
Abstract
Study Design
Retrospective cohort study.
Objectives
To investigate the incidence of neurological deficits associated with percutaneous vertebral augmentation (PVA) surgery and to identify related risk factors.
Methods
We performed a retrospective analysis of the clinical data of patients who underwent PVA surgery at our institution between 2017 and 2022. A range of clinical parameters, including age, sex, fracture cause, fracture segment, number of vertebrae treated, surgical approach and surgical method, were collected.
Results
This study included a total of 1847 patients, including 422 (22.8%) men and 1425 (77.2%) women, with a total of 2319 diseased vertebrae. The mean age of the patients was 70.71 ± 8.80 years, with 211 (11.4%) patients aged under 60 years and 1636 (88.6%) patients aged over 60 years. Forty-six (2.5%) patients, accounting for 67 diseased vertebrae, were treated for tumors, whereas the remaining 1801 (97.5%) patients underwent surgery for fractures. Four hundred seventy-eight (20.6%) vertebrae underwent unilateral puncture, and the remaining 1841 (79.4%) vertebrae underwent bilateral puncture. Percutaneous vertebroplasty was performed on 1781 (76.8%) vertebrae, whereas percutaneous kyphoplasty was chosen for the remaining 538 (23.2%) vertebrae. Postoperative X-ray evaluations were conducted on the treated vertebrae, revealing that 403 (17.4%) vertebrae experienced polymethylmethacrylate (PMMA) leakage. Among the 1847 patients, 6 (7 diseased vertebrae) experienced nerve injuries postoperatively, and the incidence of neurological deficits after PVA surgery was 0.32%. Four of the 6 patients had nerve injuries due to PMMA leakage, and the other 2 patients had failed punctures. There was no statistically significant difference in terms of neurological complication rates according to patient age, sex, fracture segment, number of vertebrae treated, surgical approach or surgical method. However, the incidence of neurological complications was greater for patients with neoplastic fractures who underwent PVA surgery than for those with osteoporotic fractures.
Conclusions
PVA is an effective minimally invasive procedure for treating osteoporotic and neoplastic vertebral fractures. However, PVA can lead to serious neurological deficits. The incidence of neurological deficits associated with PVA surgery is 0.32%. Compared with patients with osteoporotic fractures, patients with neoplastic vertebral fractures who undergo PVA have a greater risk of neurological complications.
Keywords
Introduction
With the aging of the population, osteoporotic vertebral compression fracture (OVCF), the most common type of fracture in elderly patients with osteoporosis, has become a major issue in geriatric care. 1 In recent years, with the development of minimally invasive technology and the further development of minimally invasive concepts, percutaneous vertebral augmentation (PVA) surgery has become an important method for the treatment of OVCFs and neoplastic vertebral fractures (NVFs). The benefits of PVA include reduced tissue trauma, a shorter surgery time, and an accelerated recovery period postoperatively. 2 This procedure aims to alleviate pain, reinforce weakened vertebrae, and enhance the mobility of patients.3,4
As PVA surgery becomes more widespread, related complications are more frequently reported. The most frequently observed complication is the extravasation of polymethylmethacrylate (PMMA), which can lead to compression of the spinal cord or nerve roots, potentially causing spinal cord or nerve root injuries. Additional complications, such as epidural hematoma, rib fracture, cardiopulmonary embolism, PMMA toxicity, fractures in adjacent vertebrae, and vertebral infection, have also been documented on multiple occasions.5-8 The primary clinical signs of nerve injury following PVA surgery typically include radicular pain, weakness in the lower extremities, and sensory deficits. In 2007, Patel and colleagues reported 14 patients who sustained nerve injuries after PVP. However, their report was a retrospective analysis of disease progression, without an investigation into the incidence rate of nerve injuries or their associated risk factors. 9 In 2019, Hsieh et al conducted a retrospective review of the clinical data of 3175 patients who underwent PVP. However, their analysis was limited to patients with symptomatic OVCFs, and they did not explore operation-related complications in patients with vertebral tumors. 10
To our knowledge, the incidence of neurological deficits associated with PVA surgery has not been analyzed in a large group at a single institution. Therefore, we conducted this study to investigate the incidence of and risk factors for neurological deficits associated with PVA surgery.
Materials and Methods
A retrospective analysis of the medical records of patients enrolled in this study was conducted. The study protocol was reviewed and approved by the Institutional Review Board of Taizhou People’s Hospital (Approval No. KY202307101).
The data collected for the study included demographic information such as age, sex, and cause of the fracture. Furthermore, pertinent imaging data, surgical details, and perioperative complications were recorded and subjected to analysis. These included the fracture segment (thoracic or lumbosacral vertebrae), number of surgical vertebral segments, surgical approach (unilateral or bilateral pedicle approach), surgical method (percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP)), occurrence of PMMA extravasation, and neurological status following PVA surgery. The neurological status of each patient was assessed both preoperatively and postoperatively, utilizing the American Spinal Injury Association (ASIA) Spinal Cord Injury Classification method as the standardized evaluation tool.
Categorical variables are presented as numbers and percentages. Statistical analysis of the collected data was performed using SPSS software, and the chi-square test or Fisher’s exact test was employed for categorical variables. Statistical significance was set at a P value <0.05.
Results
This study included 1847 patients, including 422 men (22.8%) and 1425 women (77.2%). The mean age of the cohort was 70.71 years, with a standard deviation of 8.80 years. Two hundred eleven patients (11.4%) were younger than 60 years, and 1636 patients (88.6%) were older than 60 years. Among all the patients, 1478 patients (80.0%) underwent PVA surgery on a single vertebral segment, and 278 patients (15.1%) underwent this procedure on 2 segments. Eighty patients (4.3%) underwent this surgery on three segments, 10 patients (0.5%) had four segments treated, and 1 patient (0.1%) underwent a five-segment PVA. PVA surgery was conducted for tumors in 46 patients (2.5%), whereas the remaining 1801 patients (97.5%) received PVA surgery for OVCFs.
Among the 1847 patients, a total of 2319 vertebrae underwent PVA surgery, and the distribution of vertebral segments is shown in Figure 1. Among the 2319 diseased vertebrae, tumor destruction was the cause in 67 (2.9%) cases. Unilateral puncture was performed on 478 vertebrae (20.6%), whereas bilateral puncture was utilized for 1841 vertebrae (79.4%). In terms of surgical methods, PVP was performed on 1781 vertebrae (76.8%), and PKP was applied to the remaining 538 vertebrae (23.2%). Postoperative X-ray examinations were conducted on the treated vertebrae, revealing PMMA leakage in 403 vertebrae (17.4%). The detailed clinical data and imaging characteristics of the patient cohort are presented in Table 1. Frequency distribution of diseased vertebral segments. Patient Demographics and Clinical Data. Abbreviations: NVF, neoplastic vertebral fractures; OVCF, osteoporotic vertebral compression fracture; PVP, percutaneous vertebroplasty; PKP, percutaneous kyphoplasty.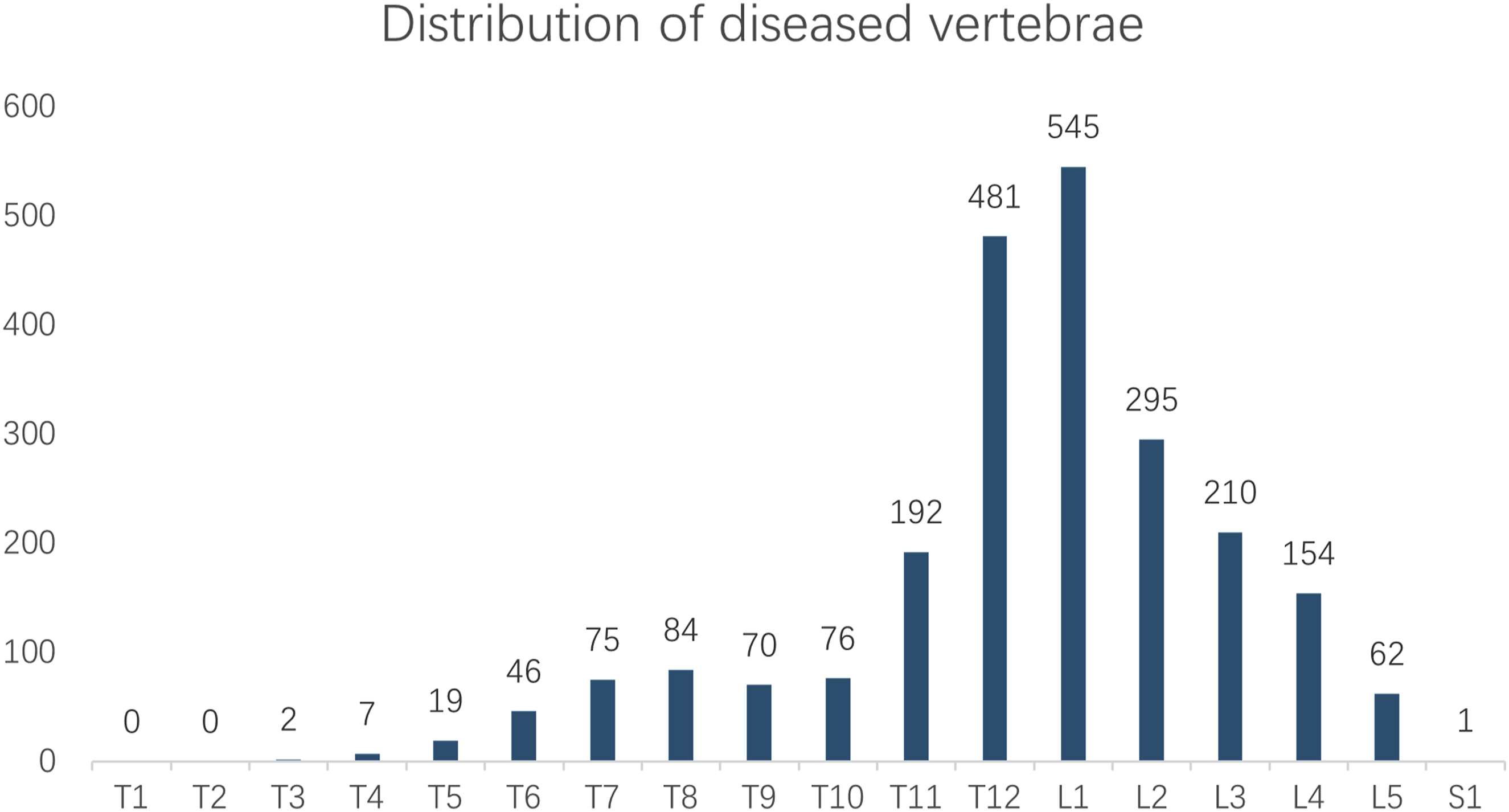

Clinical Data of Patients With Severe Neurological Deficits after PVA Surgery.
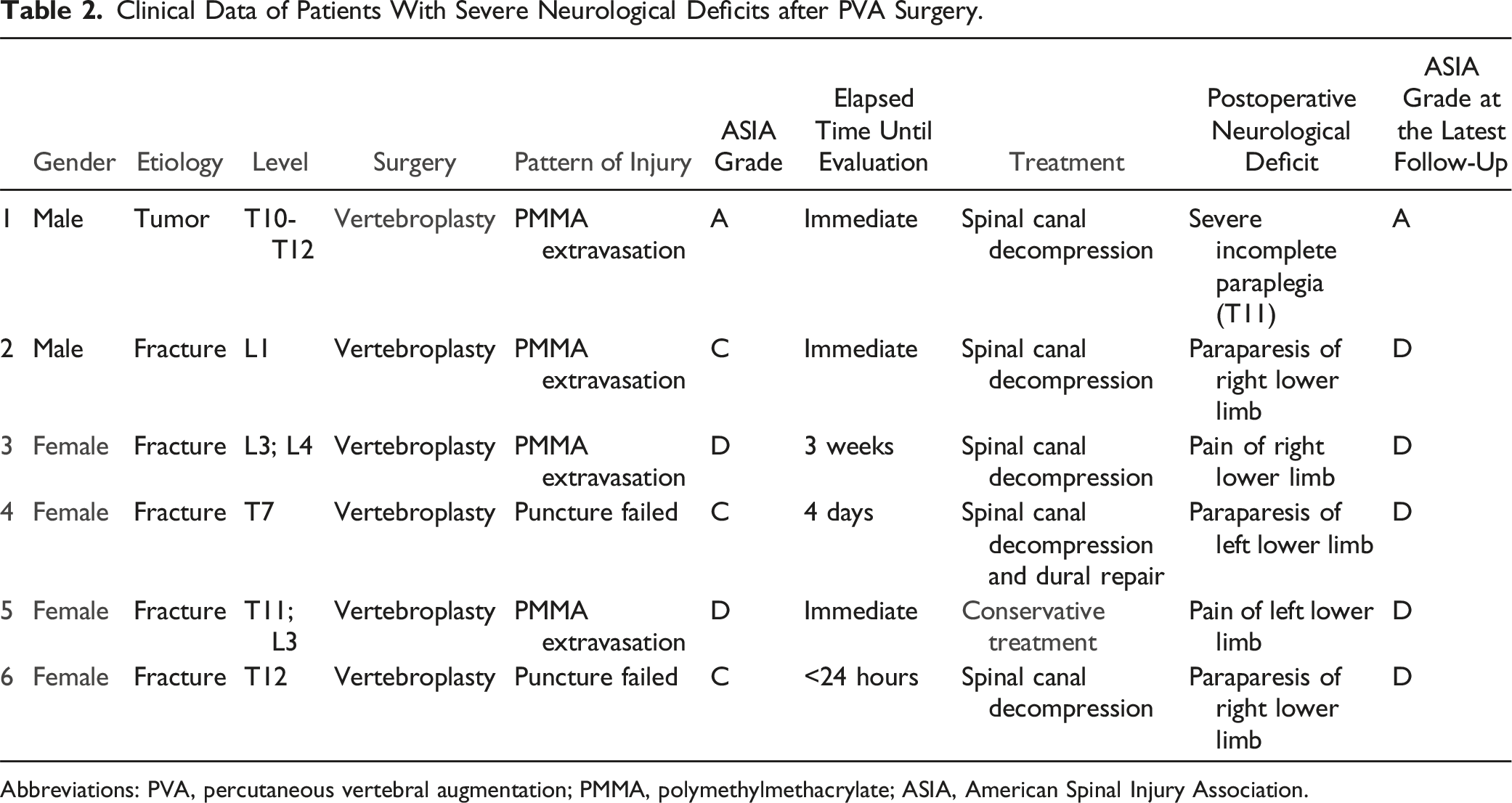
Abbreviations: PVA, percutaneous vertebral augmentation; PMMA, polymethylmethacrylate; ASIA, American Spinal Injury Association.
The Incidence of Neurological Deficits in 1847 Patients (2319 Vertebra) With PVA Surgery.
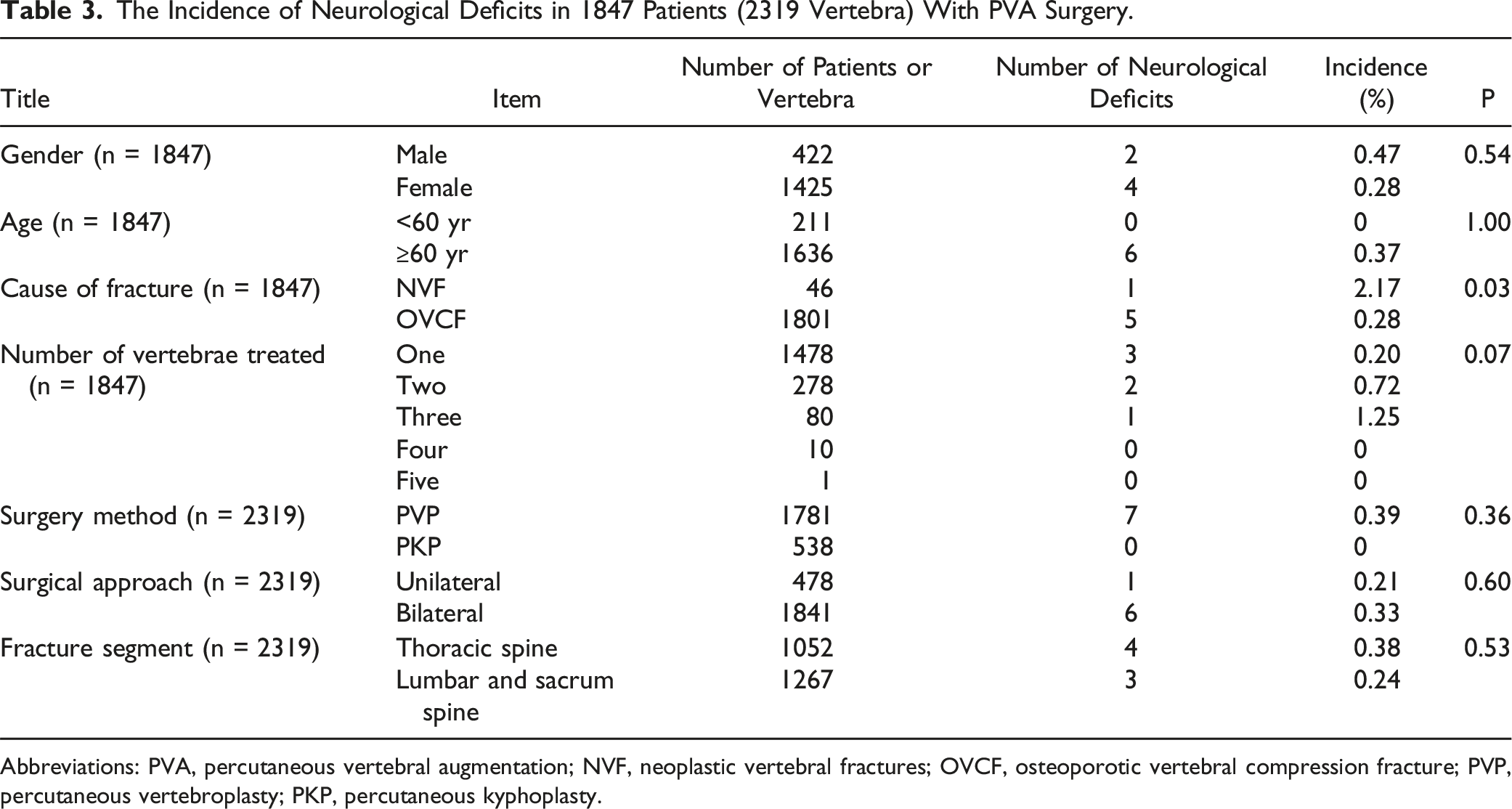
Abbreviations: PVA, percutaneous vertebral augmentation; NVF, neoplastic vertebral fractures; OVCF, osteoporotic vertebral compression fracture; PVP, percutaneous vertebroplasty; PKP, percutaneous kyphoplasty.
Illustrated Cases
Patient 1
An 80-year-old female patient was admitted to the hospital due to persistent low back pain and was subsequently diagnosed with OVCFs at the L3 and L4 vertebrae. The primary symptom experienced by the patient was low back pain, with no manifestations of lower limb pain or motor dysfunction. During the preoperative examination, no contraindications for surgery were identified, and the surgical plan was established as PVP for the L3 and L4 vertebrae.
During the PVA procedure, PMMA was injected into the vertebra through bilateral pedicle punctures. Unfortunately, the patient developed pain and weakness in the right lower limb following surgery. Postoperative physical examination revealed that the sensation and muscle strength of the right lower limb were decreased, with a muscle strength of approximately grade 4. The postoperative computed tomography (CT) scan shown in Figure 2 confirmed that PMMA had leaked into the lumbar spinal canal, resulting in spinal stenosis and nerve compression. An 80-year-old female patient underwent PVA surgery at the L3 and L4 vertebrae. CT scans in the sagittal (A), axial (B), and coronal (C) planes revealed PMMA leakage into the epidural space.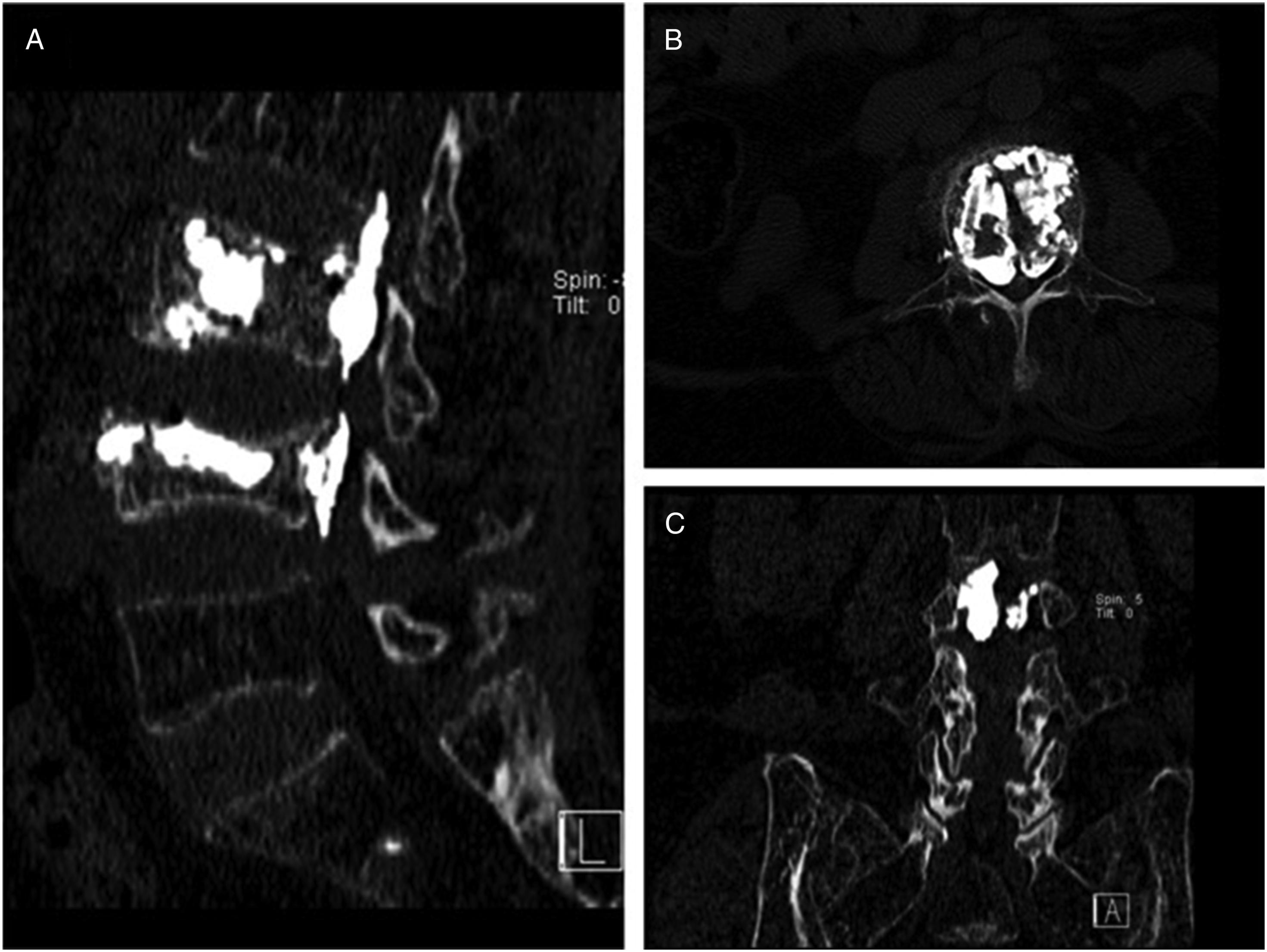
Upon confirming PMMA leakage, posterior lumbar spinal canal decompression surgery was performed. The postoperative spinal cord function score was assessed as ASIA grade D, indicating some preservation of sensory and motor functions below the neurological level of injury.
Patient 2
A 75-year-old female patient with low back pain following a fall was admitted to the hospital. Preoperative MRI revealed a T7 vertebral compression fracture. Physical examination prior to surgery revealed no symptoms of lower limb pain or motor dysfunction. Considering the severity of her back pain, we performed PVA surgery at the T7 segment. During the procedure, PMMA was injected into the vertebra through bilateral pedicle punctures.
Postoperatively, the patient experienced left lower limb numbness extending below the left costal margin accompanied by weakness, with a muscle strength grade of 3. The subsequent CT image shown in Figure 3 revealed that the left pedicle puncture was medially misplaced, causing the puncture needle to enter the spinal canal. A 75-year-old female patient underwent PVA surgery at the T7 vertebra. Postoperative X-ray films (A) and (B) revealed no obvious complications. However, postoperative CT images (C) demonstrated an error in the puncture of the left pedicle.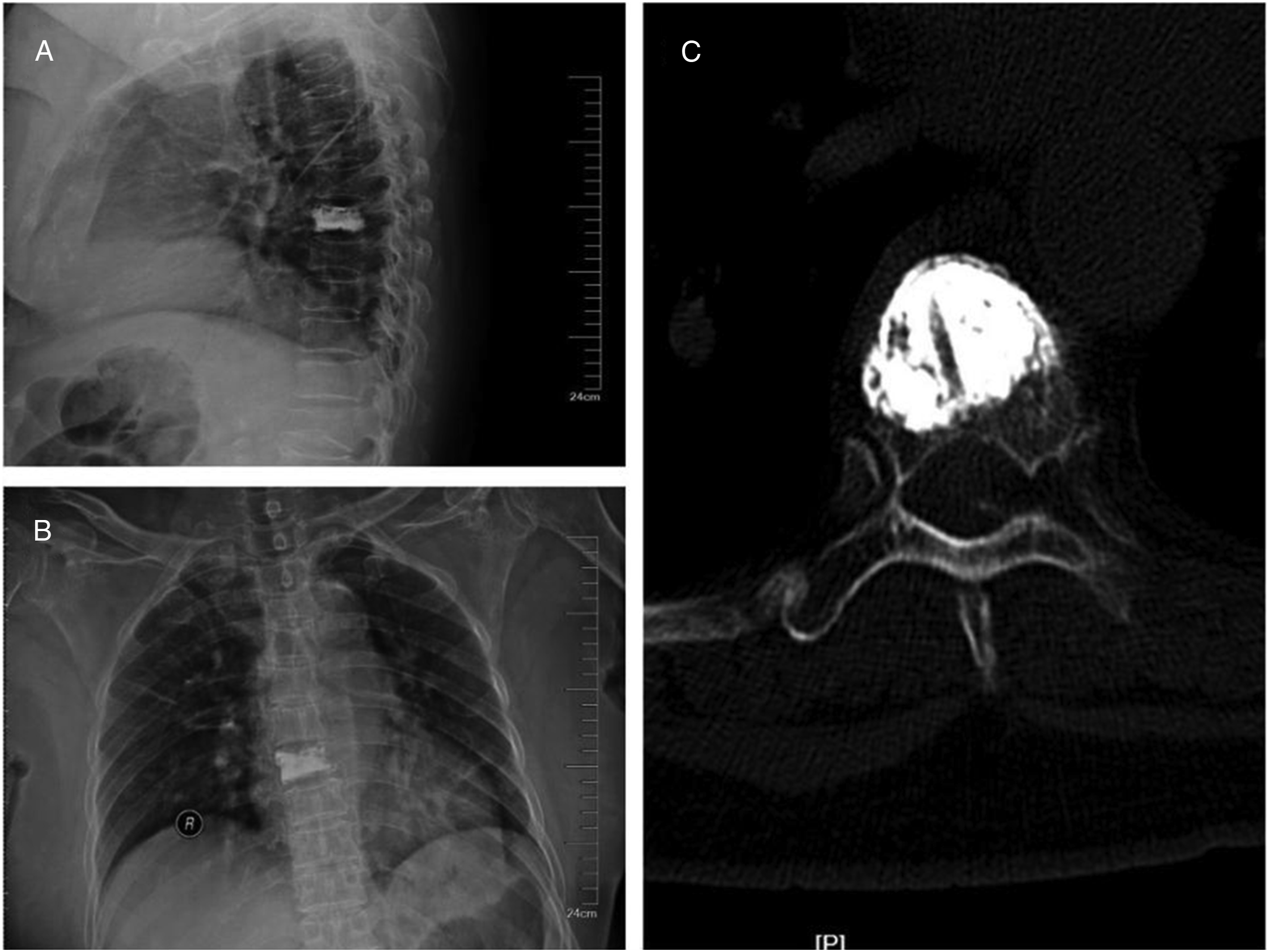
After confirming thoracic spinal cord injury, emergency posterior thoracic spinal canal decompression surgery was performed. During surgery, dural rupture was discovered and subsequently repaired. The patient’s spinal cord function improved from preoperative ASIA grade C to postoperative grade D.
Discussion
PVA surgery is an effective treatment for OVCFs or NVFs in elderly individuals, significantly alleviating their clinical symptoms. However, numerous studies have highlighted the risk of various complications following this surgical procedure.11-13 Despite widespread reports of complications at various centers, large clinical studies on neurological deficits following PVA surgery are lacking. To address this gap, we conducted this study and reported that the incidence of neurological deficits in PVA surgery patients is 0.32%, and compared with OVCFs, vertebral tumor lesions are a more notable risk factor for neurological deficits associated with PVA surgery. The 2 causes of neurological deficits associated with PVA surgery are related to intraoperative PMMA leakage and puncture errors.
Some researchers posit that the thoracic spine may be more susceptible to neurological deficits during PVA surgery than the lumbar spine is. This hypothesis is based on the anatomical differences between the 2 regions: the thoracic spinal canal is inherently narrower than its lumbar counterpart and houses a more vulnerable spinal cord, whereas the lumbar canal contains the cauda equina, which is considered more resilient. Consequently, if PMMA leaks into the spinal canal during PVA surgery, the potential for neurological deficits is greater in the thoracic spine. In their study of 1340 thoracic and 2472 lumbar vertebroplasty procedures, Hsieh et al. reported a significantly higher rate of neurological complications following thoracic vertebroplasty (0.22%) than following lumbar vertebroplasty (0.04%) (P < 0.01). 10 They identified intraoperative PMMA leakage as the primary cause of nerve injury. Our study, however, which included 1052 thoracic and 1267 lumbosacral vertebrae, revealed neurological complication rates of 0.38% and 0.24%, respectively. This difference was not statistically significant (P = 0.53). These findings suggest that the risk of neurological deficits following PVA surgery may not be significantly different between the thoracic and lumbar spine.
There are 2 possible reasons why our results are different from those of previous studies. First, we usually perform unilateral punctures in the thoracic vertebrae and bilateral punctures in the lumbar vertebrae, and reducing the number of punctures may decrease the risk of neurological deficits. Yan et al. compared unilateral transverse process-pedicle and bilateral puncture techniques in PKP, and the results revealed that unilateral PKP resulted in a lower radiation dose and operation time, offered a greater degree of deformity correction and resulted in fewer complications than did bilateral PKP. 14 Second, compared with the lumbar vertebrae, we are accustomed to injecting less PMMA into the thoracic vertebrae, which correspondingly reduces the risk of PMMA leakage. Some researchers have reported that epidural leakage of PMMA after percutaneous vertebroplasty is dose dependent. The larger the amount of injected PMMA is, the greater the risk of leakage.15-17
The question of whether the risk of neurological deficits following PVA surgery differs between osteoporotic and tumor-related vertebral fractures remains a subject of ongoing debate. Studies have shown that the incidence of transient neurological injury after vertebroplasty in patients with NVFs ranges from 3% to 6%, whereas the incidence of permanent neurological deficits falls between 2% and 3%. 18 In 2009, Lee et al 19 reported that tumor-related fractured vertebrae were more prone to neurological deficits than osteoporotic fractured vertebrae were. In their study comparing 176 patients with OVCFs to 18 patients with NVFs, Tom é - Bermejo et al reported that the incidence of PMMA leakage was 24.6 times greater in the NVF group. 20 Lee et al 11 reported a higher rate of PMMA leakage in NVFs than in OVCFs.
Our results support the above conclusions. Among all the patients, 46 underwent PVA surgery for neoplastic vertebrae. One patient (2.17%) in the NVF group developed postoperative neurological deficits. In contrast, the incidence of neurological deficits following PVA surgery for OVCFs was significantly lower at 0.28% (P = 0.03). Our results, therefore, indicate that PVA surgery for NVFs is associated with a greater risk of nerve injury. The possible reason for this phenomenon is that the tumor lesion causes the bone tissue of the vertebra to be replaced by highly vascularized tumor tissue, and the posterior cortex of the vertebra is destroyed by the tumor, resulting in the loss of integrity, thereby increasing the risk of PMMA leakage. Some scholars believe that an incomplete bone cortex, which is a defining characteristic of NVFs, increases the risk of PMMA leakage.21-23
PMMA leakage is a prevalent complication of PVA surgery, potentially leading to severe consequences, including nerve injury. At present, the reported incidence of PMMA leakage varies from 34.0% to 91.3%,2,24-26 but most cases of PMMA leakage are asymptomatic. CT thin-layer scanning is the gold standard for detecting PMMA leakage following PVA surgery.23,27 In this study, we found that the incidence of PMMA leakage during PVA surgery was 17.4%, which is lower than that previously reported. The main reason for the low rate of PMMA leakage in our study may be that the method for detecting PMMA leakage was anteroposterior and lateral X-ray films, not a CT scan. We observed that in most cases, PMMA leaked anteriorly, laterally, or into the intervertebral spaces of the vertebral body, including the surrounding small blood vessels. These findings are similar to those of previous studies.17,28 Severe consequences of PMMA leakage include nerve compression caused by PMMA leakage into the spinal canal, as well as pulmonary vascular, cardiac, and cerebrovascular PMMA embolisms.29-32 Despite the relatively high incidence of PMMA leakage observed in our study, only 4 patients experienced neurological deficits. Importantly, all 4 cases involved PMMA extravasation into the spinal canal, leading to direct nerve compression. To date, we have not encountered any cases of pulmonary, cardiac, or cerebral PMMA embolism at our institution. The illustrated case 1 selected as a typical example exhibited neurological deficits caused by PMMA extravasation into the spinal canal.
Puncture failure, particularly penetration into the spinal canal, can result in severe nerve injury. 5 However, its incidence is relatively low. According to the current literature, its occurrence rate is between 0.8% and 4.0%. 33 Noguchi et al 33 reported that all patients who underwent puncture into the spinal canal exhibited no clinical symptoms postoperatively and that all patients were managed conservatively after surgery, including extended rest periods and regular imaging follow-ups. We believe that the lack of reported nerve injury by Noguchi et al may be attributed to the puncture needle only slightly breaching the medial wall of the pedicle without significantly entering the spinal canal. In our study, 6 patients experienced nerve injuries, with 2 cases caused by puncture into the spinal canal. The illustrated case 2 selected as a typical example exhibited neurological deficits caused by puncture into the spinal canal.
Among the 6 patients with nerve injury, 5 patients received remedial spinal canal decompression surgery. Among them, the spinal cord function of 3 patients improved from ASIA grade C before remedial surgery to ASIA grade D after remedial surgery. We believe that spinal canal decompression surgery is an effective treatment for improving the neurological function of patients with neurological deficits after PVA surgery.
This study has several limitations. First, this study was performed retrospectively. Second, the study did not include the PMMA injection volume as a research indicator. Third, the difference in skill levels among the operators was not considered. A prospective study involving experts of relatively uniform skill levels that takes into account the volume of injected PMMA is necessary.
Conclusion
PVA is an effective minimally invasive procedure for treating osteoporotic and neoplastic vertebral fractures. However, PVA can lead to serious neurological deficits. The incidence of neurological deficits associated with PVA surgery is 0.32%. PVA for neoplastic vertebral fractures is associated with a greater risk of neurological complications than PVA for osteoporotic fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The General Project of the Science and Technology Development Fund of Nanjing Medical University (NMUB20230298).
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Aibing Huang, upon reasonable request.