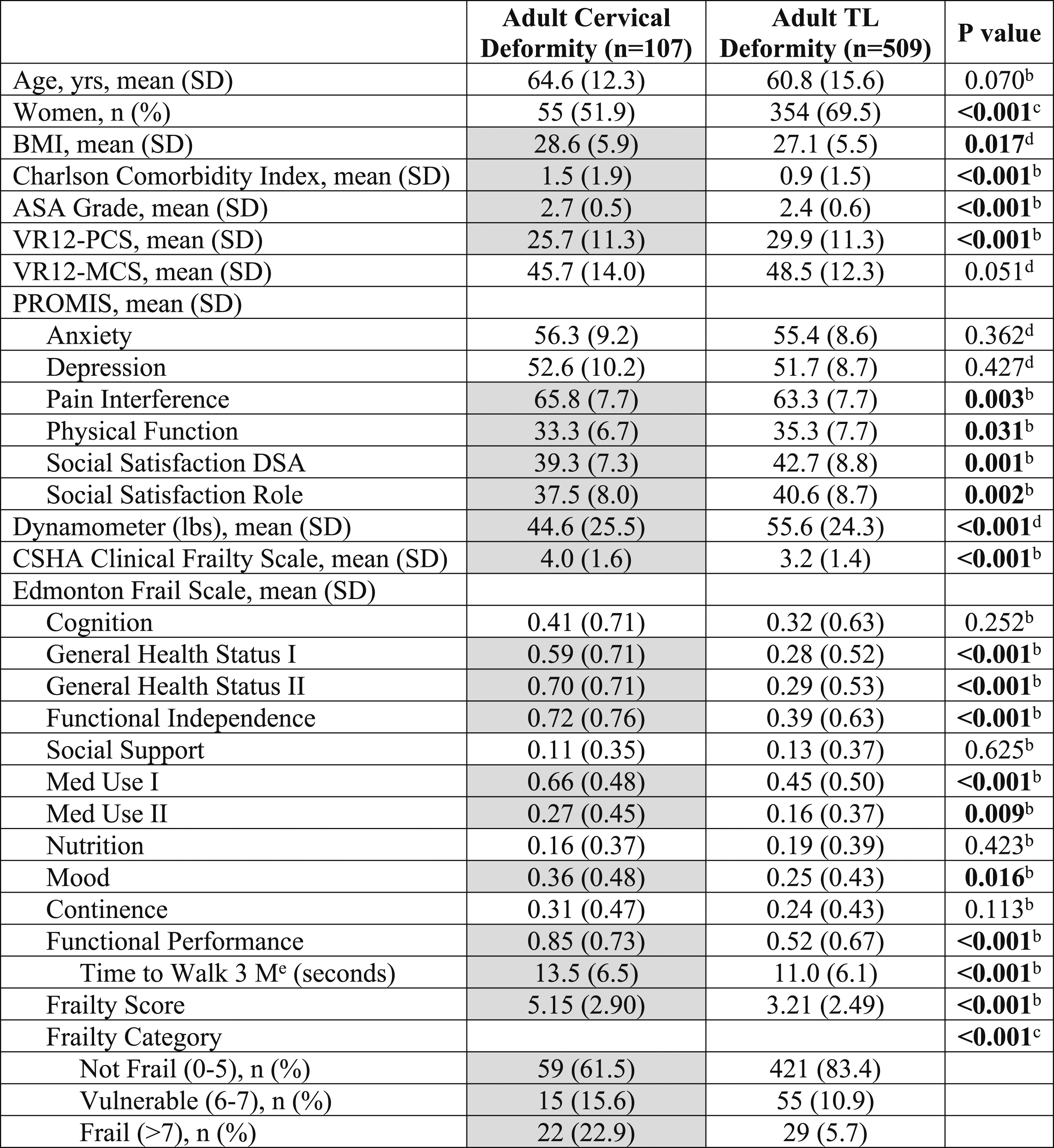
Statistically significant p values are shown in bold.
aTL = thoracolumbar, SD = standard deviation, BMI = body mass index, ASA = American Society of Anesthesiologists, VR = Veterans RAND, PROMIS = Patient-Reported Outcomes Measurement System, DSA = discretionary social activities, CSHA = Canadian Study of Health and Aging; for differences with statistically significant differences, gray-highlighted boxes reflect the more negatively impacted group.
bMann-Whitney U Test.
cPearson’s chi-squared test.
dStudent’s t test.
eTime to walk 3 M starting from and returning to a seated position in a chair.
Comparisons of Frailty Measures Between Adult Cervical Deformity and Adult Thoracolumbar Deformity Patients
Baseline measures of frailty are summarized and compared between ACD and ATLD patients in Table 3. Grip strength, as assessed by a dynamometer, was significantly lower for ACD patients (44.6 lbs vs 55.6 lbs, P < .001). The mean CFS score for ACD patients was 4.0 (SD = 1.6), which corresponds to “vulnerable” and was 3.2 (SD = 1.4) for ATLD patients, which corresponds to “managing well” (P < .001). The overall EFS score was significantly worse for ACD compared with ATLD patients (5.15 vs 3.21, P < .001). For the majority of the individual frailty domains within the EFS, ACD patients score significantly worse than ATLD patients, including General Health Status I and II, Functional Independence, Med Use I and II, Mood, and Functional Performance (Table 3). Compared with ATLD patients, a significantly greater proportion of ACD patients were categorized as vulnerable (15.6% vs 10.9%) or frail (22.9% vs 5.7%) based on the EFS (P < .001). Radiographs of representative ACD and ATLD patients with a range of frailty severities are shown in Figure 1. Postero-anterior (PA, left) and lateral (right) radiographs of representative adult cervical deformity (A-F) and adult thoracolumbar deformity (G-L) patients with a range of frailty severities. A and B: 37-year-old woman with dropped head syndrome and “no frailty” based on Edmonton Frail Scale [EFS] score of 3 and Canadian Study on Health & Aging Clinical Frailty Scale (CFS) score of 3 (“managing well”). C and D: 82-year-old man with degenerative cervical kyphosis and “vulnerable” to frailty based on EFS score of 7 and CFS score of 3 (“managing well”). E and F: 35-year-old man with ankylosing spondylitis and “moderate frailty” based on EFS score of 11 and CFS score of 6 (“moderately frail”). G and H: 64-year-old woman with degenerative thoracolumbar scoliosis and “no frailty” based on EFS score of 3 and CFS score of 3 (“managing well”). I and J: 58-year-old woman degenerative thoracolumbar scoliosis and “vulnerable” to frailty based on EFS score of 6 and CFS score of 3 (“managing well”). K and L: 66-year-old woman with iatrogenic flatback and positive sagittal malalignment and “moderate frailty” based on EFS score of 10 and CFS score of 5 (“mildly frail”).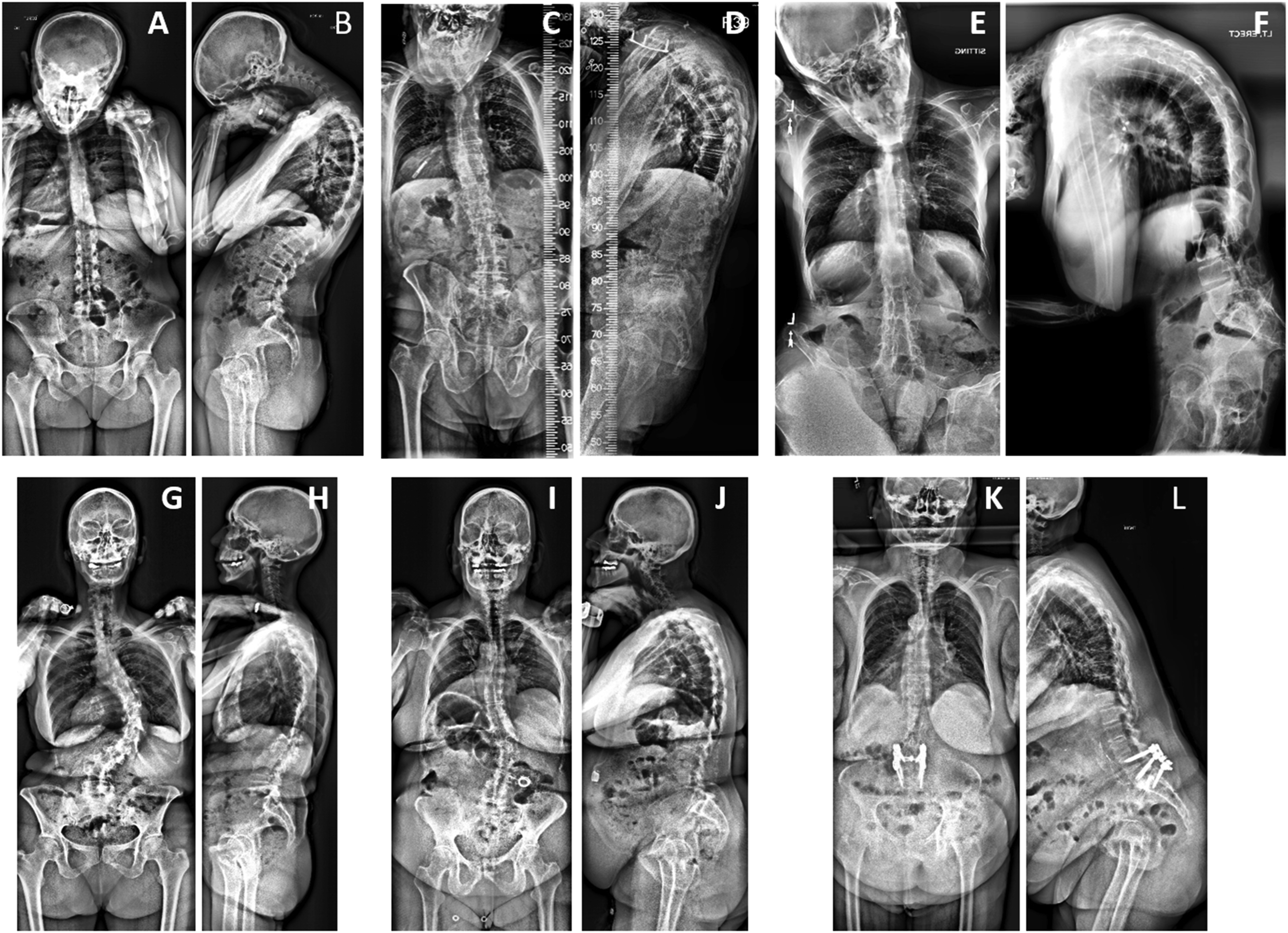
Multivariate Assessment of Factors Distinguishing Between Adult Cervical Deformity and Adult Thoracolumbar Deformity Patients
Multivariate logistic regression analysis was performed in order to assess for baseline factors that independently distinguished between ACD and ATLD patients. Of all baseline factors from univariate analyses with a P < .1 (Table 3), 3 significant factors were identified: increased hand grip strength had an OR of 1.029 (95% CI = 1.017-1.041, P < .001) for ATLD vs ACD, increased EFS had an OR of .811 (95% CI = .744-.885, P < .001) for ATLD vs ACD, and female gender had an OR of 4.094 (95% CI = 2.403-6.974, P < .001) for ATLD vs ACD.
Correlations Between Baseline Disability and Frailty Measures
Correlations Between Frailty Measures and Baseline Disability, Function, Health Status and Age in a Combined Cohort of 616 Adult Cervical and Thoracolumbar Spinal Deformity Patients. a
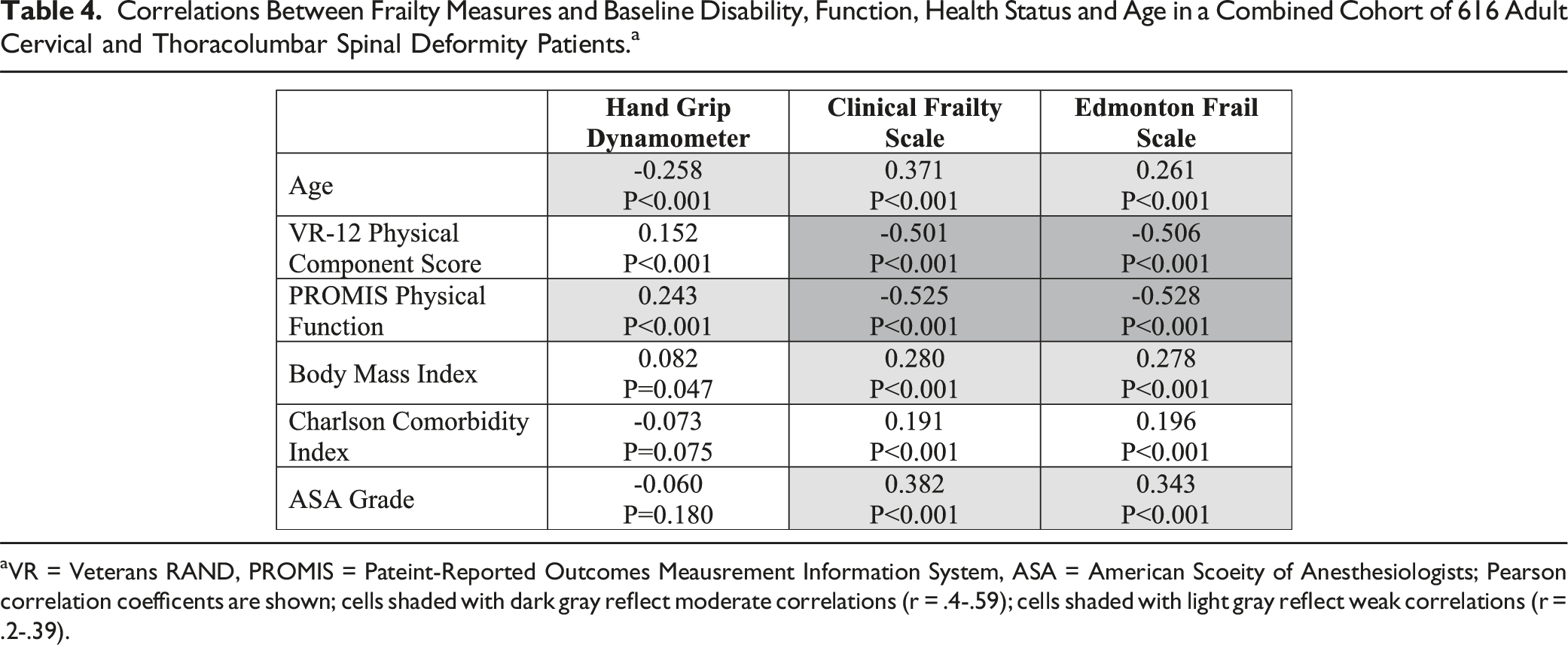
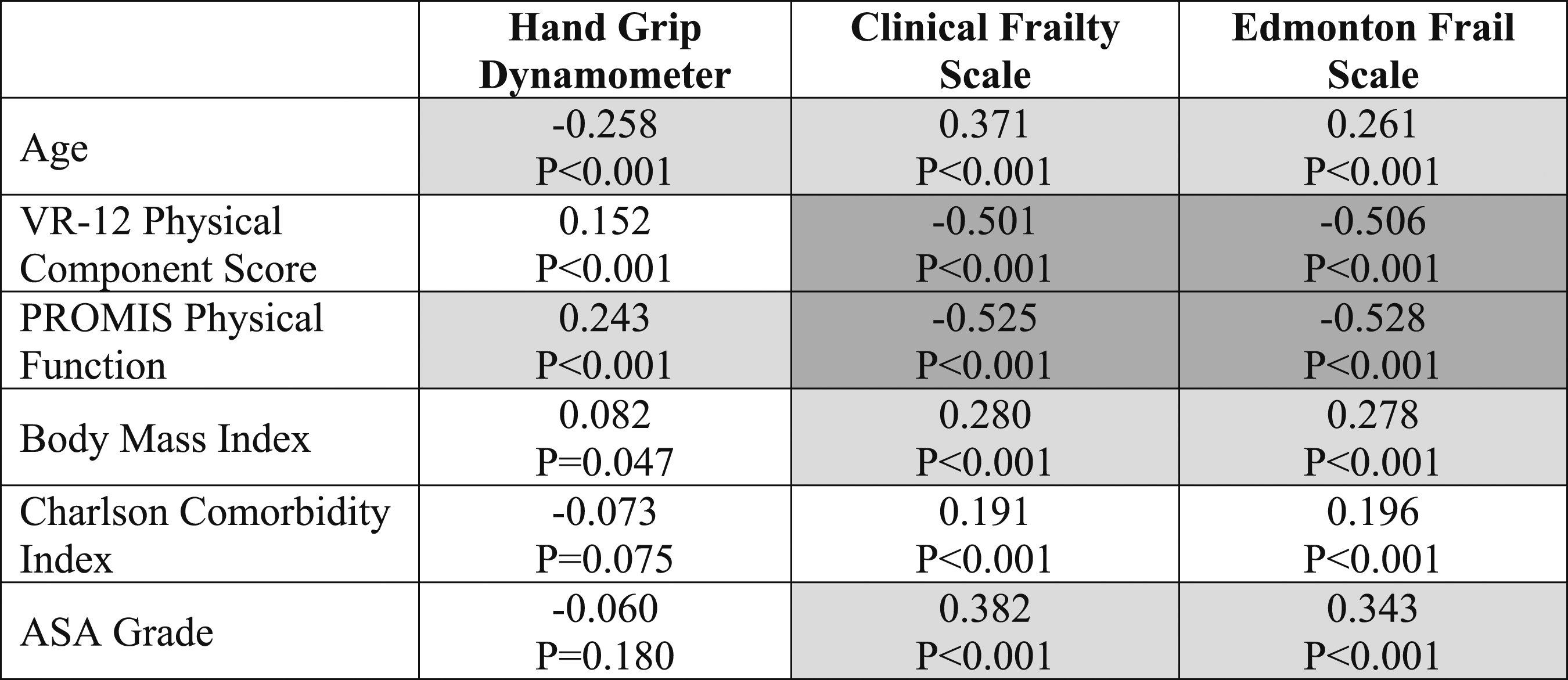
aVR = Veterans RAND, PROMIS = Pateint-Reported Outcomes Meausrement Information System, ASA = American Scoeity of Anesthesiologists; Pearson correlation coefficents are shown; cells shaded with dark gray reflect moderate correlations (r = .4-.59); cells shaded with light gray reflect weak correlations (r = .2-.39).
Discussion
The potential for operative treatment to markedly improve pain, function, and overall health-related quality of life for adults with spinal deformity has been shown through multiple clinical studies.2,15,17-21,23,26,36-38,44,45 However, our understanding of why these deformities develop and progress, as well as how best to treat these patients while minimizing adverse events, remains incomplete.1,7,28,46 Study of ATLD has advanced considerably over recent decades. In contrast, study of ACD has only recently gained traction. Although each of these deformity groups consists of a heterogeneous collection of pathologies, it has become clear that there are key differences between ACD and ATLD. Perhaps most notable, are the higher rates of complications and all-cause mortality following operative treatment observed with ACD compared with ATLD patients.17-19,37,39,40 Although it remains unclear why ACD patients tend to face much greater risk despite surgical treatments employing similar techniques and types of implants, these differences have typically been loosely attributed to baseline poorer health state among ACD patients. The present study used 2 large prospective, multicenter registries of ACD and ATLD patients to provide comparisons of baseline frailty, disability and comorbidities. Based on an overall cohort of 616 patients (107 ACD and 509 ATLD), ACD patients had significantly worse baseline comorbidities, disability and frailty compared with ATLD patients. Collectively, these findings may help account for the greater risk of complications faced by ACD patients with surgery, may provide insights into the etiology of ACD, and may facilitate opportunities to provide better preoperative optimization for ACD patients.
Three separate baseline measures of frailty were used in the present study, hand grip strength, CFS, and EFS. Compared with ATLD patients, ACD patients had significantly worse baseline frailty across all measures. The grip test measures the maximum isometric strength of the hand and forearm and is used as a general indication of muscle functioning status.47-49 The grip test has been shown to be associated with osteoporosis and fracture risk,48,50,51 and low hand grip strength has been associated with adverse outcomes among older adults with gastric cancer. 52 In the present study, ACD patients had 20% lower hand grip strength (44.6 vs 55.6 lbs, P < .001) compared with ATLD patients, despite a markedly lower proportion of women (51.9% vs 69.5%, P < .001) in the ACD group compared with ATLD patients. This suggests that at baseline ACD patients may have lower overall muscle strength and greater risk of bony fracture, both factors that would be expected to increase the risk of mechanical failures following deformity surgery. Notably, it is possible that grip strength could have been negatively impacted in a subset of patients in the ACD group with spinal cord or nerve root compromise. Although we attempted to help mitigate this impact by assessing both left and right hand grip strength and using the higher value, this remains a potential limitation of using hand grip strength assessment in cervical deformity patients.
The CFS is a general measure of frailty status, with a single score ranging from 1 to 9, and is assigned by the healthcare provider. 42 The mean CFS score for ACD patients was almost a full point lower than for ATLD patients (4.0 vs 3.2, P < .001). Although these mean scores correspond to relatively low degrees of frailty (3 = “managing well” and 4 = “vulnerable”), it is important to recognize that the CFS was developed to capture frailty across the range of health conditions, from very fit to terminally ill. Both registries from which patients were drawn for the present study only include patients who were deemed surgical candidates. Therefore, some degree of selection bias is likely present, since surgeons may be less likely to offer major surgery to less healthy patients. Nevertheless, the CFS measure also demonstrates a significantly greater overall degree of baseline frailty among the ACD patients.
The EFS provides assessment of 9 domains and an overall frailty score. 41 The EFS has been applied previously to older patients undergoing orthopedic procedures, and higher scores have been shown to correlate with greater risk of postoperative complications and prolonged hospital stay. 53 In the present study, ACD patients had a 60% higher EFS compared with ATLD patients (5.15 vs 3.21, P < .001). Across the majority of EFS domains, ACD patients had worse scores compared with ATLD patients. The only domains without a significant difference between the 2 groups were Cognition, Social Support, Nutrition, and Continence. Domains with the greatest differences included General Health Status I and II, and Functional Independence. For each of these domains, the scores for ACD patients were approximately twice as high as for ATLD patients. Medication Use I and II, Mood, and Functional Performance domains were also significantly worse for ACD patients. Collectively, assessment based on the EFS demonstrates overall greater frailty in ACD patients and offers insights into the specific domains that may be most impacted.
In addition to greater frailty, ACD patients also demonstrated worse clinical baseline health and function. ACD patients had a modest but significantly higher BMI (28.6 vs 27.1, P < .001) than ATLD patients, but both groups had mean values placing them in the “overweight” category. The CCI and ASA grade were also modestly but significantly worse in the ACD group, suggesting a greater degree of health compromise in ACD patients. Interestingly, all of the patient-reported outcomes measures were significantly worse at baseline for ACD patients, except those related to mental health (VR12-MCS and PROMIS Anxiety and Depression).
The mean age of the ACD patients was modestly but not significantly greater than that of the ATLD patients (64.6 yrs vs 60.8 yrs, P = .070). Notably, the ACD and ATLD groups had similar proportions of patients <40 years of age (6.5% vs 12.6%, P = .095). In order to assess for potential confounding effects of baseline factors on frailty differences between the 2 patient groups, multivariate analyses were performed. When baseline factors from the univariate analysis with a P < .1 were tested in multivariate regression, only 3 remained statistically significant: hand grip strength, EFS, and gender (all P-values <.001). This indicates that, even after adjusting for the differences in gender, both the hand grip strength and EFS remained significantly different between the ACD and ATLD patients.
The strongest correlations between frailty measures and other baseline parameters were between physical function scores (VR-12 PCS and PROMIS Physical Function) and the CFS and EFS scores. These correlations were all only moderate in strength, suggesting that the CFS and EFS assessments capture some information that overlaps with current patient-reported outcome measures while also reflecting unique measures of patient health status. Notably, increasing age correlated with worse frailty measures, but these correlations were weak and not as strong as patient-reported measures of physical function.
Although outcomes and occurrence of complications following adult spinal deformity surgery are complex and multifactorial, the present study may offer some insights. Compared with ATLD patients, ACD patients have worse baseline characteristics on all measures assessed, including greater comorbidities, worse disability, and a greater severity of frailty. Notably, the ATLD registry from which thoracolumbar deformity patients were extracted for the present study was focused specifically on more complex deformities, with inclusion criteria that favored older patients, greater severity of deformity, and more invasive corrective procedures. Thus, the differences in baseline measures between ACD and ATLD patients may be even more marked than those presented.
Strengths of the present study include the relatively large numbers of patients, multicenter design, and prospective patient enrollment. Limitations include the potential for selection bias, since only patients seeking surgery and deemed surgical candidates were enrolled in the patient registries. In addition, both the ACD and ATLD registries include considerable heterogeneity with regard to types of spinal deformities which could impact the results. However, the heterogeneity in each registry is reflective of the spinal pathologies encountered in practice at major centers across the United States and may add to the generalizability of the findings. The lack of specific spine deformity measures of frailty is another limitation of the current study. The available measures of frailty used in this study are relatively blunt and nonspecific. In addition, other factors beyond baseline frailty that were not specifically addressed in the present study may contribute to differences in surgical complication rates between ACD and ATLD patients, including potentially greater need for higher-grade osteotomies and greater challenges with anesthetic management and difficult airways in ACD patients compared with ATLD patients. Lastly, the current study does not include assessments of postoperative complications or outcome, as both registries were relatively recently created. Further maturity of both registries in the years ahead will enable comparisons between frailty and outcomes in these cohorts.
Conclusion
Compared with ATLD patients, ACD patients had worse baseline characteristics on all measures assessed (comorbidities/disability/frailty). These differences may help account for greater risk of complications and all-cause mortality previously observed in ACD patients and facilitate strategies to provide better preoperative optimization. Further analysis may reveal why these populations are so distinct.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Medtronic, Globus, Stryker, SI Bone, and Carlsmed.