
Abstract
Study Design:
Prospective cohort study.
Objectives:
Most studies of dysphagia in the cervical spine have focused on a degenerative patient population; the rate of dysphagia following surgery for cervical deformity (CD) is unknown. This study aims to investigate if surgery for cervical deformity results in postoperative dysphagia.
Methods:
Patients with CD undergoing surgery from 2013 to 2015 were prospectively enrolled to evaluate dysphagia. Demographic, operative, and radiographic variables were analyzed. The Quality of Life in Swallowing Disorders (SWAL-QoL) was used to measure dysphagia. Paired t test, independent t tests, and bivariate Pearson correlations were performed.
Results:
A total of 88 CD patients, aged 61.52 ± 10.52 years, were enrolled. All patients (100%) had 3-month SWAL-QoL for analysis. The baseline preoperative SWAL-QoL was 78.35. This is roughly the same level of dysphagia as an anterior cervical discectomy patient that is 3 weeks removed from surgery. Increasing body mass index (BMI) was correlated with decreased SWAL-QoL score (r = −0.30, P = .001). Age, gender, smoking, and Charlson Comorbidity Index (CCI) showed no significant correlations with preoperative SWAL-QoL. Patients with prior cervical surgery had a lower preoperative SWAL-QoL (P = .04). While 11 patients had acute postoperative dysphagia, CD surgery did not result in lower SWAL-QoL at 3 months (77.26 vs 78.35, P = .53). Surgical variables, including estimated blood loss (EBL), anterior or posterior fusion levels, steroid use, preoperative traction, staged surgery, surgical approach, anterior corpectomy, posterior osteotomy, and UIV (upper instrumented vertebrae) location, showed no impact on postoperative SWAL-QoL. Correction of cervical kyphosis was not correlated to 3-month SWAL-QoL scores or the change in SWAL-QoL scores.
Conclusions:
While patients undergoing surgery for cervical deformity had swallowing dysfunction at baseline, we did not observe a significant decline in SWAL-QoL scores at 3 months. Patients with prior cervical surgery and higher BMI had a lower baseline SWAL-QoL. There were no surgical or radiographic variables correlated to a change in SWAL-QOL score.
Keywords
Introduction
Dysphagia has been widely studied in the cervical spine. One study by Rihn et al 1 showed a 71% rate of dysphagia following anterior cervical procedures at 2 weeks. Others have used indices of dysphagia such as a dysphagia disability index (DDI) or the Bazaz scale to quantify the rate of dysphagia following cervical spine surgery. 2,3 While the findings of these studies is variable, most do find some degree of swallowing dysfunction following anterior cervical procedures in the early postoperative period (<2 weeks) that gradually improves by 3 to 6 months postoperatively. 1,2,4 -9 Existing studies, however, focus on dysphagia in a population consisting predominantly of patients with degenerative cervical disease. To our knowledge, there are no studies that have examined the incidence of dysphagia in a population of patients with cervical deformity. A thorough examination of this subset of patients is important as they often undergo lengthy, multilevel procedures to correct their deformity; factors that may increase the risk of postoperative dysphagia.
A second weakness in the existing literature is that a number of studies use older outcome measures to quantify dysphagia; many of these outcome measures (such as the BZDI) have not been rigorously validated for reproducibility and responsiveness. Recently, investigators begun to utilize the Quality of Life in Swallowing Disorders (SWAL-QoL) score in order to address this weakness. 10 The SWAL-QoL is a validated outcome instrument to quantify dysphagia; it uses 44 questions across 11 domains. This score has been validated in patients with oropharyngeal dysphagia 11,12 and has been previously used in the cervical literature. 10,13 -15 In this study, we sought to describe the incidence of dysphagia in a population of patients with cervical deformity using a validated instrument of dysphagia, SWAL-QoL. We hypothesized that surgery for adult cervical deformity would not result in a substantial decline in postoperative swallowing function in the long term.
Methods
This study was a retrospective review of a prospective multicenter database of cervical deformity patients. Institutional review board approval was obtained at each center prior to patient enrollment. Inclusion criteria for this database were patients >18 years old undergoing cervical spine surgery for cervical deformity. Cervical deformity was defined as having one or more of the following criteria: cervical kyphosis >10°, cervical scoliosis >10°, C2-7 sagittal vertical axis (SVA) >4 cm, or horizontal gaze impairment (chin-brow vertical angle) >25°. Patients included in this study had also completed their preoperative and 3 month postoperative SWAL-QoL questionnaires. Patients with active tumor or infection, acute trauma, pregnant patients and prisoners were excluded from the study. Selected patients were enrolled between January 2013 and October 2015.
Data Collection
Information collected included demographic data, comorbidities, surgical variables, radiographic variables, and outcome measures. Demographic data included age, body mass index (BMI), height, weight and gender. Comorbidities included the patients’ baseline neurologic examination (gait, hand clumsiness, numbness, etc), past medical history, smoking history and calculation of the Charlson Comorbidity Index (CCI). Surgical data collected included a detailed history of prior cervical surgery (presence of prior fusion, fusion type and approach, implants, levels, corpectomy, etc) and relevant intraoperative variables (operating time, estimated blood loss [EBL], approach, levels, osteotomies, levels, steroid use, bone morphogenetic protein [BMP] use, etc).
The following cervical radiographic parameters were measured: cervical SVA (C2-C7 SVA: offset from the C2 plumb line and the posterosuperior corner of C7), C2-C7 lordosis (C2-C7: Cobb angle between C2 inferior endplate and C7 inferior endplate), C0-C2 lordosis (angle between the inferior endplate of C2 and McRae’s line), and mismatch between T1 slope and C2-C7 angle (TS-CL). Horizontal gaze parameters were also measured including the chin-brow vertical angle (CBVA, the angle subtended between a line between the brow to the chin and a vertical line), McGregor slope (McGS, angle between the line from the posterosuperior aspect of the hard palate to the caudal aspect of the opisthion [McGregor’s line] and the horizontal) and the slope line of sight (SLS, angle between Frankfurt line and the horizontal).
Finally, health-related quality of life (HRQOL) outcome measures were also collected. These included the Euro-QoL 5 (EQ-5D), the SWAL-QoL, the modified Japanese Orthopedic Association score (mJOA), and the Neck Disability Index (NDI). The SWAL-QoL is an outcomes tool that was initially conceived as a construct for use in otolaryngological patients with dysphagia. 12 It consists of 44 questions in 11 domains, including food selection, burden, physical health, mental health, social functioning, fear, eating duration, eating desire, communication, sleep, and fatigue. The questionnaire produces scores in each of the individual domains as well as a total score ranging from 0 to 100 with a score of 100 representing no impairment. The SWAL-QoL has been previously validated 11,12 and has been applied to the cervical spine patients in the past. 10
Statistical Analysis
The differences between SWAL-QoL and other continuous variables were compared using an independent Student’s t test. In cases where there were more than 2 categories (eg, surgical approach), a 1-way analysis of variance was used to determine significance. In cases where the variables were ordinal (eg, upper instrumented vertebrae [UIV]), a Kruskal-Wallis test was used to determine significance. Categorical variables were compared using the chi-square or Fisher exact test as appropriate; the P value derived from the Fisher exact test, which was used when cells had an expected count of less than 5. A bivariate, Pearson correlation was performed to find any significant relationships between SWAL-QoL and radiographic variables, HRQOL and continuous demographic and surgical variables (such as operating time, EBL, etc). The level of significance was set at P < .05 for all tests.
Results
Patient Demographics
A total of 88 patients were enrolled for analysis using the inclusion criteria detailed above. The average age was 61.52 ± 10.52 years (range 30-83 years) with 33 (38.4%) males and 53 (61.6%) females. The average BMI was 29.7 kg/m2 (range 16.8-57.8 years). There were 45 primary (52.3%) operations; 41 patients (47.7%) had had prior surgery on their cervical spine. All patients (100%) had 3-month SWAL-QoL and 45 (51.1%) had 1-year SWAL-QoL for analysis.
Baseline Swallowing Dysfunction
The baseline total SWAL-QoL score was 78.35 ± 17.53 (range 22.6-100) (Table 1) with the lowest average scores in the sleep (44.8 ± 32.3) and fatigue (45.3 ± 27.9) domains. At baseline, swallowing dysfunction was strongly correlated to global measures of disability such as NDI (R = −0.492, P < .001) and EQ5D (R = −0.540, P < .001) (Table 2). Among the various demographic variables examined, there were no differences between SWAL-QoL scores with gender (P = .231) (Table 3); however, preoperative BMI was significantly correlated to increased baseline swallowing dysfunction (R = −0.301, P = .001). Patients who had had prior cervical surgery had a lower baseline SWAL-QoL score (74.3 vs 82.0, P = 0.043) (Table 3). There were only 8 smokers included in this cohort and there were no differences in SWAL-QoL in smokers (77.9 vs 82.0, P = .539).
Swallowing Outcomes and Outcomes of HRQOL for Patients Undergoing Surgery for Cervical Deformity.
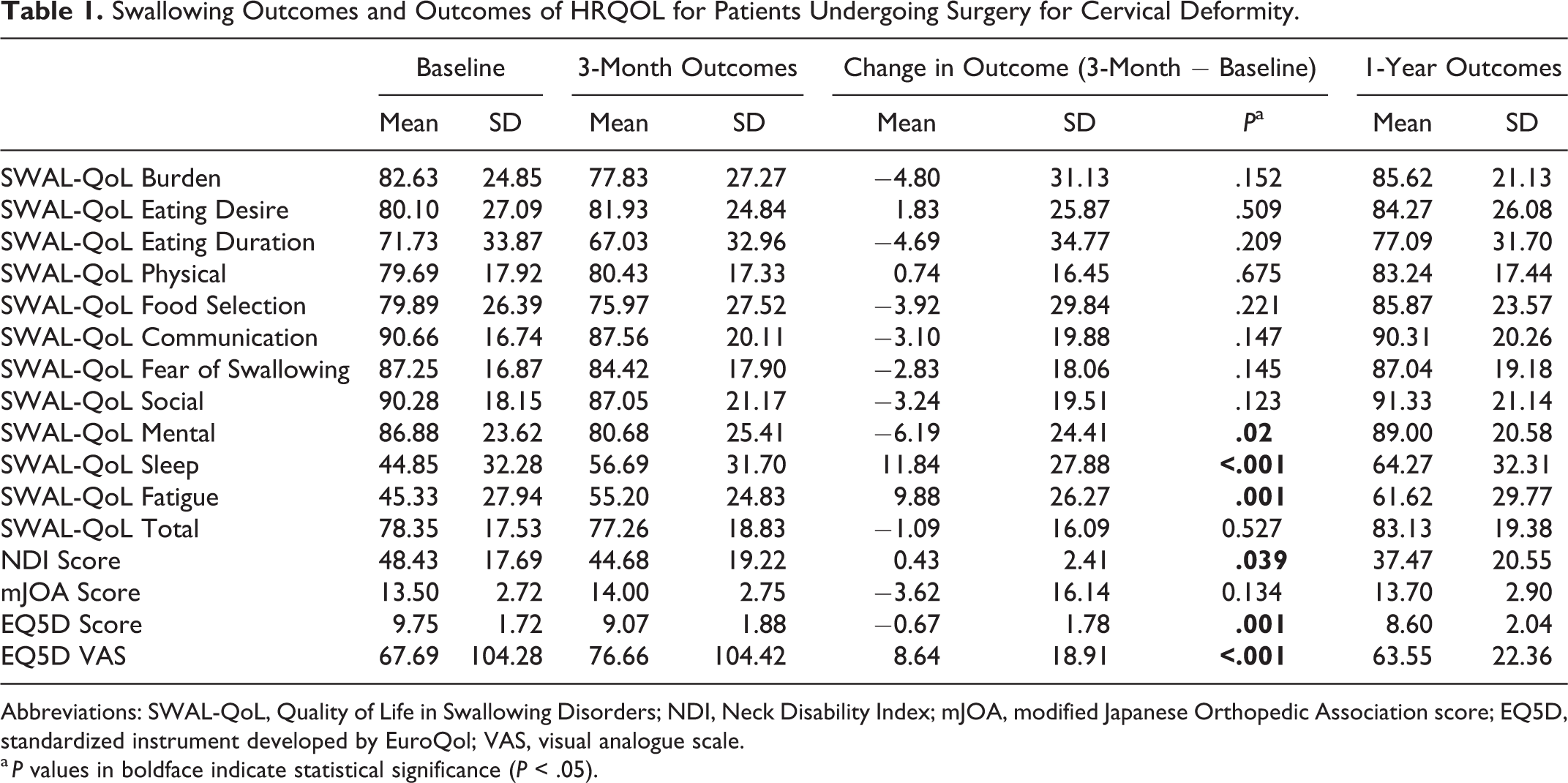
Abbreviations: SWAL-QoL, Quality of Life in Swallowing Disorders; NDI, Neck Disability Index; mJOA, modified Japanese Orthopedic Association score; EQ5D, standardized instrument developed by EuroQol; VAS, visual analogue scale.
a P values in boldface indicate statistical significance (P < .05).
Swallowing Dysfunction Is Correlated to Global Measures of Disability (EQ5D, mJOA, and NDI) in Patients Undergoing Surgery Cervical Deformity at Baseline and at 3 Months.
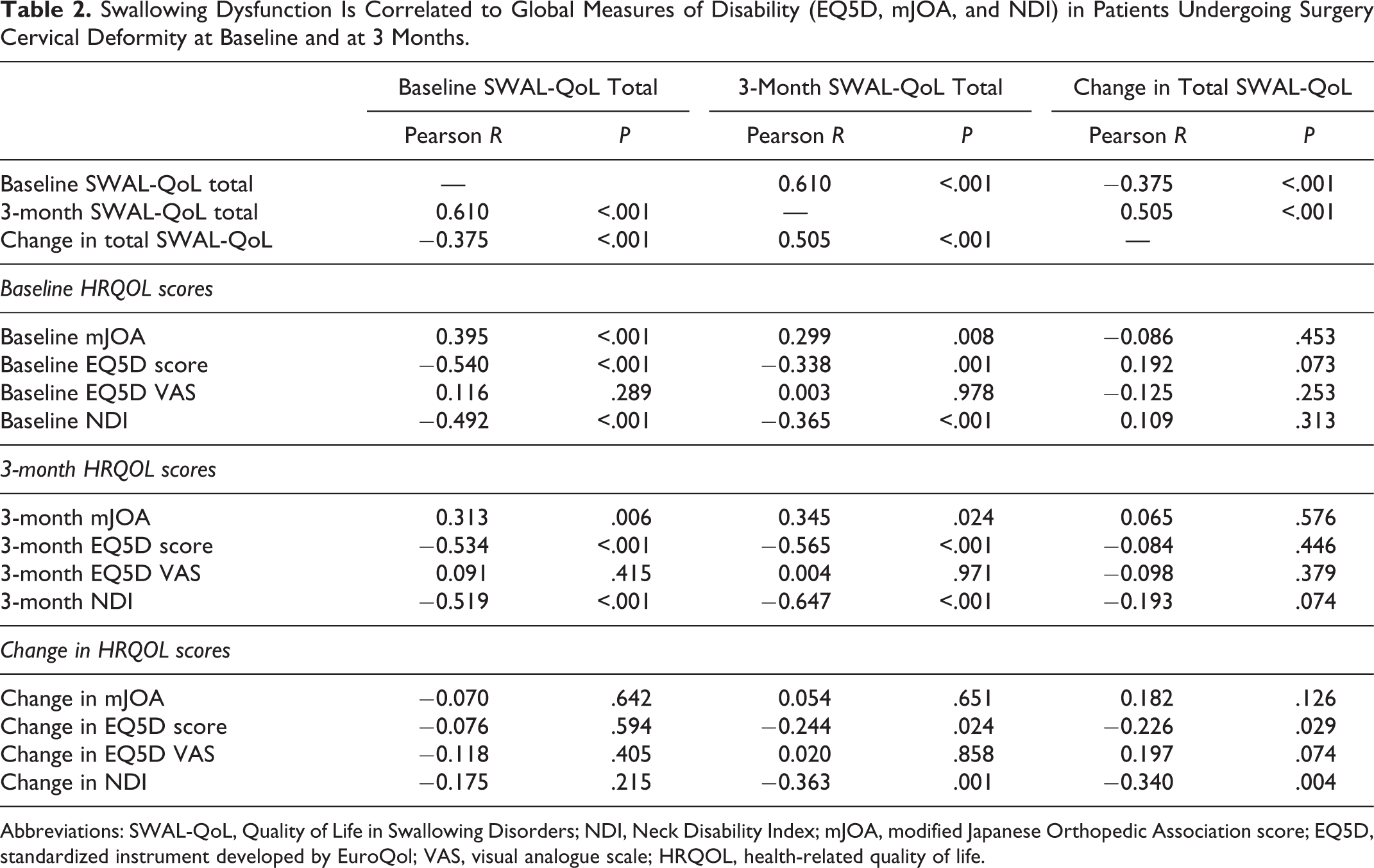
Abbreviations: SWAL-QoL, Quality of Life in Swallowing Disorders; NDI, Neck Disability Index; mJOA, modified Japanese Orthopedic Association score; EQ5D, standardized instrument developed by EuroQol; VAS, visual analogue scale; HRQOL, health-related quality of life.
Impact of Demographic Variables on Baseline and 3-Month SWAL-QoL Outcomes.a
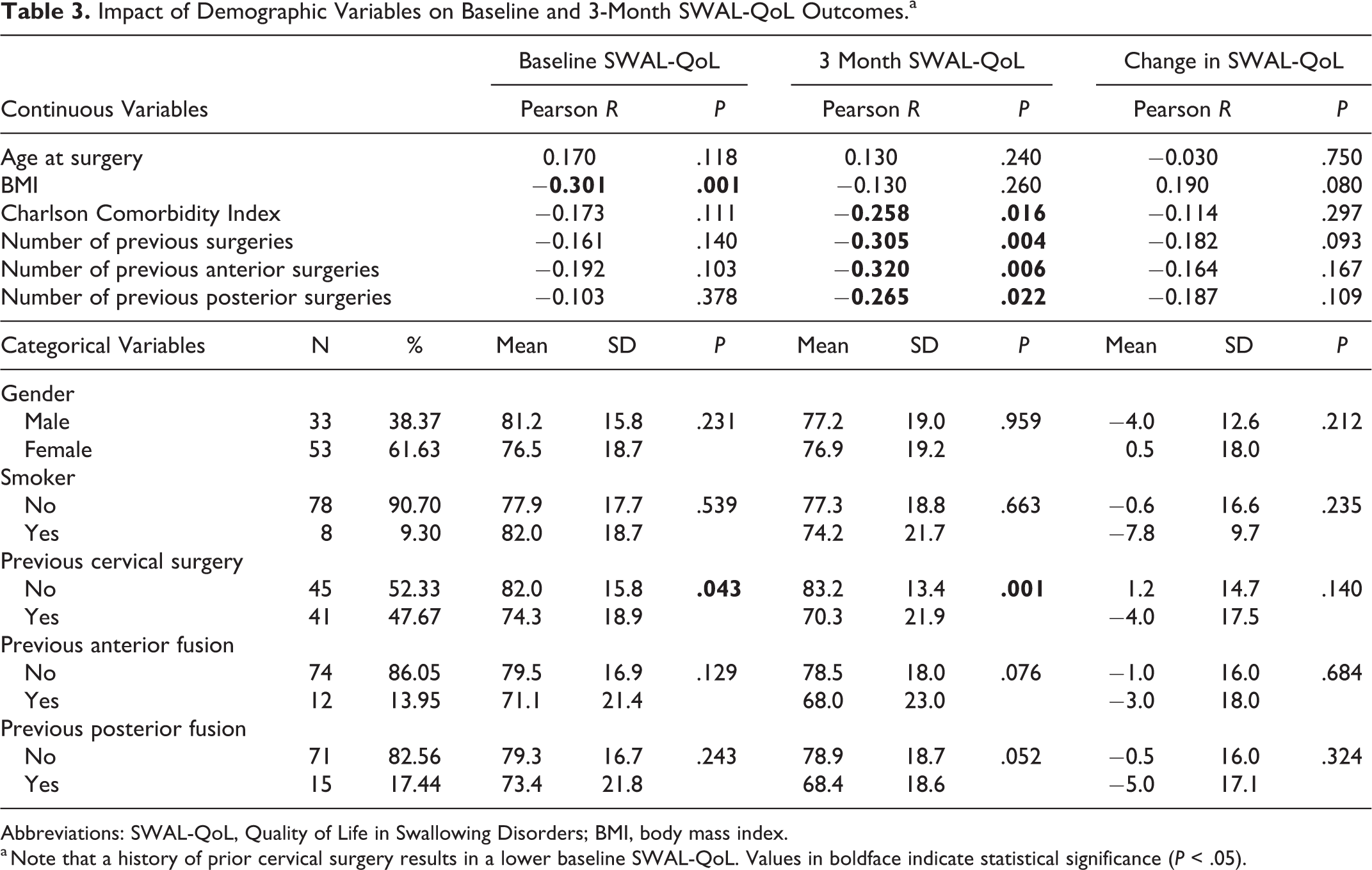
Abbreviations: SWAL-QoL, Quality of Life in Swallowing Disorders; BMI, body mass index.
a Note that a history of prior cervical surgery results in a lower baseline SWAL-QoL. Values in boldface indicate statistical significance (P < .05).
There were weak radiographic correlations between individual domains of SWAL-QoL but there were no significant relationships between any radiographic measure and total baseline SWAL-QoL score (Table 4). There was no difference in SWAL-QoL scores in patients with and without cervical kyphosis (C2-C7 angle < −10°, Figure 1).
Correlation Between Baseline Cervical Alignment and Baseline SWAL-QoL Scores.a
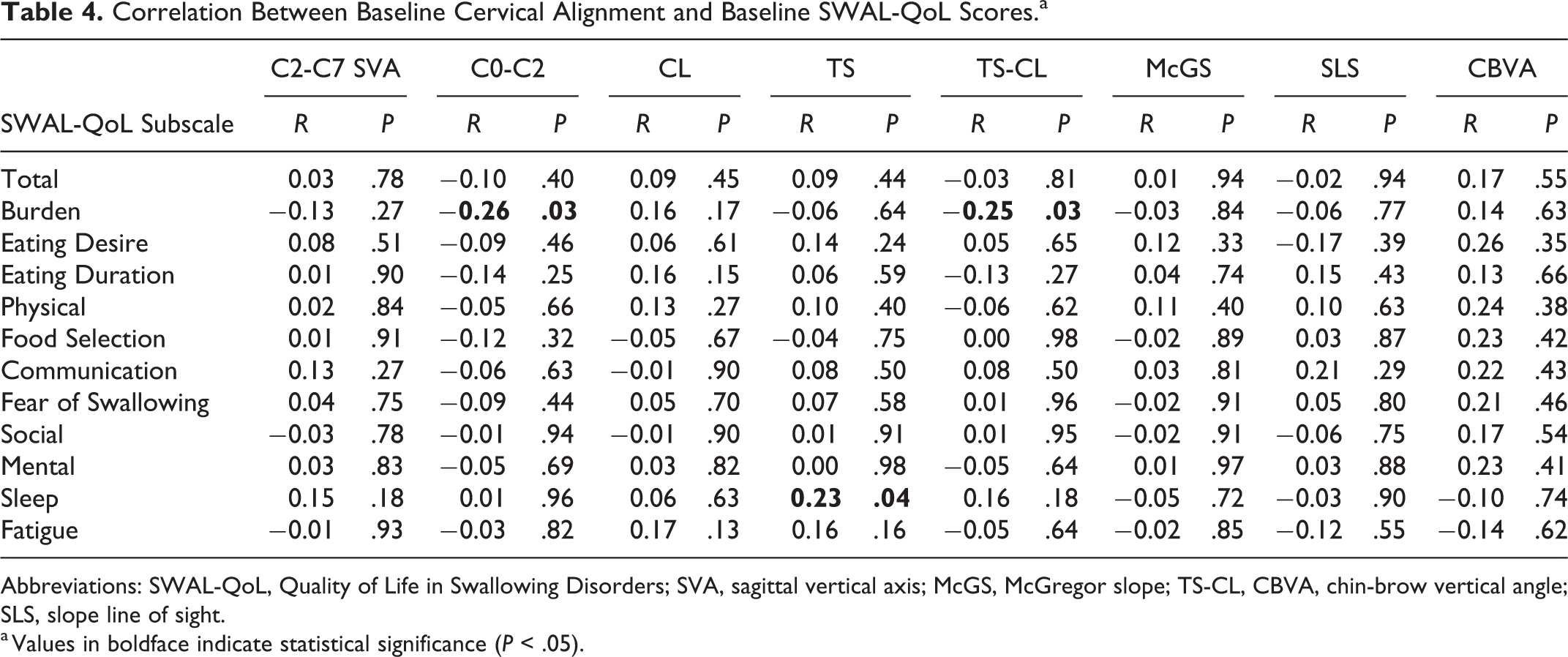
Abbreviations: SWAL-QoL, Quality of Life in Swallowing Disorders; SVA, sagittal vertical axis; McGS, McGregor slope; TS-CL, CBVA, chin-brow vertical angle; SLS, slope line of sight.
a Values in boldface indicate statistical significance (P < .05).
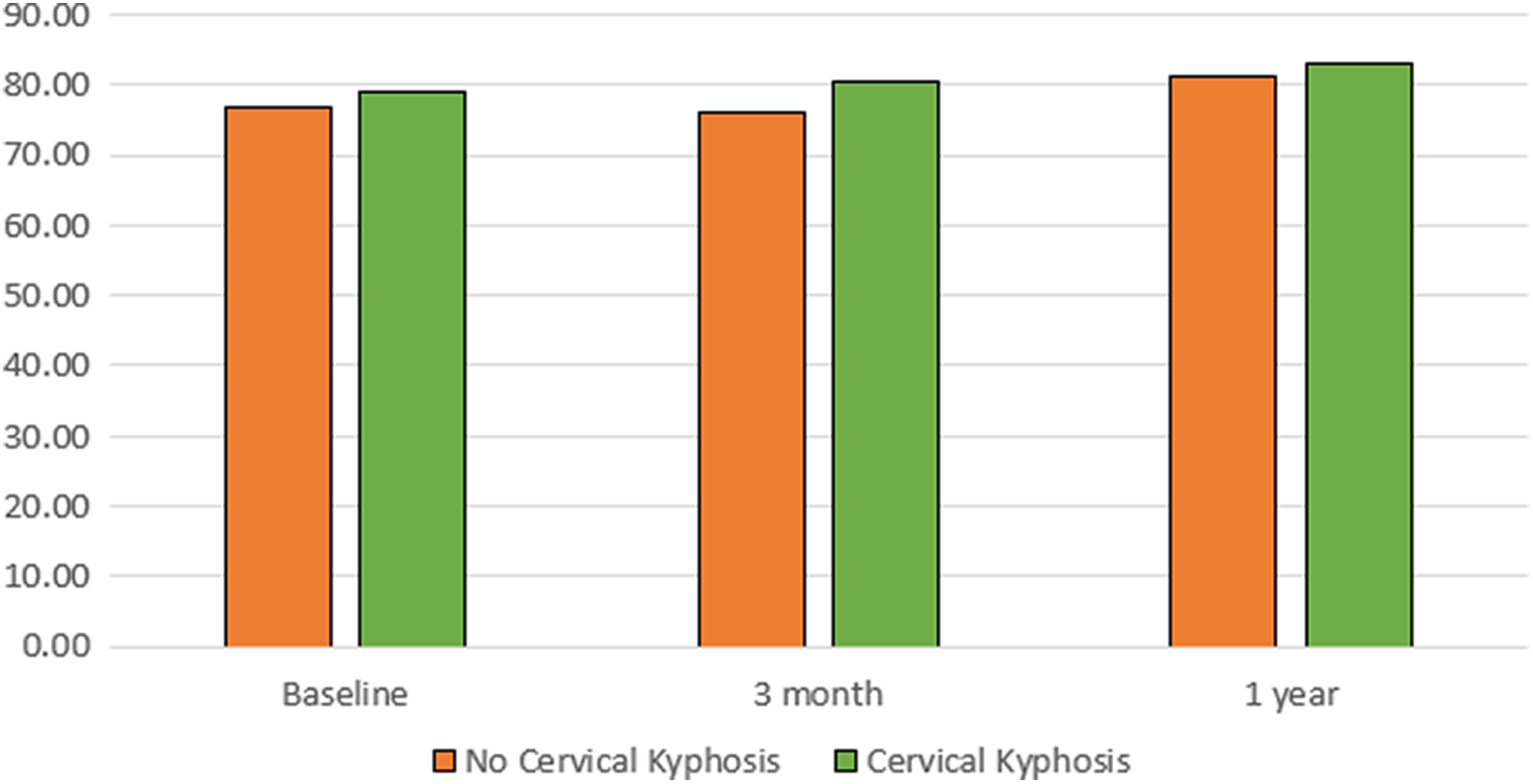
There were no differences in total Quality of Life in Swallowing Disorders (SWAL-QoL) scores in patients with and without cervical kyphosis.
Postoperative Swallowing Dysfunction
Cervical deformity surgery had not caused any significant decline in SWAL-QoL at 3-month follow-up (78.35 vs 77.26, P = .527, Table 1). There were 48 patients (54.5%) in whom the SWAL-QoL score increased (ie, improved) postoperatively and another 40 (45.5%) patients in whom SWAL-QoL score decreased. No surgical variables appeared to have a significant impact on SWAL-QoL. There were 11 patients (12.5%) who were noted to have acute postoperative dysphagia following surgery. These patients were treated with observation in all cases; no patients required barium swallowing studies. There were no esophageal perforations noted in this patient cohort.
In terms of demographic variables, 3-month SWAL-QoL had a significant negative correlation with preoperative CCI (R = −0.258, P = .016) and the number of previous cervical surgeries (R = −0.305, P = .004) (Table 3).
The number of levels fused anteriorly averaged 3.8 (range 1-6). The number of levels fused anteriorly were not correlated with 3-month SWAL-QoL score (R = 0.113, P = .466) or change in SWAL-QoL (R = −0.153, P = .322). There was also no correlation between the number of levels fused posteriorly (R = −0.040, P = .738) and 3-month SWAL-QoL scores (Table 5).
The Impact of Surgical Variables on Postoperative SWAL-QoL Scores.a
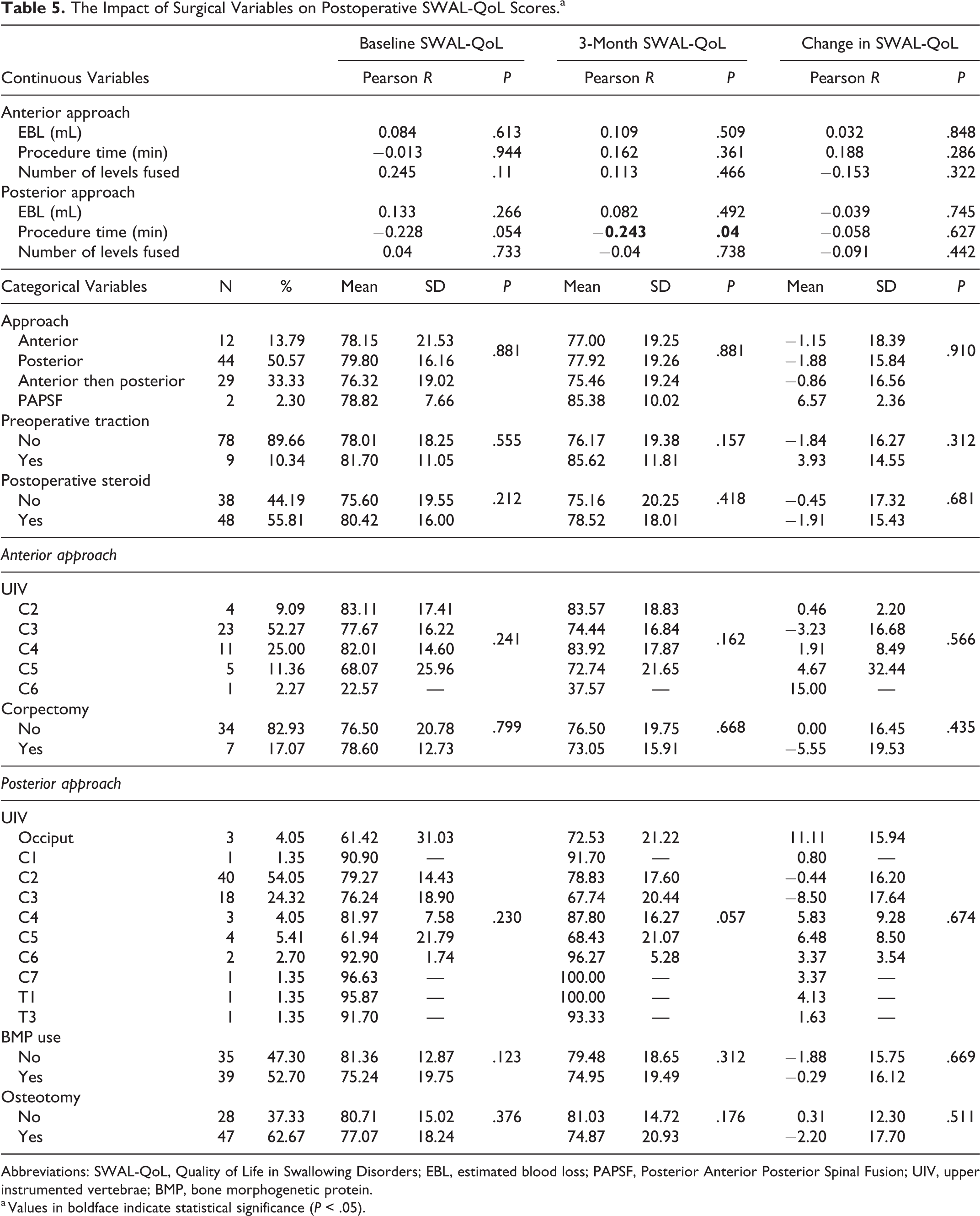
Abbreviations: SWAL-QoL, Quality of Life in Swallowing Disorders; EBL, estimated blood loss; PAPSF, Posterior Anterior Posterior Spinal Fusion; UIV, upper instrumented vertebrae; BMP, bone morphogenetic protein.
a Values in boldface indicate statistical significance (P < .05).
Similarly, there was no difference in mean 3-month SWAL-QoL scores based on anterior (P = .162) or posterior (P = .057) UIV. The surgical approach also had no impact on 3-month SWAL-QoL scores (P = .881). Only posterior procedure time showed correlation to 3-month SWAL-QoL score (R = −0.243, P = .04) (Table 5).
Other variables examined also appeared not to have an impact on swallowing dysfunction. Steroids were used in 48 patients (55.8%) but there was no difference in mean SWAL-QoL scores (P = 0.212). Similarly, posterior BMP use (n = 39, 46.4%) did not affect total SWAL-QoL scores (79.48 vs 74.95, P = .312). There was no BMP used anteriorly. Osteotomy did not have a significant impact on 3-month SWAL-QoL scores (81.03 vs 74.87, P = .176).
Finally, a change in cervical kyphosis was not correlated to 3-month SWAL-QoL scores or the change in SWAL-QoL scores (Figure 2).
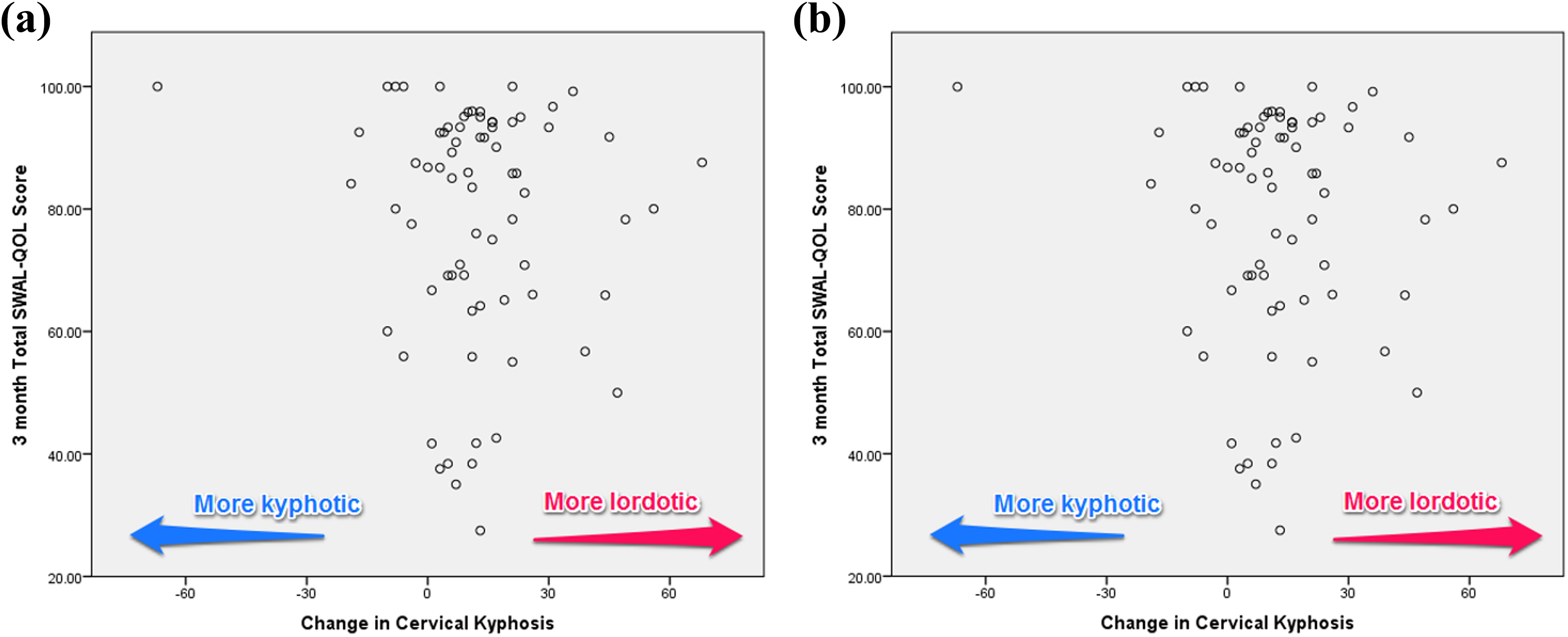
Correction of cervical kyphosis was not correlated to 3-month Quality of Life in Swallowing Disorders (SWAL-QoL) scores (a) or change in SWAL-QOL scores (b).
Discussion
In this study, we show that patients with cervical deformity have a high level of preoperative swallowing dysfunction. However, our results also support that surgery for cervical deformity does not result in a significant worsening of this dysphagia at 3 months postoperatively. Furthermore, we show that swallowing function does not change regardless of a number of surgical variables, including the number of levels fused and approach used. These findings are surprising. The patients in this cohort are undergoing complex, multilevel procedures (average levels fused was 3.8) and conventional wisdom would suggest that these patients would be at high risk for postoperative dysphagia. Several authors, for example, have shown that the incidence of dysphagia increases with multilevel surgery. 2,6,7,16 There are, however, other studies that have not been able to show a significant relationship between dysphagia and multilevel procedures. 1,17
It is important to remember that all the above studies were performed in patients with degenerative pathology. This is important because cervical deformity patients may have some preoperative swallowing dysfunction due to their deformity (eg, chin on chest); the patients in this cohort had a relatively high level of swallowing dysfunction at baseline. For example, the baseline SWAL-QoL of patients in this study (78) was similar to a group of patients with oropharyngeal cancer receiving chemotherapy and radiation. 18 Although the SWAL-QoL is now widely used in cervical surgery, a rigorous psychometric evaluation of this survey in the cervical spine has not been performed. This might mean that in this group of patients with preexisting swallowing dysfunction, the questionnaire has floor effects that make it difficult to detect increased swallowing difficulty.
A final reason for the lack of difference in SWAL-QoL scores might be that the first available time point is 12 weeks postoperatively. Most existing articles on this topic have their first follow-up time point between 1 day and 6 weeks. 1,2,7 These studies show that swallowing dysfunction peaks in the early postoperative period but gradually returns to normal in the ensuing months. It is possible that our cohort experienced a degree of swallowing dysfunction, which then slowly returned to normal by 3 months. The inclusion of an early postoperative timepoint certainly represents an avenue of future investigation. Another important area of future investigation is a closer examination of our patients with acute postoperative dysphagia. These patients were noted by the study investigators to have acute postoperative dysphagia. Unfortunately, our current data set does not allow us to comment on how these patients evolved beyond their acute postoperative course. While we know that no interventions were needed to treat these patients, a closer examination of this cohort is certainly warranted.
These limitations, however, do not diminish our finding that there is no significant dysphagia in this subset of patients in this group of patients at 3 months. At the very least, our results suggest that surgeons discussing cervical deformity surgery with their patients might be able to reasonably state that they can expect their swallowing function to return to baseline within 3 months. Of course, while having this discussion, it is important that surgeons present the findings of this study in a balanced fashion. While the average SWAL-QoL score was unchanged in this patient cohort, a significant number of patients (∼46%) did have a decrease in SWAL-QoL score. All cervical deformity patients must be made aware of this possibility (especially given that we were not able to identify any significant risk factors for changes in SWAL-QoL score). Similarly, while our findings suggest that cervical kyphosis correction did not correlate to changes in SWAL-QoL score, it is important that surgeons continue to counsel patients with severe deformity (eg, chin on chest) and patients with preexisting swallowing difficulties about the risk of postoperative dysphagia.
It is also important, however, to acknowledge this study’s unique strengths. Although the SWAL-QoL has not undergone validation in patients with cervical spine surgery, it is one of the few validated instruments available to detect postoperative dysphagia. Second, this multicenter, prospective study focuses on a patient population in whom a rigorous investigation of dysphagia has not been performed and is frequently believed to be at high risk for cervical dysphagia. The number of patients enrolled in this protocol compares favorably to other studies of cervical dysphagia. These factors make this an important addition to the cervical literature as a launching pad for further discussion and investigation.
In summary, we can show that patients undergoing surgery for cervical dysphagia have a high degree of swallowing dysfunction preoperatively but, equally importantly, show that procedures to address cervical deformity can be safely performed without increasing swallowing dysfunction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted with funding support provided to the International Spine Study Group Foundation (ISSGF) from DePuy Synthes Spine, K2M, NuVasive, Innovasis, Biomet, Orthofix, as well as individual donations.