
Abstract
Study Design
Narrative review.
Objectives
The purpose of this literature review is to evaluate various MIS techniques, assesses their roles in ASD when compared to traditional open surgery, and highlight potential future directions in minimally invasive spine surgery. Correction of spinal malalignment and decompression of neural elements through surgical intervention in adult spinal deformity (ASD) has demonstrated significant improvements in health-related quality of life (HRQOL) metrics. Historically, open surgery has been the primary approach to ensure sufficient decompression and alignment in ASD patients. However, advancements in MIS techniques, equipment, and extensive experience in managing degenerative pathologies have enabled effective corrections using less invasive methods.
Methods
An extensive review of MIS and open techniques for ASD was conducted.
Results
This review evaluates various MIS techniques, assesses their roles in ASD when compared to traditional open surgery, and highlights potential future directions in minimally invasive spine surgery.
Conclusions
The evaluation of various minimally invasive surgery (MIS) techniques in treating adult spinal deformity (ASD) compared to traditional open surgery reveals significant advantages. MIS has progressed from initially treating simple degenerative pathologies to effectively addressing complex ASD cases. This evolution underscores the increasing role of MIS in ASD treatment. Over the past two decades, there has been a noticeable shift towards the mainstream adoption of MIS techniques, reflecting their growing prevalence and acceptance within the medical community. Looking ahead, ongoing advancements and innovations in minimally invasive spine surgery suggest exciting potential future directions for improving outcomes in ASD patients and expanding the application of MIS in spine deformity correction.
Introduction
Optimization of spinopelvic parameters to obtain global alignment in adult spinal deformity (ASD) has been shown to improve health-related-quality-of-life (HRQOL), patient reported outcomes, pain, and disability.1–3 Traditionally, open surgery has been the most common and successful approach for ASD by extensive muscle dissection with ligamentous releases, osteotomies, and neural decompression. 4 However, the invasiveness of this approach carries risk of complications which may be as great as 80%.5–8 In elderly patients, who commonly have significant comorbidities and poor nutrition, complications rates can be higher. 8 Minimally invasive surgery (MIS) for the spine can potentially minimize these complications while still improving HRQOL. The underpinnings of MIS are based on the goal of minimizing tissue disruption by utilizing muscle sparing techniques and technologies while taking advantage of existing anatomical corridors.
Over the past two decades the use of MIS techniques has become more prevalent and mainstream. In 1997 Foley
9
first described the use of microendoscopic discectomy and later the use of tubular retractors for MIS lumbar fusions, ushering the era of advancement of MIS techniques
This review aims to describe the role of various MIS techniques in the treatment of ASD, comparing the results to traditional open approaches and summarizing an algorithmic approach to decision making, while noting key limitations, complications, and future paths.
Role of MIS in ASD
Radiographic Outcomes
Minimally invasive spine surgery can be divided into three categories: direct or indirect decompression, circumferential MIS (cMIS), and hybrid surgery. Hybrid surgery typically includes an MIS anterior reconstruction followed by some form of traditional posterior open techniques, each increasing in invasiveness depending on the severity of the deformity. Radiographically, MIS for ASD has shown to improve global alignment; however, not to the same degree as open surgery as it is limited to less aggressive soft tissue and osseus releases.4,14 Anand et al, 15 in a retrospective review of 90 patients, described a “ceiling effect” of cMIS, with a limit of 61% coronal Cobb angle correction and a maximum sagittal vertical axis (SVA) correction of 89 mm. Patients were successfully able to obtain sagittal correction of pelvic incidence and lumbar lordosis mismatch (PI-LL) within 10o only if the preoperative PI-LL mismatch was 38o or less. Mundis et al 16 noted similar results, with 50% coronal Cobb correction and restoration of sagittal balance in only 9% of patients with severe sagittal plane deformity (SVA >9.5 cm). However, patients with moderate deformities (SVA 4.5-9 cm) did have improvement in their HRQOL at 2 years, even though they did not achieve complete sagittal realignment.
Since the initial use of MIS, several new techniques have been developed to close the gap in deformity correction between open surgery. The anterior column realignment (ACR), was developed to take advantage of an anterior and lateral approach to release the anterior longitudinal ligament, allowing for placement of hyperlordotic interbody cages (typically 20-30°) to correct severe sagittal imbalance, which had been traditionally managed with pedicle subtraction osteotomies (PSO). Mundis et al, compared the ACR to PSO, and found similar radiographic sagittal correction, with lower blood loss (1.6 vs 3.6 liters). 17 Wang et al described the use of a “mini-open” PSO adapting MIS techniques is reducing collateral tissue damage with open technique of 3-column osteotomies for severe deformities. 18 In their series there was similar sagittal deformity correction to reported traditional PSO technique. 19
Patient Reported Outcomes and Complications
Numerous studies have shown the close correlation between restoration of global alignment and improvement in HRQOL metrics in ASD.2,20–23 The ability of MIS techniques to improve radiographic parameters and patient reported outcomes were described in a retrospective study of 184 patients comparing open, MIS, and hybrid surgeries. 24 The MIS group was able to obtain smaller coronal Cobb angles than open (13o vs 20o), with the hybrid group having more correction over MIS (26.6o vs 18.8o). There was a larger change in PI-LL in the hybrid group over open and MIS (20.6o vs 10.2o and 5.5o), but with the open group having greater SVA correction (25 mm vs <1 mm). Interestingly, however, there were no significant differences between the groups with regards to pre- and postoperative Oswestry Disability Index (ODI) and visual analog scores (VAS) at 1 year. This suggests that, although important, obtaining ideal sagittal and coronal alignment goals may not be the only factor in improving patient reported outcomes. Park et al 14 further showed that there was no difference in ODI, VAS, and radiographic outcomes between cMIS and hybrid approaches at 1 year. Later, Park et al 25 assessed patient reported outcomes in 223 aligned and misaligned patients who underwent either cMIS or hybrid surgery. Notably, patients that were misaligned had worse preoperative deformity; however, there was no difference in the proportion of patients reaching minimum clinical important difference (MCID) (52.75% vs 61.1%) and substantial clinical benefit (SCB) (40.5% vs 46.3%) between aligned and misaligned patients. When controlling for surgical and demographic factors, there was no association between reaching optimal alignment goals and obtaining MCID.
MIS techniques may allow for older patients, considered high risk for ASD surgery, to undergo these procedures more safely. In a study assessing the benefit of MIS techniques for patients older than 65 years of age, MCID was achieved for ODI (64.3%) and VAS back (82.9%) and leg (72.2%) scores. 26 Park et al 27 showed that there was no difference in outcomes between postoperatively aligned and misaligned patients older than 65 years, but that younger misaligned patients had worse ODI than young aligned patients. This suggests that alignment goals may be age dependent and that MIS techniques may overcome some of the factors that contribute to lesser patient reported scores.
The surgical management of ASD is associated with a high short and long term complication rate.6,8 Some of these adverse events can be minimized with less invasive surgery. Haque et al 24 reported less blood loss with a reduced need for transfusions. MIS and hybrid surgery had fewer major complications (14%) over open surgery (45%). A retrospective study of 189 patients revealed lower complication rates in MIS (31.7%) over an open approach (60.3%); however, there were higher reoperation rates in the hybrid group (27%) than MIS (11.1%) and open (12%). 28 The most common cause for revision surgery in hybrid and open approaches were neurological deficits and pseudoarthrosis in MIS. In propensity matched analysis, Chou et al 29 found reduced ICU length of stay (LOS) in cMIS (0.6 days) over open (1.2 days), with lower complication rates (29.5% vs 63.6%). There was no difference in hospital LOS (7.9 and 9.6 days) and ODI.
Intuitively, with less invasiveness come fewer complications. ASD patients undergoing surgery may be treated with shorter constructs, reducing operating room time, blood loss, incision size, muscle disruption, hospital length of stay, and postoperative complications. In one study, the cMIS group had a mean of 4.7 levels fused posteriorly over 10.5 levels in the open group. 24 The cMIS and hybrid groups had more interbody fusions over open (4.3 and 4.1 vs 1.9), revealing the power of clinical and radiographic improvement with MIS anterior reconstruction and the reduced need for extensive posterior work in appropriately selected patients. Uribe et al 30 examined a propensity matched cohort of 168 ASD patients, comparing construct length between open and cMIS approaches, and found that cMIS was associated with significantly fewer levels fused (4.8 vs 10.1), without any difference in postoperative ODI and VAS scores at 2 years.
Proximal junctional kyphosis (PJK) is an unfortunate and not uncommon complication of deformity correction with rates from 5% to 46% of cases.31–35 MIS approaches can avoid posterior soft tissue, ligamentous, and osseous disruption which can lead to PJK. In a comparison of lateral lumbar interbody fusions (LLIF) and open posterior surgery only, the LLIF group had significantly lower PJK rates (22.4% vs 38.9%), with lower proximal junctional failure (PJF) (8.6% vs 15.3%). Gandhi et al, 36 described lower PJK rates with the use of LLIF (0%) and ACR (30%) when compared to ACR plus open posterior column osteotomies (PCO) (42.9%). The study revealed open posterior releases, upper-instrumented-vertebra in the lower thoracic spine, severity of preoperative deformity, and degree of sagittal correction as risk factors of PJK and PJF.
Eastlack et al reported late complication and re-operation rates for 133 patients treated with either MIS (n = 68) or hybrid (n = 65) approaches for ASD. The late re-operation rates were similar between the groups (26.5% cMIS vs 27.7% hybrid). They found that junctional failure was the most common cause of re-operation in the hybrid group (13.8%), although rates of both PJF and distal junctional failure (DJF) were statistically similar to the cMIS group. The most common cause of re-operation in the cMIS group was fixation failure of pseudoarthrosis (14.7%). 37
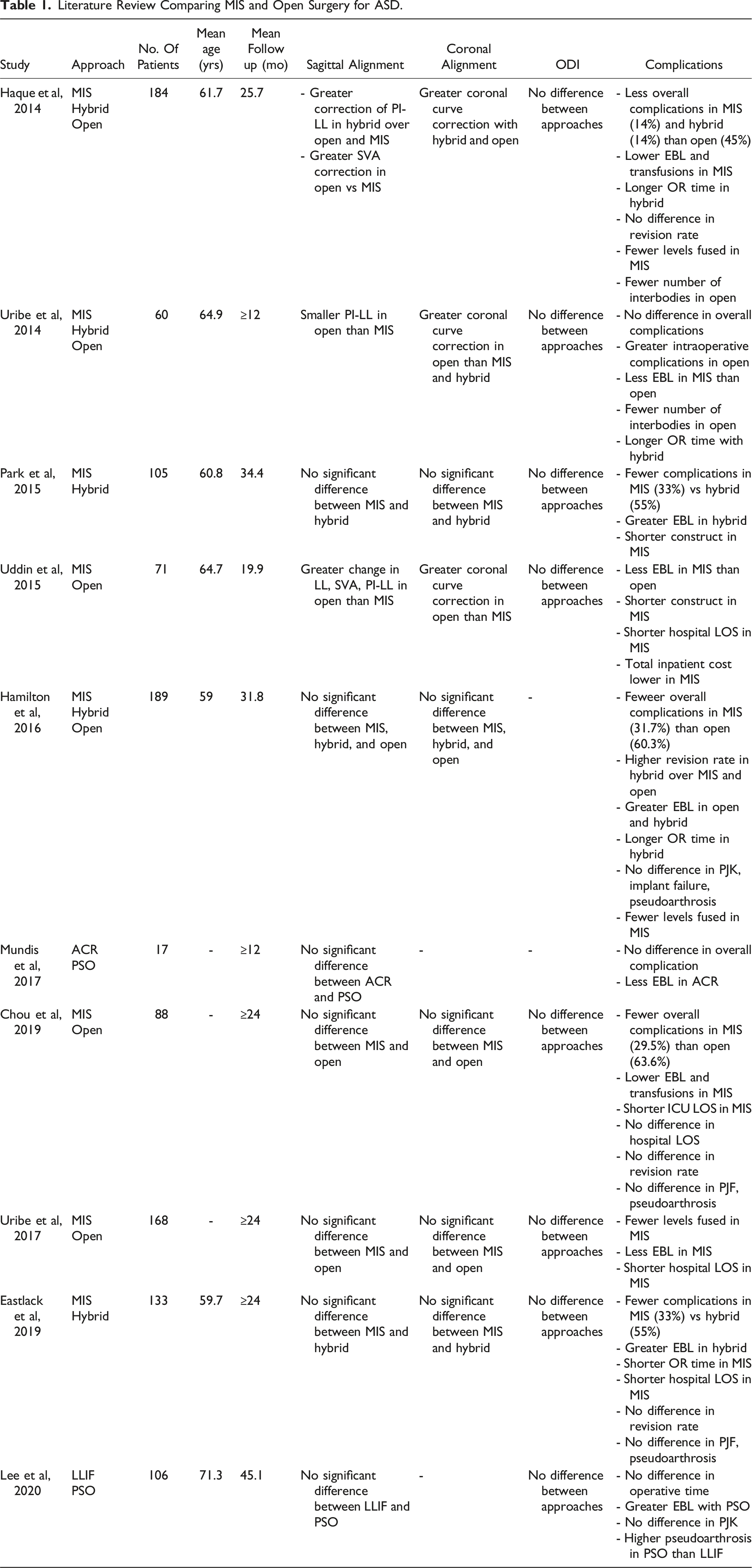
Literature Review Comparing MIS and Open Surgery for ASD.
Cost-Effectiveness of MIS in ASD
With rising health care costs, efficient and cost-effective treatment is vital for the surgical treatment of ASD, a highly resource intensive pathology to manage. Newer technologies, equipment, and implants required for MIS approaches can have higher upfront costs. However, these initial costs can be easily offset by fewer complications, reduced blood loss, reduced need for transfusion, and shorter LOS. Uddin et al 39 reported lower inpatient costs, accounting for complications and revision surgeries, in MIS of US$269,807 compared to US$391,889 in open surgery. The MIS patients had less blood loss, LOS, cardiac services, imaging, surgical cost, pharmacy cost, and nursing costs. There were about 20% reduced costs amounting to approximately US$50,000 in MIS due to operating room time utilization. In another study, MIS had lower costs (US$83,513) than open (US$111,381); however this benefit was lost when there were no complications. 41 The authors concluded that MIS was more cost effective in 57% of cases over open surgery when accounting for risks of complications.
Minimally Invasive Spinal Deformity Surgery Algorithm (MISDEF)
Given the numerous surgical options available for the treatment of adult spinal deformity, there is variability between surgeon decision making. Park et al
42
assessed 268 patients in a prospective nonrandomized study to determine factors impacting decision making for choosing either an open or MIS approach. Younger age, higher VAS back pain score, larger coronal Cobb angle, and larger T1 pelvis angle (TPA) where significant factors for choosing open surgery. As there are numerous variables involved in clinical decision making, in 2014 Mummaneni et al
43
created an algorithm to help surgeons standardize their approach to the management of ASD (Figure 1). The severity of sagittal malalignment based on the SVA is the initial branch point, with curve flexibility and additional spinopelvic parameters categorizing the treatment plan into three classes. Class I is optimal for smaller deformities with flexible curves where complete MIS treatment can be utilized for direct or indirect decompression. Class II is ideal for flexible curves with moderate deformities and stenosis. An MIS approach would be able to achieve decompression along with coronal and sagittal alignment utilizing multiple interbodies. Class III is reserved for severe deformities and/or fixed curves that require open surgery with osteotomies, typically with fusion extending into the thoracic spine. Original MISDEF algorithm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.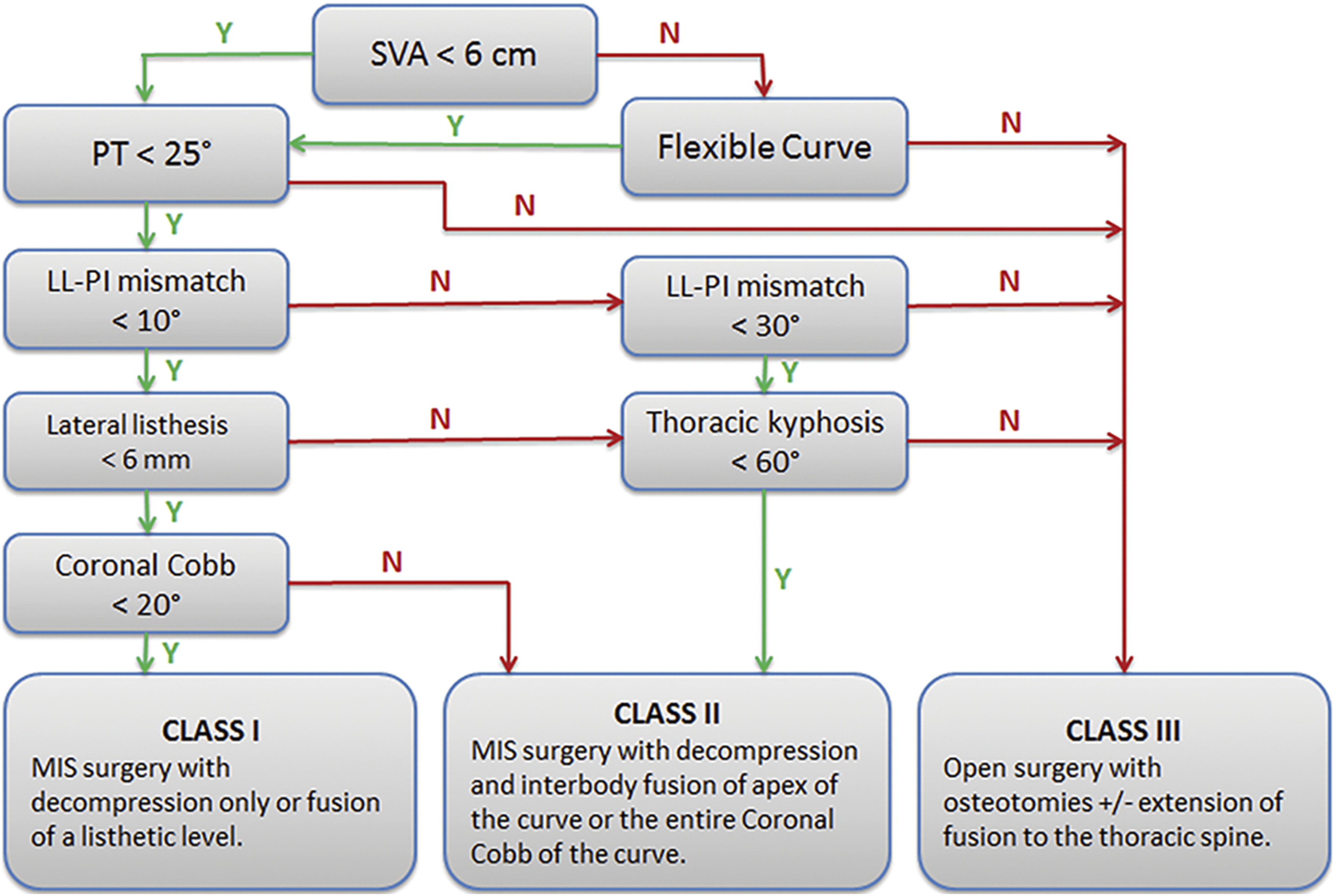
Since then, MIS techniques have evolved with the use of ACR, mini-open PSO, expandable technology, and hybrid approaches allowing for some class III patients to be treated with a MIS approach. The original algorithm was modified, accounting for these advances, creating the MISDEF-2 algorithm (Figure 2).
44
This version starts by assessing if the deformity is fixed or fused, followed by assessing the spinopelvic parameters as before. However, a new branch point looking at the number of levels to be fused and presence of previous instrumentation has been included. Altogether, the previous three classes have been expanded to four classes, further parsing out those complex deformities that can be treated with a MIS or hybrid approaches. MISDEF-2 algorithm. Used with permission from Journal of Neurosurgery.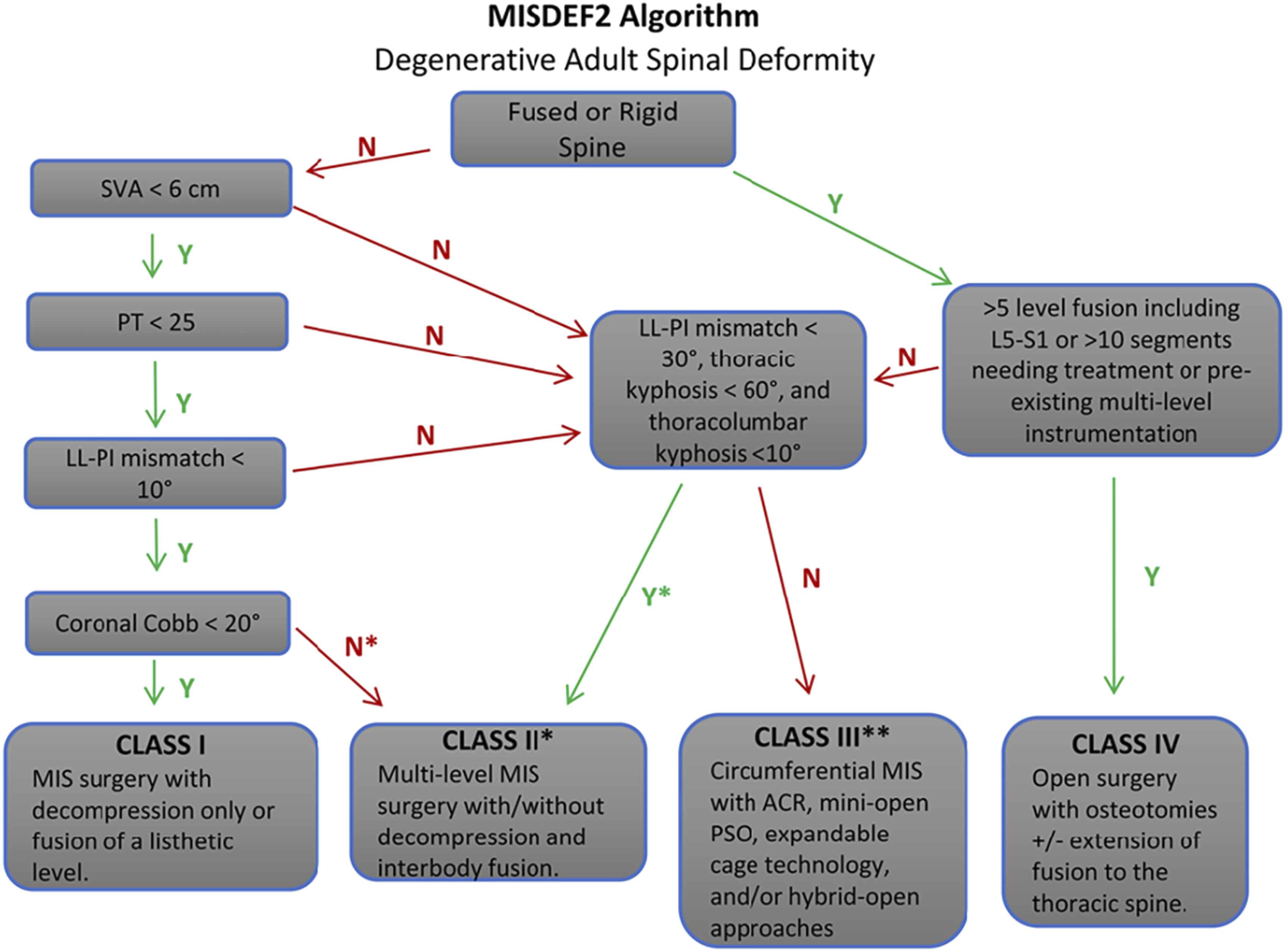
Figure 3 demonstrates a class III patient with a severe spinal deformity that was treated a cMIS approach utilizing multiple techniques to achieve successful restoration of spinal alignment. The patient underwent a L5-S1 ALIF followed by a multilevel LLIF with an addition of a ACR. Case example of circumferential MIS surgery for ASD. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.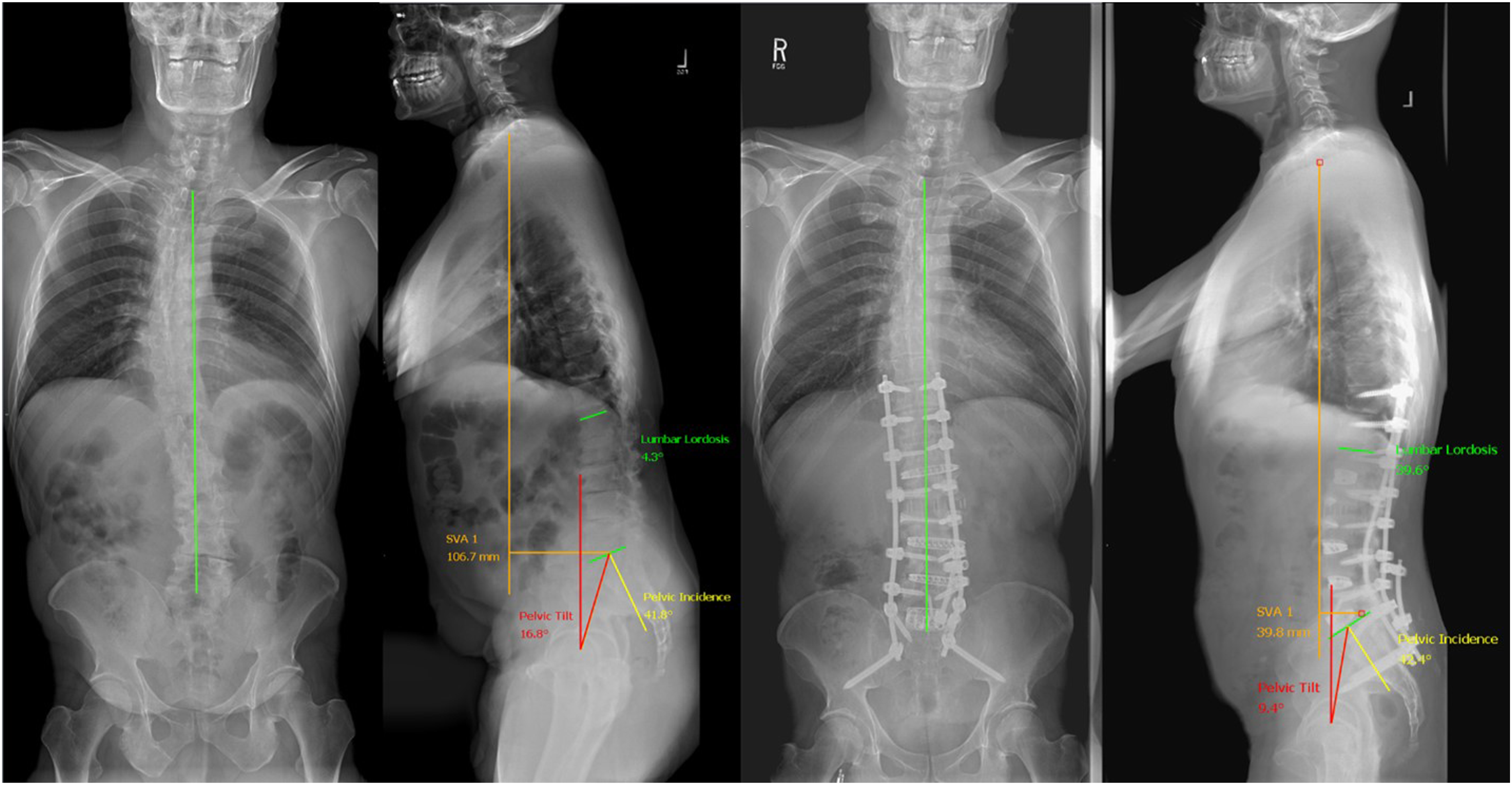
Limitations of MIS for Deformity
Besides severe fixed deformities and inability to achieve as robust radiographic correction as open techniques, there are other limitations to the application of MIS in adult spinal deformity. The steep learning curve involved with MIS techniques can present a challenge to adoption. These approaches often involve utilization of nontraditional surgical corridors with reduced visualization, forcing surgeons out of their comfort zone. Technology plays a large role in MIS procedures with the use of navigated instruments, modified fluoroscopy machines, surgeon controlled neuromonitoring, complex instrumentation, and microscopes. With multiple variables, failure of any one can lead to delays or complications and abandoning of MIS techniques. Wang et al 45 analyzed a large multicenter database of MIS patients over an 8-year period and found as surgeon experience increased there was a 47% reduction in operative time and minor complication rates reduced. There were increasing utilization of lateral and ACR techniques over time.
Current Techniques
The disc space can be approached multiple approaches for interbody fusion: anterior, lateral transpsoas, lateral prepsoas, and the traditional transforaminal trajectory. Each carry their own risks and benefits. Anterior and lateral approaches allow for placement of significantly larger interbody implants, achieving greater disc space height restoration and indirect decompression while reducing the risk of pseudarthrosis. 46
Anterior and Lateral Approaches
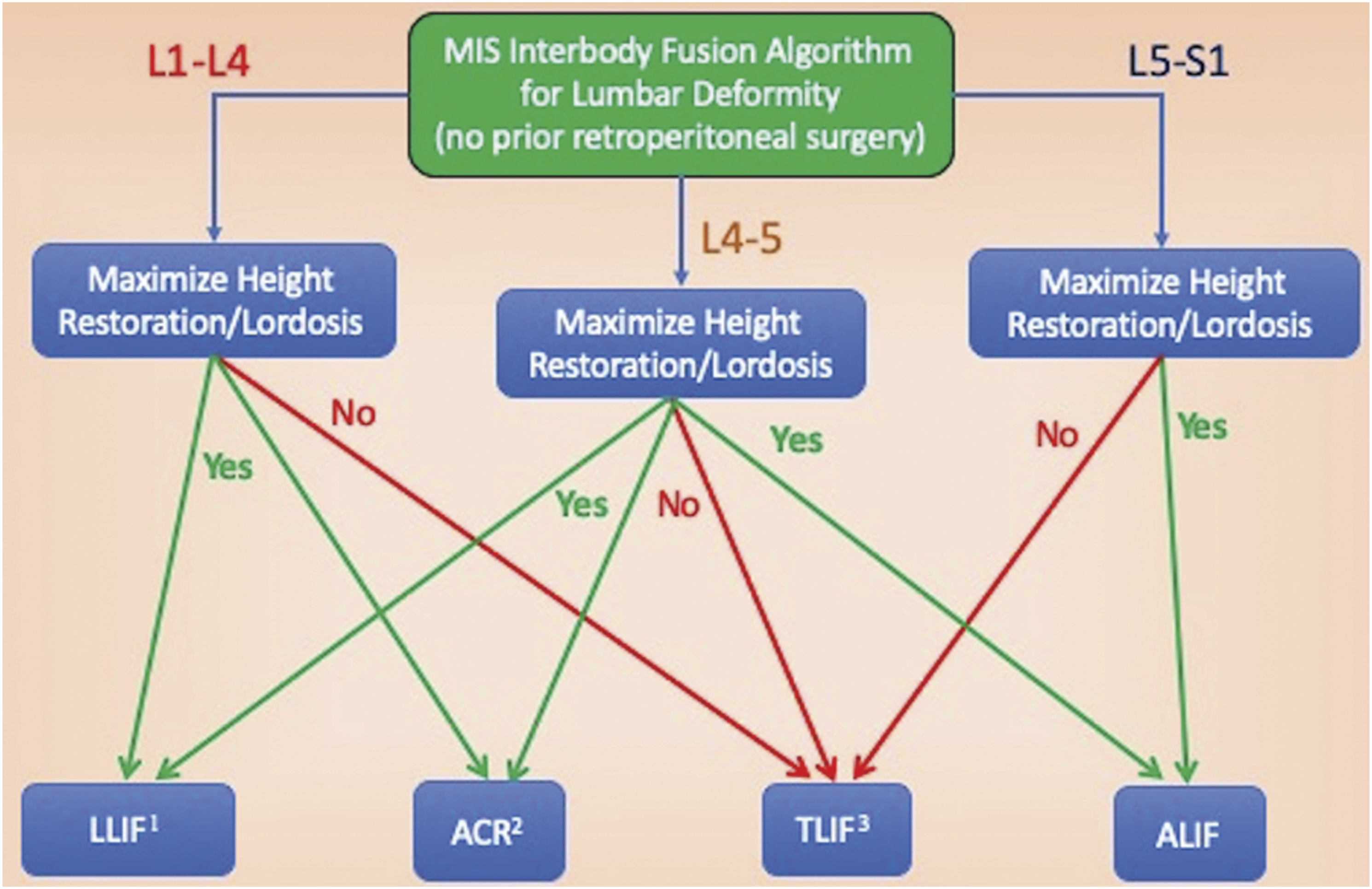
Anterior and lateral approaches are the workhorse approaches for MIS applications in ASD (Figure 4). They allow for indirect decompression, correction of coronal and sagittal plane deformity, and fusion without open posterior work. The lateral transpsoas or lateral lumbar interbody fusion (LLIF) and prepsoas or oblique lumbar interbody fusion (OLIF) approaches are ideal for levels from the thoracic spine down to L4-5. By working in the natural anatomical corridor of the retroperitoneal space, multiple disc spaces can be individually accessed – often from a single incision.47–50 The muscle splitting approach dilates through the muscles of the abdominal wall and psoas muscle, minimizing the tissue disruption that would be required in an open approach.51,49 Realtime and directional stimulation of dilators allows for insuring optimal entry through safe working zones in the psoas muscle, reducing risk of femoral nerve injury.52,53 The OLIF and anterior lumbar interbody fusion (ALIF) avoid dissection through the lumbar plexus; however, manipulation of the aorta and iliac vessels becomes necessary. Bilateral annular and osteophyte releases allow for powerful deformity correction.17,54 However, due to anatomical constraints of the iliac crest a transpsoas approach to the L5-S1 disc space is not possible with the LLIF. Here the OLIF and ALIF are utilized. Mummaneni et al
46
developed the minimally invasive interbody selection algorithm (MIISA) to creates a rational framework for decision-making in MIS deformity. Based on the level in the lumbar spine and the need for maximal lordosis or disc space height restoration the decision tree results in a recommendation for a LLIF, ALIF, ACR, or transforaminal lumbar interbody fusion (TLIF) (Figure 5). Anterior and Lateral MIS Approaches to the Spine. Used with permission from Barrow Neurological Institute, Phoenix, Arizona. The minimally invasive interbody selection algorithm (MIISA). Used with permission from Journal of Neurosurgery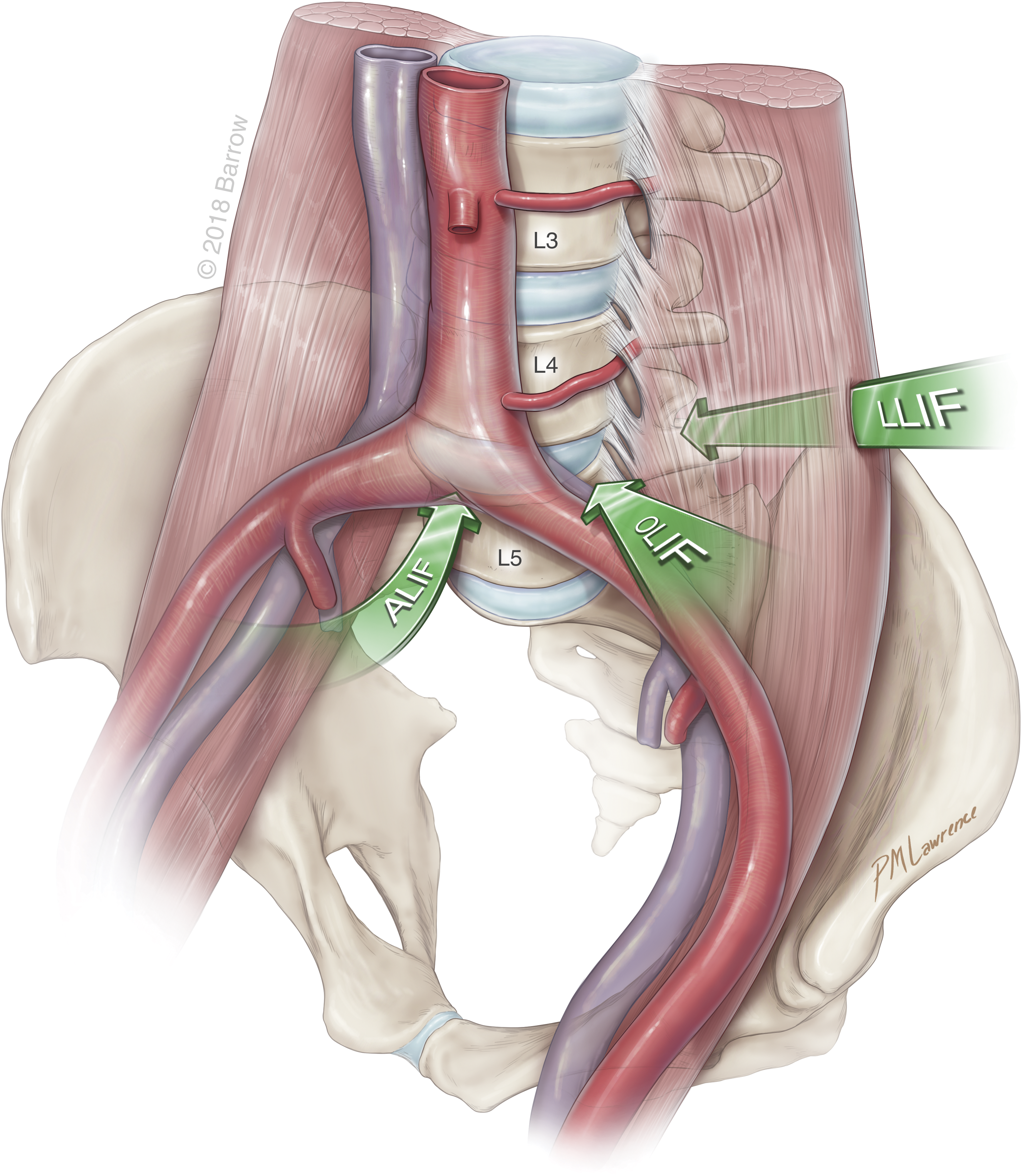
The anterior column realignment procedure (ACR) is nearly identical to the LLIF in approach to the disc space. It is typically reserved for severe deformities with at least non-fused segment in the lumbar spine to avoid open posterior osteotomies. First described in 2012, the surgeon dissects the vessel and anterior retroperitoneal structures away from the anterior longitudinal ligament (ALL) in order to safely release it, allowing for the placement of a hyperlordotic interbody (typically 20 or 30°).
55
The cage is fixated to either one or both of the adjacent vertebral bodies to prevent anterior migration. Fixation to only one vertebral body allows for subsequent posterior osteotomies to obtain even more lordosis.56,57 Uribe et al
58
in 2018, developed the ACR classification (Figure 6), combining the technique with the various osteotomies described in the SRS-Schwab osteotomy classification.
59
Mundis et al showed that the ACR technique has similar lumbar lordosis correction to a PSO (29.2 vs 25.4°) but with significantly less blood loss (1.6 L vs 3.6 L).
17
The anterior column realignment classification. Grade A ACR. ALL release with hyperlordotic cage and intact posterior elements. Grade 1 ACR: ALL release with hyperlordotic cage and inferior facetectomy. Grade 2 ACR: ALL release with hyperlordotic cage and complete facetectomies Grade 3 and 4 ACR: ALL release with hyperlordotic cage and pedicle subtraction osteotomies. Grade 5 ACR: ALL release with vertebral body resection. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.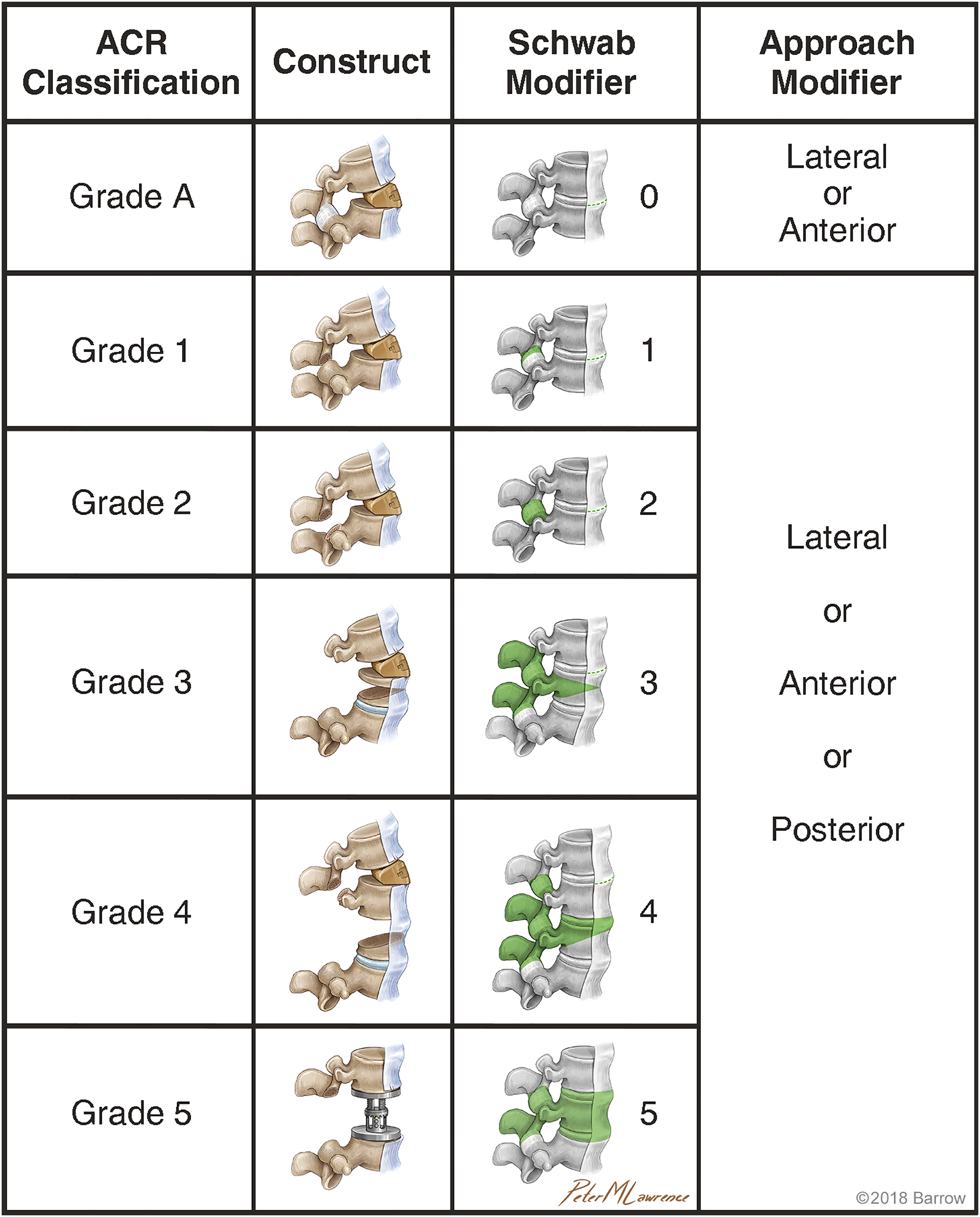
Specific anatomic challenges arise with the anterior working corridors in the setting of patients with lumbar scoliosis. The various changes to the normal vertebral alignment in both the coronal and sagittal planes as well as antero- and lateral listhesis present challenges to navigating to each disc space. Using fluoroscopic guided approaches, it is paramount to obtain perfect antero-posterior and lateral x-rays for all work within the disc space. These anatomical changes make obtaining these images difficult, and often the patient must be re-positioned for each level. With significant coronal deformity, patient positioning and side of approach are important considerations. Placing the patient in the lateral decubitus position with the concave side of the coronal curve facing up allows gravity and positioning to facilitate correction of the coronal deformity, thereby reducing the need to “force” corrections to the deformity. Additionally, accessing more vertebral levels through a smaller incision is possible with a concave approach-this can reduce surgical time and potential complications.
Additionally, with excessive degeneration of the disc spaces, anterior and lateral osteophytes are common. The presence of these osteophytes, limits access to the disc space, can lead to excess adhesions of surrounding structures, and can limit the potential segmental correction. Osteophytes often must be dissected and broken to achieve the goals of surgery through the anterior corridor. Lastly, the lumbar spine presents unique challenges due to its anatomical location and surrounding structures. In the upper lumbar area (L1-L3), the proximity of the ureters and kidneys to the spine can make accessing the retroperitoneal space more difficult. Surgeons must take care to avoid injury to these structures, which could lead to serious complications. In the lower lumbar region (L3-S1), the risk of vascular injury is a concern due to the presence of major blood vessels. Surgeons must carefully plan their approach to minimize the risk of damaging these vessels and causing significant bleeding.
Posterior Approaches
Although much of MIS deformity correction advancements focus on anterior and lateral approaches, Wang et al pushed the posterior approach in their description of the mini-open PSO. 18 This approach utilizes concepts of the traditional open-PSO, but is conducted through a smaller tissue sparing exposure isolated over the PSO site. The spine is instrumented by usual MIS percutaneous pedicle screws. However, since only the PSO site is fully exposed, closure of the osteotomy takes place by a four-rod cantilever maneuver.
Pelvic Fixation
While some MIS deformity constructs will end with the distal fixation point in the sacrum, many will require extension to the pelvis via iliac screw fixation. In such cases, the iliac screws are placed in a percutaneous fashion with the assistance of O-arm navigation. The entry point for these screws includes the posterior superior iliac spine (PSIS) or S2 alar-iliac screws, both of which have been shown to be safe methods.60–62 In all cases, intra-operative confirmation of accurate screw placement with fluoroscopy or O-arm should be obtained. A pre-contoured rod is then placed into the incision and passed in the subfascial plane such that it sits in the iliac and pedicle screw heads. A percutaneous rod reduction system is then used to reduce the rod into the screw heads.
Complications and Avoidance
Pre-Operative Evaluation
Various complication rates are reported in the literature for minimally invasive anterior and anterolateral approaches. The most important determinant of successful surgery is appropriate patient evaluation and selection pre-operatively. MRI and CT scans should be obtained prior to any procedure to ensure complication avoidance. MRI helps to identify several important anatomical factors including the location of the great vessels, the psoas muscle, and other visceral structures. CT scan helps to identify osteophytic changes or ankylosed segments which may preclude a successful discectomy. Additionally, standing 36-inch AP and lateral radiographs are obtained to help identify the height of the iliac crest and coronal cobb angle to allow for surgical access from the concave side.
Anterior Complications
The anterior approach is typically performed with the assistance of an access surgeon. Complications with this approach are most likely to stem from approach-related injuries. The most prominent complications which occur during the ALIF approach are vascular injuries and retrograde ejaculation. The iliac veins are routinely mobilized during this approach and are therefore at risk of injury, although the overall risk of vascular injury has been reported to be approximately 3%. Retrograde ejaculation, which occurs in men with injury to the superior hypogastric plexus, occurs in approximately 2% of retroperitoneal approaches. 63 Bowel injuries have been reported in the literature but are exceedingly rare with this approach. 64
Lateral Complications
Thorough knowledge of lumbar plexus anatomy and its course through the psoas muscle is key to avoidance of post-operative neurologic deficits when performing the transpsoas approach. The lumbar plexus travels anteriorly relative to the disc space as it courses caudally, and “safe zones” relative to each disc space have been reported.53,65,66 Uribe et. al. defined four zones based on sagittal quartiles of the vertebral body, with zone 1 being most anterior. They defined safe entry as the midpoint of zone 3 forward for L1-L4, and at the zone 2/3 junction and anterior for L4-5 (Figure 7). They found the genitofemoral nerve, primarily a sensory nerve, was the one nerve ventral to zone 3.
53
As such, caution must be taken to avoid injury to this and other sensory branches during the lateral discectomy as sensory nerves are not recognized by EMG. Direct visualization through the retractor helps ensure avoidance of sensory nerve injury. Radiographic safe zones for the transpsoas approach. The disc spaces and vertebral bodies on the lateral radiograph are divided into four zones anterior to posterior. The “safe zone” (zone III) is depicted in green and is the recommended trajectory through the psoas to reduce lumbar plexus and femoral nerve injury. Used with permission from Journal of Neurosurgery.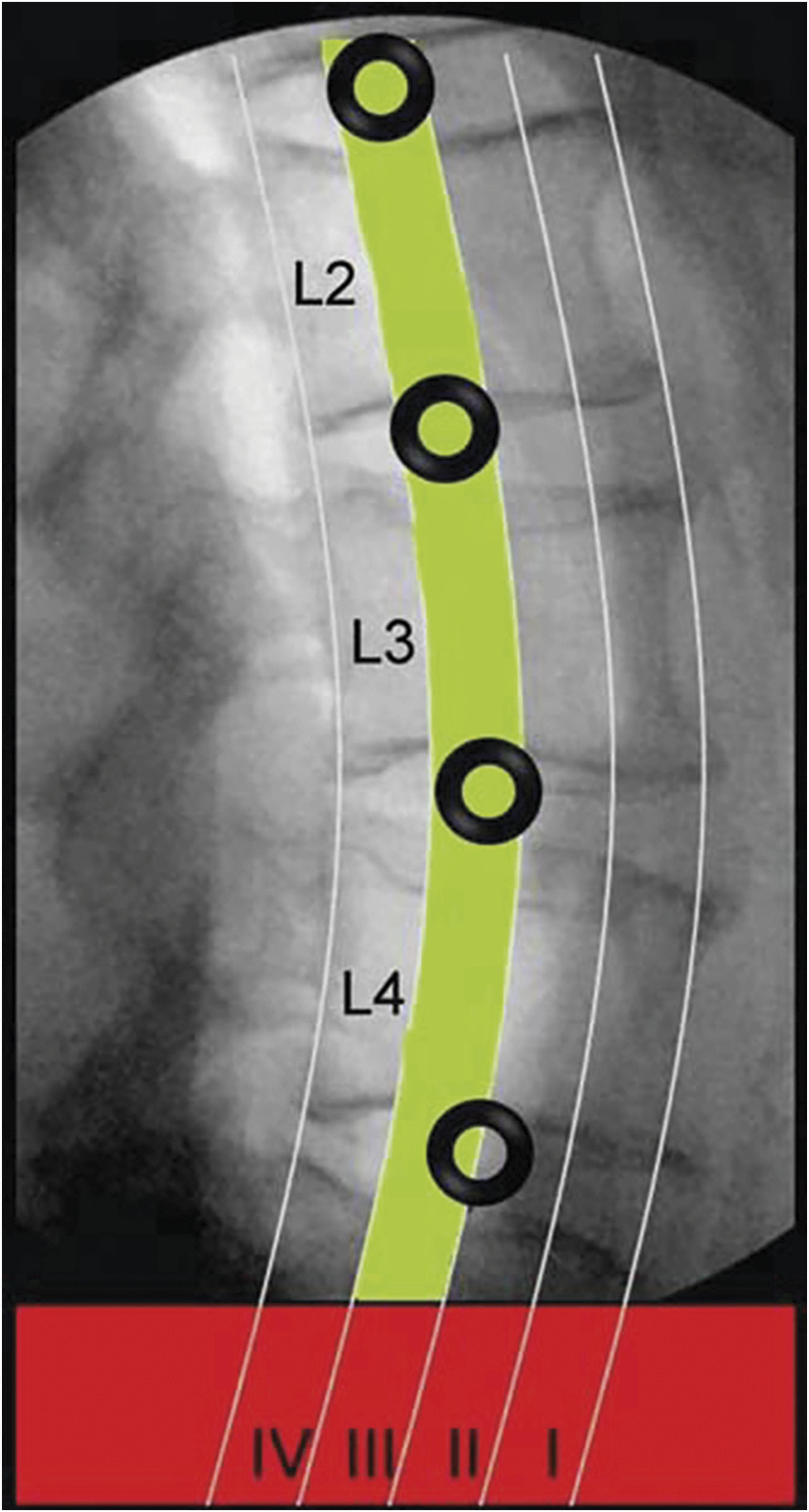
Most commonly after lateral surgery patients may report thigh symptoms such as numbness, paresthesias, or dysesthesias. There is a wide variation of reported rates from 0%–75%, most likely due to inconsistencies in reporting, study design, and technique. Femoral nerve and other motor injuries are less common, ranging from 0.7% to 33.6%.48,67–70 A large systematic review and meta-analysis of 2842 patients undergoing the transpsoas approach found that the rate of permanent motor neurologic deficit was 2.8%, compared to 1.0% in 1801 patients undergoing the prepsoas approach. 71 Other work has shown the use of recombinant human bone morphogenetic protein-2 (rhBMP-2) and ≥ four-level LLIF procedures were significantly associated with a greater risk of postoperative deficit. 70 Abdominal wall paresis, or “pseudohernia,” occurs due to injury to the iliohypogastric or ilioinguinal nerves during abdominal muscle dissection, and is usually associated with spontaneous recovery. 72
Prepsoas vs Transpsoas Approach
Complication Rates for MIS Lateral Approaches.
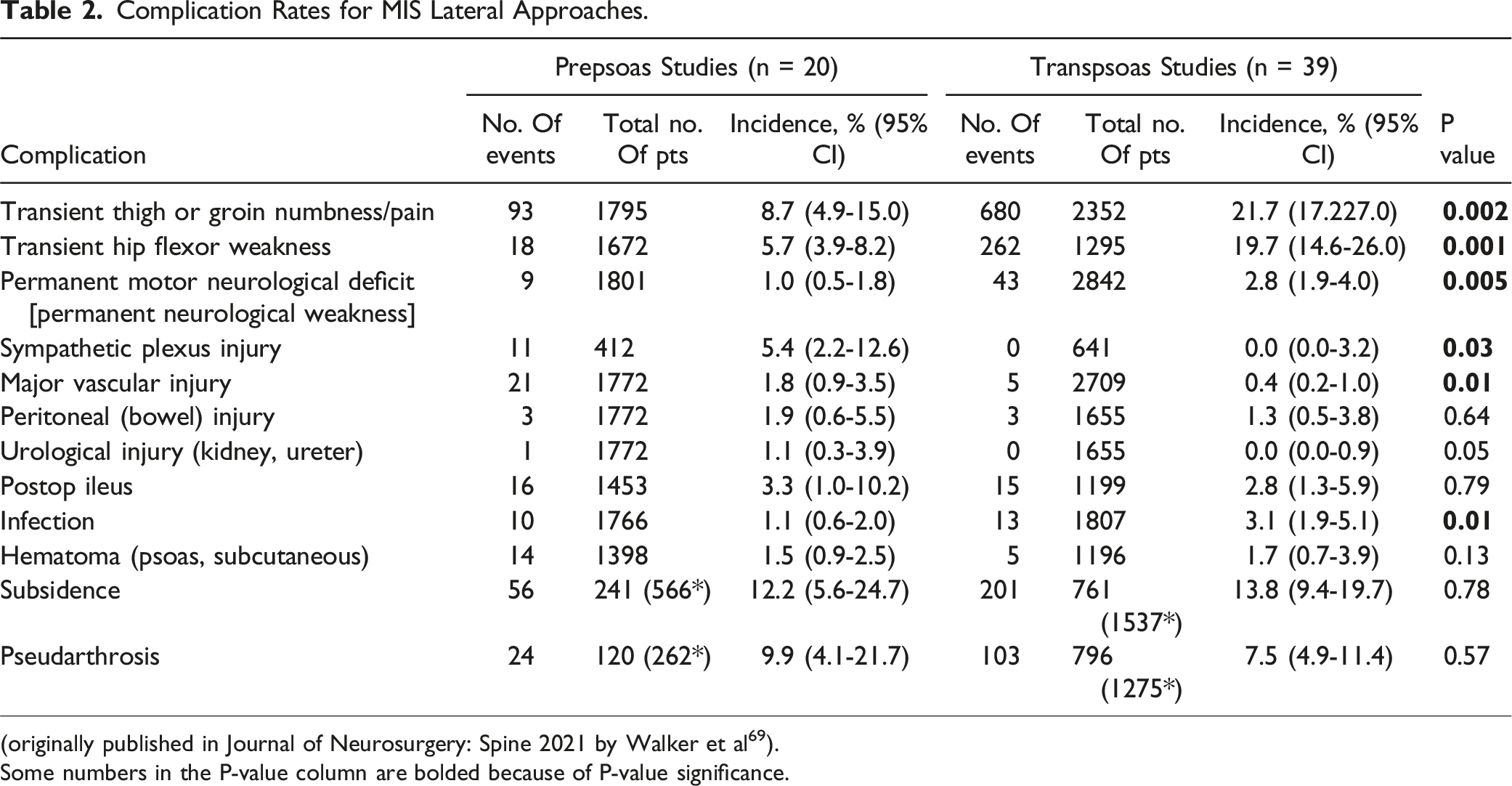
(originally published in Journal of Neurosurgery: Spine 2021 by Walker et al 69 ).
Some numbers in the P-value column are bolded because of P-value significance.
Future of MIS Techniques on Deformity
Emerging techniques and technologies will improve upon surgical efficiencies and outcomes in MIS spinal deformity correction. Technique innovations include novel patient positioning for multiple surgical stages. Developing technologies include changes to surgical navigation, robotics, and application of augmented reality/virtual reality for surgical training and intra-operative use.
Single Position Surgery
Traditionally when ALIF or LLIF are performed for MIS deformity correction these procedures are performed as separate stages with the ALIF performed in the supine position, the LLIF performed in the lateral decubitus position, followed by a third stage in the prone position for placement of pedicle screw fixation. These position changes necessitating staged surgeries lead to increased time under anesthesia and decrease overall surgical efficiency, sometime requiring multiple days for surgeries to be completed. Recent interest has emerged in combining multiple approaches into single stages to perform single position surgery.
Several reports of single-position surgery in the lateral position have reported the feasibility of this approach and improvement in operative efficiency.73–75 One study showed that patients treated with ALIF or LLIF in a single lateral position had decreased blood loss, complications, and length of stay compared to patients treated with traditional 2-stage (position) surgery. 76 More recently, multiple studies have reported the feasibility and early experience of performing LLIF and posterior pedicle screw fixation in a single prone position.77–79 This position following the PTP (prone transpsoas approach) allows the lumbar spine to fall into natural lordotic alignment during both surgical stages. Single position prone surgery does show promise for both MIS and hybrid surgical treatment of ASD. This novel approach would allow for placement of lateral interbody grafts at multiple lumbar segments followed by either percutaneous pedicle screw fixation or open fixation with the addition of osteotomies. Becoming facile in all these techniques allows the modern deformity surgeon to tailor each operation to the specific patient in a personalized manner. Further study is needed to elucidate the true safety profile and role for single stage procedures in MIS and hybrid deformity correction.
Combined Surgical Approaches
In the context of staged surgery for complex minimally invasive spine (MIS) deformity corrections, a meticulous approach is essential. Typically, anterior and lateral interbody fusions are performed to stabilize and correct the spine’s alignment and combined with posterior instrumentation, based on the clinical scenario and following MISDEF2 algorithms for MIS selection. 44 Postoperative standing X-rays are then carefully evaluated to determine the next steps. These images provide crucial insights, influencing whether a percutaneous screw placement or an open posterior approach should be used. Depending on the residual deformity and achieved alignment, the surgical team may choose to proceed with osteotomies to further refine spinal correction. This strategic, staged approach ensures optimal outcomes for patients with complex spinal deformities.
Navigation
Traditional open spine surgery requires midline incisions with subperiosteal dissection to identify bony anatomic landmarks for pedicle screw insertion. In contrast, MIS surgical techniques, rely on imaging-based landmarks for appropriate screw placement. Early imaging-based techniques included c-arm fluoroscopy and K-wire placement to assist with pedicle screw insertion. Further advancements have generated 2D and 3D computer-based navigation systems. 80 These systems rely on a stationary array which is rigidly affixed to the patient and serves as a reference while intra-operative imaging is obtained. All these technologies allow for percutaneous pedicle screw placement with decreased radiation exposure and less blood loss. Other advancements in navigation software can eliminate the need for the use of K-wires.81,82 Newer systems allow for navigated placement of interbody devices through posterior or lateral approaches with immediate application to MIS deformity correction. 80 Other navigation-based technologies include the development of robotic systems, augmented/virtual reality, and computerized rod bending and customized precontoured rods.
Robotics in Spine Surgery
Robotic systems represent another technological advancement with potential application to MIS spinal deformity correction. Other fields such as general and gynecologic surgery have previously adopted robotic technology.83,84 More recently, robotics have seen expanded application in spine surgery. Robotic systems provide a potential benefit of incorporating patient imaging to improve efficiency and accuracy of repetitive tasks which are subject to human/surgeon error such as pedicle screw placement. Multiple robotic systems are currently approved by the U.S. Food and Drug Administration and are currently in direct clinical use. One randomized trial found that pedicle screws placed using a robotic system were less accurate than those placed using a freehand technique. 85 However, numerous studies including multiple meta-analyses have since found non-inferiority or superiority of accuracy for pedicle screws inserted via robotic assistance.86–89 Other potential benefits of robotic systems include decreased radiation exposure to the surgeon, and decreased operative time. 90 Improvement in robotic software and expanded surgical applications will lead to continued adoption in the field.
Virtual Reality and Augmented Reality
Another emerging area with potential applications to MIS deformity operations and education is the addition of virtual reality (VR) and augmented reality (AR) platforms. VR consists of computer-generated 3D images which create a simulated environment while AR involves the simulation of artificial objects on a real backdrop. In spine surgery, VR has been shown to provide a benefit for surgical education. VR has been shown to improve screw placement accuracy for spine surgery trainees.91,92 AR has the potential for more direct use in the operating room as the digital overlay can be incorporated into the surgical field. There are multiple examples of new technologies including types of head-mounted and heads-up displays used to augment surgical procedures. These typically involve headsets which are worn in the operative suite and overlay pertinent information such as pre-operative imaging on to the surgical field.93–95 As this technology continues to be developed and improved, there exists a large potential application for its incorporation into MIS deformity corrections and surgical education. An important area for future development with these technologies will be the incorporation of haptic feedback to augment their utility.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.S.U. receives consulting fees and royalties from NuVasive Medical, Inc, and is a consultant for Misonix, Inc, and SI-BONE, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.