
Abstract
Study Design
Retrospective Cohort
Objective
Antiresorptive drugs are often given to minimize fracture risk for bone metastases, but data regarding optimal time or ability to reduce stereotactic body radiotherapy (SBRT)-induced fracture risk is limited. This study examines the association between antiresorptive use surrounding spinal SBRT and vertebral compression fracture (VCF) incidence to provide information regarding effectiveness and optimal timing of use.
Methods
Patients treated with SBRT for spinal metastases at a single institution between 2009-2020 were included. Kaplan-Meier analysis was used to compare cumulative incidence of VCF for those taking antiresorptive drugs pre-SBRT, post-SBRT only, and none at all. Cox proportional hazards and Fine-Gray competing risk models were used to identify additional factors associated with VCF.
Results
Of the 234 patients (410 vertebrae) analyzed, 49 (20.9%) were taking bisphosphonates alone, 42 (17.9%) were taking denosumab alone, and 25 (10.7%) were taking both. Kaplan-Meier analysis revealed a statistically significant lower VCF incidence for patients initiating antiresorptive drugs before SBRT compared to those taking none at all (4% vs 12% at 1 year post-SBRT, P = .045; and 4% vs 23% at 2 years, P = .008). On multivariate analysis, denosumab duration (HR: .87, P = .378) or dose (HR: 1.00, P = .644) as well as bisphosphonate duration (HR: .98, P= .739) or dose (HR: .99, P= .741) did not have statistical significance on VCF incidence.
Conclusion
Initiating antiresorptive agents before SBRT may reduce the risk of treatment-induced VCF. Antiresorptive drugs are underutilized in patients with spine metastases and may represent a useful intervention to minimize toxicity and improve long-term outcomes.
Introduction
Spine metastases occur in 30-50% of cancer patients and are a common cause of morbidity and mortality. 1 Stereotactic body radiotherapy (SBRT) delivers highly conformal, dose-escalated radiation that provides a higher biological effective dose (BED) than conventional radiation while also allowing superior sparing of proximal normal tissue. 2 Thus, SBRT is increasingly and effectively being used for both pain relief and tumor control in patients with spinal metastases.3-6 However, use of this method may also increase the risk of a vertebral compression fracture (VCF), a potentially debilitating adverse event. While VCF risk for conventional radiotherapy is only around 5%, the estimates for crude risk of VCF after spinal SBRT ranges from 11% to 39%. 7 Therefore, methods to decrease the risk of VCF following SBRT are critical.
Antiresorptive agents are widely utilized in the context of osteoporosis to restore balance between bone resorption and formation. Osteoblasts express RANKL on their surface which binds to RANK on pre-osteoclasts to stimulate osteoclast development. Denosumab is a monoclonal antibody to RANKL which blocks this binding and therefore inhibits osteoclastogenesis. 8 Bisphosphonates act through a different mechanism in which they are initially laid down on the bone surface and then taken up by osteoclasts during bone resorption. Once inside the osteoclasts, they inhibit a variety of cellular activities by blocking the mevalonate pathway and inhibiting osteoclast function. 9 These drugs are often given to patients with bone metastases to minimize the risk of fracture, but minimal data exist regarding their ability to reduce fracture risk from SBRT or the optimal timing of delivery.
This study examines the association between antiresorptive agent use surrounding spinal SBRT and VCF incidence. Based on the physiology of antiresorptive agents, we hypothesized that patients taking this therapy prior to SBRT will have a lower incidence of VCF than those receiving them afterward or those not receiving them at all.
Materials and Methods
Informed consent was not required as the study was approved as exempt by the local Institutional Review Board. Patients treated with SBRT for spinal metastases at a single tertiary academic Radiation Oncology center from 2009-2020 were retrospectively reviewed in accordance with best ethical research practices. All patients received SBRT following multidisciplinary evaluation by radiation oncologists, medical oncologists, and spine surgeons. Patients had confirmed spine metastases from solid tumors based on MRI. Biopsy of the spine lesions were performed when there was question regarding the etiology. Patients with prior radiation to the involved vertebral level were included. Those with hematologic malignancies and primary spine tumors were excluded. Similarly, patients that had undergone surgical stabilization to the involved level with instrumentation or cement augmentation to the treated area were not included in the analyses.
Patients underwent CT and co-registered MRI for target and organs at risk delineation. Gross tumor volume (GTV), clinical target volume (CTV), planning treatment volume (PTV), and organs at risk were contoured by the treating radiation oncologist and reviewed by a neurosurgical colleague for approval. Gross tumor volume was identified using T1 and T2 weighted MRIs and CT from simulation. Clinical target volume was defined according to the consensus contouring guidelines for spine metastases for most cases.10-13 Planning treatment volume was created with a 1-2 mm margin, subtracting the spinal cord planning risk volume (PRV), which was typically defined as the spinal cord plus a 2 mm radial expansion or the thecal sac for treatments below the conus. 14 Prescription doses were determined by the treating radiation oncologist. Radiation treatment planning parameters of prescription dose/fractionation and isodose line were collected and BED was calculated using the equation BED = D *(1 + [d/(α/β)]), where D is the total dose in Gy, d is the dose per fraction, and the α/β was estimated to be 3 for all tumors. Spinal cord constraints generally followed the 5% risk level in Sahgal et al 15 and all other normal tissue constraints followed American Association of Physics in Medicine Task Group-101. Based on institutional practice patterns, patients were generally followed with clinical evaluations and MRI imaging at 3-6 months time intervals after receiving SBRT.
Patient and disease characteristics were collected retrospectively, including age, gender, performance status, body mass index (BMI), smoking status, primary histology and tumor site, prior irradiation status, steroid use, and antiresorptive type, dose, and duration of use. Age was recorded at the first SBRT treatment. Pre-treatment Spinal Instability Neoplastic Score (SINS), as well as its subcomponents, were identified and calculated for each patient by a radiologist and radiation oncologist using the latest CT scan prior to SBRT. 16 Spinal Instability Neoplastic Score was classified as stable (total score 0-6), potentially unstable (7-12), and unstable (13-18). Factors used to calculate SINS include location, characteristics of pain, lesion type (lytic vs blastic), alignment, degree of pre-existing vertebral body collapse, and involvement of posterolateral elements.
The primary endpoint was post-SBRT VCF. Occurrence was recorded if the treated vertebra was involved and confirmed by the radiology report from comparing the VB height on serial MR imaging.
Statistical analysis was performed to determine significant factors associated with VCF. Kaplan-Meier survival analysis was utilized to compare the cumulative incidence of VCF at 6, 12, and 24 months post-SBRT for the subgroups including those taking no antiresorptive medication, those initiating antiresorptive medication before SBRT, and those initiating antiresorptive medication after SBRT. Cox proportional hazards and Fine-Gray competing risk models were used to construct models for the separate subpopulations of those taking bisphosphonates and those taking denosumab to determine hazard rates for VCF incidence. Model covariates included antiresorptive drug duration, antiresorptive drug cumulative dose, radiation dose per fraction, BMI, and total SINS, based off prior reported predictive factors of VCF. For the sake of the analyses, antiresorptive drug duration, cumulative dose, radiation dose, BMI and SINS were defined as continuous variables. Multiple imputation was used with 10 imputations for the antiresorptive drug cumulative dose variable as data was not available for all patients. Univariate Cox models were used to test separately for those factors listed above. Multivariable Cox models were generated to report the hazard ratios, along with 95% confidence intervals. Competing risks for the Fine-Gray model were local progression and death. Results were considered significant if P values < .05.
Results
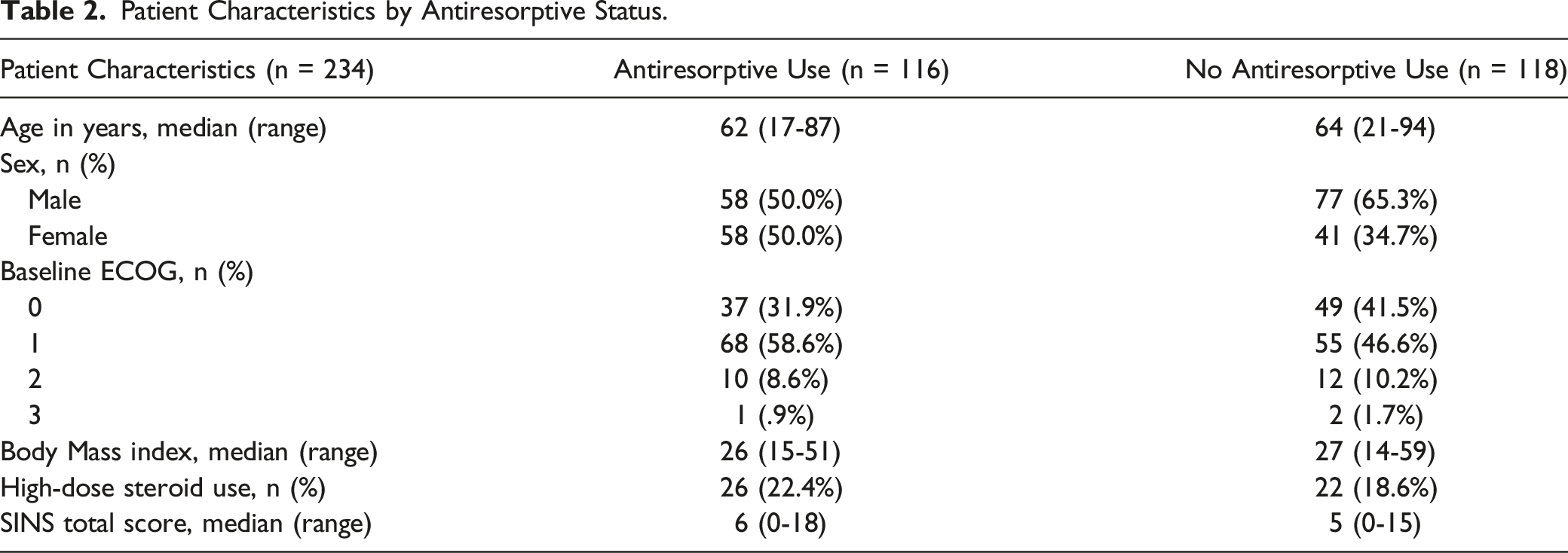
Patient, Lesion, and Treatment Characteristics.

Patient Characteristics by Antiresorptive Status.
Kaplan-Meier analysis revealed a statistically significant reduction in VCF incidence for patients initiating antiresorptive drugs before SBRT compared to those with no antiresorptive drug use (P = .008), as seen in Figure 1. Specifically, VCF incidence for those initiating antiresorptive drugs before SBRT compared to those taking no antiresorptive drugs at all were 4% vs 8% at 6 months (P = .173), 4% vs 12% at 12 months (P = .045), and 4% vs 23% at 24 months (P = .008). Overall, the crude rate of post-SBRT compression fracture was 11.0% (45 out of the 410 treated vertebrae), and median time to VCF was 269 days (range: 0-2285 days). Cumulative incidence of treatment-induced VCF by antiresorptive use status.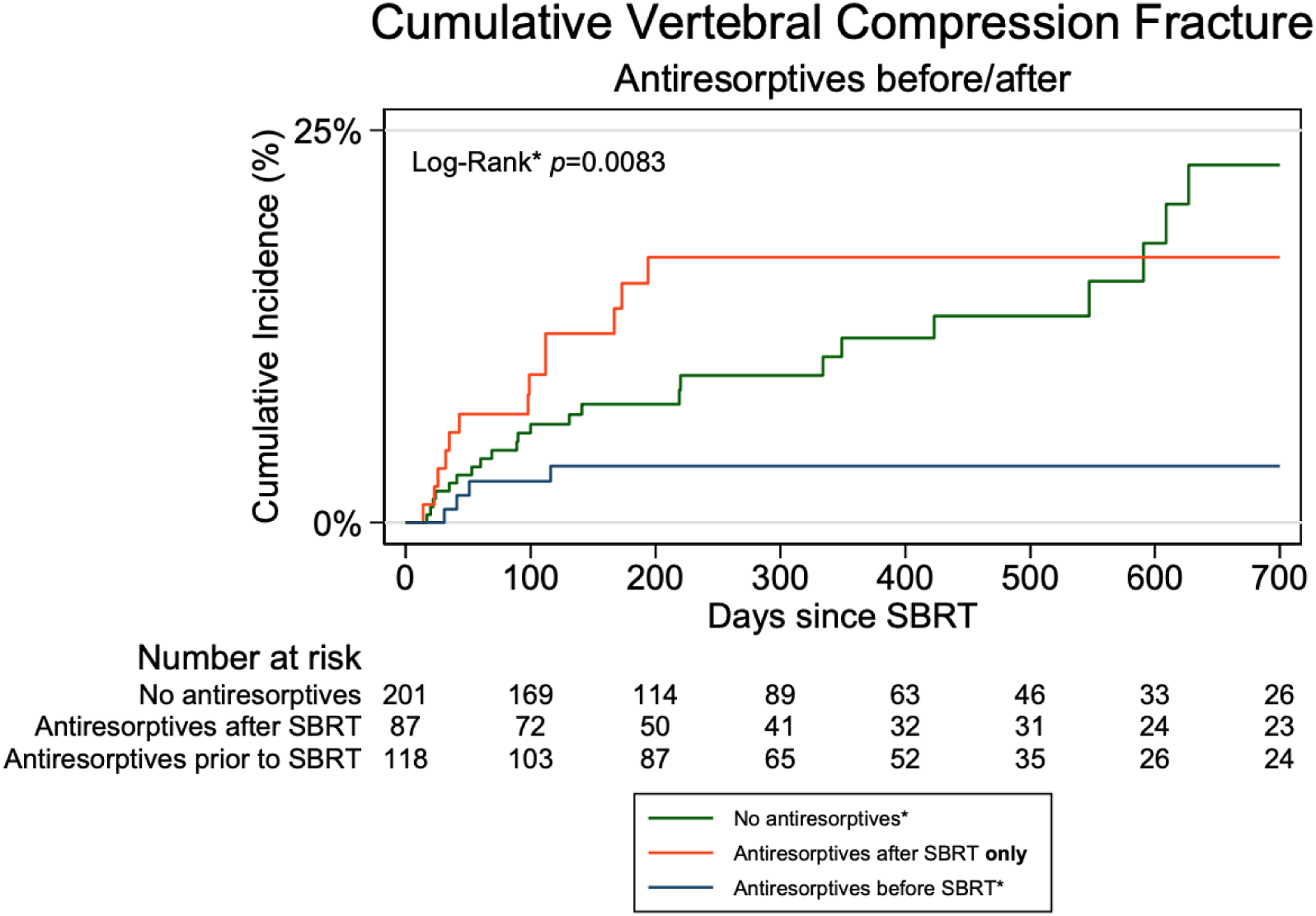
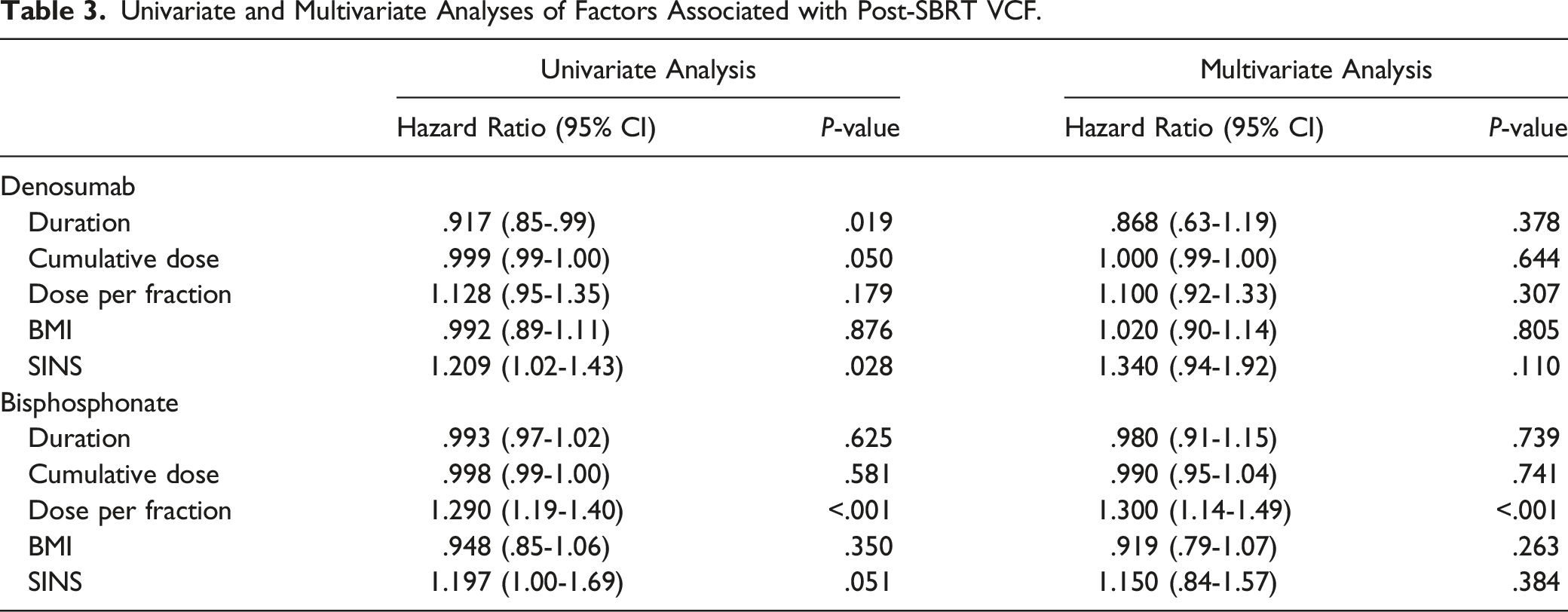
On univariate analysis for the denosumab cohort, denosumab initiation prior to SBRT had an 80% decreased risk of VCF incidence (95% CI: .04-.96, P = .045) and longer duration of use had an 8% decreased risk of VCF incidence (95% CI: .85-.99, P = .019). Higher total SINS had a 21% higher risk of VCF (95% CI: 1.02-1.43, P = .028). On univariate analysis for the bisphosphonate cohort, total SINS (HR: 1.30, 95% CI: 1.00-1.69, P = .050) and dose per fraction (HR: 1.29, 95% CI: 1.19-1.40, P < .001) were significantly associated with increased risk of VCF incidence. Bisphosphonate initiation prior to SBRT compared to those initiating after SBRT was associated with an 75% decreased risk of VCF which approached statistical significance (HR: .25, 95% CI: .04-1.38, P = .110).
Univariate and Multivariate Analyses of Factors Associated with Post-SBRT VCF.
Discussion
Although SBRT represents an excellent management approach for local control in patients with spine metastases, the risk of VCF remains high. The 12% rate of VCF at 1 year post-SBRT in this series is consistent with prior publications with VCF rates ranging from 11-39%.17-19 We present the largest study to date exploring the role of antiresorptive medications in reducing the frequency of VCF following SBRT. These data suggest that patients taking antiresorptive medication prior to SBRT had a significantly lower VCF incidence at 1 and 2 years post-SBRT compared to those not taking antiresorptive medication. Notably, while VCF cumulative incidence for those not on antiresorptive agents increased from 6-month to 2-year follow-up, the incidence remained at 4% for those initiating antiresorptive medication prior to SBRT, which is lower than would be anticipated based on historical data that did not incorporate this factor into overall VCF risk.20,21 These novel results suggest that antiresorptive medications may represent a non-invasive, low risk preventative way to reduce the risk of VCF following spine SBRT.
Denosumab use leads to a sustained 80-90% reduction of markers of bone resorption. 22 In a double-blind, multicenter study of patients receiving androgen deprivation therapy for prostate cancer, those taking denosumab had a significantly higher bone mineral density of the lumbar spine and lower 3-year vertebral fracture incidence than those in the placebo group. 23 Another study done in patients with breast cancer receiving aromatase inhibitors found similar results, demonstrating a significantly increased bone mineral density at the lumbar spine at 1-year for those taking denosumab compared to placebo. 24 Denosumab is also well-tolerated with minimal side effects, 25 and our results suggest there may be a reduced risk of radiation-induced VCF based off these properties.
As for bisphosphonates, pooled analysis of 7 studies containing 1116 patients with multiple myeloma demonstrated evidence for a difference favoring bisphosphonates compared with placebo or no treatment on prevention of pathological vertebral fractures in radiation naïve patients (RR: .74, 95% CI .62-.89). 26 In a smaller retrospective study, bisphosphonate usage for greater than 6 months prior to SBRT was significantly associated with longer VCF-free survival (P = .018), and correlation analysis showed that lack of bisphosphonate usage was the sole factor significantly correlated with post-SBRT grade 3 VCF incidence (r = −.204; P = .022). 27 Our results are consistent with these findings.
In terms of clinical predicators of VCF, recent literature has shown that SINS, including its various subcomponents, and lower BMI may predict post-SBRT VCF risk.16,28 Our findings in the denosumab cohort demonstrate a 34% higher risk of VCF incidence for patients with a higher SINS which merely approaches significance (P = .110) but nonetheless aligns with these previous results. We did not find a relationship between lower BMI and higher VCF risk, perhaps because of limited power to detect a difference. Prior publications suggest that baseline bone quality may also be related to VCF risk and a recent study by our group presented a simple approach to evaluate vertebral bone quality (VBQ) using lumbar spine MRIs. 29 Although we attempted to evaluate VBQ score for this cohort of patients, lumbar spine MRIs were not consistently available across patients.
Several studies have identified dose per fraction as another primary driver of VCF risk.16,30,31 No patients in our sizable cohort were treated with single fraction doses above 20 Gy which has previously been demonstrated to be a threshold for higher rates of VCF.16,28,32 Nonetheless, we did see a significant correlation between dose per fraction and VCF risk in the bisphosphonate subgroup. This is consistent with earlier work by our group suggesting that the volume of spine receiving lower doses of radiation also contributes to VCF risk. 21 One hypothesis is that fractionated regimens may be used to reduce VCF risk. To this end, a recent rabbit model showed that single-fraction vertebral irradiation more adversely impacted microarchitectural, cellular, and biomechanical properties of vertebral bodies than hypofractionation. 33 Future studies will be important to better understand the relationship between fractionation and VCF risk and to more explicitly explore the impact of antiresorptive agents on VCF risk following specific fractionation regimens. 34
In terms of other measures to reduce VCF risk, prior studies have explored prophylactic surgical methods35,36 and prophylactic cement augmentation 37 as potential strategies. Similarly, pre-SBRT cement augmentation may be considered and does not substantially interfere with treatment planning.38,39 Nonetheless, not all patients are candidates for invasive interventions due to factors such as age, co-morbidities or need for anti-coagulation. This alternative low-risk, non-invasive intervention, would be of particular importance to this vulnerable population.
Several limitations exist in this study including its retrospective nature and the resultant inherent biases in patient and treatment selection. In addition, there was incomplete data regarding dosages and duration of the antiresorptive agents for some patients, limiting the sample size of the study. It is important to acknowledge that the routine use of these agents is historically histology dependent, so patients on these agents may differ from those who did not take them which potentially introduces confounding bias. However, this dataset does present a broad mix of antiresorptive use across primary sites represented, rather than notable localization to any one tumor type. Additionally, although the temporal relationship was established, it was difficult to comment on specific doses or optimal duration of antiresorptive therapy. For instance, although patients initiating antiresorptive therapy were often taking it for many months or even years prior to SBRT, it remains unclear if intentional initiation of antiresorptive therapy in the weeks immediately preceding SBRT would be beneficial. This concept certainly warrants further investigation through prospective clinical trials. Nonetheless, the cumulative incidence of 4% risk of VCF at 2-year follow-up for those initiating antiresorptive agents prior to SBRT is notable and seemingly lower than the 11-39% risk seen in other series.7,18,19,28
To conclude, these data suggest that antiresorptive use prior to SBRT may reduce the risk of treatment-induced VCF. Antiresorptive agents are underutilized in patients with spine metastases and may represent a low risk and non-invasive intervention to reduce toxicity of spine SBRT. Confirmation of these findings using larger multi-institution datasets and prospective trials will be important as will an exploration of this concept in patients with non-spine bone metastases. 40
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.